
Anticancer Therapy and Mortality of Adult Patients with Hematologic Malignancy and COVID-19: A Systematic Review and Meta-Analysis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
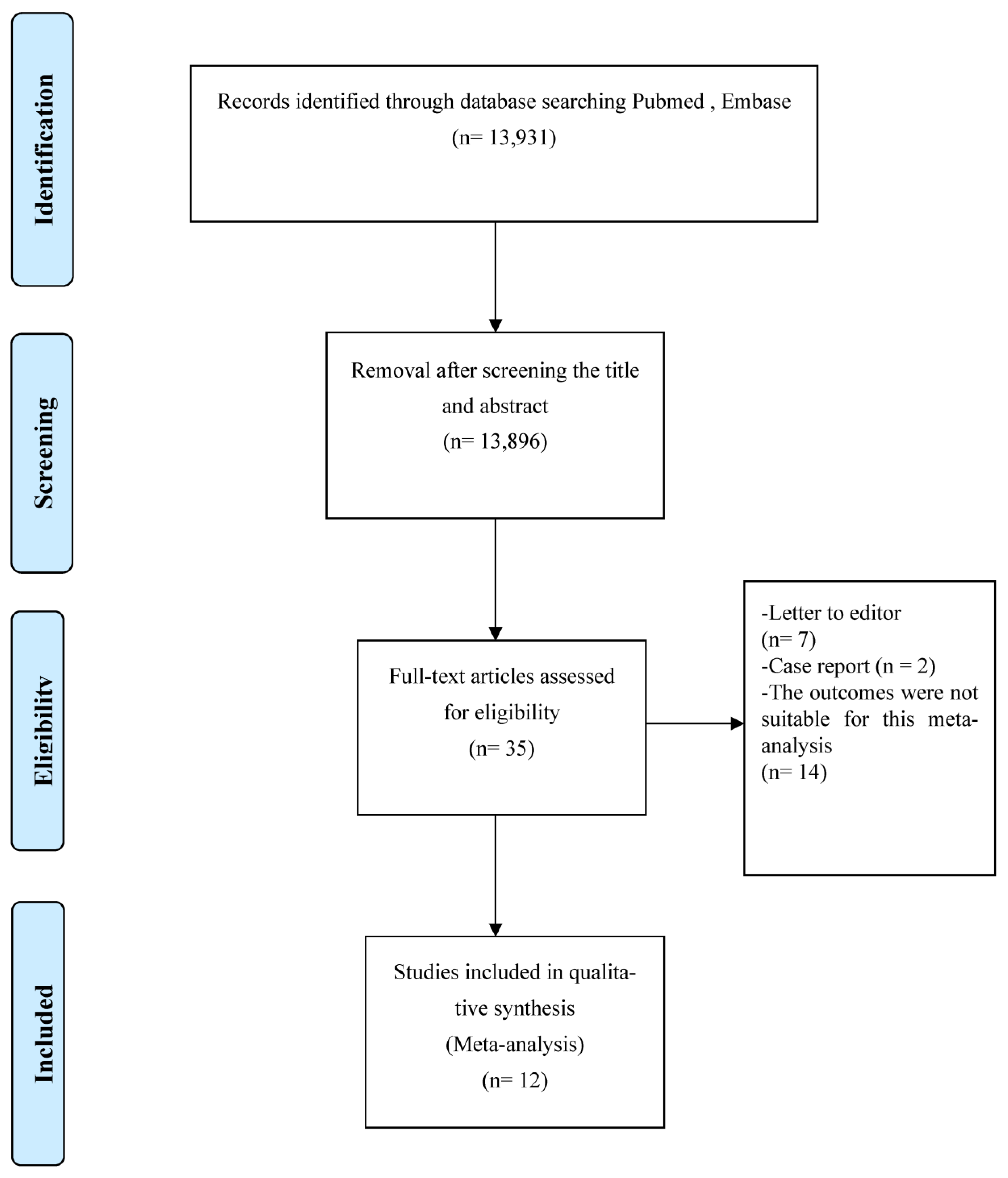
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Appraisal
2.5. Meta-Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weekly Epidemiological Update on COVID-19—28 September 2022. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---28-september-2022 (accessed on 1 October 2022).
- Hamming, I.; Timens, W.; Bulthuis, M.L.; Lely, A.T.; Navis, G.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef]
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef]
- Tsamakis, K.; Gavriatopoulou, M.; Schizas, D.; Stravodimou, A.; Mougkou, A.; Tsiptsios, D.; Sioulas, V.; Spartalis, E.; Sioulas, A.D.; Tsamakis, C.; et al. Oncology during the COVID-19 pandemic: Challenges, dilemmas and the psychosocial impact on cancer patients (Review). Oncol. Lett. 2020, 20, 441–447. [Google Scholar] [CrossRef]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef]
- Li, J.Y.; Duan, X.F.; Wang, L.P.; Xu, Y.J.; Huang, L.; Zhang, T.F.; Liu, J.Y.; Li, F.; Zhang, Z.; Yue, D.L.; et al. Selective depletion of regulatory T cell subsets by docetaxel treatment in patients with nonsmall cell lung cancer. J. Immunol. Res. 2014, 2014, 286170. [Google Scholar] [CrossRef]
- Longbottom, E.R.; Torrance, H.D.; Owen, H.C.; Fragkou, P.C.; Hinds, C.J.; Pearse, R.M.; O’Dwyer, M.J. Features of Postoperative Immune Suppression Are Reversible with Interferon Gamma and Independent of Interleukin-6 Pathways. Ann. Surg. 2016, 264, 370–377. [Google Scholar] [CrossRef]
- Sica, A.; Massarotti, M. Myeloid suppressor cells in cancer and autoimmunity. J. Autoimmun. 2017, 85, 117–125. [Google Scholar] [CrossRef]
- Reda, G.; Noto, A.; Cassin, R.; Zamprogna, G.; Borella, C.; Scarfò, L.; Farina, L.; Molteni, A.; Ghia, P.; Tedeschi, A.; et al. Rete Ematologica Lombarda (REL) Clinical Network (2020). Reply to “CLL and COVID-19 at the Hospital Clinic of Barcelona: An interim report” Analysis of six hematological centers in Lombardy: On behalf of CLL commission of Lombardy Hematology Network (REL). Leukemia 2020, 34, 2531–2532. [Google Scholar] [CrossRef]
- Thibaud, S.; Tremblay, D.; Bhalla, S.; Zimmerman, B.; Sigel, K.; Gabrilove, J. Protective role of Bruton tyrosine kinase inhibitors in patients with chronic lymphocytic leukaemia and COVID-19. Br. J. Haematol. 2020, 190, e73–e76. [Google Scholar] [CrossRef]
- Treon, S.P.; Castillo, J.J.; Skarbnik, A.P.; Soumerai, J.D.; Ghobrial, I.M.; Guerrera, M.L.; Meid, K.; Yang, G. The BTK inhibitor ibrutinib may protect against pulmonary injury in COVID-19-infected patients. Blood 2020, 135, 1912–1915. [Google Scholar] [CrossRef]
- Brissot, E.; Labopin, M.; Baron, F.; Bazarbachi, A.; Bug, G.; Ciceri, F.; Esteve, J.; Giebel, S.; Gilleece, M.H.; Gorin, N.C.; et al. Management of patients with acute leukemia during the COVID-19 outbreak: Practical guidelines from the acute leukemia working party of the European Society for Blood and Marrow Transplantation. Bone Marrow Transpl. 2021, 56, 532–535. [Google Scholar] [CrossRef]
- Yahalom, J.; Dabaja, B.S.; Ricardi, U.; Ng, A.; Mikhaeel, N.G.; Vogelius, I.R.; Illidge, T.; Qi, S.; Wirth, A.; Specht, L. ILROG emergency guidelines for radiation therapy of hematological malignancies during the COVID-19 pandemic. Blood 2020, 135, 1829–1832. [Google Scholar] [CrossRef]
- Giannakoulis, V.G.; Papoutsi, E.; Siempos, I.I. Effect of Cancer on Clinical Outcomes of Patients with COVID-19: A Meta-Analysis of Patient Data. JCO Glob. Oncol. 2020, 6, 799–808. [Google Scholar] [CrossRef]
- Grivas, P.; Khaki, A.R.; Wise-Draper, T.M.; French, B.; Hennessy, C.; Hsu, C.Y.; Shyr, Y.; Li, X.; Choueiri, T.K.; Painter, C.A.; et al. Association of clinical factors and recent anticancer therapy with COVID-19 severity among patients with cancer: A report from the COVID-19 and Cancer Consortium. Ann. Oncol. 2021, 32, 787–800. [Google Scholar] [CrossRef]
- Sharafeldin, N.; Bates, B.; Song, Q.; Madhira, V.; Yan, Y.; Dong, S.; Lee, E.; Kuhrt, N.; Shao, Y.R.; Liu, F.; et al. Outcomes of COVID-19 in Patients with Cancer: Report from the National COVID Cohort Collaborative (N3C). J. Clin. Oncol. 2021, 39, 2232–2246. [Google Scholar] [CrossRef]
- Desai, A.; Sachdeva, S.; Parekh, T.; Desai, R. COVID-19 and Cancer: Lessons from a Pooled Meta-Analysis. JCO Glob. Oncol. 2020, 6, 557–559. [Google Scholar]
- Vijenthira, A.; Gong, I.Y.; Fox, T.A.; Booth, S.; Cook, G.; Fattizzo, B.; Martín-Moro, F.; Razanamahery, J.; Riches, J.C.; Zwicker, J.; et al. Outcomes of patients with hematologic malignancies and COVID-19: A systematic review and meta-analysis of 3377 patients. Blood 2020, 136, 2881–2892. [Google Scholar] [CrossRef]
- Mato, A.R.; Roeker, L.E.; Lamanna, N.; Allan, J.N.; Leslie, L.; Pagel, J.M.; Patel, K.; Osterborg, A.; Wojenski, D.; Kamdar, M.; et al. Outcomes of COVID-19 in patients with CLL: A multicenter international experience. Blood 2020, 136, 1134–1143. [Google Scholar] [CrossRef]
- Li, H.C.; Wang, H.H.; Chou, F.H.; Chen, K.M. The effect of music therapy on cognitive functioning among older adults: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2015, 16, 71–77. [Google Scholar] [CrossRef]
- Yang, K.; Sheng, Y.; Huang, C.; Jin, Y.; Xiong, N.; Jiang, K.; Lu, H.; Liu, J.; Yang, J.; Dong, Y.; et al. Clinical characteristics, outcomes, and risk factors for mortality in patients with cancer and COVID-19 in Hubei, China: A multicentre, retrospective, cohort study. Lancet Oncol. 2020, 21, 904–913. [Google Scholar] [CrossRef]
- Zaki, A.; Soomar, S.M.; Khan, D.H.; Shaharyar Sheikh, H.; Iftikhar, R.; Mir, A.; Aziz, Z.; Bano, K.; Naseer, H.; Chaudhry, Q.U.; et al. “Outcomes of COVID-19 infection in patients with hematological malignancies- A multicenter analysis from Pakistan”. PLoS ONE 2022, 17, e0267139. [Google Scholar] [CrossRef]
- Azhdari Tehrani, H.; Ramezaninejad, S.; Mardani, M.; Shokouhi, S.; Darnahal, M.; Hakamifard, A. Hematologic malignancies and COVID-19 infection: A monocenter retrospective study. Health Sci. Rep. 2022, 5, e638. [Google Scholar] [CrossRef]
- Booth, S.; Willan, J.; Wong, H.; Khan, D.; Farnell, R.; Hunter, A.; Eyre, T.; Katz, H.; Dungarwalla, M.; Chen, L.; et al. Regional outcomes of severe acute respiratory syndrome coronavirus 2 infection in hospitalised patients with haematological malignancy. Eur. J. Haematol. 2020, 105, 476–483. [Google Scholar] [CrossRef]
- Fox, T.A.; Troy-Barnes, E.; Kirkwood, A.A.; Chan, W.Y.; Day, J.W.; Chavda, S.J.; Kumar, E.A.; David, K.; Tomkins, O.; Sanchez, E.; et al. Clinical outcomes and risk factors for severe COVID-19 in patients with haematological disorders receiving chemo- or immunotherapy. Br. J. Haematol. 2020, 191, 194–206. [Google Scholar] [CrossRef]
- Martín-Moro, F.; Marquet, J.; Piris, M.; Michael, B.M.; Sáez, A.J.; Corona, M.; Jiménez, C.; Astibia, B.; García, I.; Rodríguez, E.; et al. Survival study of hospitalised patients with concurrent COVID-19 and haematological malignancies. Br. J. Haematol. 2020, 190, e16–e20. [Google Scholar] [CrossRef]
- Puła, B.; Pruszczyk, K.; Pietrusza, E.; Morawska, M.; Piszczek, W.; Kalicińska, E.; Szeremet, A.; Tryc-Szponder, J.; Wąsik-Szczepanek, E.; Drozd-Sokołowska, J.; et al. Outcome of SARS-CoV-2-Infected Polish Patients with Chronic Lymphocytic Leukemia. Cancers 2022, 14, 558. [Google Scholar] [CrossRef]
- Sanchez-Pina, J.M.; Rodríguez Rodriguez, M.; Castro Quismondo, N.; Gil Manso, R.; Colmenares, R.; Gil Alos, D.; Paciello, M.L.; Zafra, D.; Garcia-Sanchez, C.; Villegas, C.; et al. Clinical course and risk factors for mortality from COVID-19 in patients with haematological malignancies. Eur. J. Hematol. 2020, 105, 597–607. [Google Scholar] [CrossRef]
- Scarfò, L.; Chatzikonstantinou, T.; Rigolin, G.M.; Quaresmini, G.; Motta, M.; Vitale, C.; Garcia-Marco, J.A.; Hernández-Rivas, J.Á.; Mirás, F.; Baile, M.; et al. COVID-19 severity and mortality in patients with chronic lymphocytic leukemia: A joint study by ERIC, the European Research Initiative on CLL, and CLL Campus. Leukemia 2020, 34, 2354–2363. [Google Scholar] [CrossRef]
- Tığlıoğlu, P.; Albayrak, M.; Tığlıoğlu, M.; Öztürk, H.; Aras, M.R.; Sağlam, B.; Maral, S. The outcome of COVID-19 in patients with hematological malignancy. Memo 2022, 15, 83–89. [Google Scholar] [CrossRef]
- Wang, B.; Van Oekelen, O.; Mouhieddine, T.H.; Del Valle, D.M.; Richter, J.; Cho, H.J.; Richard, S.; Chari, A.; Gnjatic, S.; Merad, M.; et al. A tertiary center experience of multiple myeloma patients with COVID-19: Lessons learned and the path forward. J. Hematol. Oncol. 2020, 13, 94. [Google Scholar] [CrossRef]
- Wu, Y.; Chen, W.; Li, W.; Zhao, M.; Wei, Q.; Zhang, X.; Mei, H.; Wang, Y.; Hu, Y. Clinical characteristics, therapeutic management, and prognostic factors of adult COVID-19 inpatients with hematological malignancies. Leuk. Lymphoma 2020, 61, 3440–3450. [Google Scholar] [CrossRef] [PubMed]
- Malkan, U.Y.; Haznedaroglu, I.C. Hematological aspects of the COVID-19 syndrome. Eur. Rev. Med. Pharmacol. 2022, 26, 4463–4476. [Google Scholar]
- Yigenoglu, T.N.; Ata, N.; Altuntas, F.; Bascı, S.; Dal, M.S.; Korkmaz, S.; Namdaroglu, S.; Basturk, A.; Hacıbekiroglu, T.; Dogu, M.H.; et al. The outcome of COVID-19 in patients with hematological malignancy. J. Med. Virol. 2021, 93, 1099–1104. [Google Scholar] [CrossRef]
- Lin, Z.; Chen, J.; Han, S. Impact of anticancer therapy on disease severity and mortality in cancer patients with COVID-19: A systematic review and meta-analysis. Expert Rev. Anticancer Ther. 2021, 21, 1055–1066. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zheng, Y.; Niu, Z.; Zhang, B.; Wang, C.; Yao, X.; Peng, H.; Franca, D.N.; Wang, Y.; Zhu, Y.; et al. SARS-CoV-2 spike protein dictates syncytium-mediated lymphocyte elimination. Cell Death Differ. 2021, 28, 2765–2777. [Google Scholar] [CrossRef] [PubMed]
- Erdogdu, B.; Cinar, O.E.; Malkan, U.Y.; Aksu, S.; Demiroglu, H.; Buyukasik, Y.; Goker, H.; Sayinalp, N.; Haznedaroglu, I.C. Hematopoietic Adverse Events Associated with BNT162b2 mRNA Covid-19 Vaccine. UHOD 2022, 32, 65–67. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Studies/Years | Region | Number of Patients | Age (Year) | Sex (Male) | Anticancer Therapy | Mortality (Event/Total) | Newcastle–Ottawa |
|---|---|---|---|---|---|---|---|
| Azhdari Tehrani, 2022 [23] | Iran | 194 | 44 (15–81) | 135 | Chemotherapy vs. no treatment | 47.4% (92/194) | 7 |
| Booth, 2020 [24] | UK | 66 | 73 (63–81) | 41 | Immunosuppressive or chemotherapy in the last 3 months vs. no treatment | 51.5% (34/66) | 7 |
| Fox, 2020 [25] | UK | 55 | 63 (23–88) | 37 | Immunosuppressive or chemotherapy vs. no treatment | 34.6% (19/55) | 7 |
| Martín-Moro, 2020 [26] | China | 34 | 72.5 (35–94) | 19 | Chemotherapy vs. no treatment | 32.4% (11/34) | 9 |
| Mato, 2020 [19] | USA | 178 | 71 (41–98) | 110 | Immunosuppressive or chemotherapy vs. no treatment | 37.1% (66/178) | 9 |
| Puła, 2022 [27] | Poland | 175 | 68 (37–87) | 70 | Targeted therapy vs. no treatment | 26.6% (50/188) | 9 |
| Sanchez-Pina, 2020 [28] | Spain | 39 | 64.7 (36–88) | 23 | Chemotherapy vs. no treatment | 35.8% (14/39) | 9 |
| Scarfò, 2020 [29] | Italy | 190 | 72 (48–94) | 126 | Chemotherapy vs. no treatment | 29.5 (56/190) | 6 |
| Tığlıoğlu, 2021 [30] | Turkey | 77 | 60 (27–93) | 40 | Immunosuppressive or chemotherapy vs. no treatment | 20.7% (16/77) | 7 |
| Wang, 2020 [31] | USA | 58 | 67 | 30 | Immunosuppressive vs. no treatment | 24.0% (14/58) | 7 |
| Wu, 2020 [32] | China | 14 | 36.5 (14–68) | 9 | Immunosuppressive or chemotherapy vs. no treatment | 42.8% (6/14) | 7 |
| Zaki, 2022 [22] | Pakistan | 107 | NA * | 72 | Immunosuppressive or chemotherapy vs. no treatment | 23.4% (25/107) | 9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, W.-L.; Nguyen, T.-H.-Y.; Wu, L.-M.; Huang, W.-T.; Su, S.-B. Anticancer Therapy and Mortality of Adult Patients with Hematologic Malignancy and COVID-19: A Systematic Review and Meta-Analysis. Life 2023, 13, 381. https://doi.org/10.3390/life13020381
Lin W-L, Nguyen T-H-Y, Wu L-M, Huang W-T, Su S-B. Anticancer Therapy and Mortality of Adult Patients with Hematologic Malignancy and COVID-19: A Systematic Review and Meta-Analysis. Life. 2023; 13(2):381. https://doi.org/10.3390/life13020381
Chicago/Turabian StyleLin, Wen-Li, Thi-Hoang-Yen Nguyen, Li-Min Wu, Wen-Tsung Huang, and Shih-Bin Su. 2023. "Anticancer Therapy and Mortality of Adult Patients with Hematologic Malignancy and COVID-19: A Systematic Review and Meta-Analysis" Life 13, no. 2: 381. https://doi.org/10.3390/life13020381
APA StyleLin, W.-L., Nguyen, T.-H.-Y., Wu, L.-M., Huang, W.-T., & Su, S.-B. (2023). Anticancer Therapy and Mortality of Adult Patients with Hematologic Malignancy and COVID-19: A Systematic Review and Meta-Analysis. Life, 13(2), 381. https://doi.org/10.3390/life13020381