Ovarian Carcinosarcoma with Retroperitoneal Para-Aortic Lymph Node Dissemination Followed by an Unusual Postoperative Complication: A Case Report with a Brief Literature Review

 ,
,  , ,
, , 
Abstract
1. Introduction
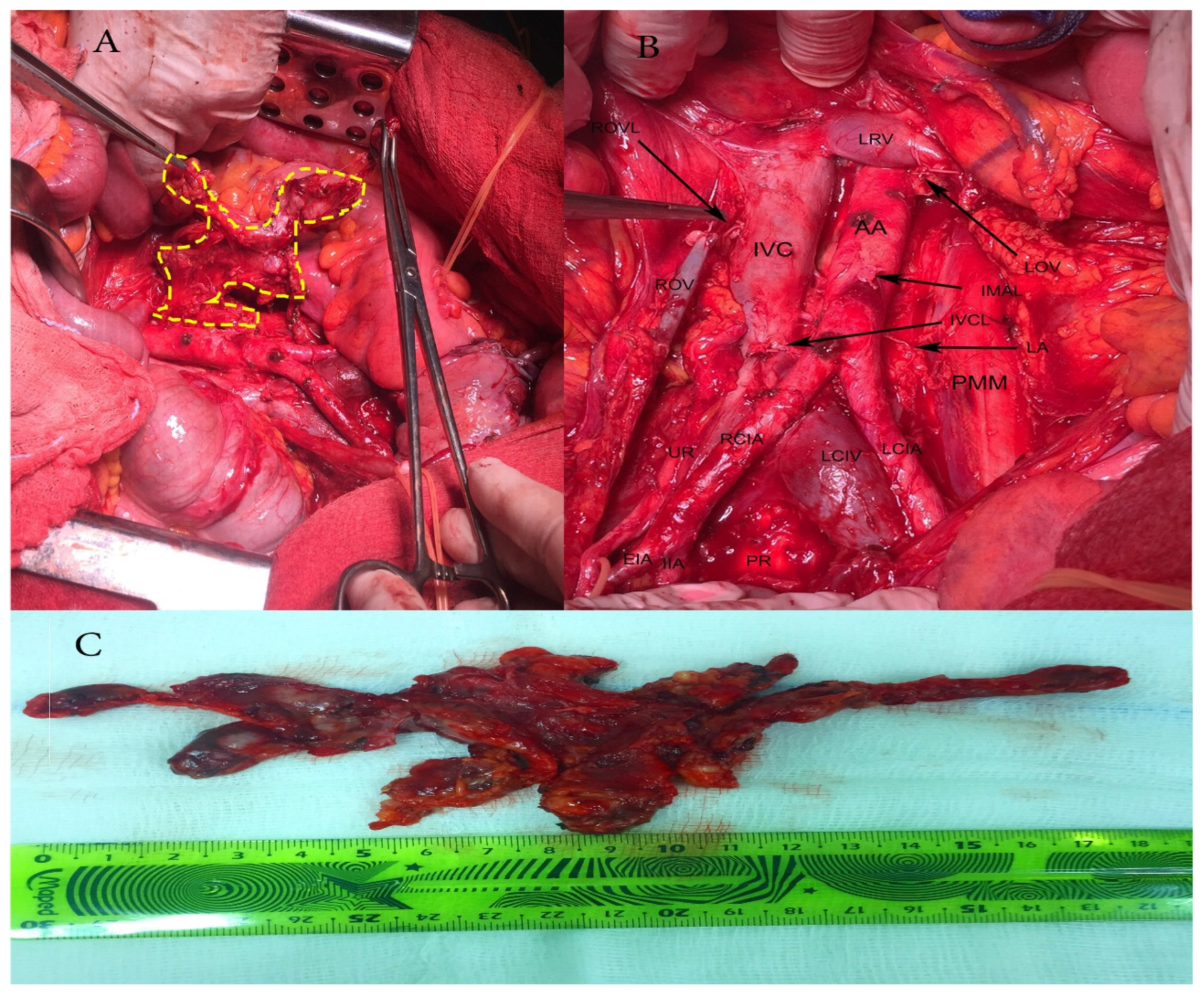
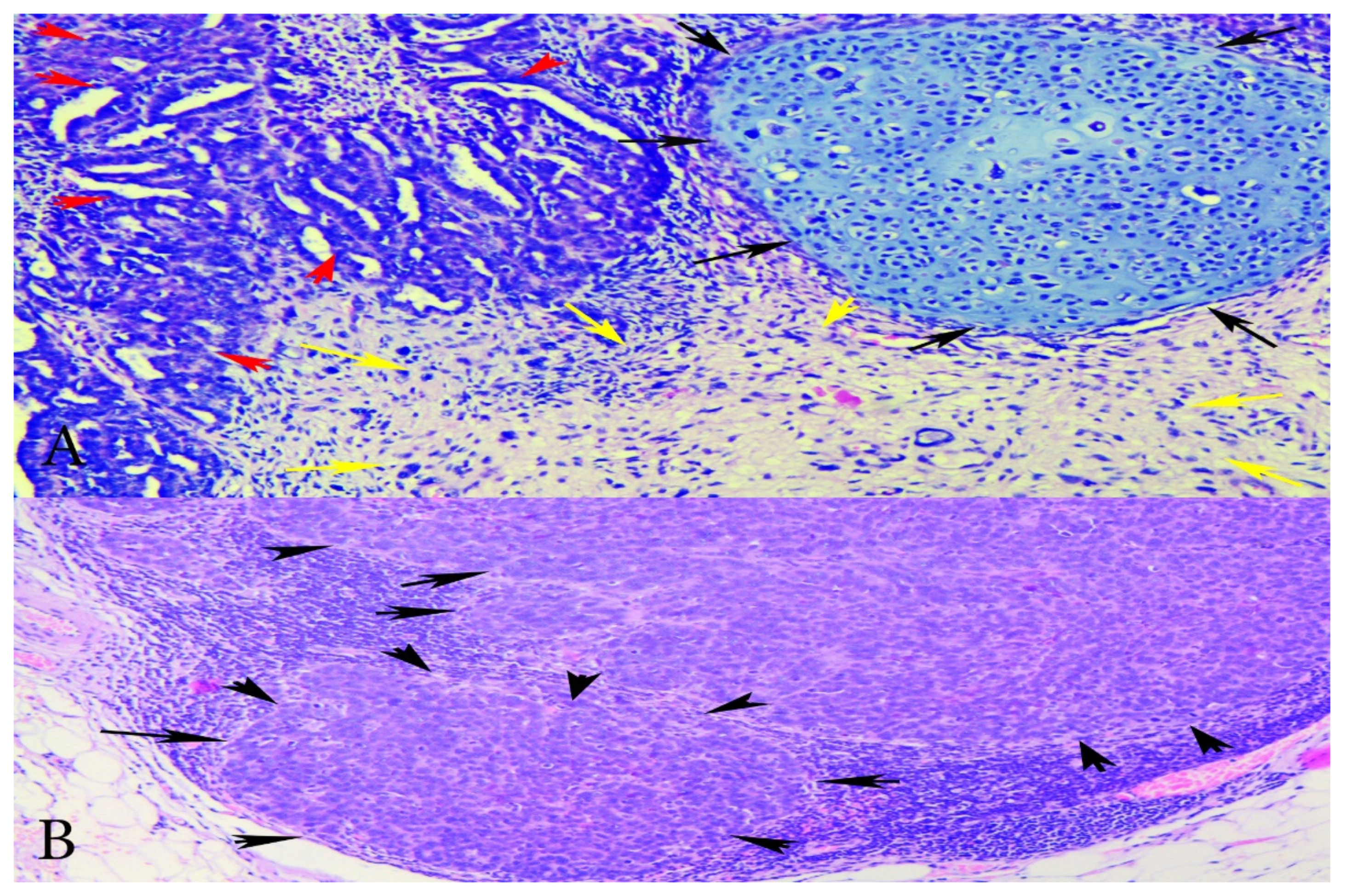
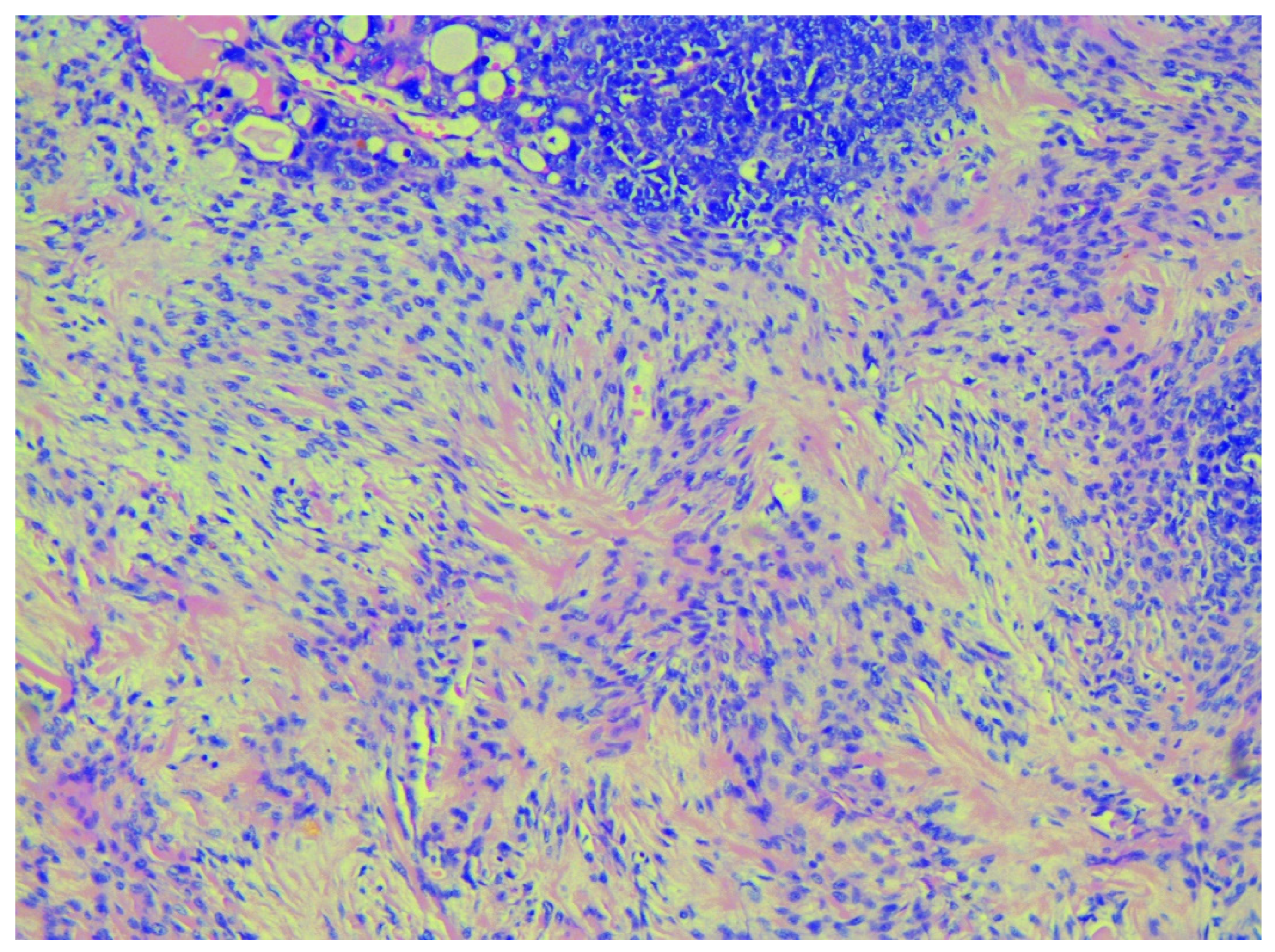
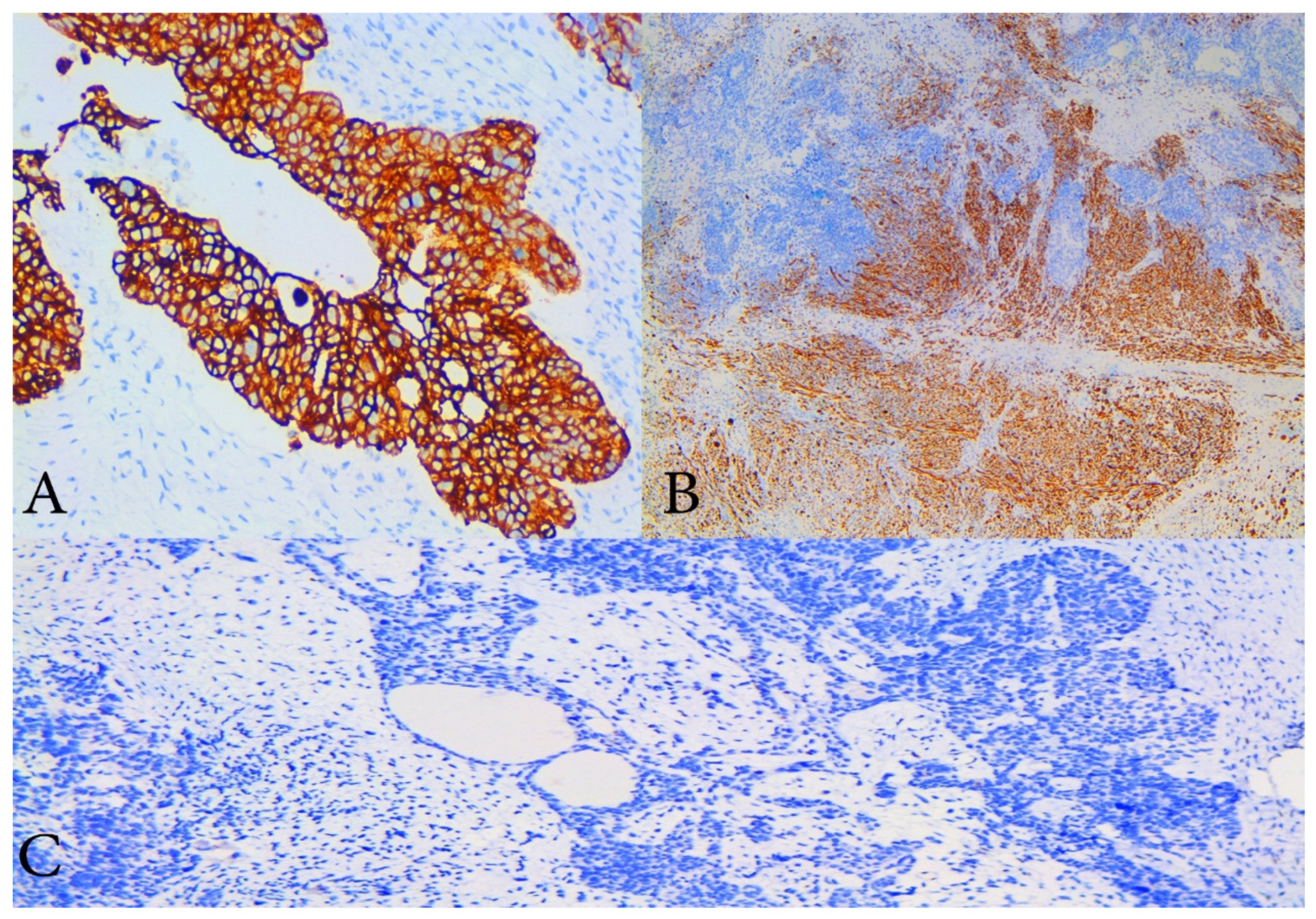
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Boussios, S.; Karathanasi, A.; Zakynthinakis-Kyriakou, N.; Tsiouris, A.K.; Chatziantoniou, A.A.; Kanellos, F.S.; Tatsi, K. Ovarian carcinosarcoma: Current developments and future perspectives. Crit. Rev. Oncol. Hematol. 2019, 134, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Daimon, A.; Fujiwara, S.; Tanaka, Y.; Tanaka, T.; Ohmichi, M. A rare case of ovarian carcinosarcoma with squamous cell carcinoma. J. Ovarian Res. 2019, 12, 32. [Google Scholar] [CrossRef] [PubMed]
- Makris, G.M.; Siristatidis, C.; Battista, M.J.; Chrelias, C. Ovarian carcinosarcoma: A case report, diagnosis, treatment and literature review. Hippokratia 2015, 19, 256–259. [Google Scholar]
- Belbaraka, R.; Taleb, A.; Errihani, H. A Rare Tumor of the Ovary: Carcinosarcoma. J. Med. Cases 2010, 1, 55–57. [Google Scholar] [CrossRef]
- Dasgupta, S.; Bose, D.; Bhattacharyya, N.K.; Biswas, P.K. Carcinosarcoma of ovary with its various immunohistochemical expression: Report of a rare case. J. Cancer Res. Ther. 2015, 11, 1022. [Google Scholar] [CrossRef] [PubMed]
- Inthasorn, P.; Beale, P.; Dalrymple, C.; Carter, J. Malignant mixed mullerian tumour of the ovary: Prognostic factor and response of adjuvant platinum-based chemotherapy. Aust. N. Z. J. Obstet. Gynaecol. 2003, 43, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Uçar, M.G.; Çakir, T.; Ilhan, T.T.; Karabagli, P.; Çelik, Ç. Primary Ovarian Malignant Mixed Mullerian Tumour: A Case Report and Brief Review of Literature. J. Clin. Diagn. Res. 2016, 10, QD04–QD06. [Google Scholar] [CrossRef]
- Timmerman, D.; Valentin, L.; Bourne, T.H.; Collins, W.P.; Verrelst, H.; Vergote, I.; International Ovarian Tumor Analysis (IOTA) Group. Terms, definitions and measurements to describe the sonographic features of adnexal tumours: A consensus opinion from the International Ovarian Tumor Analysis (IOTA) Group. Ultrasound Obstet. Gynecol. 2000, 16, 500–505. [Google Scholar] [CrossRef]
- Abramowicz, J.S.; Timmerman, D. Ovarian mass-differentiating benign from malignant: The value of the International Ovarian Tumor Analysis ultrasound rules. Am. J. Obstet. Gynecol. 2017, 217, 652–660. [Google Scholar] [CrossRef]
- Available online: https://emedicine.medscape.com/article/2007140-overview (accessed on 20 September 2020).
- Priyadarshini, P.; Majumdar, S.K.; Parida, D.K. Carcinosarcoma of ovary with long-term overall survival. Oncol. J. India 2019, 3, 41–44. [Google Scholar] [CrossRef]
- Duman, B.B.; Kara, I.O.; Günaldi, M.; Ercolak, V. Malignant mixed Mullerian tumour of the ovary with two cases and review of the literature. Arch. Gynecol. Obstet. 2011, 283, 1363–1368. [Google Scholar] [CrossRef] [PubMed]
- Chiu, S.Y.; Twu, N.F.; Lai, C.H.; Yen, M.S.; Chao, K.C. Primary malignant mixed müllerian tumour of the ovary. Taiwan J. Obstet. Gynecol. 2010, 49, 87–90. [Google Scholar] [CrossRef] [PubMed][Green Version]
- del Carmen, M.G.; Birrer, M.; Schorge, J.O. Carcinosarcoma of the ovary: A review of the literature. Gynecol. Oncol. 2012, 125, 271–277. [Google Scholar] [CrossRef] [PubMed]
- McCluggage, W.G. Malignant biphasic uterine tumours: Carcinosarcomas or metaplastic carcinomas? J. Clin. Pathol. 2002, 55, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Mayall, F.; Rutty, K.; Campbell, F.; Goddard, H. p53 immunostaining suggests that uterine carcinosarcomas are monoclonal. Histopathology 1994, 24, 211–214. [Google Scholar] [CrossRef]
- Moritani, S.; Moriya, T.; Kushima, R.; Sugihara, H.; Harada, M.; Hattori, T. Ovarian carcinoma recurring as carcinosarcoma. Pathol. Int. 2001, 51, 380–384. [Google Scholar] [CrossRef]
- Hale, D.; Senem, D.A.; Ovgu, A.; Hakan, E.; Sennur, I.; Zerrin, C.; Fuat, D. Serous Ovarian Carcinoma Recurring as Malignant Mixed Mullerian Tumor. Case Rep. Obstet. Gynecol. 2015, 2015, 612824. [Google Scholar] [CrossRef]
- Badyal, R.; Dey, P. Primary ovarian malignant mixed mullerian tumours/carcinosarcomas: A clinico-pathological and immunohistochemical analysis of four cases and review of literature. Ann. Pathol. Lab. Med. 2015, 2, 50–57. [Google Scholar]
- Sood, A.K.; Sorosky, J.I.; Gelder, M.S.; Buller, R.E.; Anderson, B.; Wilkinson, E.J.; Benda, J.A.; Morgan, L.S. Primary ovarian sarcoma: Analysis of prognostic variables and the role of surgical cytoreduction. Cancer 1998, 82, 1731–1737. [Google Scholar] [CrossRef]
- Althavale, R.; Thomakos, N.; Godrey, K.; Kew, F.; Cross, P.; de Barros Lopes, A.; Hatem, M.H.; Naik, R. The effect of epithelial and stromal tumour components on FIGO stages III and IV ovarian carcinosarcomas treated with primary surgery and chemotherapy. Int. J. Gynecol. Cancer 2007, 17, 1025–1030. [Google Scholar] [CrossRef]
- George, E.; Lillemoe, T.J.; Twiggs, L.B.; Perrone, T. Malignant mixed müllerian tumour versus high-grade endometrial carcinoma and aggressive variants of endometrial carcinoma: A comparative analysis of survival. Int. J. Gynecol. Pathol. 1995, 14, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Nayha, V.; Stenback, F. Angiogenesis and expression of angiogenic agents in uterine and ovarian carcinosarcomas. APMIS 2008, 116, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.S.; Kohler, M.F.; Marks, J.R.; Bast, R.C., Jr.; Boyd, J.; Berchuck, A. Mutation and overexpression of the p53 tumour suppressor gene frequently occurs in uterine and ovarian sarcomas. Obstet. Gynecol. 1994, 83, 118–124. [Google Scholar] [PubMed]
- Ariyoshi, K.; Kawauchi, S.; Kaku, T.; Nakano, H.; Tsuneyoshi, M. Prognostic factors in ovarian carcinosarcoma: A clinicopathological and immunohistochemical analysis of 23 cases. Histopathology 2000, 37, 427–436. [Google Scholar] [CrossRef]
- Kunkel, J.; Peng, Y.; Tao, Y.; Krigman, H.; Cao, D. Presence of a sarcomatous component outside the ovary is an adverse prognostic factor for primary ovarian malignant mixed mesodermal/mullerian tumours: A clinicopathologic study of 47 cases. Am. J. Surg. Pathol. 2012, 36, 831–837. [Google Scholar] [CrossRef]
- Jain, V.; Pundir, S.; Sekhon, R.; Mishra, A.; Nayyar, N.; Vishwakarma, G.; Kamboj, M.; Rawal, S. Carcinosarcoma of the Ovary: A Single-Institute Experience with Surgical Cytoreduction and Platinum-Based Chemotherapy. J. Gynecol. Surg. 2019, 35, 224–231. [Google Scholar] [CrossRef]
- Debuquoy, C.; Romeo, C.; Vanacker, H.; Ray-Coquard, I. Rare ovarian tumours: An update on diagnosis and treatment. Int. J. Gynecol. Cancer 2020, 30, 879–887. [Google Scholar] [CrossRef]
- Feng, Z.; Wen, H.; Jiang, Z.; Liu, S.; Ju, X.; Chen, X.; Xia, L.; Xu, J.; Bi, R.; Wu, X. A triage strategy in advanced ovarian cancer management based on multiple predictive models for R0 resection: A prospective cohort study. J. Gynecol. Oncol. 2018, 29, e65. [Google Scholar] [CrossRef]
- Barakat, R.R.; Rubin, S.C.; Wong, G.; Saigo, P.E.; Markman, M.; Hoskins, W.J. Mixed mesodermal tumour of the ovary: Analysis of prognostic factors in 31 cases. Obstet. Gynecol. 1992, 80, 660–664. [Google Scholar]
- Plaxe, S.C.; Dottino, P.R.; Goodman, H.M.; Deligdisch, L.; Idelson, M.; Cohen, C.J. Clinical features of advanced ovarian mixed mesodermal tumours and treatment with doxorubicin and cisplatin-based chemotherapy. Gynecol. Oncol. 1990, 37, 244–249. [Google Scholar] [CrossRef]
- Duska, L.R.; Garrett, A.; Eltabbakh, G.H.; Oliva, E.; Penson, R.; Fuller, A.F. Paclitaxel and platinum chemotherapy for malignant mixed mullerian tumours of the ovary. Gynecol. Oncol. 2002, 85, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Rutledge, T.L.; Gold, M.A.; McMeekin, D.S.; Huh, W.K.; Powell, M.A.; Lewin, S.N.; Mutch, D.G.; Johnson, G.A.; Walker, J.L.; Mannel, R.S. Carcinosarcoma of the ovary—A case series. Gynecol. Oncol. 2006, 100, 128–132. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Available online: http://www.nccn.org (accessed on 20 September 2020).
- Jernigan, A.M.; Fader, A.N.; Nutter, B.; Rose, P.; Tseng, J.H.; Escobar, P.F. Ovarian carcinosarcoma: Effects of cytoreductive status and platinum-based chemotherapy on survival. Obstet. Gynecol. Int. 2013, 2013, 490508. [Google Scholar] [CrossRef] [PubMed]
- Morrow, C.P.; Bundy, B.N.; Hoffman, J.; Sutton, G.; Homesley, H. Adriamycin chemotherapy for malignant mixed mesodermal tumour of the ovary. A Gynecologic Oncology Group Study. Am. J. Clin. Oncol. 1986, 9, 24–26. [Google Scholar] [CrossRef] [PubMed]
- Brackmann, M.; Stasenko, M.; Uppal, S.; Erba, J.; Reynolds, R.K.; McLean, K. Comparison of first-line chemotherapy regimens for ovarian carcinosarcoma: A single institution case series and review of the literature. BMC Cancer 2018, 18, 172. [Google Scholar] [CrossRef]
- Heinzelmann-Schwarz, V.; Kind, A.B.; Vetter, M.; Russell, K.; Omar, S.; Schoetzau, A.; Hoeck, K.; Fink, D.; Friedlander, M.L.; Hacker, N.F. Should MMMT still be treated with adjuvant taxane-based combination chemotherapy? J. Cancer Res. Clin. Oncol. 2020, 146, 695–704. [Google Scholar] [CrossRef]
- Yalcin, I.; Meydanli, M.M.; Turan, A.T.; Taskin, S.; Sari, M.E.; Gungor, T.; Akbayir, O.; Ayhan, A. Carcinosarcoma of the ovary compared to ovarian high-grade serous carcinoma: Impact of optimal cytoreduction and standard adjuvant treatment. Int. J. Clin. Oncol. 2018, 23, 329–337. [Google Scholar] [CrossRef]
- Brown, E.; Stewart, M.; Rye, T.; Al-Nafussi, A.; Williams, A.R.; Bradburn, M.; Smyth, J.; Gabra, H. Carcinosarcoma of the ovary: 19 years of prospective data from a single center. Cancer 2004, 100, 2148–2153. [Google Scholar] [CrossRef]
- Loizzi, V.; Cormio, G.; Camporeale, A.; Falagario, M.; De Mitri, P.; Scardigno, D.; Putignano, G.; Selvaggi, L.E. Carcinosarcoma of the ovary: Analysis of 13 cases and review of the literature. Oncology 2011, 80, 102–106. [Google Scholar] [CrossRef]
- Nizam, A.; Bustamante, B.; Shan, W.; Shih, K.K.; Whyte, J.S.; Sakaris, A.; Dos Santos, L.; Frimer, M.; Menzin, A.W.; Truskinovsky, A.; et al. Overall Survival and Adjuvant Therapy in Women with Ovarian Carcinosarcoma: A Single-Institution Experience. Diagnostics 2019, 9, 200. [Google Scholar] [CrossRef]
- Chi, D.S.; Mychalczak, B.; Saigo, P.E.; Rescigno, J.; Brown, C.L. The role of whole-pelvic irradiation in the treatment of early-stage uterine carcinosarcoma. Gynecol. Oncol. 1997, 65, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Geisler, J.P.; Wiemann, M.C.; Miller, G.A.; Zhou, Z.; Geisler, H.E. Estrogen and progesterone receptors in malignant mixed mesodermal tumours of the ovary. J. Surg. Oncol. 1995, 59, 45–47. [Google Scholar] [CrossRef] [PubMed]
- Ansink, A.C.; Cross, P.A.; Scorer, P.; de Barros Lopes, A.; Monaghan, J.M. The hormonal receptor status of uterine carcinosarcomas (mixed müllerian tumours): An immunohistochemical study. J. Clin. Pathol. 1997, 50, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Chandran, E.; Kennedy, I. Significant Tumor Response to the Poly (ADP-ribose) Polymerase Inhibitor Olaparib in Heavily Pretreated Patient with Ovarian Carcinosarcoma Harboring a Germline RAD51D Mutation. JCO Precis. Oncol. 2018. [Google Scholar] [CrossRef]
- Charan, I.; Kapoor, A.; Singhal, M.K.; Jagawat, N.; Bhavsar, D.; Jain, V.; Kumar, V.; Kumar, H.S. High Ligation of Inferior Mesenteric Artery in Left Colonic and Rectal Cancers: Lymph Node Yield and Survival Benefit. Indian J. Surg. 2015, 77 (Suppl. 3), 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Li, A. High ligation of inferior mesenteric artery in laparoscopic resection of rectal cancer: Is it safe or dangerous? Ann. Laparosc. Endosc. Surg. 2016, 1, 49. [Google Scholar] [CrossRef]
- Horvath, S.; George, E.; Herzog, T.J. Unintended consequences: Surgical complications in gynecologic cancer. Womens Health (Lond.) 2013, 9, 595–604. [Google Scholar] [CrossRef]
- Fauci, J.M.; Schneider, K.E.; Frederick, P.J.; Wilding, G.; Consiglio, J.; Sutton, A.L.; Kilgore, L.C.; Barnes, M.N. Assessment of risk factors for 30-day hospital readmission after surgical cytoreduction in epithelial ovarian carcinoma. Int. J. Gynecol. Cancer 2011, 21, 806–810. [Google Scholar] [CrossRef]
- Venara, A.; Neunlist, M.; Slim, K.; Barbieux, J.; Colas, P.A.; Hamy, A.; Meurette, G. Postoperative ileus: Pathophysiology, incidence, and prevention. J. Visc. Surg. 2016, 153, 439–446. [Google Scholar] [CrossRef]
- Stakenborg, N.; Gomez-Pinilla, P.J.; Boeckxstaens, G.E. Postoperative Ileus: Pathophysiology, Current Therapeutic Approaches. Handb. Exp. Pharmacol. 2017, 239, 39–57. [Google Scholar] [CrossRef]
- Story, S.K.; Chamberlain, R.S. A Comprehensive Review of Evidence-Based Strategies to Prevent and Treat Postoperative Ileus. Dig. Surg. 2009, 26, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Fanning, J.; Hojat, R. Safety and efficacy of immediate postoperative feeding and bowel stimulation to prevent ileus after major gynecologic surgical procedures. J. Am. Osteopath Assoc. 2011, 111, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Glaser, G.; Dowdy, S.C.; Peedicayil, A. Enhanced recovery after surgery in gynecologic oncology. Int. J. Gynaecol. Obstet. 2018, 143 (Suppl. 2), 143–146. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Prognostic Factors | Favourable | Unfavourable |
|---|---|---|
| Patient’s age | <65 years | >65 years |
| Initial tumour stage | Early | Advanced |
| Surgery | Optimal surgical resection | Suboptimal surgical resection |
| Ca-125 levels at presentation | Low | High |
| Epithelial carcinoma histologic grade | Low | High |
| Myometrial vascular invasion | No | Yes |
| Epithelial components | Non-serous | Serous |
| Sarcomatous components | Homologous | Heterologous |
| Sarcomatous components outside the ovary | No | Yes |
| Presence of sarcomatous components | <25% | >25% |
| Histological stromal sarcoma predominance | No | Yes |
| Number of small vessels in the primary tumour | Low | High |
| VEGF, VEGFR-3 expression | Normal | Increased |
| P53 overexpression | Absent | Presented |
| Ki67 reactivity | Low | High |
| Adjuvant chemotherapy | Platinum-based regimens | Non-platinum-based regimes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostov, S.; Kornovski, Y.; Ivanova, Y.; Dzhenkov, D.; Stoyanov, G.; Stoilov, S.; Slavchev, S.; Trendafilova, E.; Yordanov, A. Ovarian Carcinosarcoma with Retroperitoneal Para-Aortic Lymph Node Dissemination Followed by an Unusual Postoperative Complication: A Case Report with a Brief Literature Review. Diagnostics 2020, 10, 1073. https://doi.org/10.3390/diagnostics10121073
Kostov S, Kornovski Y, Ivanova Y, Dzhenkov D, Stoyanov G, Stoilov S, Slavchev S, Trendafilova E, Yordanov A. Ovarian Carcinosarcoma with Retroperitoneal Para-Aortic Lymph Node Dissemination Followed by an Unusual Postoperative Complication: A Case Report with a Brief Literature Review. Diagnostics. 2020; 10(12):1073. https://doi.org/10.3390/diagnostics10121073
Chicago/Turabian StyleKostov, Stoyan, Yavor Kornovski, Yonka Ivanova, Deyan Dzhenkov, George Stoyanov, Stanislav Stoilov, Stanislav Slavchev, Ekaterina Trendafilova, and Angel Yordanov. 2020. "Ovarian Carcinosarcoma with Retroperitoneal Para-Aortic Lymph Node Dissemination Followed by an Unusual Postoperative Complication: A Case Report with a Brief Literature Review" Diagnostics 10, no. 12: 1073. https://doi.org/10.3390/diagnostics10121073
APA StyleKostov, S., Kornovski, Y., Ivanova, Y., Dzhenkov, D., Stoyanov, G., Stoilov, S., Slavchev, S., Trendafilova, E., & Yordanov, A. (2020). Ovarian Carcinosarcoma with Retroperitoneal Para-Aortic Lymph Node Dissemination Followed by an Unusual Postoperative Complication: A Case Report with a Brief Literature Review. Diagnostics, 10(12), 1073. https://doi.org/10.3390/diagnostics10121073