Efficacy and Safety of Digital Single-Operator Cholangioscopy in the Diagnosis of Indeterminate Biliary Strictures by Targeted Biopsies: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Methods
2.1. Search Method
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Outcomes, Definitions and Gold Standard
2.6. Statistical Analysis
3. Results
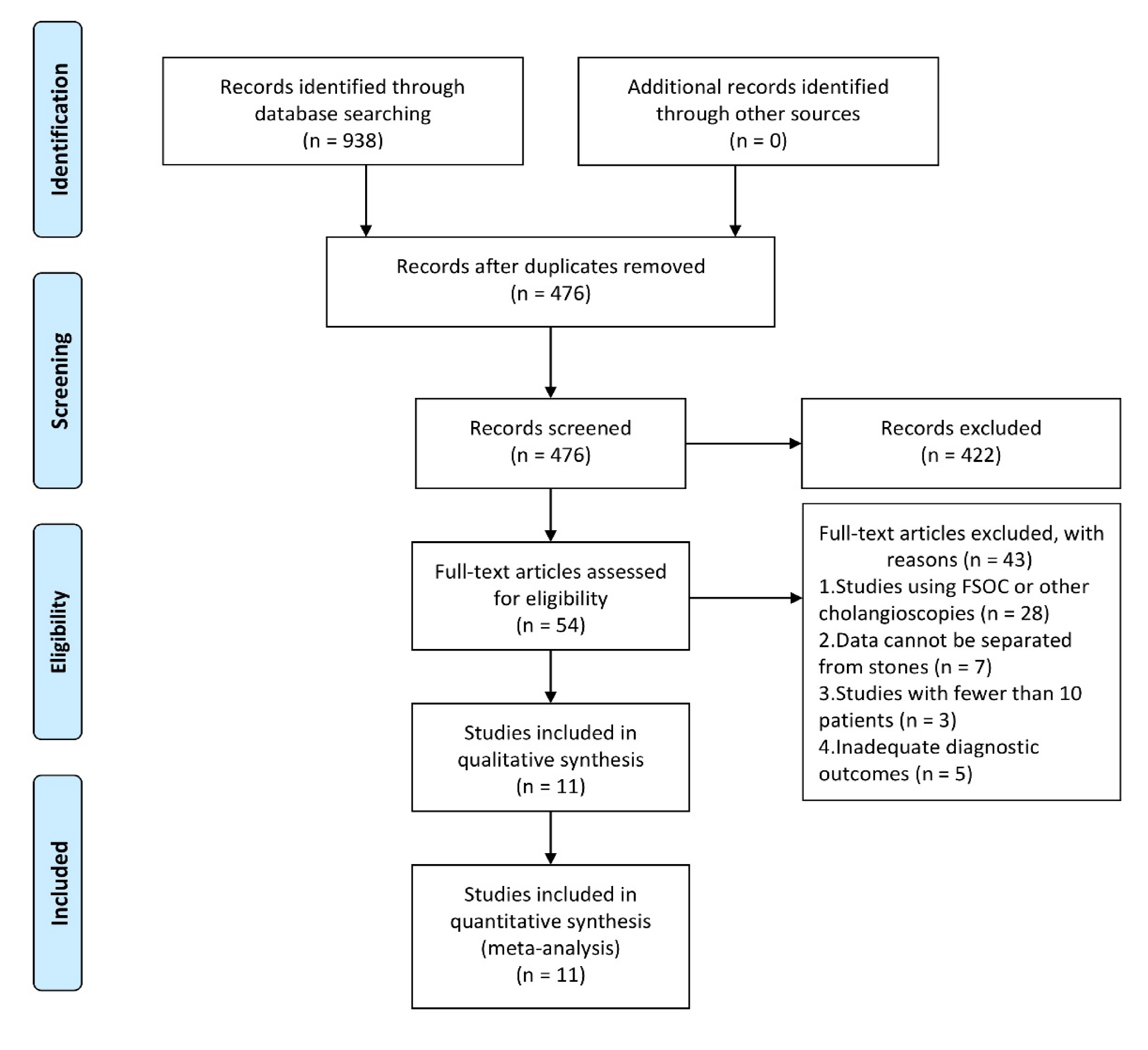
3.1. Search Results
3.2. Characteristics of the Included Studies
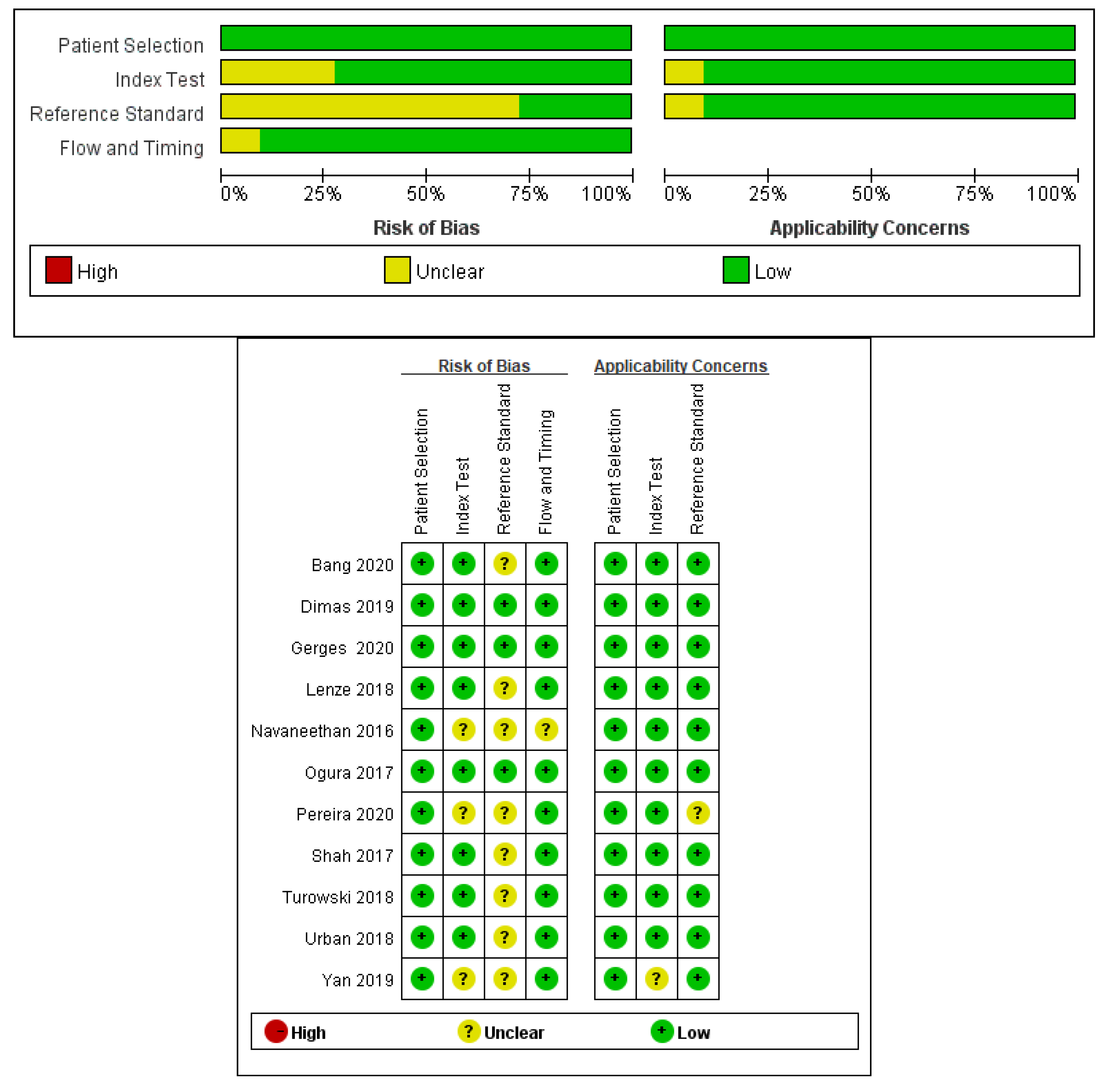
3.3. Assessment of the Bias and Quality of Studies
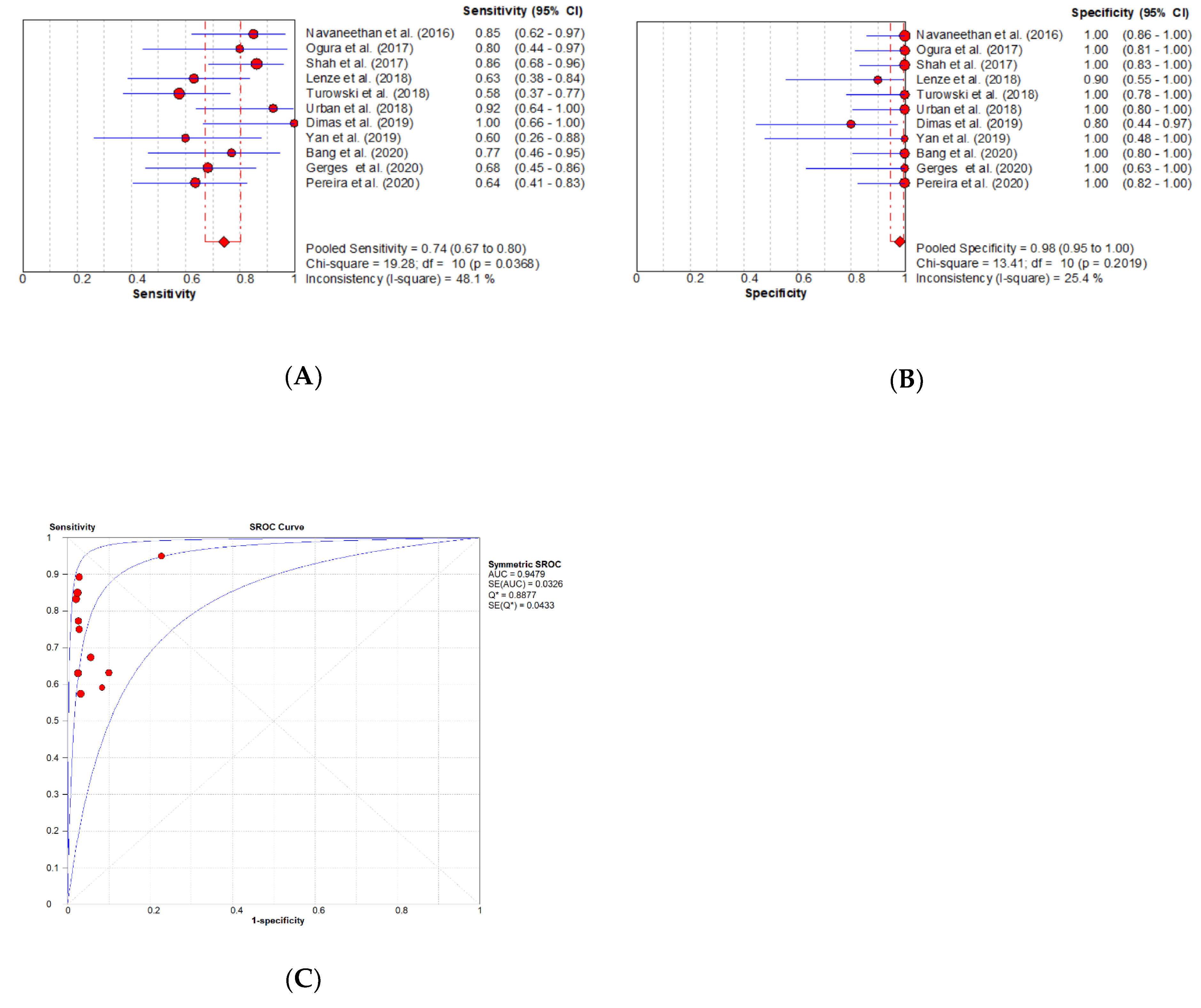
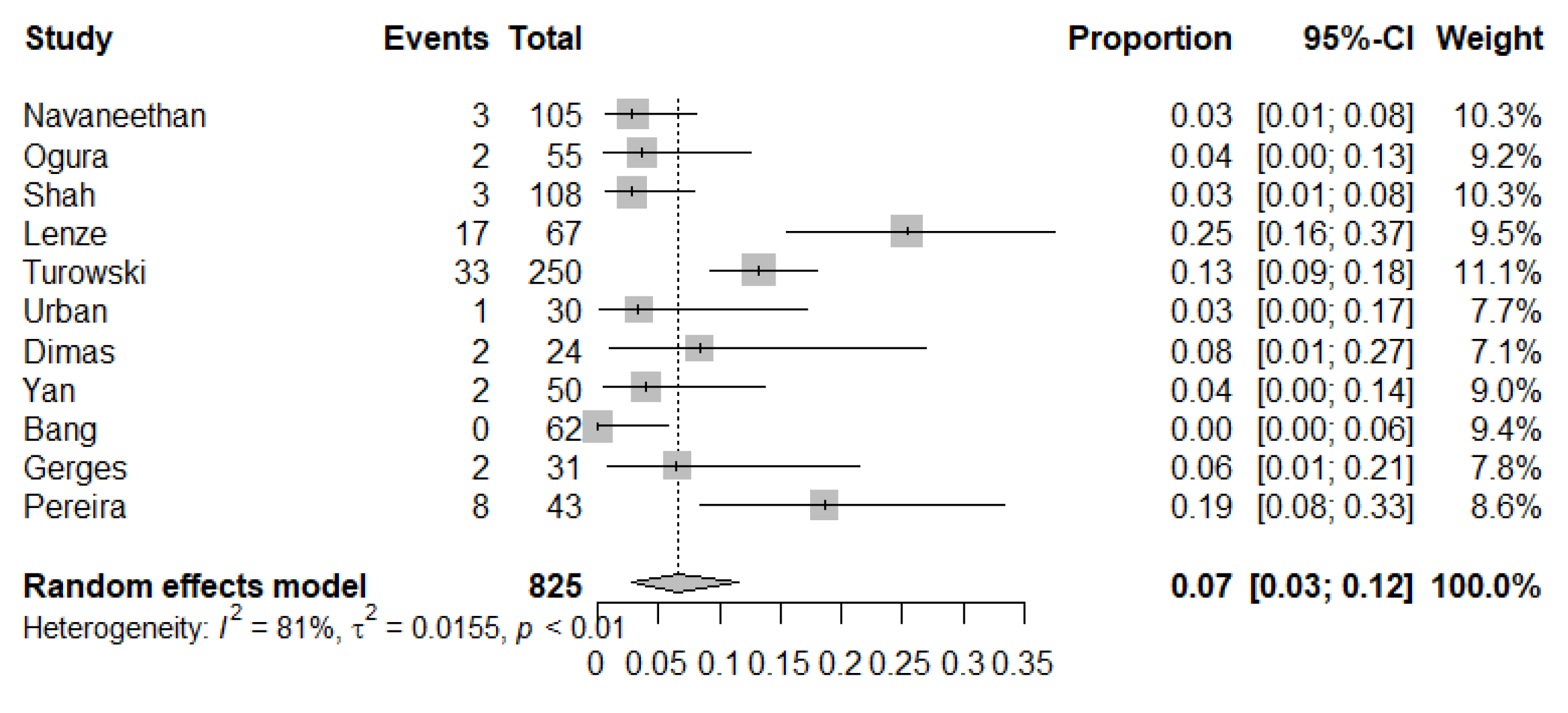
3.3.1. Meta-Analysis
3.3.2. Meta-Regression and Subgroup Analysis
3.3.3. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bowlus, C.L.; Olson, K.A.; Gershwin, M.E. Evaluation of indeterminate biliary strictures. Nat. Rev. Gastroenterol. Hepatol. 2015, 13, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Navaneethan, U.; Njei, B.; Lourdusamy, V.; Konjeti, V.R.; Vargo, J.J.; Parsi, M.A. Comparative effectiveness of biliary brush cytology and intraductal biopsy for detection of malignant biliary strictures: A systematic review and meta-analysis. Gastrointest. Endosc. 2014, 81, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Tacelli, M.; Celsa, C.; Magro, B.; Barchiesi, M.; Barresi, L.; Capurso, G.; Arcidiacono, P.G.; Cammà, C.; Crinò, S.F. Diagnostic performance of endoscopic ultrasound through-the-needle microforceps biopsy of pancreatic cystic lesions: Systematic review with meta-analysis. Dig. Endosc. 2020. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.K.; Parsi, M.A.; Binmoeller, K.F.; Hawes, R.H.; Pleskow, D.; Slivka, A.; Haluszka, O.; Petersen, B.T.; Sherman, S.; Devière, J.; et al. Single-operator cholangioscopy in patients requiring evaluation of bile duct disease or therapy of biliary stones (with videos). Gastrointest. Endosc. 2011, 74, 805–814. [Google Scholar] [CrossRef]
- Kulpatcharapong, S.; Pittayanon, R.; Kerr, S.J.; Rerknimitr, R. Diagnostic performance of different cholangioscopes in patients with biliary strictures: A systematic review. Endoscopy 2020, 52, 174–185. [Google Scholar] [CrossRef] [PubMed]
- Arvanitakis, M. Digital single-operator cholangioscopy-guided biopsy for indeterminate biliary strictures: Seeing is believing? Gastrointest. Endosc. 2020, 91, 1114–1116. [Google Scholar] [CrossRef] [PubMed]
- Navaneethan, U. You cannot go wrong: Choosing digital single-operator cholangioscopy for the diagnosis of biliary strictures. Endoscopy 2020, 52, 168–169. [Google Scholar] [CrossRef]
- De Oliveira, P.V.A.G.; De Moura, D.T.H.; Ribeiro, I.B.; Bazarbashi, A.N.; Franzini, T.; Dos Santos, M.E.L.; Bernardo, W.M.; De Moura, E.G.H. Efficacy of digital single-operator cholangioscopy in the visual interpretation of indeterminate biliary strictures: A systematic review and meta-analysis. Surg. Endosc. 2020, 1–9. [Google Scholar] [CrossRef]
- Whiting, P.; Rutjes, A.W.S.; Westwood, M.E.; Leeflang, M.M.; Sterne, J.A.C.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Bossuyt, P.M. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Pereira, P.; Santos, S.; Morais, R.; Gaspar, R.; Rodrigues-Pinto, E.; Vilas-Boas, F.; Macedo, G. Role of Peroral Cholangioscopy for Diagnosis and Staging of Biliary Tumors. Dig. Dis. 2020, 1–9. [Google Scholar] [CrossRef]
- Bang, J.Y.; Navaneethan, U.; Hasan, M.; Sutton, B.; Hawes, R.; Varadarajulu, S. Optimizing Outcomes of Single-Operator Cholangioscopy–Guided Biopsies Based on a Randomized Trial. Clin. Gastroenterol. Hepatol. 2020, 18, 441–448.e1. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.L.; Tejaswi, S. Clinical impact of digital cholangioscopy in management of indeterminate biliary strictures and complex biliary stones: A single-center study. Ther. Adv. Gastrointest. Endosc. 2019, 12. [Google Scholar] [CrossRef] [PubMed]
- Dimas, I. Comparison of digital versus fiberoptic cholangioscopy in patients requiring evaluation of bile duct disease or treatment of biliary stones. Ann. Gastroenterol. 2019, 32, 199–204. [Google Scholar] [CrossRef]
- Lenze, F.; Bokemeyer, A.; Gross, D.; Nowacki, T.; Bettenworth, D.; Ullerich, H. Safety, diagnostic accuracy and therapeutic efficacy of digital single-operator cholangioscopy. United Eur. Gastroenterol. J. 2018, 6, 902–909. [Google Scholar] [CrossRef] [PubMed]
- Turowski, F.; Hügle, U.; Dormann, A.; Bechtler, M.; Jakobs, R.; Gottschalk, U.; Nötzel, E.; Hartmann, D.; Lorenz, A.; Kolligs, F.; et al. Diagnostic and therapeutic single-operator cholangiopancreatoscopy with SpyGlassDS™: Results of a multicenter retrospective cohort study. Surg. Endosc. 2018, 32, 3981–3988. [Google Scholar] [CrossRef]
- Shah, R.J.; Raijman, I.; Brauer, B.; Gumustop, B.; Pleskow, D. Performance of a fully disposable, digital, single-operator cholangiopancreatoscope. Endoscopy 2017, 49, 651–658. [Google Scholar] [CrossRef]
- Ogura, T.; Imanishi, M.; Kurisu, Y.; Onda, S.; Sano, T.; Takagi, W.; Okuda, A.; Miyano, A.; Amano, M.; Nishioka, N.; et al. Prospective evaluation of digital single-operator cholangioscope for diagnostic and therapeutic procedures (with videos). Dig. Endosc. 2017, 29, 782–789. [Google Scholar] [CrossRef]
- Navaneethan, U.; Hasan, M.K.; Kommaraju, K.; Zhu, X.; Hébert-Magee, S.; Hawes, R.H.; Vargo, J.J.; Varadarajulu, S.; Parsi, M.A. Digital, single-operator cholangiopancreatoscopy in the diagnosis and management of pancreatobiliary disorders: A multicenter clinical experience (with video). Gastrointest. Endosc. 2016, 84, 649–655. [Google Scholar] [CrossRef]
- Gerges, C.; Beyna, T.; Tang, R.S.; Bahin, F.; Lau, J.Y.; Van Geenen, E.; Neuhaus, H.; Reddy, D.N.; Ramchandani, M. Digital single-operator peroral cholangioscopy-guided biopsy sampling versus ERCP-guided brushing for indeterminate biliary strictures: A prospective, randomized, multicenter trial (with video). Gastrointest. Endosc. 2019, 91, 1105–1113. [Google Scholar] [CrossRef]
- Urban, O.; Škanderová, E.; Fojtík, P.; Lovecek, M.; Falt, P. Sa1328 digital cholangioscopy: The diagnostic yield and impact on management of patients with indeterminate biliary stricture. Gastrointest. Endosc. 2018, 87, AB215. [Google Scholar] [CrossRef]
- Navaneethan, U.; Hasan, M.K.; Lourdusamy, V.; Njei, B.; Varadarajulu, S.; Hawes, R.H. Single-operator cholangioscopy and targeted biopsies in the diagnosis of indeterminate biliary strictures: A systematic review. Gastrointest. Endosc. 2015, 82, 608–614.e2. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Zhou, Z.; Tian, J.; Wang, Z.; Huang, Q.; Fan, K.; Mao, Y.; Sun, G.; Yang, Y.-S. Is single-operator peroral cholangioscopy a useful tool for the diagnosis of indeterminate biliary lesion? A systematic review and meta-analysis. Gastrointest. Endosc. 2015, 82, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Puli, S.R.; Bechtold, M.L.; Buxbaum, J.L.; Eloubeidi, M.A. How Good Is Endoscopic Ultrasound–Guided Fine-Needle Aspiration in Diagnosing the Correct Etiology for a Solid Pancreatic Mass? Pancreas 2013, 42, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Gonda, T.A.; Glick, M.P.; Sethi, A.; Poneros, J.M.; Palmas, W.; Iqbal, S.; Gonzalez, S.; Nandula, S.V.; Emond, J.C.; Brown, R.S.; et al. Polysomy and p16 deletion by fluorescence in situ hybridization in the diagnosis of indeterminate biliary strictures. Gastrointest. Endosc. 2012, 75, 74–79. [Google Scholar] [CrossRef]
- Fugazza, A.; Gaiani, F.; Carra, M.C.; Brunetti, F.; Levy, M.; Sobhani, I.; Azoulay, D.; Catena, F.; Angelis, G.L.D.; De Angelis, N. Confocal Laser Endomicroscopy in Gastrointestinal and Pancreatobiliary Diseases: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2016, 2016, 1–31. [Google Scholar] [CrossRef]
- Mounzer, R.; Austin, G.L.; Wani, S.; Brauer, B.C.; Fukami, N.; Shah, R.J. Per-oral video cholangiopancreatoscopy with narrow-band imaging for the evaluation of indeterminate pancreaticobiliary disease. Gastrointest. Endosc. 2017, 85, 509–517. [Google Scholar] [CrossRef]
- Mizrahi, M.; Khoury, T.; Wang, Y.; Cohen, J.; Sheridan, J.; Chuttani, R.; Berzin, T.M.; Sawhney, M.S.; Pleskow, D. “Apple Far from the Tree”: Comparative effectiveness of fiberoptic single-operator cholangiopancreatoscopy (FSOCP) and digital SOCP (DSOCP). HPB 2018, 20, 285–288. [Google Scholar] [CrossRef]
- Kalaitzakis, E.; Webster, G.J.; Oppong, K.W.; Kallis, Y.; Vlavianos, P.; Huggett, M.; Dawwas, M.F.; Lekharaju, V.; Hatfield, A.; Westaby, D.; et al. Diagnostic and therapeutic utility of single-operator peroral cholangioscopy for indeterminate biliary lesions and bile duct stones. Eur. J. Gastroenterol. Hepatol. 2012, 24, 656–664. [Google Scholar] [CrossRef]
- Jin, Z.; Wei, Y.; Tang, X.; Shen, S.; Yang, J.; Jin, H.; Zhang, X. Single-operator peroral cholangioscope in treating difficult biliary stones: A systematic review and meta-analysis. Dig. Endosc. 2018, 31, 256–269. [Google Scholar] [CrossRef]
- Sethi, A.; Doukides, T.P.; Sejpal, D.V.; Pleskow, D.; Slivka, A.; Adler, U.G.; Shah, R.J.; Edmundowicz, S.A.; Itoi, T.; Petersen, B.T.; et al. Interobserver Agreement for Single Operator Choledochoscopy Imaging: Can We Do Better? Diagn. Ther. Endosc. 2014, 2014, 1–4. [Google Scholar] [CrossRef]
- Sethi, A.; Tyberg, A.; Slivka, A.; Adler, D.G.; Desai, A.P.; Sejpal, D.V.; Pleskow, D.K.; Bertani, H.; Gan, S.-I.; Shah, R.; et al. Digital Single-operator Cholangioscopy (DSOC) Improves Interobserver Agreement (IOA) and Accuracy for Evaluation of Indeterminate Biliary Strictures. J. Clin. Gastroenterol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Egger, M.; Smith, G.D. Systematic reviews in health care: Investigating and dealing with publication and other biases in meta-analysis. BMJ 2001, 323, 101–105. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Country | Study Design | Age (y) Mean ± SD | Gender, MALE n (%) | No. of SB | AEs n (%) | No. of Patients | Raw Data of VI | Raw Data of SB | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| VI | SB | TP | FP | FN | TN | TP | FP | FN | TN | |||||||
| Navaneethan et al. [18] (2016) | USA | Retrospective Multicenter | 62 ± 15.3 ‡ | 56 (53.3) ‡ | 1 (1–6) | 3 (2.9) | 44 | 44 | 18 | 1 | 2 | 23 | 17 | 0 | 3 | 24 |
| Ogura et al. [17] (2017) | Japan | Prospective Single center | 69 (43–89) | 24 (72.7) | 2.75 | 2 (3.7) | 30 | 28 | 10 | 2 | 2 | 16 | 8 | 0 | 2 | 18 |
| Shah et al. [16] (2017) | USA | Prospective Multicenter | 59.7 ± 8.3 ‡ | 57 (53) ‡ | NR | 3 (2.8) | 74 | 49 | 28 | 3 | 1 | 42 | 25 | 0 | 4 | 20 |
| Lenze et al. [14] (2018) | Germany | Retrospective Single center | 66 (54–77) ‡ | 38 (56.7) ‡ | 3 | 17 (25.4) | 67 | 29 | 24 | 1 | 3 | 39 | 12 | 1 | 7 | 9 |
| Turowski et al. [15] (2018) | Germany | Retrospective Multicenter | 68 ± 14.4 ‡ | 97 (47.1) ‡ | 1.31 | 33 (13.2) | 99 | 41 | 42 | 3 | 2 | 52 | 15 | 0 | 11 | 15 |
| Urban et al. [20] (2018) | Czech | Prospectively Single center | 67.3 ± 10.7 | 19 (63) | 5 (0–13) | 1 (3.3) | 30 | 30 | 13 | 4 | 0 | 13 | 12 | 0 | 1 | 17 |
| Dimas et al. [13] (2019) | Greece | Retrospective Single center | 64.2 ± 19.1 | 15 (62.5) | NR | 2 (8.3) | 19 | 19 | 9 | 0 | 0 | 10 | 9 | 2 | 0 | 8 |
| Yan et al. [12] (2019) | USA | Retrospective Single center | 59.7 (21–86) | 15 (68) | NR | 2 (4.0) | 22 | 15 | 10 | 0 | 0 | 12 | 6 | 0 | 4 | 5 |
| Bang et al. [11] (2020) | USA | RCT Single center | 66.4 ± 14.7 | 38 (61.3) | 1 (1–1.5) | 0 | 0 | 30 | 0 | 0 | 0 | 0 | 10 | 0 | 3 | 17 |
| Gerges et al. [19] (2020) | multiple continents | RCT Multicenter | 62 (54–79) | 17 (54.8) | 1.18 | 2 (6.5) | 31 | 30 | 21 | 3 | 1 | 6 | 15 | 0 | 7 | 8 |
| Pereira et al. [10] (2020) | Portugal | Retrospective Single center | 61 ± 13 ‡ | 27 (62.8) ‡ | NA | 8 (18.6) | 41 | 41 | 22 | 2 | 0 | 17 | 14 | 0 | 8 | 19 |
| Diagnostic Method | Sensitivity (%) | Specificity (%) | Accuracy (%) |
|---|---|---|---|
| DSOC visual impression | 95 | 92 | 94 |
| DSOC SpyBite biopsy | 74 | 98 | 85 |
| FSOC visual impression | 84.5 | 82.6 | 83.5 |
| FSOC SpyBite biopsy | 60.1 | 98 | 78 |
| DPCS visual impression | 83–92 | 84–92 | NA |
| DPCS biopsy | 43–89.5 | 97 | NA |
| ERCP brush cytology and biopsy | 59.4 | 100 | 50 |
| ERCP plus FISH | 79 | 91 | 80 |
| EUS-FNA | 43–86 | 96 | NA |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wen, L.-J.; Chen, J.-H.; Xu, H.-J.; Yu, Q.; Liu, K. Efficacy and Safety of Digital Single-Operator Cholangioscopy in the Diagnosis of Indeterminate Biliary Strictures by Targeted Biopsies: A Systematic Review and Meta-Analysis. Diagnostics 2020, 10, 666. https://doi.org/10.3390/diagnostics10090666
Wen L-J, Chen J-H, Xu H-J, Yu Q, Liu K. Efficacy and Safety of Digital Single-Operator Cholangioscopy in the Diagnosis of Indeterminate Biliary Strictures by Targeted Biopsies: A Systematic Review and Meta-Analysis. Diagnostics. 2020; 10(9):666. https://doi.org/10.3390/diagnostics10090666
Chicago/Turabian StyleWen, Li-Jia, Jun-Hong Chen, Hong-Ji Xu, Qiong Yu, and Kai Liu. 2020. "Efficacy and Safety of Digital Single-Operator Cholangioscopy in the Diagnosis of Indeterminate Biliary Strictures by Targeted Biopsies: A Systematic Review and Meta-Analysis" Diagnostics 10, no. 9: 666. https://doi.org/10.3390/diagnostics10090666
APA StyleWen, L.-J., Chen, J.-H., Xu, H.-J., Yu, Q., & Liu, K. (2020). Efficacy and Safety of Digital Single-Operator Cholangioscopy in the Diagnosis of Indeterminate Biliary Strictures by Targeted Biopsies: A Systematic Review and Meta-Analysis. Diagnostics, 10(9), 666. https://doi.org/10.3390/diagnostics10090666