
A Comparative Study: Cardioprotective Effects of High-Intensity Interval Training Versus Ischaemic Preconditioning in Rat Myocardial Ischaemia–Reperfusion

Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Approval
2.2. Animal Preparation
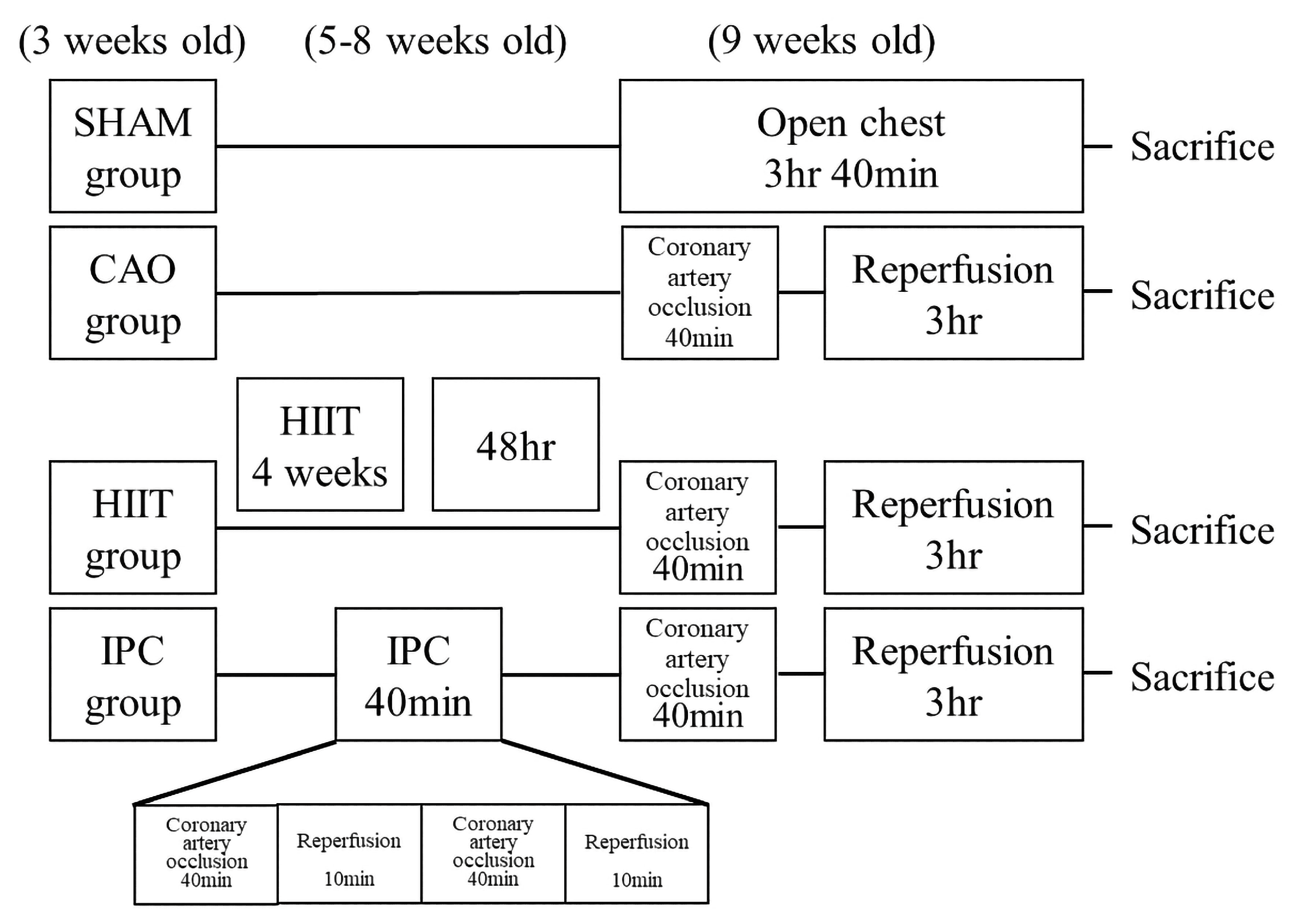
2.3. Experimental Protocol
2.4. Biochemical Analysis of the Cardiac Function
2.5. Histological Examination of Cardiac Injury
2.6. Determination of Area at Risk and MI Size
2.7. Terminal Deoxynucleotidyl Transferase dUTP Nick End Labeling Analysis of the Hearts of Rats
2.8. Calculation of Serum Levels of TNF-α, IL-1β, IL-6, and IL-10
2.9. Western Blot Analysis of PTEN, Bax-to-Bcl-2 Ratio, TNF-α, Cleaved-Caspase-3-to-Proactive-Caspase-3 Ratio in the Heart
2.10. Statistical Analysis
3. Results
3.1. Heart Tissue and Serum Analysis
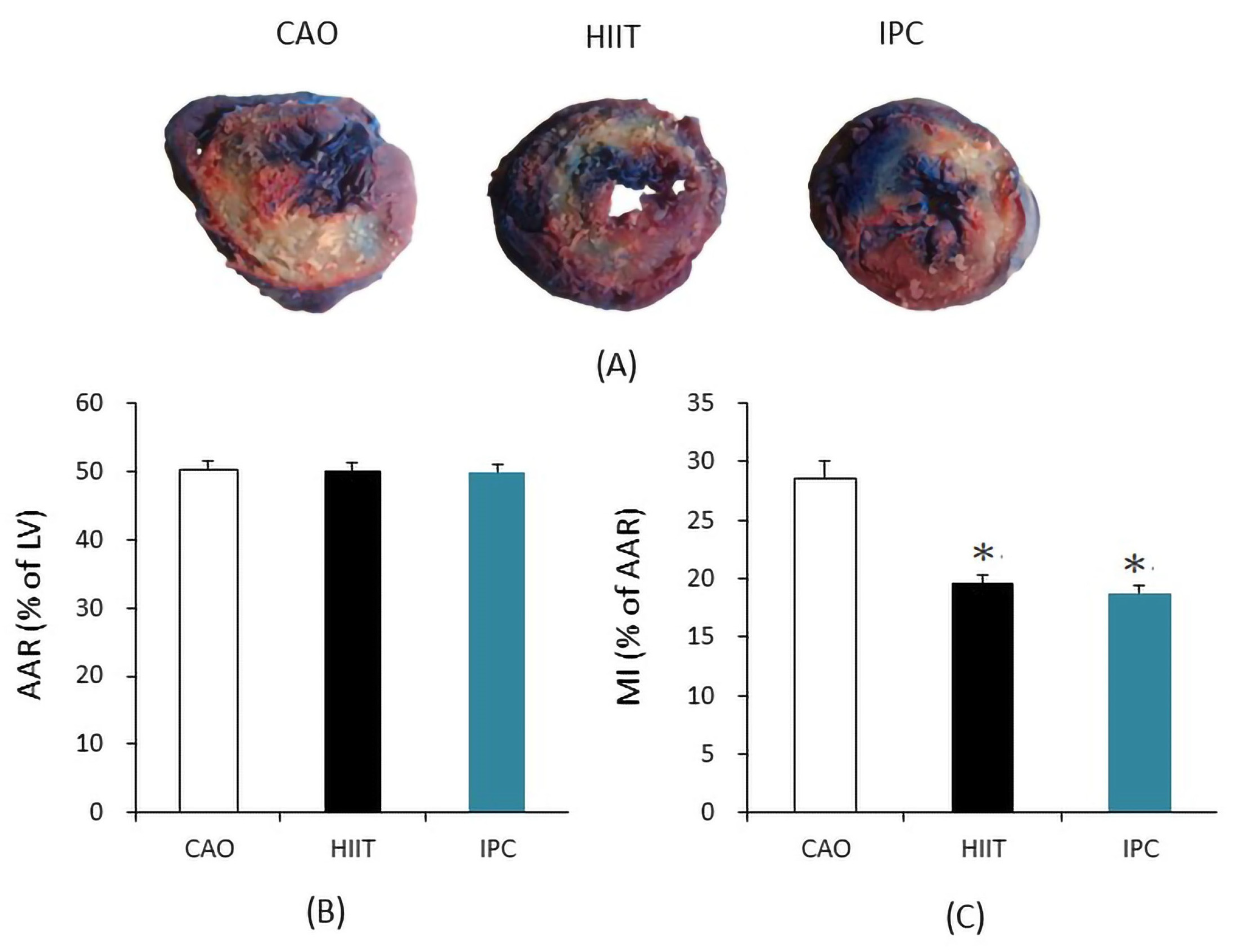
3.1.1. AAR and MI Size Analysis
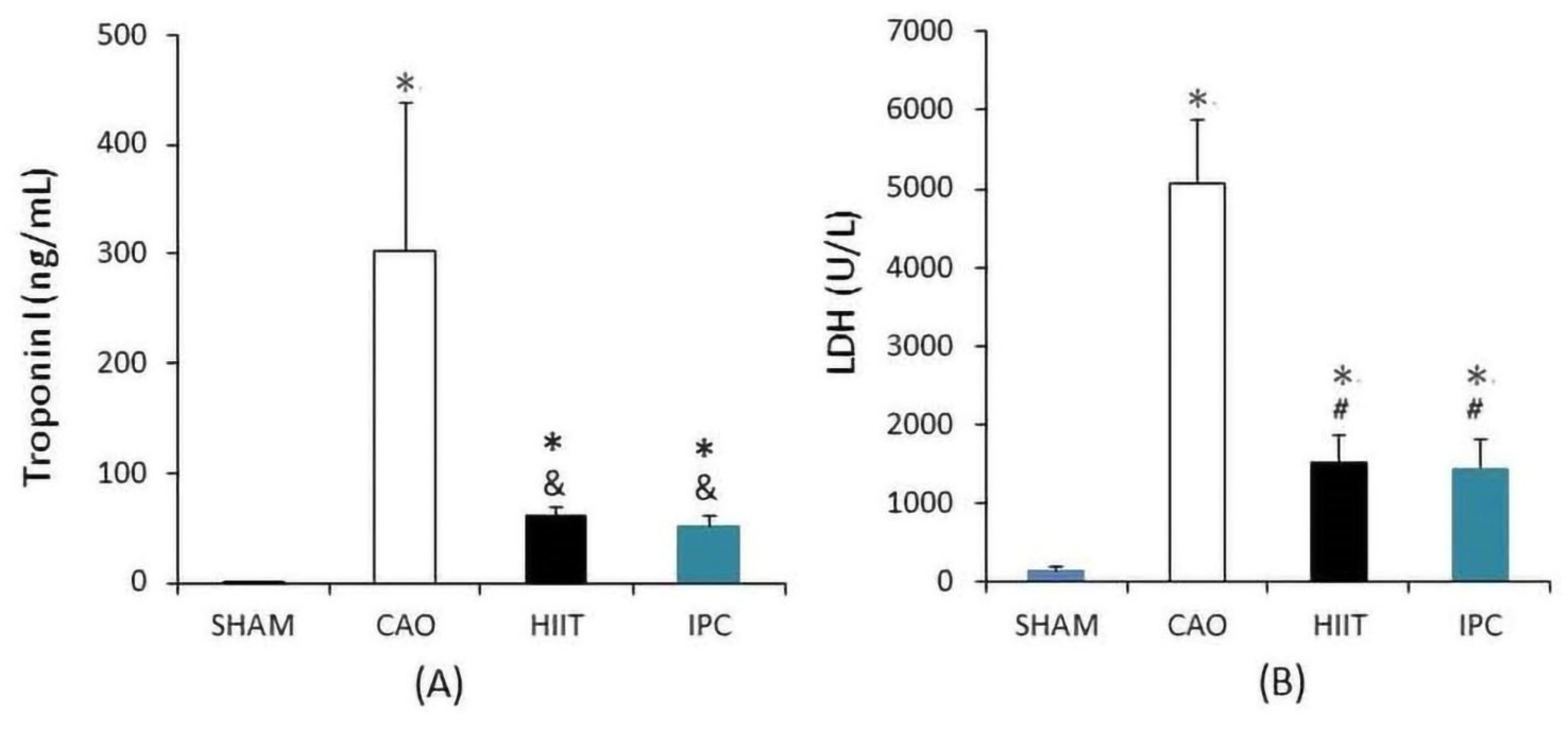
3.1.2. Biochemical Analysis of Cardiac Function
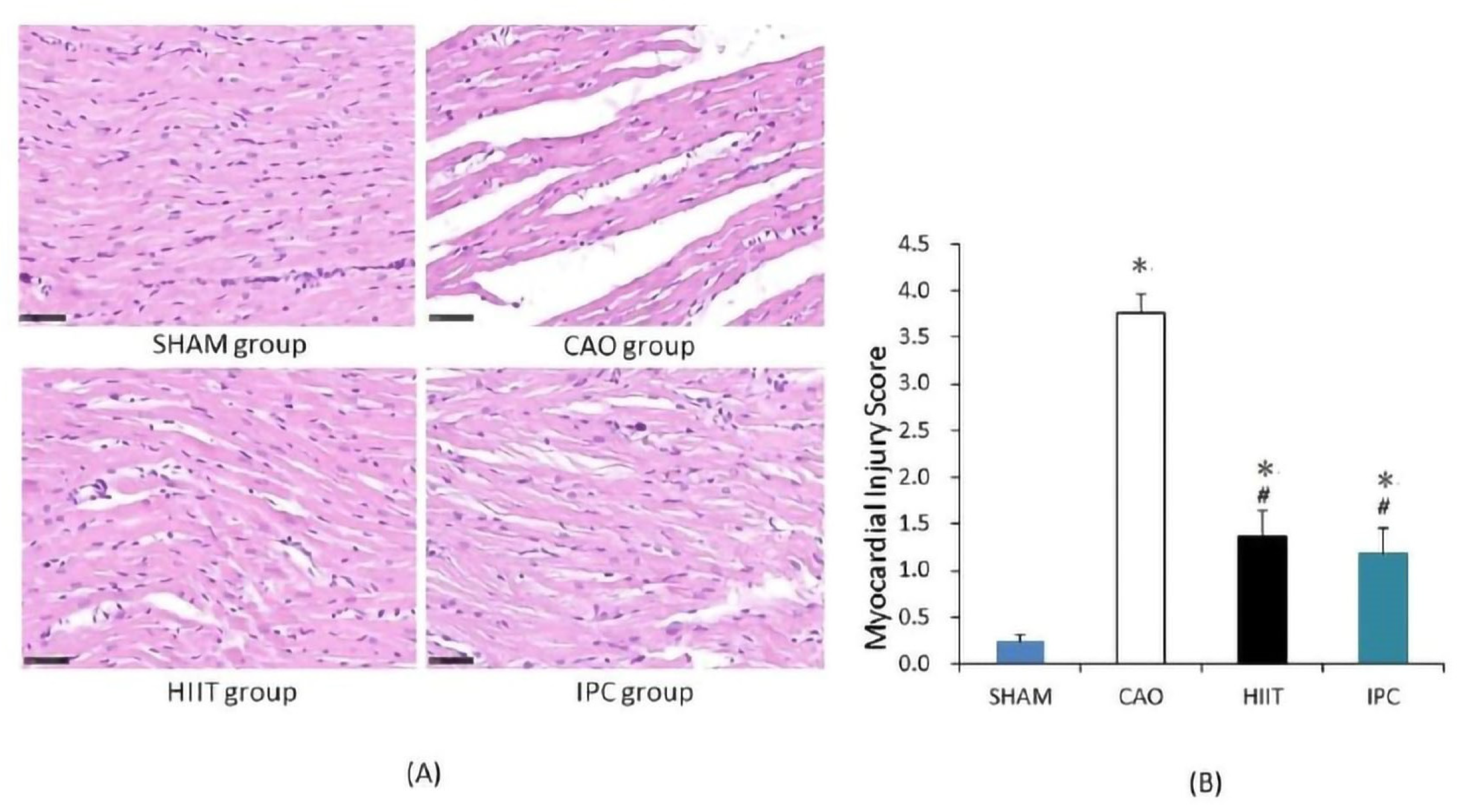
3.1.3. Histological Examination of Cardiac Injury
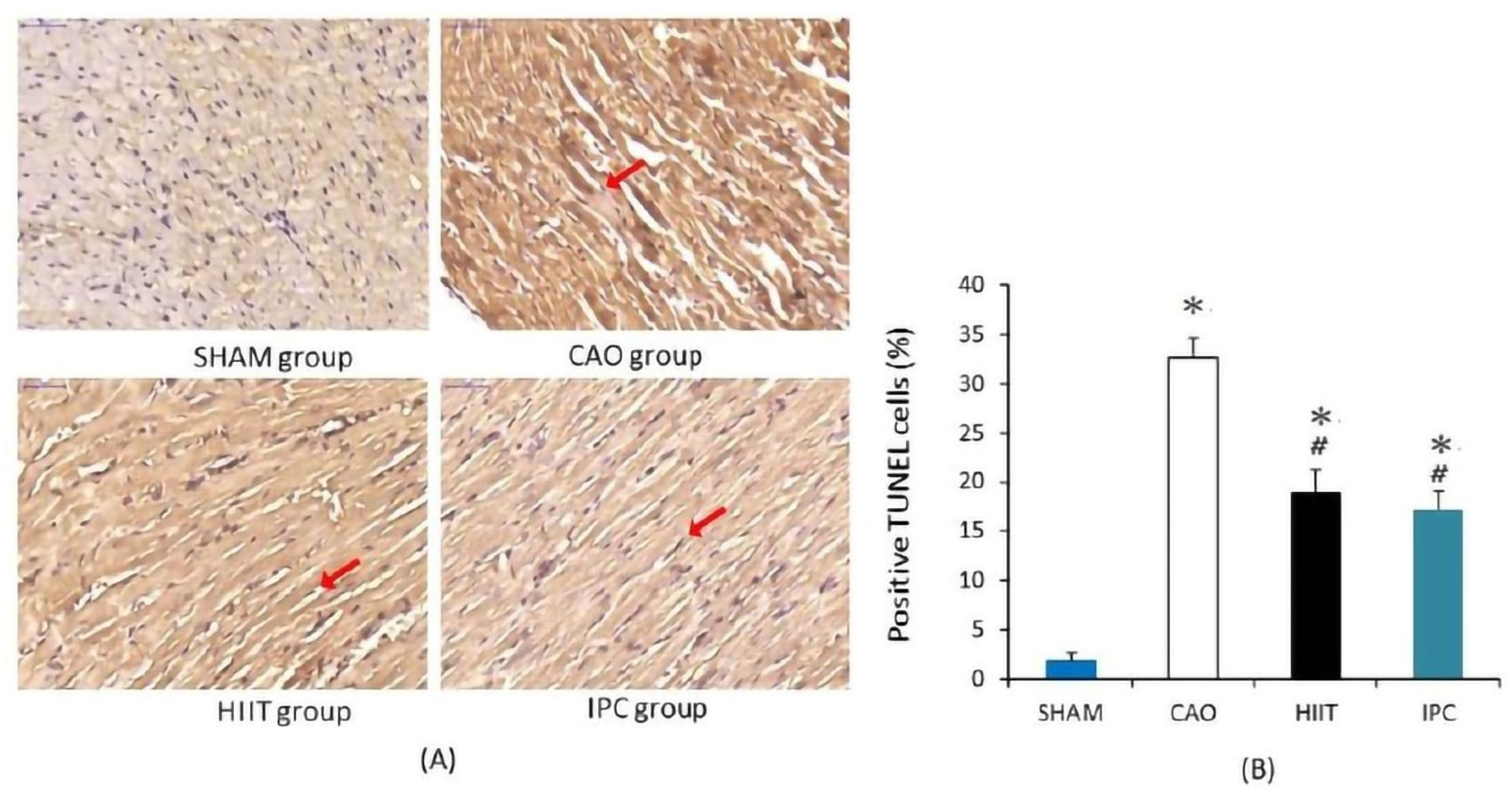
3.1.4. TUNEL Staining of Hearts
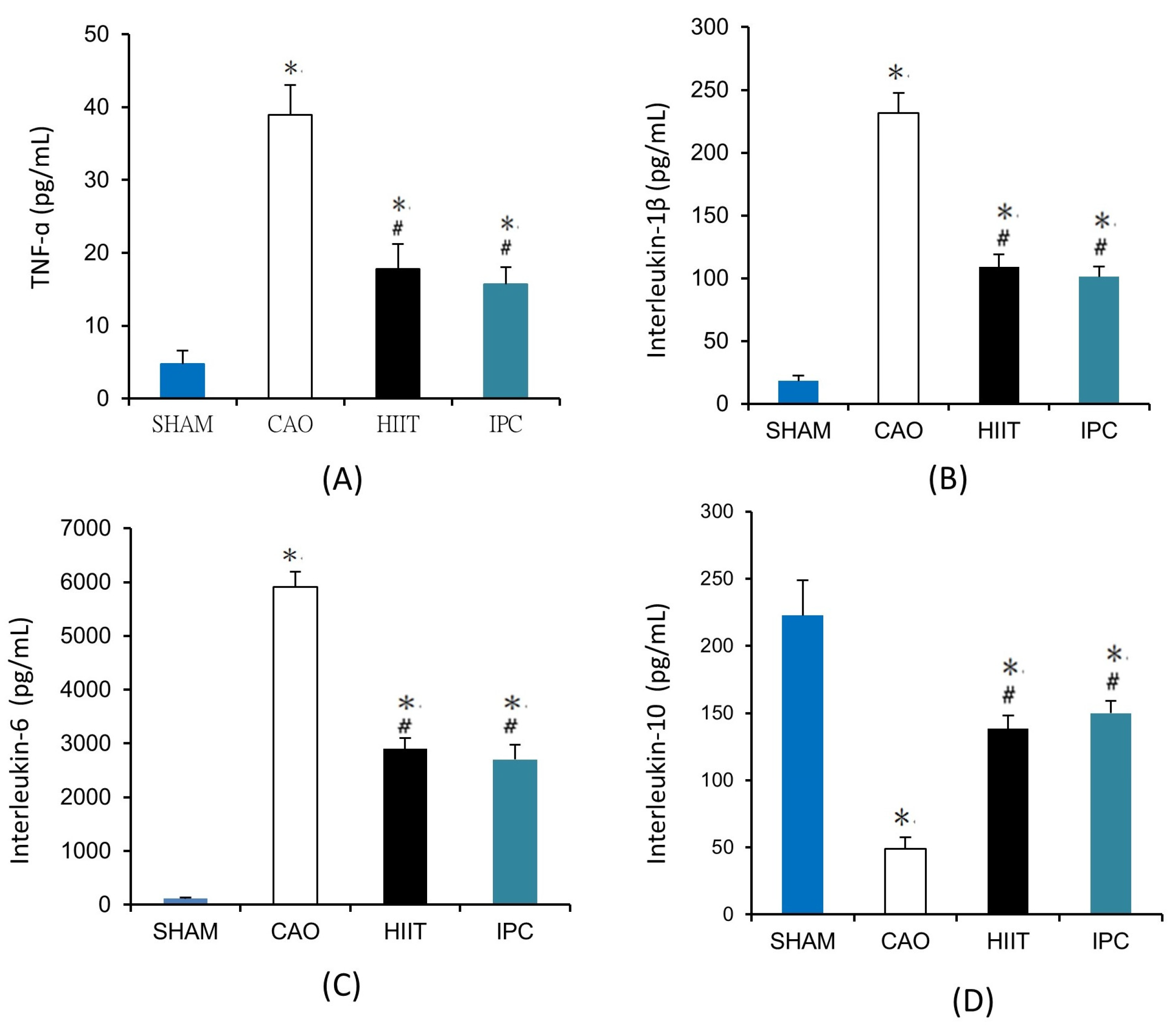
3.1.5. Determination of Serum Levels of TNF-α, IL-1β, IL-6, and IL-10
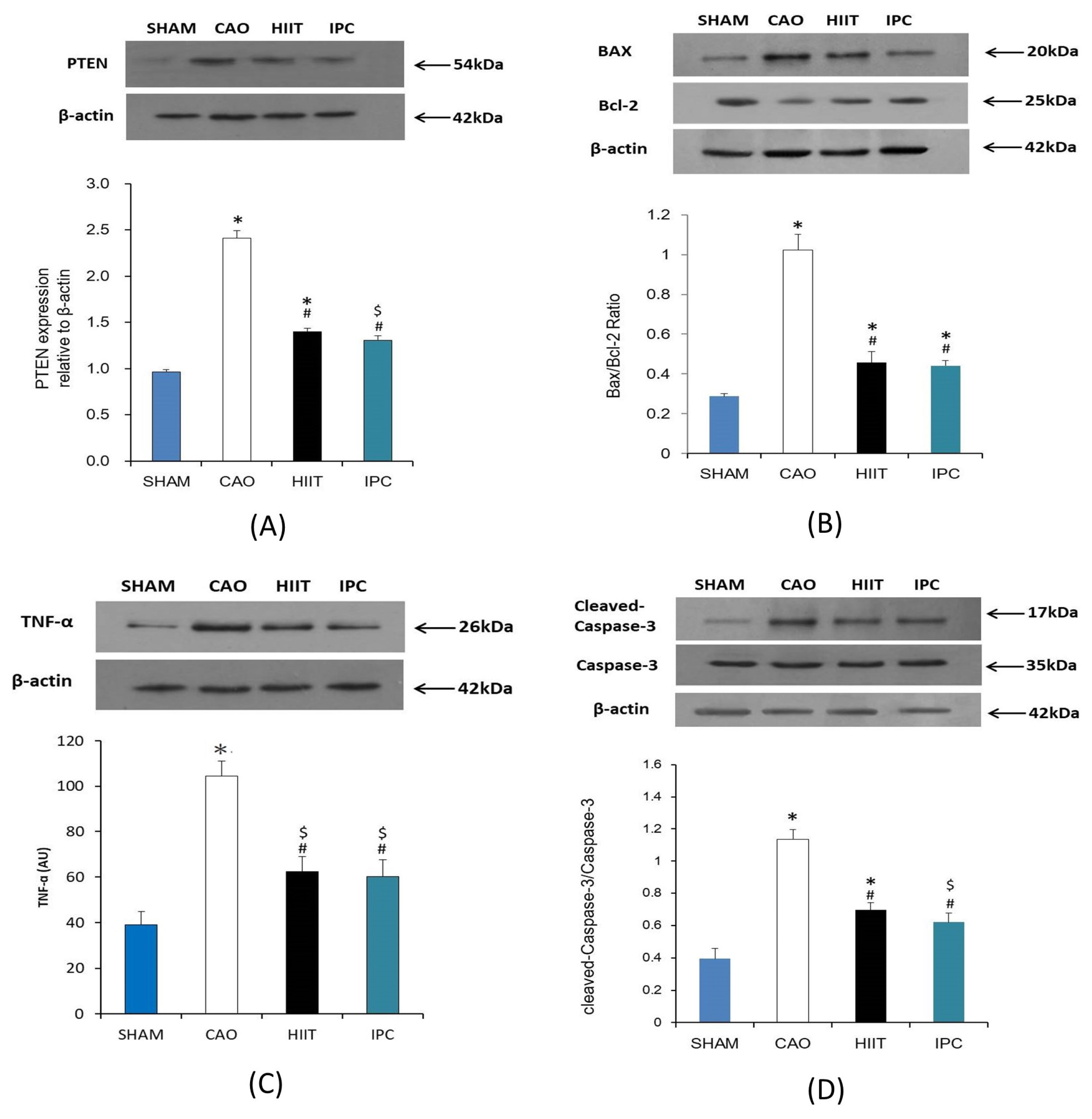
3.1.6. Assay of PTEN, Bax-to-Bcl-2 Ratio, TNF-α, and Cleaved-Caspase-3-to-Proactive Caspase-3 Ratio in the Heart
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Baseline | CAO | CAR | ||||
|---|---|---|---|---|---|---|---|
| 20 min | 40 min | 1 h | 2 h | 3 h | |||
| Mean arterial pressure, mmHg | |||||||
| 1 | SHAM | 80 ± 3 | 79 ± 9 | 79 ± 3 | 81 ± 8 | 82 ± 4 | 81 ± 3 |
| 2 | CAO | 83 ± 8 | 75 ± 4 | 74 ± 4 | 75 ± 6 | 78 ± 5 | 80 ± 4 |
| 3 | HIIT | 81 ± 6 | 77 ± 7 | 75 ± 5 | 76 ± 4 | 78 ± 7 | 82 ± 5 |
| 4 | IPC | 82 ± 4 | 78 ± 5 | 76 ± 2 | 76 ± 3 | 79 ± 2 | 83 ± 6 |
| Heart rate, beats/min | |||||||
| 1 | SHAM | 431 ± 27 | 427 ± 22 | 431 ± 33 | 435 ± 31 | 440 ± 19 | 438 ± 21 |
| 2 | CAO | 437 ± 29 | 460 ± 28 | 456 ± 27 | 451 ± 19 | 448 ± 26 | 450 ± 18 |
| 3 | HIIT | 451 ± 18 | 453 ± 31 | 440 ± 24 | 446 ± 23 | 446 ± 37 | 449 ± 33 |
| 4 | IPC | 442 ± 30 | 454 ± 39 | 455 ± 17 | 452 ± 18 | 451 ± 40 | 452 ± 26 |
| Mean arterial pressure-heart rate product/1000, mmHg×eats/min | |||||||
| 1 | SHAM | 35.26 ± 2.17 | 35.26 ± 1.94 | 34.40 ± 2.38 | 34.18 ± 2.01 | 34.47 ± 1.38 | 35.01 ± 2.03 |
| 2 | CAO | 38.67 ± 1.72 | 37.35 ± 1.29 | 36.04 ± 1.88 | 37.75 ± 2.11 | 37.82 ± 1.84 | 38.28 ± 2.35 |
| 3 | HIIT | 36.48 ± 2.38 | 34.85 ± 1.24 | 34.58 ± 1.22 | 35.46 ± 1.38 | 34.19 ± 2.11 | 35.21 ± 1.48 |
| 4 | IPC | 37.29 ± 1.21 | 35.37 ± 1.44 | 35.04 ± 2.50 | 36.00 ± 2.54 | 36.89 ± 1.68 | 37.08 ± 2.33 |
References
- Matter, M.A.; Paneni, F.; Libby, P.; Frantz, S.; Stähli, B.E.; Templin, C.; Matter, C.M. Inflammation in acute myocardial infarction: The good, the bad and the ugly. Eur. Heart J. 2024, 45, 89–103. [Google Scholar] [CrossRef]
- Shao, C.; Wang, J.; Tian, J.; Tang, Y.D. Coronary artery disease: From mechanism to clinical practice. Coron. Artery Dis. Ther. Drug Discov. 2020, 1177, 1–36. [Google Scholar]
- Liu, Y.; Yang, H.; Liu, L.X.; Yan, W.; Guo, H.J.; Li, W.J.; Tian, C.; Li, H.H.; Wang, H.X. NOD2 contributes to myocardial ischemia/reperfusion injury by regulating cardiomyocyte apoptosis and inflammation. Life Sci. 2016, 149, 10–17. [Google Scholar] [CrossRef]
- Zhao, Z.; Sun, W.; Guo, Z.; Liu, B.; Yu, H.; Zhang, J. Long noncoding RNAs in myocardial ischemia-reperfusion injury. Oxidative Med. Cell. Longev. 2021, 2021, 8889123. [Google Scholar] [CrossRef]
- Popgeorgiev, N.; Sa, J.D.; Jabbour, L.; Banjara, S.; Nguyen, T.T.M.; Akhavan-E-Sabet, A.; Gadet, R.; Ralchev, N.; Manon, S.; Hinds, M.G.; et al. Ancient and conserved functional interplay between Bcl-2 family proteins in the mitochondrial pathway of apoptosis. Sci. Adv. 2020, 6, eabc4149. [Google Scholar] [CrossRef]
- Chou, P.L.; Chen, K.H.; Chang, T.C.; Chien, C.T. Repetitively hypoxic preconditioning attenuates ischemia/reperfusion-induced liver dysfunction through upregulation of hypoxia-induced factor-1 alpha-dependent mitochondrial Bcl-xl in rat. Chin. J. Physiol. 2020, 63, 68. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; Ma, X.; Chen, H.; Jia, H.; Xiong, Y. Diazepam ameliorated myocardial ischemia-reperfusion injury via inhibition of CC chemokine receptor type 2/tumor necrosis factor-alpha/interleukins and Bcl-2-associated X protein/caspase-3 pathways in experimental rats. J. Vet. Med. Sci. 2021, 83, 1965–1976. [Google Scholar] [CrossRef] [PubMed]
- Tian, D.; Meng, J. Exercise for prevention and relief of cardiovascular disease: Prognoses, mechanisms, and approaches. Oxidative Med. Cell. Longev. 2019, 2019, 3756750. [Google Scholar] [CrossRef]
- Nomaguchi, K.M.; Bianchi, S.M. Exercise time: Gender differences in the effects of marriage, parenthood, and employment. J. Marriage Fam. 2004, 66, 413–430. [Google Scholar] [CrossRef]
- Norton, K.; Norton, L.; Sadgrove, D. Position statement on physical activity and exercise intensity terminology. J. Sci. Med. Sport 2010, 13, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Kessler, H.S.; Sisson, S.B.; Short, K.R. The potential for high-intensity interval training to reduce cardiometabolic disease risk. Sports Med. 2012, 42, 489–509. [Google Scholar] [CrossRef] [PubMed]
- Facioli, T.D.P.; Buranello, M.C.; Regueiro, E.M.G.; Basso-Vanelli, R.P.; Durand, M.D.T. Effect of physical training on nitric oxide levels in patients with arterial hypertension: An integrative review. Int. J. Cardiovasc. Sci. 2021, 35, 253–264. [Google Scholar] [CrossRef]
- Nebel, R.; Bjarnason-Wehrens, B. High Intensity Interval Training in Patients with CHD and Preserved Ventricular Function. Dtsch. Z. Für Sportmed. (Ger. J. Sports Med.) 2018, 69, 206–215. [Google Scholar]
- Naderi, N.; Hemmatinafar, M.; Gaeini, A.A.; Bahramian, A.; Ghardashi-Afousi, A.; Kordi, M.R.; Darbandi-Azar, A.; Karimzade, F.; Mohebbi, H.; Barati, M. High-intensity interval training increases GATA4, CITED4 and c-Kit and decreases C/EBPβ in rats after myocardial infarction. Life Sci. 2019, 221, 319–326. [Google Scholar] [CrossRef]
- Zheng, J.; Cheng, J.; Zheng, S.; Zhang, L.; Guo, X.; Zhang, J.; Xiao, X. Physical exercise and its protective effects on diabetic cardiomyopathy: What is the evidence? Front. Endocrinol. 2018, 9, 729. [Google Scholar] [CrossRef]
- Ishida, T.; Yarimizu, K.; Gute, D.C.; Korthuis, R.J. Mechanisms of ischemic preconditioning. Shock 1997, 8, 86–94. [Google Scholar] [CrossRef]
- Zhao, Z.Q.; Vinten-Johansen, J. Myocardial apoptosis and ischemic preconditioning. Cardiovasc. Res. 2002, 55, 438–455. [Google Scholar] [CrossRef]
- Nystoriak, M.A.; Bhatnagar, A. Cardiovascular effects and benefits of exercise. Front. Cardiovasc. Med. 2018, 5, 135. [Google Scholar] [CrossRef] [PubMed]
- Hausenloy, D.J.; Yellon, D.M. Ischaemic conditioning and reperfusion injury. Nat. Rev. Cardiol. 2016, 4, 193–209. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.D.; Gebhart, G.F.; Gonder, J.C.; Keeling, M.E.; Kohn, D.F. The 1996 guide for the care and use of laboratory animals. ILAR J. 1997, 38, 41–48. [Google Scholar] [CrossRef]
- Tucker, P.S.; Briskey, D.R.; Scanlan, A.T.; Coombes, J.S.; Dalbo, V.J. High intensity interval training favourably affects antioxidant and inflammation mRNA expression in early-stage chronic kidney disease. Free. Radic. Biol. Med. 2015, 89, TSP466–TSP472. [Google Scholar] [CrossRef]
- Lee, H.W.; Han, T.H.; Yi, K.J.; Choi, M.C.; Lee, S.Y.; Ryu, P.D. Time course of diurnal rhythm disturbances in autonomic function of rats with myocardial infarction. Auton. Neurosci. Basic Clin. 2013, 179, 28–36. [Google Scholar] [CrossRef]
- Thornberry, N.A.; Lazebnik, Y. Caspases: Enemies within. Science 1998, 281, 1312–1316. [Google Scholar] [CrossRef]
- El-Shitany, N.A.; Tolba, O.A.; El-Shanshory, M.R.; El-Hawary, E.E. Protective effect of carvedilol on adriamycin-induced left ventricular dysfunction in children with acute lymphoblastic leukemia. J. Card. Fail. 2012, 18, 607–613. [Google Scholar] [CrossRef]
- Marini, M.; Lapalombella, R.; Margonato, V.; Ronchi, R.; Samaja, M.; Scapin, C.; Veicsteinas, A. Mild exercise training, cardioprotection and stress genes profile. Eur. J. Appl. Physiol. 2007, 99, 503–510. [Google Scholar] [CrossRef]
- Rahimi, M.; Shekarforoush, S.; Asgari, A.R.; Khoshbaten, A.; Rajabi, H.; Bazgir, B.; Mohammadi, M.T.; Sobhani, V.; Shakibaee, A. The effect of high intensity interval training on cardioprotection against ischemia-reperfusion injury in Wistar rats. EXCLI J. 2015, 14, 237. [Google Scholar]
- Ramez, M.; Rajabi, H.; Ramezani, F.; Naderi, N.; Darbandi-Azar, A.; Nasirinezhad, F. The greater effect of high-intensity interval training versus moderate-intensity continuous training on cardioprotection against ischemia-reperfusion injury through Klotho levels and attenuate of myocardial TRPC6 expression. BMC Cardiovasc. Disord. 2019, 19, 118. [Google Scholar] [CrossRef]
- Rankovic, M.; Jakovljevic, V.; Bradic, J.; Jakovljevic, B.; Zivkovic, V.; Srejovic, I.; Bolevich, S.; Milosavljevic, I.; Jeremic, J.; Ravic, M.; et al. Effects of high intensity interval vs. endurance training on cardiac parameters in ischemia/reperfusion of male rats: Focus on oxidative stress. Front. Physiol. 2021, 12, 534127. [Google Scholar] [CrossRef]
- Abdel-Aty, H.; Cocker, M.; Meek, C.; Tyberg, J.V.; Friedrich, M.G. Edema as a very early marker for acute myocardial ischemia: A cardiovascular magnetic resonance study. J. Am. Coll. Cardiol. 2009, 53, 1194–1201. [Google Scholar] [CrossRef] [PubMed]
- Valaei, K.; Taherkhani, S.; Arazi, H.; Suzuki, K. Cardiac oxidative stress and the therapeutic approaches to the intake of antioxidant supplements and physical activity. Nutrients 2021, 13, 3483. [Google Scholar] [CrossRef] [PubMed]
- Akki, R.; Siracusa, R.; Cordaro, M.; Remigante, A.; Morabito, R.; Errami, M.; Marino, A. Adaptation to oxidative stress at cellular and tissue level. Arch. Physiol. Biochem. 2022, 128, 521–531. [Google Scholar] [CrossRef]
- Quindry, J.C.; Miller, L.; McGinnis, G.; Kliszczewicz, B.; Irwin, J.M.; Landram, M.; Urbiztondo, Z.; Nanayakkara, G.; Amin, R. Ischemia reperfusion injury, KATP channels, and exercise-induced cardioprotection against apoptosis. J. Appl. Physiol. 2012, 113, 498–506. [Google Scholar] [CrossRef]
- Honda, H.M.; Korge, P.; Weiss, J.N. Mitochondria and ischemia/reperfusion injury. Ann. N. Y. Acad. Sci. 2005, 1047, 248–258. [Google Scholar] [CrossRef] [PubMed]
- Garlid, K.D.; Dos Santos, P.; Xie, Z.J.; Costa, A.D.; Paucek, P. Mitochondrial potassium transport: The role of the mitochondrial ATP-sensitive K+ channel in cardiac function and cardioprotection. Biochim. Biophys. Acta-Bioenerg. 2003, 1606, 1–21. [Google Scholar] [CrossRef]
- Cheng-hsien, C.; Tieh-cheng, F.; Hsing-hua, T. High-intensity interval training enhances mitochondrial bioenergetics of platelets in patients with heart failure. Int. J. Cardiol. 2018, 274, 214–220. [Google Scholar]
- Wang, B.; Zhou, R.; Wang, Y.; Liu, X.; Shou, X.; Yang, Y.; Yang, C.; Tong, Q.; Mao, G.; Wu, Q. Effect of high-intensity interval training on cardiac structure and function in rats with acute myocardial infarct. Biomed. Pharmacother. 2020, 131, 110690. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.Y.; Zhu, S.; Wu, J.; Zhang, M.; Xu, Y.; Xu, W.; Cui, J.; Yu, B.; Cao, W.; Liu, J. Exercise enhances cardiac function by improving mitochondrial dysfunction and maintaining energy homeostasis in the development of diabetic cardiomyopathy. J. Mol. Med. 2020, 98, 245–261. [Google Scholar] [CrossRef]
- Ramez, M.; Ramezani, F.; Nasirinezhad, F.; Rajabi, H. High-intensity interval training increases myocardial levels of Klotho and protects the heart against ischaemia–reperfusion injury. Exp. Physiol. 2020, 105, 652–665. [Google Scholar] [CrossRef]
- Marino, A.; Hausenloy, D.J.; Andreadou, I.; Horman, S.; Bertrand, L.; Beauloye, C. AMP-activated protein kinase: A remarkable contributor to preserve a healthy heart against ROS injury. Free. Radic. Biol. Med. 2021, 166, 238–254. [Google Scholar] [CrossRef]
- Thirupathi, A.; De Souza, C.T. Multi-regulatory network of ROS: The interconnection of ROS, PGC-1 alpha, and AMPK-SIRT1 during exercise. J. Physiol. Biochem. 2017, 73, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Lira, V.A.; Benton, C.R.; Yan, Z.; Bonen, A. PGC-1α regulation by exercise training and its influences on muscle function and insulin sensitivity. Am. J. Physiol.-Endocrinol. Metab. 2010, 299, E145–E161. [Google Scholar] [CrossRef]
- Nazarali, P. Effect of high-intensity interval training (HIIT) on vascular endothelial growth factor (VEGF) in heart muscle in healthy rats. 2015. [Google Scholar]
- Banaei, P.; Nazem, F.; Nazari, A.; Arjomand, A. Preconditioning effect of high-intensity interval training (HIIT) and berberine supplementation on the gene expression of angiogenesis regulators and caspase-3 protein in the rats with myocardial ischemia-reperfusion (IR) injury. Biomed. Res. Int. 2020, 2020, 4104965. [Google Scholar] [CrossRef]
- Wu, L.; Xiong, X.; Wu, X.; Ye, Y.; Jian, Z.; Zhi, Z.; Gu, L. Targeting oxidative stress and inflammation to prevent ischemia-reperfusion injury. Front. Mol. Neurosci. 2020, 13, 28. [Google Scholar] [CrossRef]
- Khalifa, A.A.; Rashad, R.M.; El-Hadidy, W.F. Thymoquinone protects against cardiac mitochondrial DNA loss, oxidative stress, inflammation and apoptosis in isoproterenol-induced myocardial infarction in rats. Heliyon 2021, 7, e07561. [Google Scholar] [CrossRef]
- Zhao, Z.Q.; Budde, J.M.; Morris, C.; Wang, N.P.; Velez, D.A.; Muraki, S.; Guyton, R.A.; Vinten-Johansen, J. Adenosine attenuates reperfusion-induced apoptotic cell death by modulating expression of Bcl-2 and Bax proteins. J. Mol. Cell. Cardiol. 2001, 33, 57–68. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, X. Ischaemic preconditioning-induced serum exosomes protect against myocardial ischaemia/reperfusion injury in rats by activating the PI3K/AKT signalling pathway. Cell Biochem. Funct. 2021, 39, 287–295. [Google Scholar] [CrossRef]
- Chen, L.; Shi, D.; Guo, M. The roles of PKC-δ and PKC-ε in myocardial ischemia/reperfusion injury. Pharmacol. Res. 2021, 170, 105716. [Google Scholar] [CrossRef]
- Lu, K.; Wang, L.; Wang, C.; Yang, Y.; Hu, D.; Ding, R. Effects of high-intensity interval versus continuous moderate intensity aerobic exercise on apoptosis, oxidative stress and metabolism of the infarcted myocardium in a rat model. Mol. Med. Rep. 2015, 12, 2374–2382. [Google Scholar] [CrossRef]
- Yamamoto, M.; Morita, T.; Ishikawa, M.; Sakamoto, A. Specific microRNAs are involved in the renoprotective effects of sevoflurane preconditioning and ischemic preconditioning against ischemia-reperfusion injury in rats. Int. J. Mol. Med. 2020, 45, 1141–1149. [Google Scholar]
- Bei, Y.; Lu, D.; Bär, C.; Chatterjee, S.; Costa, A.; Riedel, I.; Mooren, F.C.; Zhu, Y.; Huang, Z.; Wei, M. miR-486 attenuates cardiac ischemia/reperfusion injury and mediates the beneficial effect of exercise for myocardial protection. Mol. Ther. 2022, 30, 1675–1691. [Google Scholar] [CrossRef]


| Rat Age | Wk3 | Wk4 | Wk5 | Wk6 | Wk7 | Wk8 | ||
|---|---|---|---|---|---|---|---|---|
| Variable/Measure | ||||||||
| Max. speed | meters/min | 20 | 30 | 50 | 50 | 50 | 50 | |
| Incline | degrees | 5 | 10 | 10 | 10 | 10 | 10 | |
| Duration | minutes | 30 | 30 | 30 | 30 | 30 | 30 | |
| Intensity | 2 min stationary period followed by 1 min sprint period × 10 reps | |||||||
| Frequency | bouts/wk | 4 | 4 | 4 | 4 | 4 | 4 | |
| Distance per bout | meters | 200 | 300 | 500 | 500 | 500 | 500 | |
| Distance per week | meters | 800 | 1200 | 2000 | 2000 | 2000 | 2000 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.-Y.; Fu, S.-K.; Tai, H.-L.; Tseng, K.-W.; Tang, C.-Y.; Yu, C.-H.; Lai, C.-C. A Comparative Study: Cardioprotective Effects of High-Intensity Interval Training Versus Ischaemic Preconditioning in Rat Myocardial Ischaemia–Reperfusion. Life 2024, 14, 310. https://doi.org/10.3390/life14030310
Zhang J-Y, Fu S-K, Tai H-L, Tseng K-W, Tang C-Y, Yu C-H, Lai C-C. A Comparative Study: Cardioprotective Effects of High-Intensity Interval Training Versus Ischaemic Preconditioning in Rat Myocardial Ischaemia–Reperfusion. Life. 2024; 14(3):310. https://doi.org/10.3390/life14030310
Chicago/Turabian StyleZhang, Jia-Yuan, Szu-Kai Fu, Hsia-Ling Tai, Kuo-Wei Tseng, Chia-Yu Tang, Chia-Hsien Yu, and Chang-Chi Lai. 2024. "A Comparative Study: Cardioprotective Effects of High-Intensity Interval Training Versus Ischaemic Preconditioning in Rat Myocardial Ischaemia–Reperfusion" Life 14, no. 3: 310. https://doi.org/10.3390/life14030310
APA StyleZhang, J.-Y., Fu, S.-K., Tai, H.-L., Tseng, K.-W., Tang, C.-Y., Yu, C.-H., & Lai, C.-C. (2024). A Comparative Study: Cardioprotective Effects of High-Intensity Interval Training Versus Ischaemic Preconditioning in Rat Myocardial Ischaemia–Reperfusion. Life, 14(3), 310. https://doi.org/10.3390/life14030310