


Sharing Circulating Micro-RNAs between Osteoporosis and Sarcopenia: A Systematic Review
 , , ,
, , ,  ,
,  , ,
, , 

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategies
2.3. Selection Process
2.4. Data Collection Process and Synthesis Methods
2.5. Risk of Bias Assessment

{kind=link}
{kind=link}
{kind=link}
| Ref. | Country of Publication | Study Design | Patients Number | Ethnicity | Sex/Age | Comorbidities | Osteoporosis Diagnostic Measures |
|---|---|---|---|---|---|---|---|
| Al-Rawaf 2021 [26] | Saudi Arabia | Prospective | 100 Osteoporotic (N = 55) Healthy controls (N = 45) | NR | Female 50–80 years | None | DXA |
| Baloun 2022 [27] | Czechia | Prospective | 22 After oophorectomy and hysterectomy (N = 11) Before oophorectomy and hysterectomy (N = 11) | NR | Female | NR | DXA |
| Bedene 2016 [28] | Slovenia | NR | 74 Osteoporotic (N = 17) Healthy controls (N = 57) | NR | Female | NR | DXA FRAX |
| Chen 2016 [29] | China | NR | NR | Patients from Peking Union Medical College Hospital | Female | None | DXA |
| Chen 2017 [30] | China | NR | 60 Osteoporotic (N = 30) Healthy controls (N = 30) | Chinese women | Female Osteoporotic: 59–80 years Non-osteoporotic: 62–74 years | None | NR |
| Chen 2019 [31] | China | NR | 84 Osteoporotic (N = 42) Healthy controls (N = 42) | NR | Female | NR | NR |
| Chen 2019 b [32] | USA | NR | 75 Osteoporotic/osteopenic (N = 46) Sarcopenic (N = 1) Sarco-osteopenic (N = 15) Non-osteoporotic/non-sarcopenic (N = 13) | NR | Female 60–85 years | None | DXA |
| Cheng 2019 [33] | China | NR | 60 Osteoporotic (N = 30) Healthy controls (N = 30) | NR | Female | NR | NR |
| Ciuffi 2022 [34] | Italy | Prospective multicenter study | 213 Osteoporotic (N = 105) Osteopenic (N = 62) Healthy controls (N = 46) | Female/male Osteoporotic 68.0 ± 4.9 years Osteoporotic with fragility fracture 68.6 ± 5.0 years Osteoporotic without fragility fracture 67.0 ± 4.5 years Osteopenic healthy controls 67.2 ± 5.0 years | NR | DXA | |
| Ding 2019 [35] | China | NR | 240 Osteoporotic (N = 120) Healthy controls (N = 120) | Chinese woman | Female | NR | NR |
| Feurer 2019 [36] | France | Prospective | 682 Post-menopausal women (N = 583) Pre-menopausal women (N = 99) | NR | Female | Stage 4 renal failure (n = 2), hyperthyroidism (n = 5), rheumatoid arthritis (n = 3), diabetes (n = 18), | DXA HRpQCT |
| Fu 2019 [37] | China | Prospective | 40 Osteoporotic (N = 20) Healthy controls (N = 20) | NR | Female | NR | NR |
| Fu 2021 [38] | China | Prospective | 161 Osteoporotic (N = 82) Healthy controls (N = 79) | NR | Female/male Osteoporotic (60 female, 22 male) 50.48 ± 3.5 years Healthy controls (58 female, 21 male) 49.68 ± 4.17 years | NR | DXA |
| Gao 2020 [39] | China | NR | NR | NR | NR | NR | NR |
| Guo 2022 [40] | China | NR | 40 Osteoporotic fractured patients (N = 20) Healthy controls (N = 20) | NR | Female Osteoporotic 59–80 years Healthy controls 62–75 | NR | NR |
| Ismail 2020 [41] | Egypt | Prospective pilot | 140 Osteoporotic (N = 70) Healthy controls (N = 70) | NR | Female Premenopausal (control: 34.03 ± 5.72 years and osteoporotic: 36.00 ± 7.15 years) Postmenopausal (control: 60.06 ± 6.57 and osteoporotic: 61.29 ± 7.69) | None | DXA |
| Li 2014 [42] | China | Prospective | 120 Osteoporotic (N = 40) Osteopenic (N = 40) Healthy controls (N = 40) | Chinese woman | Female Osteoporotic 57.5 ± 11.3 years Osteopenic 56.7 ± 10.7 Healthy controls 56.5 ± 10.5 | None | DXA |
| Li 2018 [43] | China | NR | 20 Osteoporotic (N = 10) Healthy controls (N = 10) | Chinese woman | Female Age range 62–75 years | None | DXA |
| Li 2020 [44] | China | NR | 72 Osteoporotic (N = 36) Healthy controls (N = 36) | NR | Female Osteoporotic 62 ± 3.98 years Healthy controls 59 ± 5.15 years | None | DXA |
| Lu 2021 [45] | China | NR | 120 Osteoporotic (N = 63) Healthy controls (N = 57) | NR | Female Osteoporotic 49.97 ± 4.20 years Healthy controls 50.58 ± 4.14 years | None | DXA |
| Luo 2019 [46] | China | NR | NR | NR | NR | NR | NR |
| Lv 2019 [47] | China | Prospective | 60 Osteoporotic (N = 30) Healthy controls (N = 30) | NR | NR | NR | NR |
| Ma 2021 [48] | China | Case-control | 100 Osteoporotic (N = 86) Healthy controls (N = 14) | NR | Female Osteopenic/osteoporotic 65.00 ± 8.51 years Healthy controls 39.07 ± 2.87 years | None | DXA |
| Ma 2022 [49] | China | Case-control | 158 Osteoporotic (N = 108; 58 with fragility fracture) Healthy controls (N = 50) | NR | Female Osteoporotic 64.82 ± 6.08 years Fragility fracture 63.72 ± 5.59 Healthy controls 64.26 ± 6.52 years | None | DXA |
| Mandourah 2018 [50] | United Kingdom | NR | Osteopenic without fracture (N = 63; F 53/M 10) Osteopenic with fracture (N = 15; F 13/M 2) Osteoporotic without fracture (N = 34; F 28/M6) Osteoporotic with fracture (N = 19; F 17/M 2) Healthy controls (N = 30; F 20/M 10) | NR | Female/male Osteopenic without fracture 65.6 ± 9.5 years Osteopenic with fracture 67 ± 9.5 years Osteoporotic without fracture 68.6 ± 10 years Osteoporotic with fracture 70 ± 10 years Healthy controls 67 ± 9.6 years | None | DXA |
| Mi 2020 [51] | China | NR | 100 Osteoporotic (N = 50) Healthy controls (N = 50) | NR | Age range 53–74 | NR | DXA |
| Nakashima 2020 [52] | Japan | Cross-sectional | 352 Osteoporotic (N = 125) Healthy controls (N = 227) | Yakumo population | Female/male 64.1 ± 9.6 years | NR | DXA |
| Nobrega 2020 [53] | Brazil | Cross-sectional | 40 | Brazilian very old adults | Female and male 84.2 ± 4.5 | Type-2 diabetes, hypertension, metabolic syndrome | DXA |
| Panach 2015 [54] | Spain | NR | 25 Osteoporotic fractured (N = 14) Healthy controls (N = 11) | Caucasian women | Female Osteoporotic with fracture 79.6 ± 3.1 years Controls 63.4 ± 8.1 years | NR | DXA |
| Pertusa 2021 [55] | Spain | NR | 77 Osteoporotic fractured (N = 25) Healthy controls (N = 52) | Caucasian women | Female Osteoporotic with fracture 79.6 ± 3.1 years Controls 76.8 ± 8.3 years | None | DXA |
| Qiao 2019 [56] | China | NR | 100 Osteoporotic (N = 60) Healthy controls (N = 40) | NR | Female Osteoporotic 63.4 ± 2.4 years Healthy controls 59.3 ± 3.2 years | NR | DXA |
| Ramírez-Salazar 2019 [57] | Mexico | NR | 87 Osteoporotic with fracture (N = 21) Osteoporotic without fracture (N = 16) Osteopenic (N = 28) Healthy controls (N = 22) | Mexican-Mestizo women | Female Osteoporotic 73.75 ± 4.46 years Healthy controls 71.1 ± 3.72 years | None | DXA |
| Salman 2021 [58] | Iraq | NR | 95 Osteoporotic (N = 50) Healthy controls (N = 45) | NR | Female/male Osteoporotic 72.5 ± 9.45 years Healthy controls 71.4 ± 8.33 years | None | Physician diagnosis |
| Seeliger 2014 [59] | Germany | NR | 60 Osteoporotic (N = 30) Healthy controls (N = 30) | NR | Female/male Osteoporotic 78.3 years Healthy controls 76.6 years | None | DXA, X-ray, qCT |
| Shuai 2020 [60] | China | Case-control | 448 Osteopenia (N = 132) Osteoporotic (N = 134) Healthy controls (N = 182) | Northwest China | Female/male Osteopenia 49.0 years Osteoporosis 61.1 years Healthy controls 42.3 years | None | DXA |
| Sun 2020a [61] | China | NR | 18 Osteoporotic with fracture (N = 6) Osteoporotic without fracture (N = 6) Healthy controls (N = 6) | NR | Female/male Osteoporotic without fracture 68.0 years Osteoporotic with fracture 69.7 years Healthy controls 47.8 years | None | DXA |
| Sun 2020b [62] | China | NR | 81 Osteoporotic (N = 41) Healthy controls (N = 40) | NR | Female/male Osteoporotic with fracture 44 years | None | NR |
| Tang 2019 [63] | China | NR | 30 Osteoporotic (N = 15) Healthy controls (N = 15) | NR | Female Age range 54–64 | NR | NR |
| Wang 2018 [64] | China | NR | 60 Osteoporotic (N = 45) Healthy controls (N = 15) | NR | NR | NR | NR |
| Weilner 2015 [65] | Austria | NR | 23 Osteoporotic fractured (N = 12) Healthy controls (N = 11) | White Caucasian | Female age ≥ 65 years | Type-2 diabetes | DXA |
| Wu 2021 [66] | China | NR | 20 Osteoporotic (N = 10; 6 females and 4 males) Healthy controls (N = 10; 5 females and 5 males) | NR | Female and male Osteoporotic Range 56–73 years Healthy controls Range 57–72 years | None | DXA |
| Xia 2018 [67] | China | NR | 120 Osteoporotic (N = 60) Healthy controls (N = 60) | NR | Female | NR | qCT |
| Xu 2022 [68] | China | Retrospective | 160 Osteoporotic patients with vertebral fractures (N = 78) Osteoporotic patients without vertebral fractures (N = 82) | NR | Osteoporotic patients with vertebral fractures 67.90 ± 7.04 years Osteoporotic patients without vertebral fractures 66.84 ± 6.58 years | None | DXA |
| Yang 2019 [69] | China | NR | 30 Osteoporotic (N = 15) Healthy controls (N = 15) | NR | NR | NR | NR |
| Yavropoulou 2017 [70] | Greece | Multicenter cross-sectional, observational | 100 Osteoporotic patients with vertebral fractures (N = 35) Osteoporotic patients without vertebral fractures (N = 35) Healthy controls (N = 30) | NR | Female Osteoporotic patients with vertebral fractures 71 ± 7 years Osteoporotic patients without vertebral fractures 68 ± 7 years Healthy controls 68 ± 5 years | None | DXA |
| Yin 2022 [71] | China | NR | 95 Osteoporotic (N = 52) Healthy controls (N = 43) | NR | NR | None | NR |
| You 2016 [72] | China | NR | 155 Osteoporotic (N = 81) Healthy controls (N = 74) | NR | Female Osteoporotic 65.8 ± 1.9 years Healthy controls 43.3 ± 1.4 years | NR | DXA |
| Yu 2020 [73] | China | NR | 80 Osteoporotic with fracture (N = 40) Healthy controls (N = 40) | NR | Female/male Osteoporotic with fracture 60.8 ± 1.9 years Healthy controls 62 ± 2.5 years | None | DXA |
| Yuan 2021 [74] | China | NR | 89 Osteoporotic (N = 47) Healthy controls (N = 42) | NR | NR | None | DXA |
| Zarecki 2020 [75] | United Kingdom | Case-control, observational, cross-sectional | 107 Osteoporotic patients with vertebral fractures (N = 26) Osteoporotic patients without fractures (N = 39) Healthy controls (N = 42) | NR | Osteoporotic patients with vertebral fractures 69.6 years Osteoporotic patients without vertebral fractures 67.9 years Healthy controls 68.8 years | None | DXA |
| Zhang 2019 [76] | China | NR | Osteoporotic patients Healthy controls | NR | NR | None | NR |
| Zhang 2021 [77] | China | NR | 116 Osteoporotic with fracture (N = 60) Healthy controls (N = 56) | NR | Female/male Osteoporotic with fracture 68.00 ± 1.00 years Healthy controls 68.10 ± 1.00 years | None | DXA |
| Zhao 2019 [78] | China | NR | 96 Osteoporotic (N = 48) Healthy controls (N = 48) | NR | NR | None | NR |
| Zhou 2019 [79] | China | NR | 144 Osteoporotic (N = 99) Healthy controls (N = 45) | NR | Female Osteoporotic 62.6 ± 3.5 years Healthy controls 42.8 ± 5.5 years | None | DXA |
| Ref. | Country of Publication | Study Design | Patients Number | Ethnicity | Sex/Age | Comorbidities | Sarcopenia Diagnostic Measures |
|---|---|---|---|---|---|---|---|
| Chen 2019 b [32] | USA | NR | 75 Osteoporotic/osteopenic (N = 46) Sarcopenic (N = 1) Sarco-osteopenic (N = 15) Non-osteoporotic/non-sarcopenic (N = 13) | NR | Female 60–85 years | None | Handgrip dynamometer (grip strength), gait speed, and countermovement jumps |
| He 2020 [80] | China | NR | 186 Sarcopenic (N = 93) Non-sarcopenic (N = 93) | NR | Sarcopenic 76.15 ± 0.58 years Non-sarcopenic 76.19 ± 0.58 years | Hypertension, diabetes mellitus | Appendicular skeletal muscle mass (ASM); relative skeletal muscle mass index (ASM/Ht2) |
| He 2021 [81] | China | NR | 186 Sarcopenic (N = 93) Non-sarcopenic (N = 93) | Ximen Community of Ningbo | Sarcopenic 76.15 ± 0.58 years Non-sarcopenic 76.19 ± 0.58 years | Hypertension, diabetes mellitus | Appendicular skeletal muscle mass (ASM); relative skeletal muscle mass index (ASM/Ht2) |
| Liu 2021 [82] | China | NR | 77 Sarcopenic (N = 18) Dynapenic (loss of muscular function without mass) (N = 35) Non-sarcopenic (N = 24) | Community-dwelling older adults | Female/male Sarcopenic 79.8 ± 5.9 years Dynapenic 80.2 ± 5.7 years Non-sarcopenic 75.8 ± 6.1 years | None | Handgrip strength, gait speed |
| Valášková 2021 [83] | Slovakia | NR | 80 patients classified based on a short physical performance battery score (SPPB): Sarcopenia SPPB ≤ 6 (low muscle performance) (N = 31) Sarcopenia SPPB 7–9 (moderate muscle performance) (N = 17) Sarcopenia SPPB > 9 (high muscle performance) (N = 32) | NR | Female/male 55–86 years | NR | SPPB |
| Ref. | miR | miR Assay | Tissue | Endogenous Control | Technical Replicates | Timing of Sample Collection | miR Direction | Main Results |
|---|---|---|---|---|---|---|---|---|
| Al-Rawaf 2021 [26] | miR-148a and miR-122-5p | qRT-PCR | Serum | NR | Triplicate | In the morning, in fasted state | ↑ miR-148a ↓ miR-122-5p | ↑ miR-148a and ↓ miR-122-5p significantly associated with bone loss or osteoporosis in elderly postmenopausal women |
| Baloun 2022 [27] | let-7b-5p, miR-320a, miR-375, miR-188-5p, miR-152-3p, miR-582-5p, miR-144-5p, miR-141-3p, miR-127-3p, miR-17-5p | qRT-PCR | Serum | NR | NR | Before oophorectomy/ hysterectomy 201 ± 24 days after surgery 508 ± 127 days after Oophorectomy/hysterectomy 203 ± 71 days after estradiol treatment | No differences | No association of miRs with osteoporosis |
| Bedene 2016 [28] | let-7d-5p, let-7e-5p, miR-30d-5p, miR-30e-5p, miR-126-3p, miR-148a-3p, miR-199a-3p, miR-423-5p, and miR-574-5p | qRT-PCR | Serum | NR | NR | NR | ↑ miR-148a-3p | miR-148a-3p as a potential plasma-based biomarker for osteoporosis |
| Chen 2016 [29] | miR-30a-5p, miR-30e-5p, miR-425-5p, miR-142-3p, miR-191a-3p, miR-215, miR-29b-3p, miR-30b-5p, miR-26a-5p, miR-345-5p, miR-361-5p, miR-185-5p, miR-103-3p | qRT-PCR | Serum | NR | NR | NR | ↓ miR-30b-5p in osteopenia/osteoporosis; ↓ miR-103-3p, miR-142-3p, miR-328-3p in osteoporosis | miR-30b-5p down regulated in postmenopausal women with osteopenia or osteoporosis; ↓miR-103-3p, miR-142-3p, miR-328-3p only in osteoporosis |
| Chen 2017 [30] | miR-30, miR-96, miR-125b, miR-4665-3p, miR-5914 | qRT-PCR | Serum | U6 | NR | NR | ↑ miR-125b, miR-30, and miR-5914 | miR-125b significantly upregulated in postmenopausal osteoporosis |
| Chen 2019 [31] | miR-19a-3p | qRT-PCR | Serum | U6 | NR | In the morning, in fasted state | ↓miR-19a-3p | miR-19a-3p down-regulated in osteoporosis |
| Chen 2019 b [32] | miR-1-3p, miR-21-5p, miR-23a-3p, miR-24-3p, miR-100-5p, miR-125b-5p, miR-133a-3p, miR-206 | qRT-PCR | Serum | miR-16-5p, -93-5p, and -191-5p | NR | In the morning, in fasted state | ↓ miR-125b-5p and ↑ miR-21-5p and -23a-3 in osteoporosis | Relative expression level of miR-21-5p significantly negatively correlated with trochanter bone mineral content. |
| Cheng 2019 [33] | miR-365a-3p | qRT-PCR | Serum | NR | NR | In the morning, in fasted state | ↑miR-365a-3p | miR-365a-3p highly expressed in osteoporosis |
| Ciuffi 2022 [34] | miR-8085, miR-320a-3p, miR-23a-3p, miR-4497, miR-145-5p | ddPCR | Serum | Synthetic RNA spike-ins, UniSp2, UniSp4, and UniSp5 | NR | NR | ↓ miR-23a-3p ↑ miR-320a-3p | Levels of miR-23a-3p and miR-21-5p able to distinguish osteoporotic patients and subjects with normal BMD |
| Ding 2019 [35] | miR-100 | qRT-PCR | Serum | NR | NR | NR | ↑ miR-100 | miR-100 as potential biomarker for the diagnosis and treatment osteoporosis |
| Feurer 2019 [36] | miR-133a-3p, miR-20a-5p, miR-25-3p, miR-100-5p, miR-133b, miR-214-3p, miR-26a-5p, miR-103a-3p, miR-145-5p, miR-21-5p, miR-29a-3p, miR-106a-5p, miR-146a-5p, miR-221-5p, miR-29b-3p, miR-122-5p, miR-148a-3p, miR-222-3p, miR-338-3p, miR-124-3p, miR-155-5p, miR-223-5p, miR-34a-5p, miR-125b-5p, miR-17-5p, miR-23a-3p, miR-503-5p, miR-127-3p, miR-204-5p, miR-24-3p, miR-93-5p, miR-16-5p | qRT-PCR | Serum | UniSp6 | NR | In the morning, in fasted state | None | No significant association between prevalent or incident fractures, BTM, DXA, and HRpQCT parameters and analyzed miR |
| Fu 2019 [37] | miR-27a-3p | qRT-PCR | Serum | NR | NR | NR | ↓ miR-27a-3p | ↓miR-27a-3p in osteoporosis in comparison to controls |
| Fu 2021 [38] | miR-145-5p | qRT-PCR | Serum | U6 | Triplicate | In the morning, in fasted state | ↑ miR-145-5p | ↑miR-145-5p in osteoporotic in comparison to control |
| Gao 2020 [39] | miR-217 | qRT-PCR | Serum | NR | NR | NR | ↑ miR-217 | Up-regulation of miR-217 in osteoporotic in comparison to controls |
| Guo 2022 [40] | miR-221-5p | qRT-PCR | Serum | U6 | NR | NR | ↓ miR-221-5p | Down-regulation of miR-221-5p in osteoporotic in comparison to controls |
| Ismail 2020 [41] | miR-208a-3p, miR-155-5p, miR-637 | qRT-PCR | Serum | Hs_Snord68_11 | Duplicate | For premenopausal women: during the early follicular phase, i.e., days 3–7 of the menstrual cycle | ↑ miR-208a-3p, ↓ miR-155-5p | miR-208a-3p significantly upregulated, miR-155-5p markedly down-regulated in the premenopausal patients compared to its respective controls |
| Li 2014 [42] | miR-21, miR-133a, miR-146a | qRT-PCR | Plasma | miR-16 | NR | In the morning, in fasted state | ↓ miR-21 ↑ miR-133a | Downregulation of miR-21 and upregulation of miR-133a in osteoporosis and osteopenia patients versus controls |
| Li 2018 [43] | miR-133a | qRT-PCR | Serum | U6 | NR | NR | ↑ miR-133a | miR-133a significantly upregulated and negatively correlated with lumbar spine BMD in post-menopausal osteoporotic women |
| Li 2020 [44] | miR-483-5p | qRT-PCR | Serum | U6 | NR | NR | ↑ miR-483-5p | ↑ expression of miR-483–5p in osteoporotic patients |
| Lu 2021 [45] | miR-206 | qRT-PCR | Serum | U6 | NR | NR | ↓ miR-206 | ↓ miR-206 in osteoporotic patient group versus controls |
| Luo 2019 [46] | miR-579-3p | qRT-PCR | Serum | U6 | NR | NR | ↑ miR-579-3p | ↑ miR-579-3p in osteoporotic patients than controls |
| Lv 2019 [47] | miR-200a-3p | qRT-PCR | Serum | U6 | NR | NR | ↑ miR-200a-3p | ↑miR 200a-3p in osteoporotic patients relative to controls |
| Ma 2021 [48] | miR-181c-5p, miR-497-5p, miR-204-3p, miR-1290 | qRT-PCR | Serum | 5S rRNA | NR | In the morning, in fasted state | ↓ miR-181c-5p and miR-497-5p ↑ miR-204-3p | miR-181c-5p and miR-497-5p involved in bone metabolism and associated with progressive bone loss due to osteoporosis |
| Ma 2022 [49] | miR-455–3p | qRT-PCR | Serum | U6 | NR | NR | ↓ miR-455–3p | ↓ miR-455–3p in osteoporosis and fragility fracture patients compared to controls |
| Mandourah 2018 [50] | 370 mature miRs | qRT-PCR | Plasma and serum | SNORD61, SNORD68, SNORD72, SNORD95, SNORD96A, and RNU6-6P | NR | NR | ↓ miR122-5p and miR4516 | miR122-5p and miR4516 present at significantly different levels between non-osteoporotic control, osteopenia, and osteoporosis patients |
| Mi 2020 [51] | miR-194-5p | qRT-PCR | Serum | U6 | Triplicate | NR | ↑ miR-194-5p | ↑ miR-194-5p level linked to osteoporosis |
| Nakashima 2020 [52] | let7d, miR1, miR17, miR20a, miR21, miR27a, miR34a, miR92, miR103a, miR122, miR126, miR130a, miR133a, miR146, miR150, miR192, miR195, miR197, miR199, miR221, miR222, miR320 | qRT-PCR | Serum | NR | NR | In the morning, in fasted state | ↓ miR195, ↑ miR150 and miR222 | ↓ miR195 in osteoporotic females, ↑ miR150 and miR222 in osteoporotic males |
| Nobrega 2020 [53] | miR-1-3p, miR-21-5p, miR-34a-5p, miR-92a-3p, miR-100-5p, miR-126-3p, miR-130a-3p, miR-146a-5p, miR-155-5p, and miR-221-3p | qRT-PCR | Whole blood | RNU43 | NR | In the morning, in fasted state | ↑ miR-34a-5p | ↑ miR-34a-5p among very old adults who display the lowest scores of BMD |
| Panach 2015 [54] | Serum/Plasma microRNA PCR Panel | qRT-PCR | Serum | UniSP6 and cel-miR-39 | NR | NR | ↑ miR-122-5p, miR-125b-5p, and miR-21-5p | miR-122-5p, miR-125b-5p, and miR-21-5p upregulated biomarkers in bone fracture with respect to controls |
| Pertusa 2021 [55] | miR-497-5p, miR-155-5p, miR-423-5p, miR-365-3p | qRT-PCR | Serum | Cel-miR-39 | NR | NR | ↑ miR-497 and miR-423 ↓ miR-155 and miR-365 | ↑ miR-497 and miR-423 and ↓ miR-155 and miR-365 in osteoporotic than in control |
| Qiao 2019 [56] | miR-203 | qRT-PCR | Serum | NR | NR | In fasted state | ↓ miR-203 | ↓ miR-203 in patients with postmenopausal osteoporosis than in controls |
| Ramírez-Salazar 2019 [57] | miR-23b-3p, miR-140-3p, miR-885-5p | qRT-PCR | Serum | RNU6 | NR | NR | ↑ miR-140-3p and miR-23b-3p | miR-140-3p and miR-23b-3p as potential biomarkers candidates for osteoporosis |
| Salman 2021 [58] | miR-133a, miR-25 3p | qRT-PCR | Serum | RNU43 | NR | NR | ↑ miR-133a | miR-133a as biomarker for osteoporosis |
| Seeliger 2014 [59] | let-7a-5p, miR-1, miR-100-5p, miR-106b-5p, miR-10b-5p, miR-122-5p, miR-124-3p, miR-125b-5p, miR-126-3p, miR-133a, miR-133b, miR-134, miR-141-3p, miR-143-3p, miR-146a-5p, miR-150-5p, miR-155-5p, miR-17-5p/106a-5p, miR-17-3p, miR-18a-5p, miR-192-5p, miR-195-5p, miR-196a-5p, miR-19a-3p, miR-19b-3p, miR-200a-3p, miR-200b-3p, miR-200c-3p, miR-203a, miR-205-5p, miR-208a, miR-20a-5p, miR-21-5p, miR-210, miR-214-3p, miR-215, miR-221-3p, miR-222-3p, miR-223-3p, miR-224-5p, miR-23a-3p, miR-25-3p | qRT-PCR | Serum | RNU6 | Duplicate | NR | ↑ miR-21, miR-23a, miR-24, miR-93, miR-100, miR-122a, miR-124a, miR-125b, miR-148a | miR-21, miR-23a, miR-24, miR-93, miR-100, miR-122a, miR-124a, miR-125b, and miR-148a significantly upregulated in the serum of patients with osteoporosis |
| Shuai 2020 [60] | miR-29b-3p, miR-30c-2-3p, miR-145-5p, miR-199a-5p, miR-301a-3p, miR-497-5p, miR-526b-5p, miR-550a-5p, miR-575, miR-654-5p, miR-877-3p, miR-1260b, miR-4769-3p, miR-15a-5p, miR-424-5p, miR-663a, miR-708-5p, miR-1246, miR-1299, miR-1323, miR-4447, miR-5685 | qRT-PCR | Serum | U6 | NR | NR | ↑ miR-30c-2-3p, miR-497-5p, 550a-5p, miR-654-5p, miR-663a, miR-877-3p, miR-1299 ↓ miR-199a-5p, miR424-5p, miR-1260b | miR-30c-2-3p, miR-199a-5p, miR424-5p, miR-497-5p, miR-550a-5p, miR-654-5p, miR-663a, miR-877-3p, miR-1260b, miR-1299 ere highly expressed in serum and differed significantly among osteopenic, osteoporotic, and healthy patients |
| Sun 2020a [61] | miR-19b | qRT-PCR | Serum | U6 | NR | In the morning, in fasted state | ↓ miR-19b | ↓ miR-19b in osteoporotic patients with vertebral compression fractures than that in controls |
| Sun 2020b [62] | miR-211 | qRT-PCR | Serum | NR | NR | NR | ↑ miR-211 | In the fracture group, miR-211 expression was significantly up-regulated compared with controls |
| Tang 2019 [63] | miR-144 | qRT-PCR | Serum | U6 | NR | NR | ↑ miR-144 | Expression of miR-144 upregulated in osteoporotic patients compared with control |
| Wang 2018 [64] | miR-7-5p miR-211-5p, miR-24-3p, miR-27a-3p, miR-100, miR-125b, miR-122a, miR-128, miR 145, miR-144-3p | qRT-PCR | Serum | NR | Triplicate | NR | ↑ miR-24-3p, 27a-3p, 100, 125b, 122a, 145 ↓ miR-144-3p | Significant upregulation of miR-24-3p, 27a-3p, 100, 125b, 145, and 122a in osteoporosis compared to control. miR-144-3p downregulated in in osteoporosis compared to control |
| Weilner 2015 [65] | miR-10a-5p, miR-10b-5p, miR-133b, miR-22-3p, miR-328-3p, let-7g-5p | qRT-PCR | Serum | U6 and 5S rRNA | NR | Between 8:00 a.m. and 10:00 a.m. in fasted state | ↑ miR-22-3p, ↓ miR-328-3p and let-7g-5p | De-regulation of miR-22-3p, miR-328-3p, and let-7g-5p in osteoporotic fractured patients |
| Wu 2021 [66] | miR-10a-3p | qRT-PCR | Serum | U6 | Triplicate | NR | ↑ miR-10a-3p | ↑ miR-10a-3p in osteoporotic patients |
| Xia 2018 [67] | miR-203 | qRT-PCR | Serum | NR | Triplicate | In the morning, in fasted state | ↓ miR-203 | ↓ miR-203 in osteoporosis patients that in controls |
| Xu 2022 [68] | miR-491-5p, miR-485-3p | qRT-PCR | Plasma | U6 | NR | NR | ↓ miR-491-5p and miR-485-3p | Expression levels of miR-491-5p and miR-485-3p declined in osteoporotic patients with vertebral fractures when compared to those without fractures |
| Yang 2019 [69] | miR-217 | qRT-PCR | Serum | NR | NR | In the morning, in fasted state | ↑ miR-217 | ↑ miR-217 in osteoporotic patients |
| Yavropoulou 2017 [70] | miR-21-5p, miR-23a-3p, miR-24-2-5p, miR-26a-5p, miR-29a, miR-33a-5p, miR-124-3p, miR-135b-5p, miR-214-3p, miR-218-5p, miR-335-3p, miR-2861 | qRT-PCR | Serum | RNU6-2 | Triplicate | NR | ↑ miR-124 and miR-2861; ↓ miR-21, miR-23, miR-29, miR-21-5p | miR-21-5p, miR-23a, miR-29a-3p, miR-124-3p, and miR-2861 significantly deregulated in osteoporotic compared with controls. ↑ miR-124 and miR-2861 and ↓ miR-21, miR-23 and miR-29 in osteoporotic compared with controls. ↓miR-21-5p in osteoporotic/osteopenic women with vertebral fractures |
| Yin 2022 [71] | miR-215-5p | qRT-PCR | Serum | U6 | Triplicate | In fasted state | ↓ miR-215-5p | ↓ miR-215-5p in patients with osteoporosis |
| You 2016 [72] | miR-27a | qRT-PCR | Serum | U6 | Triplicate | NR | ↓ miR-27a | miR-27a significantly down-regulated in postmenopausal osteoporotic patients |
| Yu 2020 [73] | miR-137 | qRT-PCR | Serum | U6 | NR | NR | ↑ miR-137 | ↑ miR-137 in osteoporotic in comparison to controls |
| Yuan 2021 [74] | miR-26a | qRT-PCR | Serum | NR | NR | NR | ↑ miR-26a | ↑ miR-26a in patients with osteoporosis |
| Zarecki 2020 [75] | miR-19b-3p miR-486-3p, miR-550a-3p, miR-106b-5p, miR-144-3p, miR-451a, miR-29b-3p, miR-96-5p, miR-188-5p, miR-532-3p, miR-30e-5p, miR-214-3p, miR-143-3p, miR-133b, miR-21-5p, miR-23a-3p, miR-152-3p, miR-335-5p, miR-127-3p, miR-375 | qRT-PCR | Serum | cel-miR-39-3p | NR | After an overnight fast | ↑ miR-375, miR-532-3p, miR-19b-3p, miR-152-3p, miR-23a-3p, miR-335-5p, miR-21-5p | Up-regulated miR-375, miR-532-3p, miR-19b-3p, miR-152-3p, miR-23a-3p, miR-335-5p, miR-21-5p in patients with vertebral fractures and osteoporosis compared to osteoporosis without fracture and controls |
| Zhang 2019 [76] | miR-30a-5p | qRT-PCR | Serum | NR | NR | NR | ↑ miR-30a-5p | miR-30a-5p significantly upregulated in osteoporosis patients |
| Zhang 2021 [77] | miR-502-3p | qRT-PCR | Serum | U6 | Three duplicates | NR | ↓ miR-502-3p | ↓ miR-502-3p in osteoporotic than in controls |
| Zhao 2019 [78] | miR-17, miR-20a, miR-21, miR-26a, miR-29b, and miR-106b | qRT-PCR | Serum | U6 | NR | NR | ↓ miR-21 | ↓ miR-21 expression in patients with osteoporosis than in controls |
| Zhou 2019 [79] | miR-let-7c | qRT-PCR | Serum | NR | Triplicate | NR | ↑ miR-let-7c | miR-let-7c up-regulated in patients with postmenopausal osteoporosis compared with controls |
| Ref. | miR | miR Assay | Tissue | Reference Genes | Technical Replicates | Timing of Sample Collection | miR Direction | Main Results |
|---|---|---|---|---|---|---|---|---|
| Chen 2019 b [32] | miR-1-3p, miR-21-5p, miR-23a-3p, miR-24-3p, miR-100-5p, miR-125b-5p, miR-133a-3p, miR-206 | qRT-PCR | Serum | miR-16-5p, miR-93-5p, miR-191-5p | NR | In the early morning after overnight fasting | None | The study did not determine specific circulating miRs as biomarkers for sarcopenia |
| He 2020 [80] | miR-155, miR-208b, miR-222, miR-210, miR-328, miR-499, mir-133a, miR-133b, miR-21, miR-146a, miR-126, miR-221, and miR-20a | qRT-PCR | Plasma | cel-miR-39 | NR | After overnight fasting | ↓ miR-155, miR-208b, miR-222, miR-210, miR-328, and miR-499 | miR-155, miR-208b, miR-222, miR-210, miR-328, and miR-499 significantly down-regulated in sarcopenic patients compared to non-sarcopenic |
| He 2021 [81] | miR-637, miR-148a-3p, miR-125b-5p, miR-124-3p, miR-122-5p, miR-100-5p, miR-93-5p, miR-21-5p, miR-23a-3p, and miR-24-3p | qRT-PCR | Plasma | cel-miR-39 | NR | After overnight fasting | ↓ miR-23a-3p, miR-93-5p, and miR-637 | ↓ miR-23a-3p, miR-93-5p, miR-637 in the sarcopenia group than in the non-sarcopenia group |
| Liu 2021 [82] | miR-133a, miR-486, miR-21, miR-146a | qRT-PCR | Plasma | cel-miR-39-3p | NR | Fasting for at least 8 h and avoidance of strenuous physical exercise for at least 48 h | ↓ miR-486 and miR-146a | Myo-miR (miR-486) and inflammation-related miR (miR-146a) as biomarkers of age-related sarcopenia |
| Valášková 2021 [83] | miR-29a, miR-29b, miR-1, miR-133a, miR-133b, miR-206, miR-208b and miR-499 | qRT-PCR | Plasma | ce-miR-39 | NR | NR | ↑ miR-1, miR-29a and miR-29b; ↓ miR-206, miR-133a, miR-133b, miR-208b, and miR-499 | ↑ miR-1, miR-29a, and miR-29b and ↓miR-206, miR-133a, miR-133b, miR-208b, and miR-499 expression in patients with low muscle performance |
3. Results
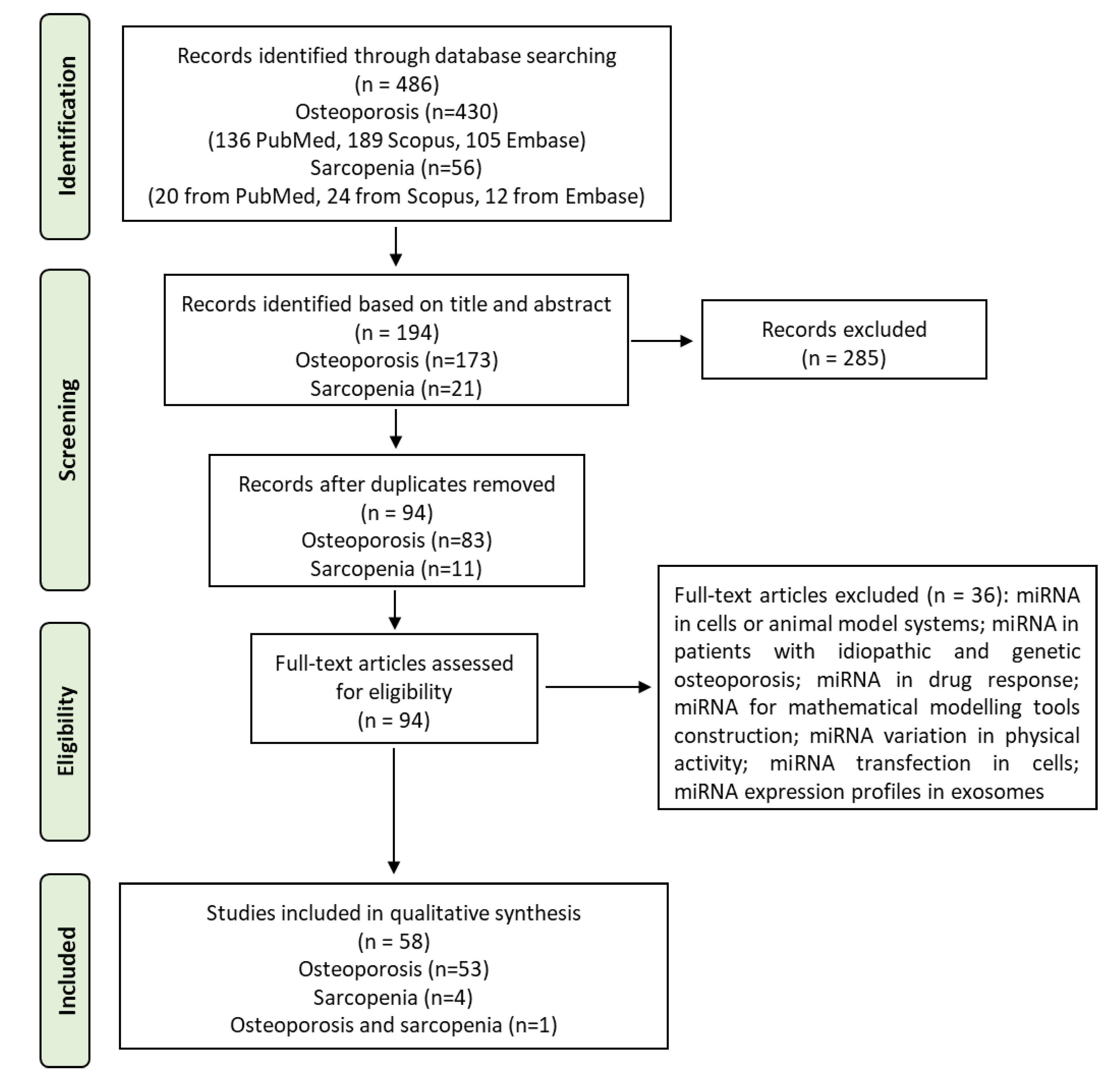
3.1. Study Selection and Characteristics
3.2. Study General Characteristics
3.3. miRs Dysregulation in Osteoporosis and Sarcopenia
3.4. miRs in Osteoporosis
3.5. miRs in Sarcopenia
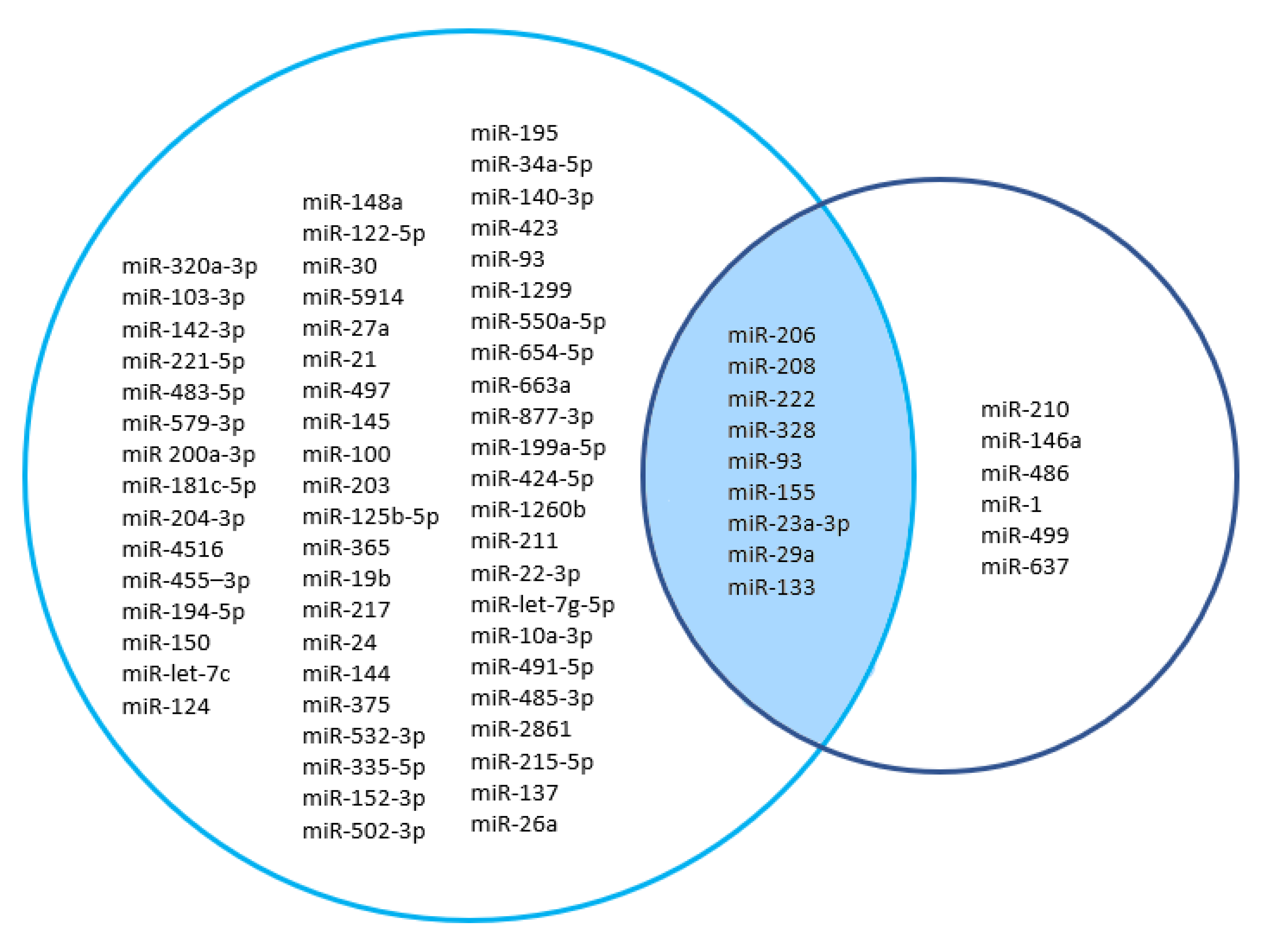
3.6. Sharing miRs between Osteoporosis and Sarcopenia
3.7. Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dawson, A.; Dennison, E. Measuring the musculoskeletal aging phenotype. Maturitas 2016, 93, 13–17. [Google Scholar] [CrossRef]
- Frost, H.M. On our age-related bone loss: Insights from a new paradigm. J. Bone Miner Res. 1997, 12, 1539–1546. [Google Scholar] [CrossRef]
- Frost, H.M. Bone’s mechanostat: A 2003 update. Anat. Rec. A Discov. Mol. Cell. Evol. Biol. 2003, 275, 1081–1101. [Google Scholar] [CrossRef]
- Kaji, H. Interaction between Muscle and Bone. J. Bone Metab. 2014, 21, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Tiidus, P.M. Benefits of estrogen replacement for skeletal muscle mass and function in post-menopausal females: Evidence from human and animal studies. Eurasian J. Med. 2011, 43, 109–114. [Google Scholar] [CrossRef]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef]
- Liu, J.; Curtis, E.M.; Cooper, C.; Harvey, N.C. State of the art in osteoporosis risk assessment and treatment. J. Endocrinol. Investig. 2019, 42, 1149–1164. [Google Scholar] [CrossRef]
- Bhasin, S.; Travison, T.G.; Manini, T.M.; Patel, S.; Pencina, K.M.; Fielding, R.A.; Magaziner, J.M.; Newman, A.B.; Kiel, D.P.; Cooper, C.; et al. Sarcopenia definition: The position statements of the sarcopenia definition and outcomes consortium. J. Am. Geriatr. Soc. 2020, 68, 1410–1418. [Google Scholar] [CrossRef]
- Bruyère, O.; Beaudart, C.; Ethgen, O.; Reginster, J.Y.; Locquet, M. The health economics burden of sarcopenia: A systematic review. Maturitas 2019, 119, 61–69. [Google Scholar] [CrossRef]
- Huo, Y.R.; Suriyaarachchi, P.; Gomez, F.; Curcio, C.-L.; Boersma, D.; Muir, S.W.; Montero-Odasso, M.; Gunawardene, P.; Demontiero, O.; Duque, G. Phenotype of osteosarcopenia in older individuals with a history of falling. J. Am. Med. Dir. Assoc. 2015, 16, 290–295. [Google Scholar] [CrossRef]
- Wang, Y.J.; Wang, Y.; Zhan, J.K.; Tang, Z.Y.; He, J.Y.; Tan, P.; Deng, H.Q.; Huang, W.; Liu, Y.S. Sarco-osteoporosis: Prevalence and association with frailty in chinese community-dwelling older adults. Int. J. Endocrinol. 2015, 2015, 482940. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.G.; Chang, M.C. Dorsal scapular nerve injury after trigger point injection into the rhomboid major muscle: A case report. J. Back Musculoskelet. Rehabil. 2018, 31, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Pasha, E.P.; Birdsill, A.; Parker, P.; Elmenshawy, A.; Tanaka, H.; Haley, A.P. Visceral adiposity predicts subclinical white matter hyperintensities in middle-aged adults. Obes. Res. Clin. Pract. 2017, 11, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Picetti, D.; Foster, S.; Pangle, A.K.; Schrader, A.; George, M.; Wei, J.Y.; Azhar, G. Hydration health literacy in the elderly. Nutr. Healthy Aging 2017, 4, 227–237. [Google Scholar] [CrossRef]
- Huai, Y.; Zhang, W.; Chen, Z.; Zhao, F.; Wang, W.; Dang, K.; Xue, K.; Gao, Y.; Jiang, S.; Miao, Z.; et al. A Comprehensive Analysis of MicroRNAs in Human Osteoporosis. Front. Endocrinol. 2020, 11, 516213. [Google Scholar] [CrossRef]
- Zhang, L.; Hu, C.; Huang, Z.; Li, Z.; Zhang, Q.; He, Y. In Silico screening of circulating tumor DNA, circulating microRNAs, and long non-coding RNAs as diagnostic molecular biomarkers in ovarian cancer: A comprehensive meta-analysis. PLoS ONE 2021, 16, e0250717. [Google Scholar] [CrossRef]
- Gu, J.; Rao, W.; Huo, S.; Fan, T.; Qiu, M.; Zhu, H.; Chen, D.; Sheng, X. MicroRNAs and long non-coding RNAs in cartilage homeostasis and osteoarthritis. Front. Cell Dev. Biol. 2022, 10, 1092776. [Google Scholar] [CrossRef]
- Bellavia, D.; Salamanna, F.; Raimondi, L.; De Luca, A.; Carina, V.; Costa, V.; Alessandro, R.; Fini, M.; Giavaresi, G. Deregulated miRNAs in osteoporosis: Effects in bone metastasis. Cell. Mol. Life Sci. 2019, 76, 3723–3744. [Google Scholar] [CrossRef]
- Bellavia, D.; De Luca, A.; Carina, V.; Costa, V.; Raimondi, L.; Salamanna, F.; Alessandro, R.; Fini, M.; Giavaresi, G. Deregulated miRNAs in bone health: Epigenetic roles in osteoporosis. Bone 2019, 122, 52–75. [Google Scholar] [CrossRef]
- Chen, X.; Ba, Y.; Ma, L.; Cai, X.; Yin, Y.; Wang, K.; Guo, J.; Zhang, Y.; Chen, J.; Guo, X.; et al. Characterization of microRNAs in serum: A novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res. 2008, 18, 997–1006. [Google Scholar] [CrossRef]
- He, L.; Hannon, G.J. MicroRNAs: Small RNAs with a big role in gene regulation. Nat. Rev. Genet. 2004, 5, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Gilad, S.; Meiri, E.; Yogev, Y.; Benjamin, S.; Lebanony, D.; Yerushalmi, N.; Benjamin, H.; Kushnir, M.; Cholakh, H.; Melamed, N.; et al. Serum MicroRNAs Are Promising Novel Biomarkers. PLoS ONE 2008, 3, e3148. [Google Scholar] [CrossRef] [PubMed]
- Hackl, M.; Heilmeier, U.; Weilner, S.; Grillari, J. Circulating microRNAs as novel biomarkers for bone diseases—Complex signatures for multifactorial diseases? Mol. Cell. Endocrinol. 2016, 432, 83–95. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Al-Rawaf, H.A.; Alghadir, A.H.; Gabr, S.A. Circulating MicroRNA Expression, Vitamin D, and Hypercortisolism as Predictors of Osteoporosis in Elderly Postmenopausal Women. Dis. Markers 2021, 2021, 3719919. [Google Scholar] [CrossRef]
- Baloun, J.; Pekacova, A.; Wenchich, L.; Hruskova, H.; Senolt, L.; Svec, X.; Pavelka, K.; Stepan, J.J. Menopausal Transition: Prospective Study of Estrogen Status, Circulating MicroRNAs, and Biomarkers of Bone Metabolism. Front. Endocrinol. 2022, 13, 864299. [Google Scholar] [CrossRef]
- Bedene, A.; Mencej Bedrač, S.; Ješe, L.; Marc, J.; Vrtačnik, P.; Preželj, J.; Kocjan, T.; Kranjc, T.; Ostanek, B. MiR-148a the epigenetic regulator of bone homeostasis is increased in plasma of osteoporotic postmenopausal women. Wien. Klin. Wochenschr. 2016, 128 (Suppl. S7), 519–526. [Google Scholar] [CrossRef]
- Chen, J.; Li, K.; Pang, Q.; Yang, C.; Zhang, H.; Wu, F.; Cao, H.; Liu, H.; Wan, Y.; Xia, W.; et al. Identification of suitable reference gene and biomarkers of serum miRNAs for osteoporosis. Sci. Rep. 2016, 6, 36347. [Google Scholar] [CrossRef]
- Chen, H.; Jiang, H.; Can, D.; Xu, H.; Zhang, K. Evaluation of MicroRNA 125b as a potential biomarker for postmenopausal osteoporosis. Trop. J. Pharm. Res. 2017, 16, 641–647. [Google Scholar] [CrossRef]
- Chen, R.; Qiu, H.; Tong, Y.; Liao, F.; Hu, X.; Qiu, Y.; Liao, Y. MiRNA-19a-3p alleviates the progression of osteoporosis by targeting HDAC4 to promote the osteogenic differentiation of hMSCs. Biochem. Biophys. Res. Commun. 2019, 516, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Bemben, M.G.; Bemben, D.A. Bone and muscle specific circulating microRNAs in postmenopausal women based on osteoporosis and sarcopenia status. Bone 2019, 120, 271–278. [Google Scholar] [CrossRef]
- Cheng, F.; Yang, M.M.; Yang, R.H. MiRNA-365a-3p promotes the progression of osteoporosis by inhibiting osteogenic differentiation via targeting RUNX2. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 7766–7774. [Google Scholar] [PubMed]
- Ciuffi, S.; Marini, F.; Fossi, C.; Donati, S.; Giusti, F.; Botta, A.; Masi, L.; Isaia, G.; Marcocci, C.; Migliaccio, S.; et al. Circulating MicroRNAs as Biomarkers of Osteoporosis and Fragility Fractures. J. Clin. Endocrinol. Metab. 2022, 107, 2267–2285. [Google Scholar] [CrossRef]
- Ding, W.; Ding, S.; Li, J.; Peng, Z.; Hu, P.; Zhang, T.; Pan, L. Aberrant Expression of miR-100 in Plasma of Patients with Osteoporosis and its Potential Diagnostic Value. Clin. Lab. 2019, 65. [Google Scholar] [CrossRef] [PubMed]
- Feurer, E.; Kan, C.; Croset, M.; Sornay-Rendu, E.; Chapurlat, R. Lack of Association Between Select Circulating miRNAs and Bone Mass, Turnover, and Fractures: Data from the OFELY Cohort. J. Bone Miner. Res. 2019, 34, 1074–1085. [Google Scholar] [CrossRef]
- Fu, Y.C.; Zhao, S.R.; Zhu, B.H.; Guo, S.S.; Wang, X.X. MiRNA-27a-3p promotes osteogenic differentiation of human mesenchymal stem cells through targeting ATF3. Eur. Rev. Med. Pharmacol. Sci. 2019, 23 (Suppl. S3), 73–80. [Google Scholar]
- Fu, Y.; Hu, X.; Gao, Y.; Li, K.; Fu, Q.; Liu, Q.; Liu, D.; Zhang, Z.; Qiao, J. LncRNA ROR/miR-145-5p axis modulates the osteoblasts proliferation and apoptosis in osteoporosis. Bioengineered 2021, 12, 7714–7723. [Google Scholar] [CrossRef]
- Gao, G.C.; Yang, D.W.; Liu, W. LncRNA TERC alleviates the progression of osteoporosis by absorbing miRNA-217 to upregulate RUNX2. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 526–534. [Google Scholar]
- Guo, M.; Liu, N.; Guo, Z. MiR-221-5p/Smad3 axis in osteoclastogenesis and its function: Potential therapeutic target for osteoporosis. Steroids 2022, 185, 109063. [Google Scholar] [CrossRef]
- Ismail, S.M.; El Boghdady, N.A.; Hamoud, H.S.; Shabayek, M.I. Evaluation of circulating miRNA-208a-3p, miRNA-155-5p and miRNA-637 as potential non-invasive biomarkers and the possible mechanistic insights into pre- and postmenopausal osteoporotic females. Arch. Biochem. Biophys. 2020, 684, 108331. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wang, Z.; Fu, Q.; Zhang, J. Plasma miRNA levels correlate with sensitivity to bone mineral density in postmenopausal osteoporosis patients. Biomarkers 2014, 19, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhang, W.; Huang, Y. MiRNA-133a is involved in the regulation of postmenopausal osteoporosis through promoting osteoclast differentiation. Acta Biochim. Biophys. Sin. 2018, 50, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Chen, S.; Cai, P.; Chen, K.; Li, L.; Yang, X.; Yi, J.; Luo, X.; Du, Y.; Zheng, H. MiRNA-483-5p is involved in the pathogenesis of osteoporosis by promoting osteoclast differentiation. Mol. Cell. Probes 2020, 49, 101479. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.; Wang, D.; Wang, X.; Zou, J.; Sun, J.; Bi, Z. MiR-206 regulates the progression of osteoporosis via targeting HDAC4. Eur. J. Med. Res. 2021, 26, 8. [Google Scholar] [CrossRef] [PubMed]
- Luo, B.; Yang, J.F.; Wang, Y.H.; Qu, G.B.; Hao, P.D.; Zeng, Z.J.; Yuan, J.; Yang, R.; Yuan, Y. MicroRNA-579-3p promotes the progression of osteoporosis by inhibiting osteogenic differentiation of mesenchymal stem cells through regulating Sirt1. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 6791–6799. [Google Scholar]
- Lv, R.; Pan, X.; Song, L.; Sun, Q.; Guo, C.; Zou, S.; Zhou, Q. MicroRNA-200a-3p accelerates the progression of osteoporosis by targeting glutaminase to inhibit osteogenic differentiation of bone marrow mesenchymal stem cells. Biomed. Pharmacother. 2019, 116, 108960. [Google Scholar] [CrossRef]
- Ma, J.; Lin, X.; Chen, C.; Li, S.; Zhang, S.; Chen, Z.; Li, D.; Zhao, F.; Yang, C.; Yin, C.; et al. Circulating miR-181c-5p and miR-497-5p Are Potential Biomarkers for Prognosis and Diagnosis of Osteoporosis. J. Clin. Endocrinol. Metab. 2020, 105, dgz300. [Google Scholar] [CrossRef]
- Ma, H.; Li, M.; Jia, Z.; Chen, X.; Bu, N. MicroRNA-455-3p promotes osteoblast differentiation via targeting HDAC2. Injury 2022, 53, 3636–3641. [Google Scholar] [CrossRef]
- Mandourah, A.Y.; Ranganath, L.; Barraclough, R.; Vinjamuri, S.; Hof, R.V.; Hamill, S.; Czanner, G.; Dera, A.A.; Wang, D.; Barraclough, D.L. Circulating microRNAs as potential diagnostic biomarkers for osteoporosis. Sci. Rep. 2018, 8, 8421. [Google Scholar] [CrossRef]
- Mi, B.; Yan, C.; Xue, H.; Chen, L.; Panayi, A.C.; Hu, L.; Hu, Y.; Cao, F.; Sun, Y.; Zhou, W.; et al. Inhibition of Circulating miR-194-5p Reverses Osteoporosis through Wnt5a/β-Catenin-Dependent Induction of Osteogenic Differentiation. Mol. Ther. Nucleic Acids 2020, 21, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, H.; Ando, K.; Kobayashi, K.; Seki, T.; Ishizuka, S.; Fujii, R.; Takegami, Y.; Yamada, H.; Ando, Y.; Suzuki, K.; et al. Associations of Serum MicroRNA with Bone Mineral Density in Community-Dwelling Subjects: The Yakumo Study. Biomed Res. Int. 2020, 2020, 5047243. [Google Scholar] [CrossRef] [PubMed]
- Nóbrega, O.T.; Morais-Junior, G.S.; Viana, N.I.; Reis, S.T.; Perez, D.I.V.; Freitas, W.M.; Sposito, A.C.; Leite, K.R.M.; Srougi, M. Circulating miR-34a and Bone Mineral Density of Brazilian Very-Old Adults. J. Aging Res. 2020, 2020, 3431828. [Google Scholar] [CrossRef] [PubMed]
- Panach, L.; Mifsut, D.; Tarín, J.J.; Cano, A.; García-Pérez, M.Á. Serum Circulating MicroRNAs as Biomarkers of Osteoporotic Fracture. Calcif. Tissue Int. 2015, 97, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Pertusa, C.; Tarín, J.J.; Cano, A.; García-Pérez, M.Á.; Mifsut, D. Serum microRNAs in osteoporotic fracture and osteoarthritis: A genetic and functional study. Sci. Rep. 2021, 11, 19372. [Google Scholar] [CrossRef]
- Qiao, L.; Liu, D.; Li, C.G.; Wang, Y.J. MiR-203 is essential for the shift from osteogenic differentiation to adipogenic differentiation of mesenchymal stem cells in postmenopausal osteoporosis. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 5804–5814. [Google Scholar]
- Ramírez-Salazar, E.G.; Carrillo-Patiño, S.; Hidalgo-Bravo, A.; Rivera-Paredez, B.; Quiterio, M.; Ramírez-Palacios, P.; Patiño, N.; Valdés-Flores, M.; Salmerón, J.; Velázquez-Cruz, R. Serum miRNAs miR-140-3p and miR-23b-3p as potential biomarkers for osteoporosis and osteoporotic fracture in postmenopausal Mexican-Mestizo women. Gene 2018, 679, 19–27. [Google Scholar] [CrossRef]
- Salman, H.D.; Kadhim, M.M. MiRNA-133a and MiRNA-25 3p and their relationship with some variables in serum of patients with Osteoporosis. Arch. Venez. Farmacol. Ter. 2021, 40, 775–782. [Google Scholar]
- Seeliger, C.; Karpinski, K.; Haug, A.T.; Vester, H.; Schmitt, A.; Bauer, J.S.; van Griensven, M. Five freely circulating miRNAs and bone tissue miRNAs are associated with osteoporotic fractures. J. Bone Miner. Res. 2014, 29, 1718–1728. [Google Scholar] [CrossRef]
- Shuai, Y.; Liao, L.; Su, X.; Sha, N.; Li, X.; Wu, Y.; Jing, H.; Kuang, H.; Deng, Z.; Li, Y.; et al. Circulating microRNAs in serum as novel biomarkers for osteoporosis: A case-control study. Ther. Adv. Musculoskelet. Dis. 2020, 12, 1759720X20953331. [Google Scholar] [CrossRef]
- Sun, M.; Hu, L.; Wang, S.; Huang, T.; Zhang, M.; Yang, M.; Zhen, W.; Yang, D.; Lu, W.; Guan, M.; et al. Circulating MicroRNA-19b identified from osteoporotic vertebral compression fracture patients increases bone formation. J. Bone Miner. Res. 2020, 35, 306–316. [Google Scholar] [CrossRef]
- Sun, T.; Yang, D.; Wu, Y.; Sheng, Q. The function of microRNA-211 expression in post-fracture bone cell apoptosis involving the transforming growth factor-β/ phosphoinositide 3-kinase signaling pathway. J. Int. Med. Res. 2020, 48, 300060520926353. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Lu, W.; Huang, J.; Tang, X.; Zhang, H.; Liu, S. miR-144 promotes the proliferation and differentiation of bone mesenchymal stem cells by downregulating the expression of SFRP1. Mol. Med. Rep. 2019, 20, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; He, H.; Wang, L.; Jiang, Y.; Xu, Y. Reduced miR-144-3p expression in serum and bone mediates osteoporosis pathogenesis by targeting RANK. Biochem. Cell Biol. 2018, 96, 627–635. [Google Scholar] [CrossRef] [PubMed]
- Weilner, S.; Skalicky, S.; Salzer, B.; Keider, V.; Wagner, M.; Hildner, F.; Gabriel, C.; Dovjak, P.; Pietschmann, P.; Grillari-Voglauer, R.; et al. Differentially circulating miRNAs after recent osteoporotic fractures can influence osteogenic differentiation. Bone 2015, 79, 43–51. [Google Scholar] [CrossRef]
- Wu, W.; Li, Q.; Liu, Y.F.; Li, Y. lncRNA GAS5 regulates angiogenesis by targeting miR-10a-3p/VEGFA in osteoporosis. Mol. Med. Rep. 2021, 24, 711. [Google Scholar] [CrossRef]
- Xia, Z.L.; Wang, Y.; Sun, Q.D.; Du, X.F. MiR-203 is involved in osteoporosis by regulating DKK1 and inhibiting osteogenic differentiation of MSCs. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 5098–5105. [Google Scholar]
- Xu, J.; Li, M.; Pei, W.; Ding, J.; Pan, Y.; Peng, H.; Lin, S.; Huang, Y. Reduced Circulating Levels of miR-491-5p and miR-485-3p Are Associated with the Occurrence of Vertebral Fractures in Postmenopausal Women with Osteoporosis. Genet. Res. 2022, 2022, 3838126. [Google Scholar] [CrossRef]
- Yang, L.; Zeng, Z.; Kang, N.; Yang, J.C.; Wei, X.; Hai, Y. Circ-VANGL1 promotes the progression of osteoporosis by absorbing miRNA-217 to regulate RUNX2 expression. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 949–957. [Google Scholar]
- Yavropoulou, M.P.; Anastasilakis, A.D.; Makras, P.; Tsalikakis, D.G.; Grammatiki, M.; Yovos, J.G. Expression of microRNAs that regulate bone turnover in the serum of postmenopausal women with low bone mass and vertebral fractures. Eur. J. Endocrinol. 2017, 176, 169–176. [Google Scholar] [CrossRef]
- Yin, Z.; Shen, J.; Wang, Q.; Wen, L.; Qu, W.; Zhang, Y. miR-215-5p regulates osteoporosis development and osteogenic differentiation by targeting XIAP. BMC Musculoskelet. Disord. 2022, 23, 789. [Google Scholar] [CrossRef] [PubMed]
- You, L.; Pan, L.; Chen, L.; Gu, W.; Chen, J. MiR-27a is Essential for the Shift from Osteogenic Differentiation to Adipogenic Differentiation of Mesenchymal Stem Cells in Postmenopausal Osteoporosis. Cell. Physiol. Biochem. 2016, 39, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Yao, P.; Wang, Z.; Xie, W. Down-regulation of FTX promotes the differentiation of osteoclasts in osteoporosis through the Notch1 signaling pathway by targeting miR-137. BMC Musculoskelet. Disord. 2020, 21, 456. [Google Scholar] [CrossRef] [PubMed]
- Yuan, F.; Chen, H.; Hu, P.; Su, P.; Guan, X. MiR-26a regulates the expression of serum IGF-1 in patients with osteoporosis and its effect on proliferation and apoptosis of mouse chondrocytes. J. Musculoskelet. Neuronal Interact. 2021, 21, 298–307. [Google Scholar]
- Zarecki, P.; Hackl, M.; Grillari, J.; Debono, M.; Eastell, R. Serum microRNAs as novel biomarkers for osteoporotic vertebral fractures. Bone 2020, 130, 115105. [Google Scholar] [CrossRef]
- Zhang, H.L.; Du, X.Y.; Dong, Q.R. LncRNA XIXT promotes osteogenic differentiation of bone mesenchymal stem cells and alleviates osteoporosis progression by targeting miRNA-30a-5p. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 8721–8729. [Google Scholar]
- Zhang, J.; Hou, Y.; Wang, Z.; Zhou, P.; Zhang, P.; Wang, J.; Sun, Z.; Wang, L. Study on Omentin-1 and miR-502-3p in osteoporotic fracture. J. Musculoskelet. Neuronal Interact. 2021, 21, 308–316. [Google Scholar]
- Zhao, Z.; Li, X.; Zou, D.; Lian, Y.; Tian, S.; Dou, Z. Expression of microRNA-21 in osteoporotic patients and its involvement in the regulation of osteogenic differentiation. Exp. Ther. Med. 2019, 17, 709–714. [Google Scholar] [CrossRef]
- Zhou, Z.; Lu, Y.; Wang, Y.; Du, L.; Zhang, Y.; Tao, J. Let-7c regulates proliferation and osteodifferentiation of human adipose-derived mesenchymal stem cells under oxidative stress by targeting SCD-1. Am. J. Physiol. Cell Physiol. 2019, 316, C57–C69. [Google Scholar] [CrossRef]
- He, N.; Zhang, Y.L.; Zhang, Y.; Feng, B.; Zheng, Z.; Wang, D.; Zhang, S.; Guo, Q.; Ye, H. Circulating MicroRNAs in Plasma Decrease in Response to Sarcopenia in the Elderly. Front. Genet. 2020, 11, 167. [Google Scholar] [CrossRef]
- He, N.; Zhang, Y.; Zhang, Y.; Feng, B.; Zheng, Z.; Wang, D.; Zhang, S.; Ye, H. Increasing Fracture Risk Associates with Plasma Circulating MicroRNAs in Aging People’s Sarcopenia. Front. Physiol. 2021, 12, 678610. [Google Scholar] [CrossRef]
- Liu, H.C.; Han, D.S.; Hsu, C.C.; Wang, J.S. Circulating MicroRNA-486 and MicroRNA-146a serve as potential biomarkers of sarcopenia in the older adults. BMC Geriatr. 2022, 21, 86. [Google Scholar] [CrossRef]
- Valášková, S.; Gažová, A.; Vrbová, P.; Koller, T.; Šalingova, B.; Adamičková, A.; Chomaničová, N.; Hulajová, N.; Payer, J.; Kyselovič, J. The Severity of Muscle Performance Deterioration in Sarcopenia Correlates with Circulating Muscle Tissue-Specific miRNAs. Physiol. Res. 2021, 70 (Suppl. S1), S91–S98. [Google Scholar] [CrossRef]
- Tarantino, U.; Greggi, C.; Visconti, V.V.; Cariati, I.; Tallarico, M.; Fauceglia, M.; Iundusi, R.; Albanese, M.; Chiaramonte, C.; Gasbarra, E. T-Score and Handgrip Strength Association for the Diagnosis of Osteosarcopenia: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2597. [Google Scholar] [CrossRef]
- McCloskey, E.V.; Johansson, H.; Oden, A.; Austin, M.; Siris, E.; Wang, A.; Lewiecki, E.M.; Lorenc, R.; Libanati, C.; A Kanis, J. Denosumab reduces the risk of osteoporotic fractures in postmenopausal women, particularly in those with moderate to high fracture risk as assessed with FRAX. J. Bone Miner. Res. 2012, 27, 1480–1486. [Google Scholar] [CrossRef]
- Ko, N.Y.; Chen, L.R.; Chen, K.H. The Role of Micro RNA and Long-Non-Coding RNA in Osteoporosis. Int. J. Mol. Sci. 2020, 21, 4886. [Google Scholar] [CrossRef]
- Tang, P.; Xiong, Q.; Ge, W.; Zhang, L. The Role of MicroRNAs in Osteoclasts and Osteoporosis. RNA Biol. 2014, 11, 1355–1363. [Google Scholar] [CrossRef]
- Kim, H.K.; Lee, Y.S.; Sivaprasad, U.; Malhotra, A.; Dutta, A. Muscle-specific microRNA miR-206 promotes muscle differentiation. J. Cell Biol. 2006, 174, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Goljanek-Whysall, K.; Pais, H.; Rathjen, T.; Sweetman, D.; Dalmay, T.; Münsterberg, A. Regulation of multiple target genes by miR-1 and miR-206 is pivotal for C2C12 myoblast differentiation. J. Cell Sci. 2012, 125, 3590–3600. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; Wang, H.; Liao, Y.; Zhou, P.; Xu, Y.; Zhao, Y.; Xie, S.; Zhao, S.; Li, X. miR-208b modulating skeletal muscle development and energy homoeostasis through targeting distinct targets. RNA Biol. 2020, 17, 743–754. [Google Scholar] [CrossRef] [PubMed]
- Cardinali, B.; Cappella, M.; Provenzano, C.; Garcia-Manteiga, J.M.; Lazarevic, D.; Cittaro, D.; Martelli, F.; Falcone, G. MicroRNA-222 regulates muscle alternative splicing through Rbm24 during differentiation of skeletal muscle cells. Cell Death Dis. 2016, 7, e2086. [Google Scholar] [CrossRef] [PubMed]
- Yoshizuka, M.; Nakasa, T.; Kawanishi, Y.; Hachisuka, S.; Furuta, T.; Miyaki, S.; Adachi, N.; Ochi, M. Inhibition of microRNA-222 expression accelerates bone healing with enhancement of osteogenesis, chondrogenesis, and angiogenesis in a rat refractory fracture model. J. Orthop. Sci. 2016, 21, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Nie, M.; Deng, Z.L.; Liu, J.; Wang, D.Z. Noncoding RNAs, Emerging Regulators of Skeletal Muscle Development and Diseases. BioMed Res. Int. 2015, 2015, 676575. [Google Scholar] [CrossRef]
- Nie, M.; Liu, J.; Yang, Q.; Seok, H.Y.; Hu, X.; Deng, Z.L.; Wang, D.Z. MicroRNA-155 facilitates skeletal muscle regeneration by balancing pro- and anti-inflammatory macrophages. Cell Death Dis. 2016, 7, e2261. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Cheng, P.; Chen, C.; He, H.B.; Xie, G.Q.; Zhou, H.D.; Xie, H.; Wu, X.P.; Luo, X.H. miR-93/Sp7 function loop mediates osteoblast mineralization. J. Bone Miner. Res. 2012, 27, 1598–1606. [Google Scholar] [CrossRef] [PubMed]
- Roberto, V.P.; Tiago, D.M.; Silva, I.A.; Cancela, M.L. MiR-29a is an enhancer of mineral deposition in bone-derived systems. Arch. Biochem. Biophys. 2014, 564, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Roderburg, C.; Urban, G.W.; Bettermann, K.; Vucur, M.; Zimmermann, H.; Schmidt, S.; Janssen, J.; Koppe, C.; Knolle, P.; Castoldi, M.; et al. Micro-RNA profiling reveals a role for miR-29 in human and murine liver fibrosis. Hepatology 2011, 53, 209–218. [Google Scholar] [CrossRef] [PubMed]
- van Rooij, E.; Sutherland, L.B.; Thatcher, J.E.; DiMaio, J.M.; Naseem, R.H.; Marshall, W.S.; Hill, J.A.; Olson, E.N. Dysregulation of microRNAs after myocardial infarction reveals a role of miR-29 in cardiac fibrosis. Proc. Natl. Acad. Sci. USA 2008, 105, 13027–13032. [Google Scholar] [CrossRef]
- Maurer, B.; Stanczyk, J.; Jüngel, A.; Akhmetshina, A.; Trenkmann, M.; Brock, M.; Kowal-Bielecka, O.; Gay, R.E.; Michel, B.A.; Distler, J.H.W.; et al. MicroRNA-29, a key regulator of collagen expression in systemic sclerosis. Arthritis Rheum. 2010, 62, 1733–1743. [Google Scholar] [CrossRef]
- Cushing, L.; Kuang, P.P.; Qian, J.; Shao, F.; Wu, J.; Little, F.; Thannickal, V.J.; Cardoso, W.V.; Lü, J. miR-29 is a major regulator of genes associated with pulmonary fibrosis. Am. J. Respir. Cell. Mol. Biol. 2011, 45, 287–294. [Google Scholar] [CrossRef]
- Cacchiarelli, D.; Martone, J.; Girardi, E.; Cesana, M.; Incitti, T.; Morlando, M.; Nicoletti, C.; Santini, T.; Sthandier, O.; Barberi, L.; et al. MicroRNAs involved in molecular circuitries relevant for the Duchenne muscular dystrophy pathogenesis are controlled by the dystrophin/nNOS pathway. Cell Metab. 2010, 12, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Xie, M.; Wang, X.; Jiang, X.; Li, J.; Huang, H. miR-155 modulates TNF-α-inhibited osteogenic differentiation by targeting SOCS1 expression. Bone 2012, 51, 498–505. [Google Scholar] [CrossRef] [PubMed]



| PubMed | |
|---|---|
| Osteoporosis | ((“osteoporosis” [MeSH Terms] OR “osteoporosis” [All Fields] OR “osteoporoses” [All Fields] OR “osteoporosis, postmenopausal” [MeSH Terms] OR (“osteoporosis” [All Fields] AND “postmenopausal” [All Fields]) OR “postmenopausal osteoporosis” [All Fields]) AND (((“serum” [MeSH Terms] OR “serum” [All Fields] OR “serums” [All Fields] OR “serum s” [All Fields] OR “serumal” [All Fields]) AND (“microrna s” [All Fields] OR “micrornas” [MeSH Terms] OR “micrornas” [All Fields] OR “microrna” [All Fields])) OR (“circulating microrna” [MeSH Terms] OR (“circulating” [All Fields] AND “microrna” [All Fields]) OR “circulating microrna” [All Fields]))) AND ((y_10[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter])) |
| Sarcopenia | ((“sarcopenia” [MeSH Terms] OR “sarcopenia” [All Fields] OR “sarcopenia s” [All Fields]) AND (((“serum” [MeSH Terms] OR “serum” [All Fields] OR “serums” [All Fields] OR “serum s” [All Fields] OR “serumal” [All Fields]) AND (“microrna s” [All Fields] OR “micrornas” [MeSH Terms] OR “micrornas” [All Fields] OR “microrna” [All Fields])) OR (“circulating microrna” [MeSH Terms] OR (“circulating” [All Fields] AND “microrna” [All Fields]) OR “circulating microrna” [All Fields])) AND “2013/01/02 00:00”:”3000/01/01 05:00” [Date—Publication]) AND ((y_10[Filter]) AND (fha[Filter]) AND (humans[Filter]) AND (english[Filter])) |
| Scopus | |
| Osteoporosis | (TITLE-ABS-KEY(osteoporosis)) AND (TITLE-ABS-KEY (serum AND microrna) OR TITLE-ABS-KEY (circulating AND microrna)) AND (PUBYEAR > 2011) AND (LIMIT-TO (DOCTYPE,”ar”)) AND (LIMIT-TO (LANGUAGE,”English”)) |
| Sarcopenia | (TITLE-ABS-KEY (sarcopenia) AND TITLE-ABS-KEY (serum AND microrna) OR TITLE-ABS-KEY (circulating AND microrna)) AND PUBYEAR > 2012 AND (LIMIT-TO (DOCTYPE, “ar”)) AND (LIMIT-TO (LANGUAGE, “English”)) |
| EMBASE | |
| Osteoporosis | (‘osteoporosis’/exp OR osteoporosis) AND (‘serum microrna’ OR ((‘serum’/exp OR serum) AND (‘microrna’/exp OR microrna)) OR ‘circulating microrna’/exp OR ‘circulating microrna’ OR (circulating AND (‘microrna’/exp OR microrna))) AND [2013–2023]/py AND [humans]/lim AND [abstracts]/lim AND [clinical study]/lim AND [embase]/lim AND [article]/lim AND [english]/lim |
| Sarcopenia | (‘sarcopenia’/exp OR sarcopenia) AND (‘serum microrna’ OR ((‘serum’/exp OR serum) AND (‘microrna’/exp OR microrna)) OR ‘circulating microrna’/exp OR ‘circulating microrna’ OR (circulating AND (‘microrna’/exp OR microrna))) AND [humans]/lim AND [abstracts]/lim AND [clinical study]/lim AND [embase]/lim AND [2013–2023]/py AND [article]/lim AND [english]/lim |
| Risk of Bias | Applicability Concerns | |||||||
|---|---|---|---|---|---|---|---|---|
| Patients Selection | Index Test | References Standard | Flow and Timing | Patients Selection | Index Test | References Standard | ||
| Al-Rawaf 2021 [26] | ||||||||
| Baloun 2022 [27] | ||||||||
| Bedene 2016 [28] | ||||||||
| Chen 2016 [29] | ||||||||
| Chen 2017 [30] | ||||||||
| Chen 2019 [31] | ||||||||
| Chen 2019 b [32] | ||||||||
| Cheng 2019 [33] | ||||||||
| Ciuffi 2022 [34] | ||||||||
| Ding 2019 [35] | ||||||||
| Feurer 2019 [36] | ||||||||
| Fu 2019 [37] | ||||||||
| Fu 2021 [38] | ||||||||
| Gao 2020 [39] | ||||||||
| Guo 2022 [40] | ||||||||
| Ismail 2020 [41] | ||||||||
| Li 2014 [42] | ||||||||
| Li 2018 [43] | ||||||||
| Li 2020 [44] | ||||||||
| Lu 2021 [45] | ||||||||
| Luo 2019 [46] | ||||||||
| Lv 2019 [47] | ||||||||
| Ma 2021 [48] | ||||||||
| Ma 2022 [49] | ||||||||
| Mandourah 2018 [50] | ||||||||
| Mi 2020 [51] | ||||||||
| Nakashima 2020 [52] | ||||||||
| Nobrega 2020 [53] | ||||||||
| Panach 2015 [54] | ||||||||
| Pertusa 2021 [55] | ||||||||
| Qiao 2019 [56] | ||||||||
| Ramírez-Salazar 2019 [57] | ||||||||
| Salman 2021 [58] | ||||||||
| Seeliger 2014 59] | ||||||||
| Shuai 2020 [60] | ||||||||
| Sun 2020a [61] | ||||||||
| Sun 2020b [62] | ||||||||
| Tang 2019 [63] | ||||||||
| Wang 2018 [64] | ||||||||
| Weilner 2015 [65] | ||||||||
| Wu 2021 [66] | ||||||||
| Xia 2018 [67] | ||||||||
| Xu 2022 [68] | ||||||||
| Yang 2019 [69] | ||||||||
| Yavropoulou 2017 [70] | ||||||||
| Yin 2022 [71] | ||||||||
| You 2016 [72] | ||||||||
| Yu 2020 [73] | ||||||||
| Yuan 2021 [74] | ||||||||
| Zarecki 2020 [75] | ||||||||
| Zhang 2019 [76] | ||||||||
| Zhang 2021 [77] | ||||||||
| Zhao 2019 [78] | ||||||||
| Zhou 2019 [79] | ||||||||
| He 2020 [80] | ||||||||
| He 2021 [82] | ||||||||
| Liu 2021 [82] | ||||||||
| Valášková 2021 [83] | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salamanna, F.; Contartese, D.; Ruffilli, A.; Barile, F.; Bellavia, D.; Marchese, L.; Manzetti, M.; Viroli, G.; Faldini, C.; Giavaresi, G. Sharing Circulating Micro-RNAs between Osteoporosis and Sarcopenia: A Systematic Review. Life 2023, 13, 602. https://doi.org/10.3390/life13030602
Salamanna F, Contartese D, Ruffilli A, Barile F, Bellavia D, Marchese L, Manzetti M, Viroli G, Faldini C, Giavaresi G. Sharing Circulating Micro-RNAs between Osteoporosis and Sarcopenia: A Systematic Review. Life. 2023; 13(3):602. https://doi.org/10.3390/life13030602
Chicago/Turabian StyleSalamanna, Francesca, Deyanira Contartese, Alberto Ruffilli, Francesca Barile, Daniele Bellavia, Laura Marchese, Marco Manzetti, Giovanni Viroli, Cesare Faldini, and Gianluca Giavaresi. 2023. "Sharing Circulating Micro-RNAs between Osteoporosis and Sarcopenia: A Systematic Review" Life 13, no. 3: 602. https://doi.org/10.3390/life13030602
APA StyleSalamanna, F., Contartese, D., Ruffilli, A., Barile, F., Bellavia, D., Marchese, L., Manzetti, M., Viroli, G., Faldini, C., & Giavaresi, G. (2023). Sharing Circulating Micro-RNAs between Osteoporosis and Sarcopenia: A Systematic Review. Life, 13(3), 602. https://doi.org/10.3390/life13030602