
Applying Grey Relational Analysis in the Evaluation of the Balance of Children with Intellectual Disability

Abstract
:1. Introduction
2. Grey Relational Analysis
- I.
- is a standard sequence, whereas are comparison sequences.
- II.
- is the norm betweenand, whereas is the mean of .
- III.
- .
3. Method
3.1. Participants
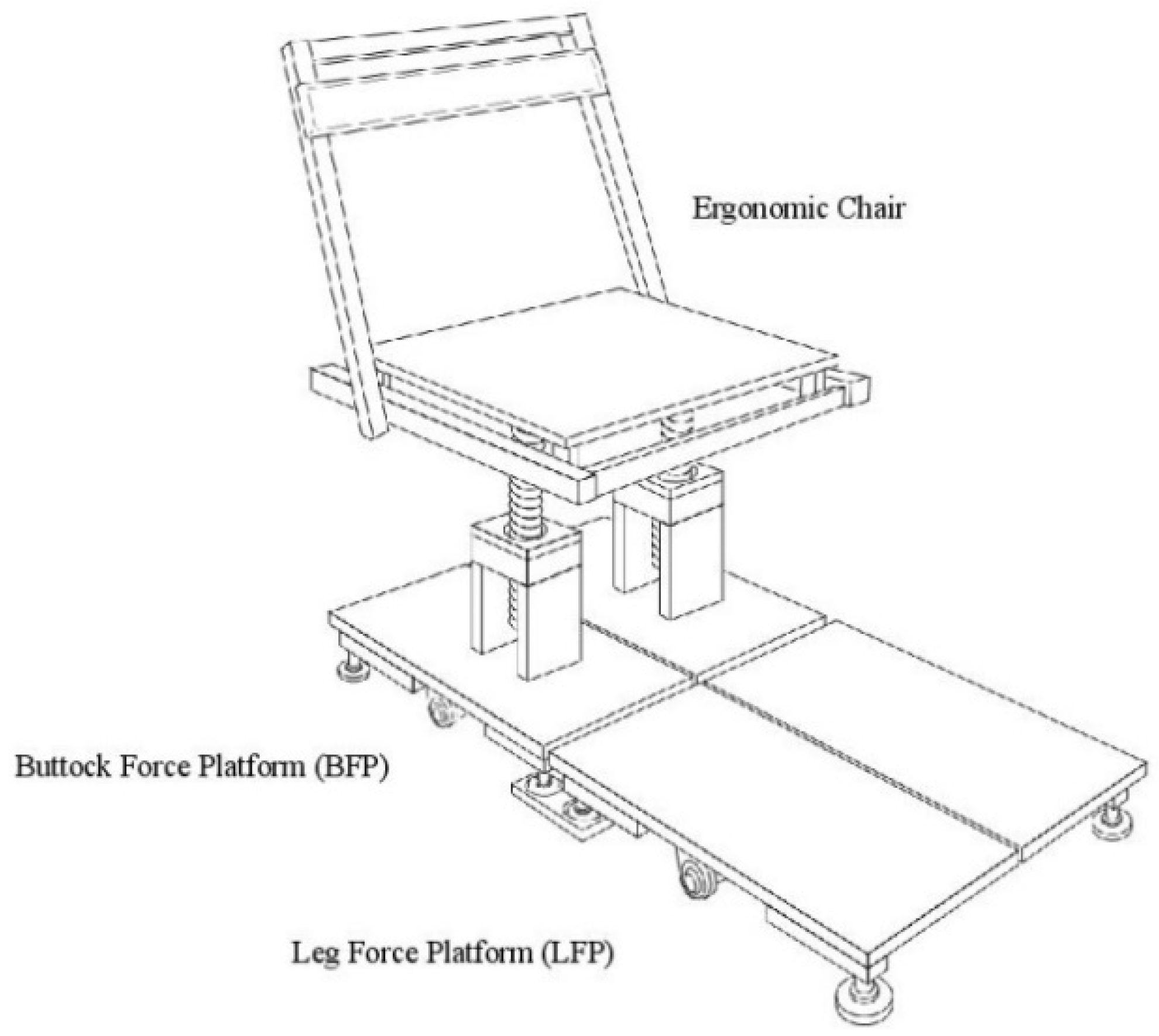
3.2. Apparatus
3.3. Procedure
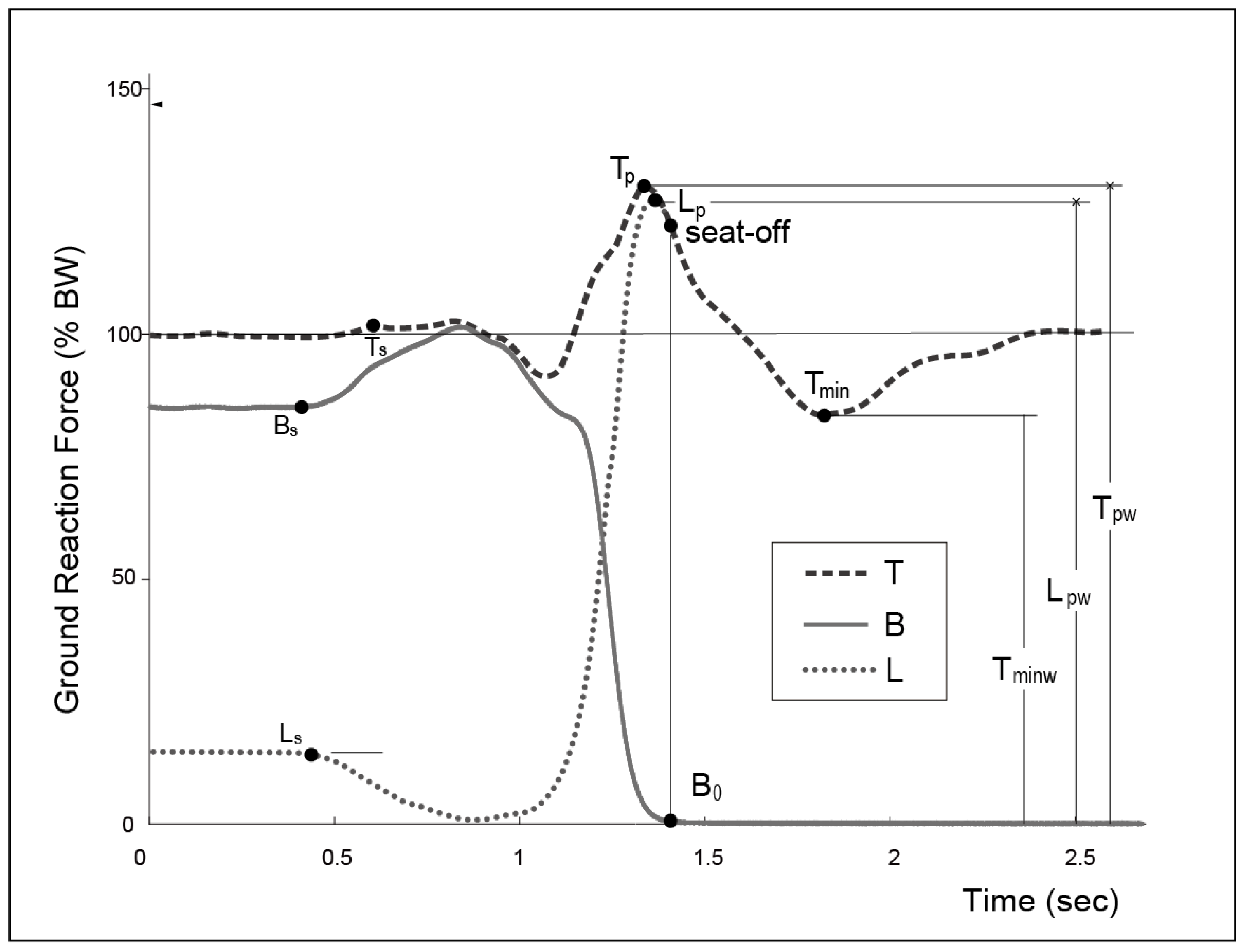
3.4. Measurements
4. Calculation Results
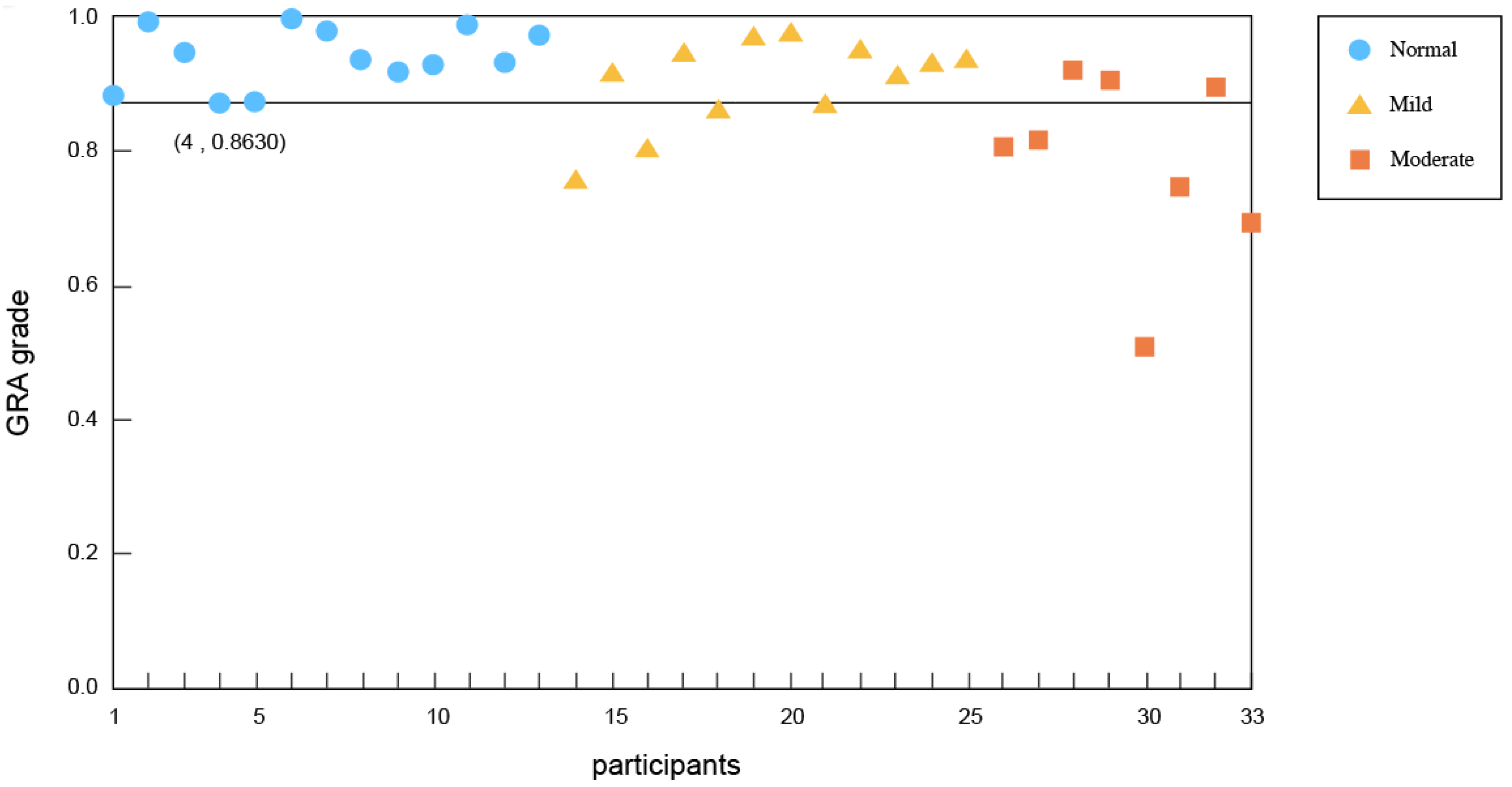
4.1. Time Factors
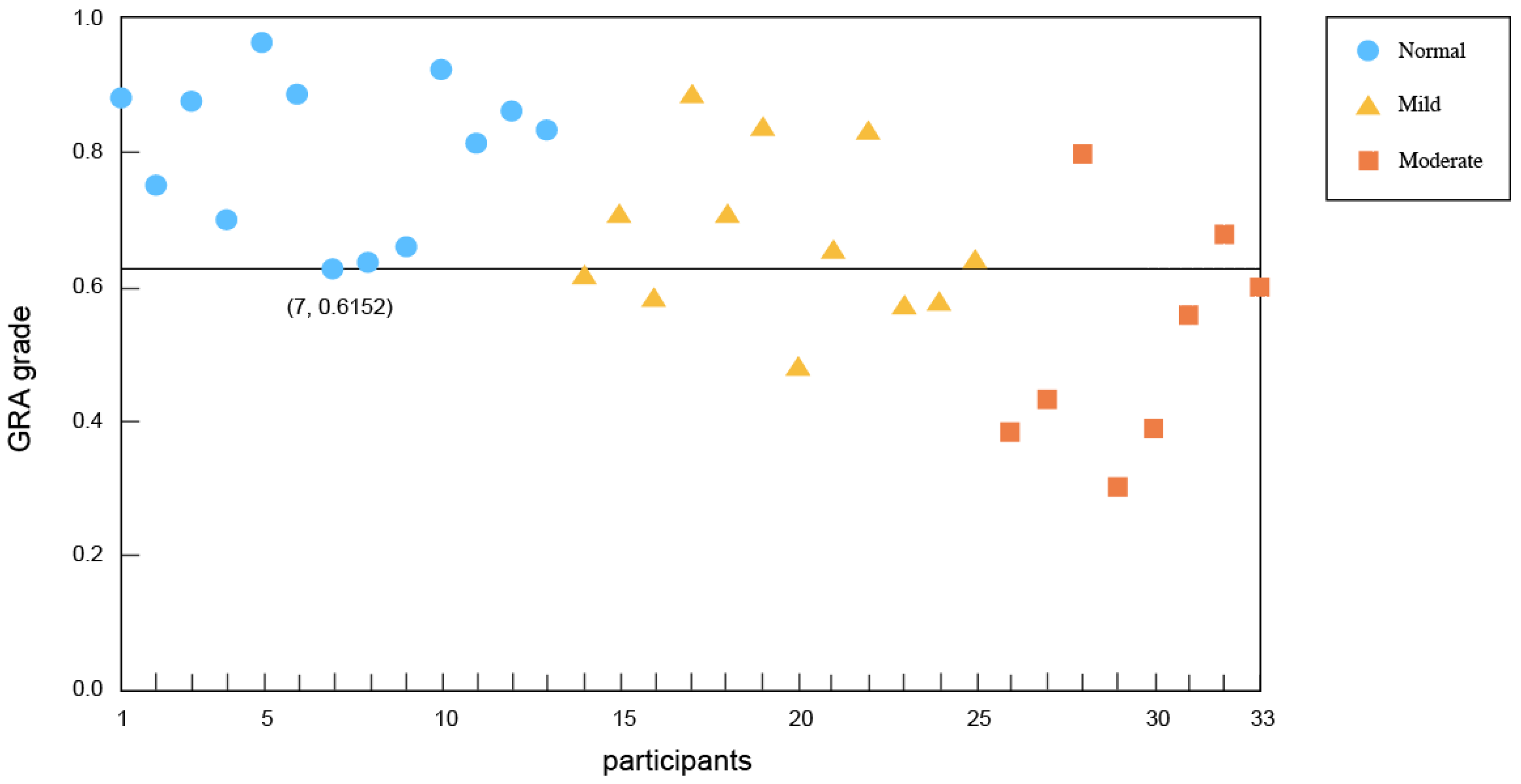
4.2. Weight Factors
5. Discussion
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- García-Soidán, J.L.; Leirós-Rodríguez, R.; Romo-Pérez, V.; García-Liñeira, J. Accelerometric Assessment of Postural Balance in Children: A Systematic Review. Diagnostics 2021, 11, 8. [Google Scholar] [CrossRef]
- Ivana, S.; Goran, N.; Srboljub, Đ. Assessment of balance in younger school age children with intellectual disability. Facta Univ. Ser. Phys. Educ. Sport 2018, 16, 687–696. [Google Scholar]
- Enkelaar, L.; Smulders, E.; van Schrojenstein Lantman-de Valk, H.; Geurts, A.C.H.; Weerdesteyn, V. A review of balance and gait capacities in relation to falls in persons with intellectual disability. Res. Dev. Disabil. 2012, 33, 291–306. [Google Scholar] [CrossRef] [PubMed]
- Giagazoglou, P.; Kokaridas, D.; Sidirropoulou, M.; Patsiaours, A.; Karra, C.; Neofotisou, K. Effects of a trampoline exercise intervention on motor performance and balabce Ability of children with intellectual disabilities. Res. Dev. Disabil. 2013, 34, 2701–2707. [Google Scholar] [CrossRef]
- Cox, C.R.; Clemson, L.; Stancliffe, R.J.; Durvasula, S.; Sherrington, C. Incidence of and risk factors for falls among adults with an intellectual disability. J. Intellect. Disabil. Res. 2010, 54, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Srikanth, R.; Cassidy, G.; Joiner, C.; Teeluckdharry, S. Osteoporosis in people with intellectual disabilities: A review and a brief study of risk factors for osteoporosis in a community sample of people with intellectual disabilities. J. Intellect. Disabil. Res. 2011, 55, 53–62. [Google Scholar] [CrossRef]
- Sherrard, J.; Tonge, B.J.; Ozanne-Smith, J. Injury in young people with intellectual disability: Descriptive epidemiology. Inj. Prev. 2001, 7, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seagraves, F.; Horvat, M.; Franklin, C.; Jones, K. Effects of a school based program on physical function and work productivity in individuals with mental retardation. Clin. Kinesiol. 2004, 58, 18–29. [Google Scholar]
- Giagazoglou, P.; Arabatzi, F.; Dipla, K.; Liga, M.; Kellis, E. Effect of a hippotherapy intervention program on static balance and strength in adolescents with intellectual disabilities. Res. Dev. Disabil. 2012, 33, 2265–2270. [Google Scholar] [CrossRef]
- Chang, C.S.; Shen, K.S.; Wang, Y.R. The study on balance for students with mental retardation in elementary school. In Proceedings of the 18th International Conference on Industrial Engineering, Seoul, Korea, 10–12 October 2016. [Google Scholar]
- Mahrokh, D.; Mehmet, G. The effect of balance training on static and dynamic balance in children with intellectual disability. J. Appl. Environ. Biol. Sci. 2015, 5, 127–131. [Google Scholar]
- Lima, C.A.; Ricci, N.A.; Nogueira, E.C.; Perracini, M.R. The Berg Balance Scale as a clinical screening tool to predict fall risk in older adults: A systematic review. Physiotherapy 2018, 104, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Mehta, T.; Young, H.-J.; Lai, B.; Wang, F.; Kim, Y.; Thirumalai, M.; Tracy, T.; Motl, R.W.; Rimmer, J.H. Comparing the Convergent and Concurrent Validity of the Dynamic Gait Index with the Berg Balance Scale in People with Multiple Sclerosis. Healthcare 2019, 7, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omana, H.; Bezaire, K.; Brady, K.; Davies, J.; Louwagie, N.; Power, S.; Santin, S.A.; Hunter, S.W. Functional Reach Test, Single-Leg Stance Test, and Tinetti Performance-Oriented Mobility Assessment for the Prediction of Falls in Older Adults: A Systematic Review. Phys. Ther. 2021, 101, pzab173. [Google Scholar] [CrossRef]
- Song, C.-Y.; Tsauo, J.-Y.; Fang, P.-H.; Fang, I.-Y.; Chang, S.-H. Physical Fitness among Community-Dwelling Older Women with and without Risk of Falling—The Taipei Study, Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 7243. [Google Scholar] [CrossRef] [PubMed]
- Larsson, B.A.M.; Johansson, L.; Johansson, H.; Axelsson, K.F.; Harvey, N.; Vandenput, L.; Magnusson, P.; McCloskey, E.; Liu, E.; Kanis, J.A.; et al. The timed up and go test predicts fracture risk in older women independently of clinical risk factors and bone mineral density. Osteoporos. Int. 2021, 32, 75–84. [Google Scholar] [CrossRef]
- Hoskens, J.; Goemans, N.; Feys, H.; De Waele, L.; Van den Hauwe, M.; Klingels, K. Normative data and percentile curves for the three-minute walk test and timed function tests in healthy Caucasian boys from 2.5 up to 6 years old. Neuromuscul. Disord. NMD 2019, 29, 585–600. [Google Scholar] [CrossRef]
- Gebel, A.; Lesinski, M.; Behm, D.G.; Granacher, U. Effects and dose–response relationship of balance training on balance performance in youth: A systematic review and meta-Analysis. Sports Med. 2018, 48, 2067–2089. [Google Scholar] [CrossRef]
- Franjoine, M.R.; Gunther, J.S.; Taylor, M.J. Pediatric balance scale: A modified version of the berg balance scale for the school-age child with mild to moderate motor impairment. Pediatr. Phys. 2003, 15, 114–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.S.; Chong, K.S.; Wu, D.C. An Exploratory Study on the Evaluation of the Intellectual Disability Children’s Balance Performance. In Proceedings of the Ergonomics Society of Taiwan 2021 Annual Meeting and Conference, Penghu, Taiwan, 18 March 2021. [Google Scholar]
- Hellec, J.; Chorin, F.; Castagnetti, A.; Colson, S.S. Sit-To-Stand Movement Evaluated Using an Inertial Measurement Unit Embedded in Smart Glasses—A Validation Study. Sensors 2020, 20, 5019. [Google Scholar] [CrossRef]
- Muñoz-Bermejo, L.; Adsuar, J.C.; Mendoza-Muñoz, M.; Barrios-Fernández, S.; Garcia-Gordillo, M.A.; Pérez-Gómez, J.; Carlos-Vivas, J. Test-Retest Reliability of Five Times Sit to Stand Test (FTSST) in Adults: A Systematic Review and Meta-Analysis. Biology 2021, 10, 510. [Google Scholar] [CrossRef]
- Chang, C.S.; Chen, W.L. Developing a rapid assessment method to estimate Berg Balance Scale score of elderly people. In Proceedings of the HCI International 2017 Conference, Vancouver, BC, Canada, 9–14 July 2017. [Google Scholar]
- Deng, J.L. Introduction to Grey System Theory. J. Grey Syst. 1989, 1, 1–24. [Google Scholar]
- Chang, C.S. Multi-Level Grey Relation Comprehensive Evaluation Method for Universal Design. J. Grey Syst. 2014, 17, 229–238. [Google Scholar]
- Fatemeh, S.; Shabnam, H.N. Improving performance evaluation based on balanced scorecard with grey relational analysis and data envelopment analysis approaches: Case study in water and wastewater companies. Eval. Program Plan. 2020, 79, 1017672. [Google Scholar]
- Hsu, P.F.; Kung, J.Y. Applying Grey Relational Analysis to select the Optimal Design Company. Int. J. Uncertain. Innov. Res. 2019, 1, 51–62. [Google Scholar]
- Zuo, W.; Li, J.; Zhang, Y.; Li, Q.; He, Z. Effects of multi-factors on comprehensive performance of a hydrogen-fueled micro-cylindrical combustor by combining grey relational analysis and analysis of variance. Energy 2020, 199, 117615. [Google Scholar] [CrossRef]
- Huang, H.C.; Tsai, T.F.; Subeq, Y.M. Using grey relational analysis and grey integrated multi-objective strategy to evaluate the risk factors of falling of aboriginal elders in Taiwan. Soft Comput. 2020, 24, 8096–8112. [Google Scholar] [CrossRef]
- Miswan, N.H.; Chan, C.S.; Ng, C.G. Hospital readmission prediction based on improved feature selection using grey relational analysis and LASSO. Grey Syst. Theory Appl. 2021, 11, 796–812. [Google Scholar] [CrossRef]
- Sun, X.L.; Hua, Z.Y.; Li, M.; Liu, L.; Xie, Z.; Lia, S.Y.; Wang, G.; Liu, F. Optimization of pollutant reduction system for controlling agricultural non-point-source pollution based on grey relational analysis combined with analytic hierarchy process. J. Environ. Manag. 2019, 243, 370–380. [Google Scholar] [CrossRef]
- Gülçin, C.; Erkan, K.; Oğuzhan, A.A. Public transportation vehicle selection by the grey relational analysis method. Public Transp. 2021, 13. [Google Scholar] [CrossRef]
- Hwang, M.H.; Hsu, H.Y.; Kung, C.Y.; Sheng, T. SuInformation Strategic Framework for Leagile Supply Chain: Grey Relational Analysis Approach. Int. J. Uncertain. Innov. Res. 2020, 2, 295–318. [Google Scholar]
- Hsu, P.F.; Kao, Y.L. Selecting Optimal Out-of-home Media Agency via AHP and GRA. Int. J. Uncertain. Innov. Res. 2021, 3, 127–142. [Google Scholar]
- Wen, K.L. Grey System Theory, 2nd ed.; Wunan Publisher: Taipei, Taiwan, 2013. [Google Scholar]
- Kralj, A.; Jaeger, R.J.; Munih, M. Analysis of standing up and sitting down in humans: Definitions and normative data presentation. J. Biomech. 1990, 23, 1123–1138. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Children Without Intellectual Disability (n = 13) | Children with Mild Intellectual Disability (n = 12) | Children with Moderate Intellectual Disability (n = 8) | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |
| Age (years) | 9.6 | 1.4 | 9.8 | 0.9 | 8.9 | 0.8 |
| Weight (kg) | 33.1 | 6.4 | 37.7 | 12.6 | 25.9 | 8.5 |
| Hight (cm) | 139.2 | 10.0 | 138.4 | 10.8 | 130.2 | 10.2 |
| BMI | 16.9 | 1.6 | 19.3 | 4.5 | 15.3 | 3.8 |
| Time Factors (Time) | |||||
|---|---|---|---|---|---|
| No. | Factors | Explanation | No. | Factors | Explanation |
| 01 | Bs–Tp | duration between Bs and Tp | 05 | Tp–Lp | duration between Tp and Lp |
| 02 | Bs–Lp | duration between Bs and Lp | 06 | Tp–seat off | duration between Tp and seat off |
| 03 | Bs–seat off | duration between Bs and seat off | 07 | Lp–seat off | duration between Lp and seatoff |
| 04 | Bs–end | duration between Bs and end | |||
| Weight Factors (Weight) | ||
|---|---|---|
| No. | Factors | Explanation |
| 01 | Tpw | The maximum ground reaction force of Curve T |
| 02 | Lpw | The maximum ground reaction force of Curve L |
| 03 | Tminw | The minimum body force during the ascending phase |
| 04 | Tpw–Tminw | The force difference between Tpw and Tminw |
| 05 | Lpw–Tminw | The force difference between Lpw and Tminw |
| Time Factors (ms) | Weight Factors | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bs–Tp | Bs–Lp | Bs–Seat off | Bs–End | Tp–Lp | Tp–Seat off | Lp–Seat off | Tpw | Lpw | Tminw | Tpw–Tminw | Lpw–Tminw | |
| 1 | 433 | 499 | 632 | 1256 | 66 | 199 | 133 | 1.30 | 1.20 | 0.77 | 0.52 | 0.43 |
| 2 | 726 | 781 | 900 | 1739 | 55 | 174 | 119 | 1.47 | 1.31 | 0.70 | 0.78 | 0.61 |
| 3 | 725 | 745 | 821 | 2034 | 20 | 96 | 76 | 1.43 | 1.41 | 0.88 | 0.55 | 0.52 |
| 4 | 1074 | 1173 | 1245 | 2135 | 99 | 171 | 72 | 1.27 | 1.12 | 0.86 | 0.40 | 0.26 |
| 5 | 1043 | 1077 | 1233 | 2204 | 34 | 190 | 156 | 1.34 | 1.30 | 0.82 | 0.51 | 0.48 |
| 6 | 732 | 794 | 927 | 1675 | 62 | 195 | 133 | 1.31 | 1.25 | 0.84 | 0.47 | 0.41 |
| 7 | 753 | 767 | 811 | 1691 | 14 | 58 | 44 | 1.52 | 1.50 | 0.76 | 0.76 | 0.74 |
| 8 | 703 | 717 | 752 | 1375 | 14 | 49 | 35 | 1.44 | 1.42 | 0.66 | 0.78 | 0.76 |
| 9 | 484 | 629 | 717 | 1481 | 145 | 233 | 88 | 1.29 | 1.21 | 0.97 | 0.32 | 0.24 |
| 10 | 904 | 999 | 1183 | 1621 | 95 | 279 | 184 | 1.34 | 1.25 | 0.74 | 0.60 | 0.50 |
| 11 | 744 | 777 | 927 | 1784 | 33 | 183 | 150 | 1.52 | 1.41 | 0.93 | 0.59 | 0.48 |
| 12 | 623 | 699 | 798 | 1213 | 76 | 175 | 99 | 1.28 | 1.20 | 0.78 | 0.50 | 0.42 |
| 13 | 820 | 874 | 896 | 1607 | 54 | 76 | 22 | 1.23 | 1.21 | 0.77 | 0.46 | 0.44 |
| Time Factors (ms) | Weight Factors | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bs–Tp | Bs–Lp | Bs–Seat off | Bs–End | Tp–Lp | Tp–Seat off | Lp–Seat off | Tpw | Lpw | Tminw | Tpw–Tminw | Lpw–Tminw | |
| 14 | 1196 | 1359 | 1495 | 2656 | 163 | 299 | 136 | 1.19 | 1.13 | 0.88 | 0.31 | 0.25 |
| 15 | 918 | 980 | 1070 | 2189 | 62 | 152 | 90 | 1.23 | 1.21 | 0.89 | 0.34 | 0.32 |
| 16 | 1255 | 1315 | 1448 | 2388 | 60 | 193 | 133 | 1.20 | 1.16 | 0.93 | 0.27 | 0.23 |
| 17 | 885 | 903 | 1046 | 1921 | 18 | 161 | 143 | 1.33 | 1.30 | 0.72 | 0.61 | 0.58 |
| 18 | 1057 | 1089 | 1193 | 2421 | 32 | 136 | 104 | 1.18 | 1.15 | 0.81 | 0.36 | 0.33 |
| 19 | 697 | 817 | 879 | 1485 | 120 | 182 | 62 | 1.24 | 1.19 | 0.74 | 0.50 | 0.45 |
| 20 | 841 | 873 | 952 | 1638 | 32 | 111 | 79 | 1.10 | 1.08 | 0.89 | 0.21 | 0.19 |
| 21 | 1033 | 1096 | 1210 | 2289 | 63 | 177 | 114 | 1.17 | 1.11 | 0.83 | 0.35 | 0.29 |
| 22 | 885 | 929 | 1045 | 1914 | 44 | 160 | 116 | 1.26 | 1.23 | 0.83 | 0.43 | 0.40 |
| 23 | 946 | 1127 | 1217 | 1713 | 181 | 271 | 90 | 1.22 | 1.13 | 0.93 | 0.28 | 0.20 |
| 24 | 861 | 885 | 977 | 2189 | 24 | 116 | 92 | 1.20 | 1.19 | 0.96 | 0.24 | 0.23 |
| 25 | 902 | 978 | 1081 | 1948 | 76 | 179 | 103 | 1.28 | 1.16 | 0.95 | 0.34 | 0.22 |
| Time Factors (ms) | Weight Factors | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bs–Tp | Bs–Lp | Bs–Seat off | Bs–End | Tp–Lp | Tp–Seat off | Lp–Seat off | Tpw | Lpw | Tminw | Tpw–Tminw | Lpw–Tminw | |
| 26 | 497 | 777 | 814 | 3085 | 280 | 317 | 37 | 1.06 | 1.03 | 0.90 | 0.16 | 0.13 |
| 27 | 1041 | 1124 | 1269 | 2754 | 83 | 228 | 145 | 1.12 | 1.09 | 0.94 | 0.18 | 0.14 |
| 28 | 972 | 1039 | 1160 | 1439 | 67 | 188 | 121 | 1.22 | 1.16 | 0.65 | 0.58 | 0.51 |
| 29 | 574 | 803 | 1079 | 1775 | 229 | 505 | 276 | 1.06 | 0.94 | 0.91 | 0.16 | 0.04 |
| 30 | 1851 | 2017 | 2218 | 3301 | 166 | 367 | 201 | 1.10 | 0.90 | 0.84 | 0.26 | 0.06 |
| 31 | 1154 | 1290 | 1375 | 3095 | 136 | 221 | 85 | 1.11 | 1.04 | 0.81 | 0.30 | 0.23 |
| 32 | 577 | 604 | 763 | 1082 | 27 | 186 | 159 | 1.21 | 1.19 | 0.56 | 0.65 | 0.63 |
| 33 | 1517 | 1602 | 1747 | 2666 | 85 | 230 | 145 | 1.15 | 1.10 | 0.84 | 0.30 | 0.26 |
| No. | Grey Relational Grade | No. | Grey Relational Grade | No. | Grey Relational Grade |
|---|---|---|---|---|---|
| x1 | 0.876104 | x15 | 0.909550 | x29 | 0.899785 |
| x2 | 0.985806 | x16 | 0.795669 | x30 | 0.502607 |
| x3 | 0.941580 | x17 | 0.939427 | x31 | 0.743228 |
| x4 | 0.863041 | x18 | 0.853622 | x32 | 0.890893 |
| x5 | 0.866535 | x19 | 0.964177 | x33 | 0.690029 |
| x6 | 0.989125 | x20 | 0.970895 | ||
| x7 | 0.968267 | x21 | 0.866975 | ||
| x8 | 0.927481 | x22 | 0.942596 | ||
| x9 | 0.911080 | x23 | 0.903536 | ||
| x10 | 0.920046 | x24 | 0.925307 | ||
| x11 | 0.977166 | x25 | 0.929919 | ||
| x12 | 0.925165 | x26 | 0.803517 | ||
| x13 | 0.966067 | x27 | 0.808698 | ||
| x14 | 0.750596 | x28 | 0.912563 |
| No. | Grey Relational Grade | No. | Grey Relational Grade | No. | Grey Relational Grade |
|---|---|---|---|---|---|
| x1 | 0.8753 | x15 | 0.6995 | x29 | 0.2879 |
| x2 | 0.7420 | x16 | 0.5694 | x30 | 0.3733 |
| x3 | 0.8676 | x17 | 0.8785 | x31 | 0.5442 |
| x4 | 0.6888 | x18 | 0.6964 | x32 | 0.6681 |
| x5 | 0.9560 | x19 | 0.8309 | x33 | 0.5903 |
| x6 | 0.8778 | x20 | 0.4673 | ||
| x7 | 0.6153 | x21 | 0.6455 | ||
| x8 | 0.6258 | x22 | 0.8226 | ||
| x9 | 0.6493 | x23 | 0.5610 | ||
| x10 | 0.9163 | x24 | 0.5637 | ||
| x11 | 0.8071 | x25 | 0.6274 | ||
| x12 | 0.8537 | x26 | 0.3680 | ||
| x13 | 0.8235 | x27 | 0.4199 | ||
| x14 | 0.6051 | x28 | 0.7889 |
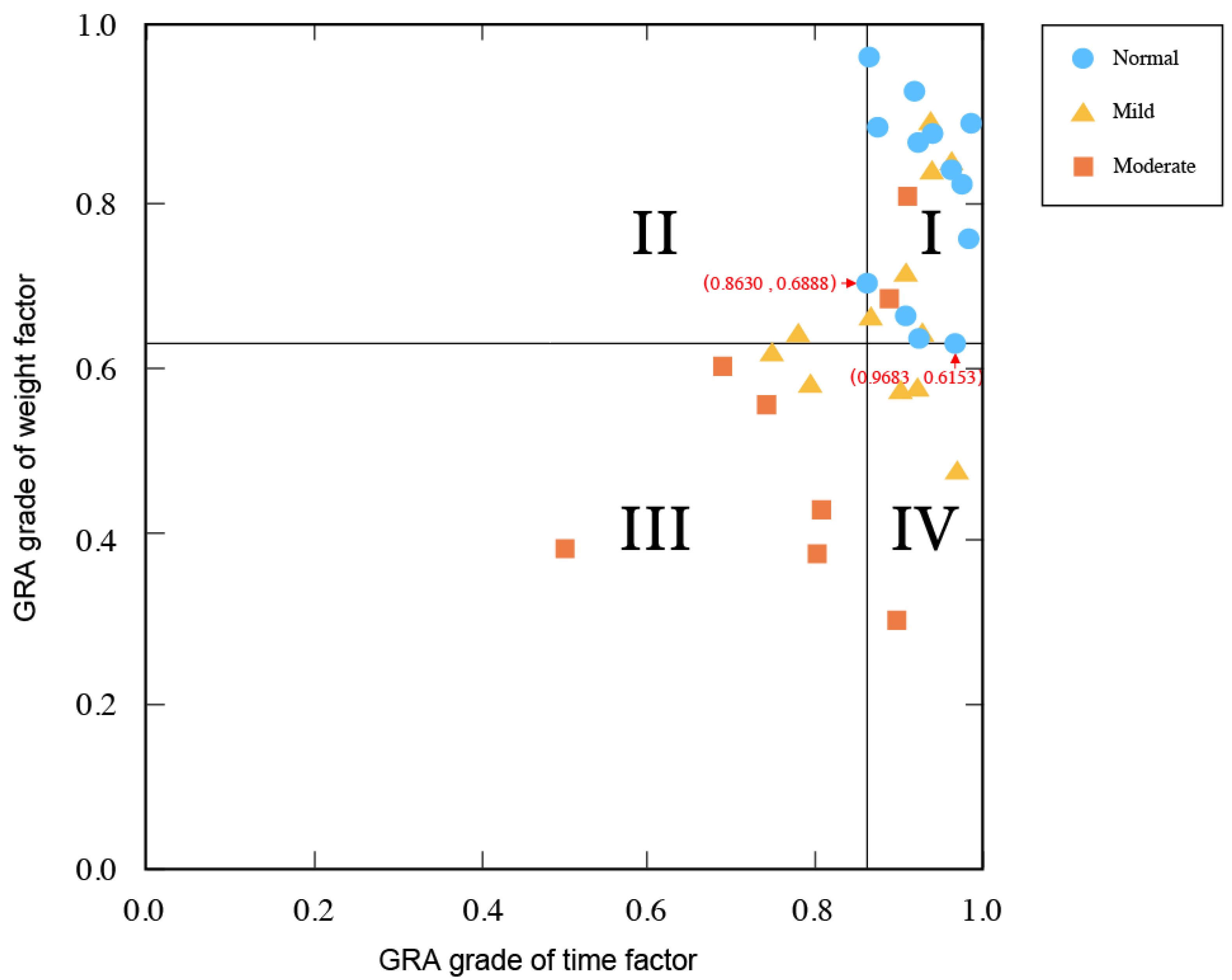
| Children Without Intellectual Disability | Children with Mild Intellectual Disability | Children with Moderate Intellectual Disability | |
|---|---|---|---|
| I | 100.0% | 50.0% | 25.0% |
| II | 0% | 8.3% | 0% |
| III | 0% | 16.7% | 62.5% |
| IV | 0% | 25.0% | 12.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-S. Applying Grey Relational Analysis in the Evaluation of the Balance of Children with Intellectual Disability. Axioms 2021, 10, 341. https://doi.org/10.3390/axioms10040341
Chang C-S. Applying Grey Relational Analysis in the Evaluation of the Balance of Children with Intellectual Disability. Axioms. 2021; 10(4):341. https://doi.org/10.3390/axioms10040341
Chicago/Turabian StyleChang, Chih-Sheng. 2021. "Applying Grey Relational Analysis in the Evaluation of the Balance of Children with Intellectual Disability" Axioms 10, no. 4: 341. https://doi.org/10.3390/axioms10040341
APA StyleChang, C.-S. (2021). Applying Grey Relational Analysis in the Evaluation of the Balance of Children with Intellectual Disability. Axioms, 10(4), 341. https://doi.org/10.3390/axioms10040341