Abstract
This article describes a medical device uses precisely generated vibrations to obtain genetic material (sperm) in injured men, tetraplegics, and paraplegics. A significant advantage is the absence of general anesthesia of the patient. The DC motor of a medical device works with a safe voltage powered by rechargeable or AA cells. The principle of generation of vibration is a crank mechanism. Rotation of the flywheel is converted to rectilinear reciprocating motion. The amplitude is set in the range between 1–4 mm and the frequency is controlled by the RPM of the DC motor. If the stimulation will be followed preciously with the methodology, the process will be completed within 12 min from the beginning of stimulation. The success rate of the device is in the range between 65–85% depending on the patient’s condition and the extent of the spinal cord lesion. The measurement of sinusoidal oscillations was performed by using a stand in which the device was mounted. The amplitude was measured with an accelerometer and then mathematically converted by software Matlab and MS-Excel to the magnitude of the deviation in mm. Measurements have shown that the proposed design meets the requirements for amplitude and frequency.
1. Introduction
According to multiple professional medical journals, human reproduction has encountered some problems, especially in terms of the decrease of sperm quality. This issue has been observed since the 19702010039s. Busy and stressful lifestyles as well as separation from traditional life and nature have been associated with this decline. In the last century, 60 million was considered the average amount of mobile sperm for males. Currently, the standard values of spermiogram are based on the 2010 norm according to WHO (World Health Organization)—volume—1.5 mL and more; pH: 7.2 and more; concentration: At least 15 million per 1 mL of the semen—total at least 39 million; mobility—minimally 40% of mobile sperm and 32% of progressively moving sperm; and morphology: Minimally 4% of the normal build. The transport of the semen into the Centre of Assisted Reproduction (CAR) must be done within an hour [1].
In the Czech Republic, on average 150–200 people fall victim to a spinal cord injury every year and a third of these are women. The most common mechanisms of injury are a car accident and falling from height [2]. From the severity perspective, it is the priority group of patients who require long-term medical care and rehabilitation, the complex approach of various professionals and specialists such as a traumatologist, neurologist, urologist, intern, rehabilitation physician, sexologist, and psychologist. Patients with a spinal cord injury are treated by spinal units, which are part of traumacentres. At the moment there are four spinal units in the Czech Republic located in Prague, Liberec, Ostrava, and Brno. The first step in treatment is a surgical decompression of the spinal cord. On the first postsurgery day, the process of complex rehabilitation and resocialisation begins. The rehabilitation of the paralysed patients continues in the rehabilitation centres and their goal is full adaptation to a wheelchair, acceptance of permanent disability, and return to family, work, and social life. In regard to the care of disabled patients, the financial costs are high, especially in the first year following injury. The lifelong expenses of a man who has become disabled at the age of 25 can go beyond 20 million Czech crowns [1,3,4]. Sexual dysfunction, sexual life, and reproduction are affected by spinal injury. The disabled patients suffer from erectile dysfunction (ED) and the condition is also connected with the change of erogenous zones, non-ejaculation with the absence of orgasm, or the change of quality of orgasm, spermatogenesis disorder, endocrine dysfunction, lowered libido, and decrease or loss of sexual satisfaction. Sexual desire is decreased by the injury and that leads to a lower frequency of sexual intercourses ranging from one per week to one per month. Erogenous zones change, and while the penis loses its dominant role as opposed to in a healthy male individual, areas with preserved sensitivity such as nipples, ear lobes, nape, and mouth become more prominent. The nature of an orgasm changes as it is not accompanied by ejaculation. A number of males describe it as a pressure in their head. Some paraplegics are able to evoke orgasm-like feelings preceding the injury, which is called a ‘psychogenic orgasm’ and the orgasm experienced simultaneously with the partner is called a ‘para-orgasm’ [2,3,4,5].
Nowadays, two of the most common and successful methods of retrieving sperm from disabled males are rectal electrostimulation and vibrostimulation. Prior to vibrostimulation or electrostimulation, the patient is thoroughly informed after which they sign the consent of acknowledgment [4]. Vibrostimulation, penile vibrostimulation (PVS) is recommended in the first line of retrieval of sperm from men with postinjury non-ejaculation. Using a penile vibrator is successful with men with a lesion segment T8 of the spinal cord. Technical parameters of the device are as follows: Reachable frequency 100 Hz and amplitude 2.5 mm. Vibrostimulation is performed while sitting down in a wheelchair. The vibrostimulator is placed on the glans or frenulum of the penis. Stimulation takes between a 2–3 min to 1–2 min intermission but the maximum number of repetitions is three. Ejaculation tends to be accompanied by spasms of the abdominal and lower limb muscles. Contraindications of PVS could be skin inflammatory changes on the penis, uncorrected hypertension, heart disorders, and a high risk of onset of autonomous dysreflexia. For some time after the injury (less than 18 months), patients tend to have problems to achieve ejaculation using PVS, which is considered noninvasive compared to electro-ejaculation. PVS is a preferred method by the patients as couples can use it for home insemination.
2. Experimental Section
An electrodynamic vibrator would probably be the most suitable solution [6]. However, the market does not offer a suitable type and size of the vibrator, which could be used in this case. If we were focusing on the development and production of the electrodynamic solution in its miniature version, it would be pointless without serial manufacturing. Another way to stimulate nerve endings via vibration is using a piezoelectric vibrator. This solution may first appear as optimal and final. On the other hand, because of its construction this kind of generator is not capable of reaching the required deviations (amplitude) in the 1–4 mm range. The crank mechanism construction then appears to be the optimal choice. While using the crank mechanism, it is possible to reach great accuracy with the set amplitude, which corresponds with the specified conditions in the 1–4 mm range. The amplitude is controlled by the eccentricity of the connecting rod pin from the rotating axis of the flywheels and frequency as well as by the spin speed of the electromotor [7]. To maintain the specified conditions, the design of the device was presented in five variants, while every variant had a different eccentricity, which corresponded to the 1–5 mm amplitude. All parts of the device were checked by the numeric calculation. The crank mechanism Figure 1. was checked by calculation on testing the stresses, bearing, and bruising of the connecting rod and pins. The maximum applied force on the stimulating plate is 10 N (Figure 2) and because of this negligible force, detailed calculations were not carried out Figure 3. [8].
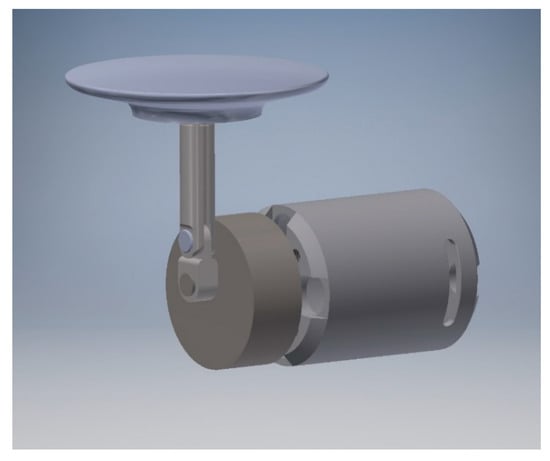
Figure 1.
Crank mechanism of the vibration generator.
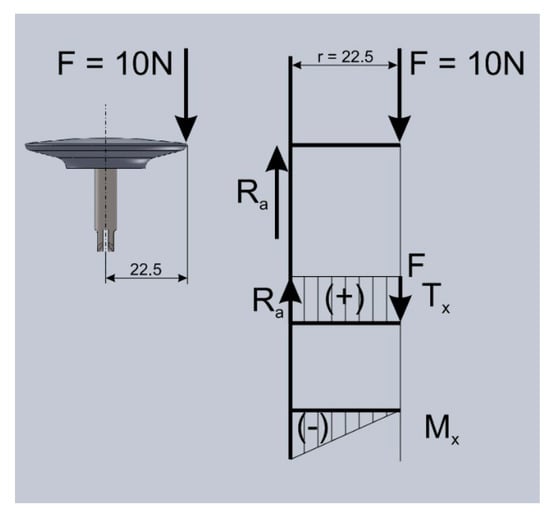
Figure 2.
Analysis of the applied forces.
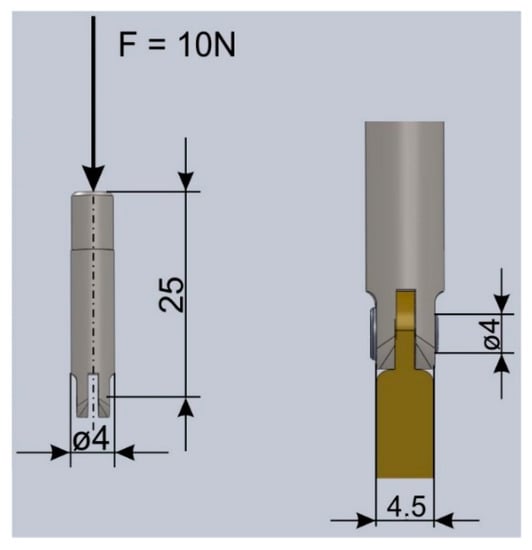
Figure 3.
Bearing calculations of the connecting rod and cutting and bruising test of the pin.
Calculation of critical force in Figure 2:
where: Fkr—critical force at the stress rupture (N), E—tensile modulus (MPa), lred—reduced length of the rod (m), and Jmin—quadratic module of the cross-section—(smallest) (m3)
The calculation matched the requirements: The operational value is 13,265 times lower than the critical pressure.
The test of the pin cutting on two levels is:
The calculation matched the requirements. The operational value is 48 times lower than the critical pressure.
The bruising test of the pin with the fork is:
The calculation matched the requirements. The operational value is 19 times lower than the critical pressure.
The bruising test of the pin of the connecting rod is:
The calculation matched the requirements. The operational value is 131,250,000 times lower than the critical pressure.
The dimensions calculation of the medical device was derived from the dimensions of the electromotor and the wall thickness of the device.
where is: Dem—diameter of the electromotor (mm), and tt—wall thickness of the device (mm)
The body of the device must be able to function even with mechanical stresses caused by vibrations. A PLA plastic type was used as the designed material for the prototype of the device. PLA is a biologically degradable plastic as a result of its natural origin from corn, sugar cane, or potatoes. In regard to longevity of the device, materials such as PET or PETG would be more suitable material solutions for the prototype since they are able to withstand greater mechanical stresses. However, since the focus is to verify the functionality of the device, it is not necessary to concentrate on the slight mechanical differences of the materials of the prototype.
3. Results
The body of the medical device was designed in a way that it would withstand the vibrations generated by the device and fall from common heights to 1.5 m above the ground [9]. The biodegradable plastic PLA was used to create the prototype with regard to the environment. The strength of this plastic is that it is able to withstand the testing needs of the prototype.
The calculation presents the bulkiness of the crank mechanism with safety and technological reserves with the sum of the length of the electromotor, electronics, and accumulators.
where: Lkm—length of the crank mechanism including technological and safety reserves (mm), Lem—length of the electromotor (mm), Le—length of the electronics (mm), La—length of the accumulators (mm), and tt—wall thickness of the device (mm)
Regarding the current consumption of the electromotor (current draw), an accumulator with hard discharging characteristics was designed. A LiFe (lithium–iron–phosphate) accumulator type was chosen because of its reliability and lifespan. It does not have any deficiencies compared to its predecessors and offers a bigger capacity with smaller dimensions.
The main task of controlling electronics is to secure the flawless operation of the device both without any load and under load while being applied to the patient. The next task is to inform the staff of the charging state of the accumulator, its overload, forced cessation of the device, or overheating of the motor [7]. The electronics of the device were designed so that the crank mechanism with the connected electromotor was able to maintain the set parameters under stress within the frequency range of 60–120 Hz (i.e., 4800–7200 RPM). The frequency is adjustable within 5 Hz steps [10]. The last function of the controlling electronics is inductive charging. The device was designed to be resistant to gushing water, in other words, IP coverage-protected from gushing water. Water is rushed through a 6.3 mm jet at all angles with a flow of 12.5 L per min and with a pressure of 30 kN/m2 for at least three minutes from a three-metre distance [11]. The controlling electronics contain an inductive part for accumulator charging, which means the device was designed for contactless inductive charging. The charging is signalled by a green LED diode, which flashes during charging and as soon as the charging process is finished, it shines green. For the experimental measuring, a simpler and, most importantly, cheaper model of the controlling electronics was developed. This model retroactively checks the speed of the electromotor. The frequency or speed is set by using a calibrated potentiometer and there is a scale on the body of the device for setting an accurate frequency. After being switched on, the electromotor maintains a constant set speed with or without a load on the device [7].
The controlling electronics of the medical device have the following properties: Dimensions of 55 × 27 mm; power supply of 5–12 V; and nominal voltage of the motor of 7.2 V. The regulated current is applied by using a power transistor with a cooler (max. 8 A, short-term 20 A) as shown in Figure 4 and Figure 5.
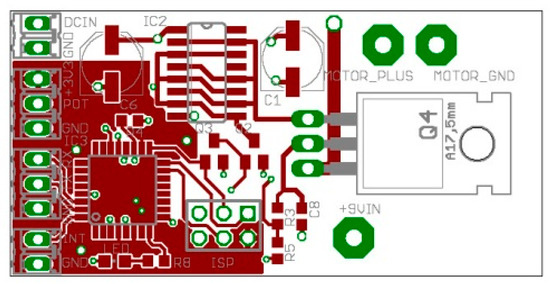
Figure 4.
Controlling electronics of the medical device FertEx CM—design of the printed connection.
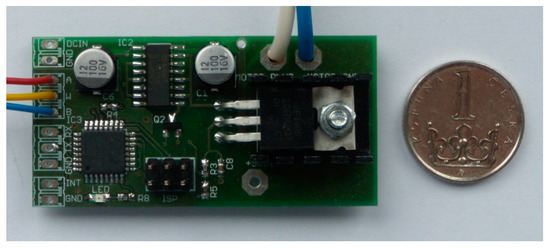
Figure 5.
Controlling electronics of the medical device FertEx CM—stocking with components.
After considering the aspects of the available electromotors in this category, an electronically switched (brushless) electromotor was designed. The reason for this choice was its affordability, lifespan, and sparkles operation, which could otherwise cause the disruption of some electronic medical devices. The price of the electronically switched electromotor is from five to 10 times higher than of a standard commutator electromotor, but the price is balanced out by its reliability and longer lifespan. From the available motors, the SPEED 500 or SPEED 400 series of electromotors can be considered. The comparison of the measured values of the current draw of the mentioned models is presented in Table 1, Table 2 and Table 3. Based on the measurements listed below, it is apparent that the SPEED 400 series electromotor was picked as optimal. Its parameters, namely, its output and current draw, fully satisfy the requirements demanded by the device.

Table 1.
Results of the measurement of the current draw of the electromotor—measured without load on the device: Messcontrol M–3800 (S/N: 225767), powered by a laboratory stabilised source (S/N: 2584).
Table 2.
Comparison of advantages and disadvantages of a medical device FertEx CM.
Table 3.
Comparison of advantages and disadvantages of FertEx CM and similar devices available on the market.
The crank mechanism method was verified in the laboratory with regard to patient safety and the emergence of own frequency or resonate. With experimental measurements, the maximum values of amplitude at frequency were found. DC engine was powered by a stabilized source and were measured engine RPM, the electric current (A), and frequency (Hz). After complete measuring, data were recalculated and placed through conversion by software Matlab for a verification of amplitude in (mm). Using the same software, the data was published on graphs as shown in Figure 6, Figure 7 and Figure 8.
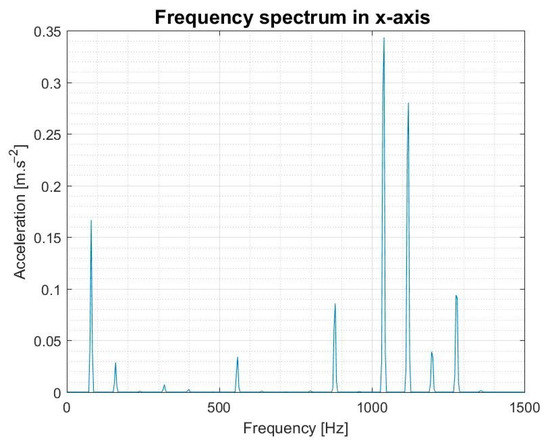
Figure 6.
Acceleration in the x direction-measurements at 4800 RPM was to achieve the maximum acceleration value of 0.3549 m/s2 in frequency 1040 Hz and 4800 RPM of the DC engine. This measurement shows that neither resonance nor natural frequency occurs.
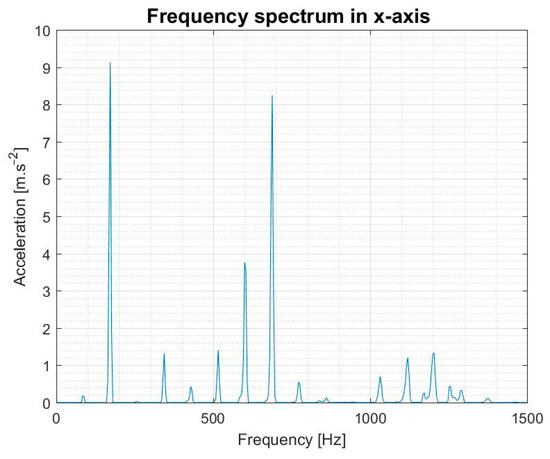
Figure 7.
Acceleration in the x direction—measurements at 5160 RPM was to achieve the maximum of acceleration value of 9.1390 m/s2 in frequency 172 Hz in 5160 RPM of the DC engine. This measurement shows that neither resonance nor natural frequency occurs.
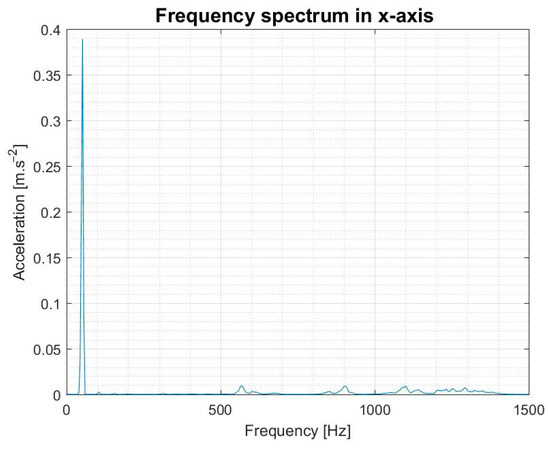
Figure 8.
Acceleration in the x direction—measurements at 3060 RPM was to achieve the maximum of acceleration value of 0.3892 m/s2 in frequency 52 Hz in 3060 RPM of DC engine. This measurement shows that neither resonance nor natural frequency occurs.
4. Discussion
The most important feature of the designed device FertEx CM for PVS is the option to safely retrieve sperm from paralysed males and the option to have their own biological offspring. This obtaining is also possible to do at home after a doctor evaluation. The retrieved sperm is then required to be transported by CAR. Another possibility is to impregnate the partner immediately after by using a ‘Baby made home’ method (artificial insemination), when the partner inserts the semen into her vagina.
Based on experience, the spermiological parameters and especially sperm mobility are better when obtaining PVS. PVS is recommended in the first line for sperm retrieval for males with postinjury non-ejaculation. Use of the penile vibrator is successful with men with a lesion above a T8 segment of the spinal cord. Rectal electrostimulation and electroejaculation (EEJ) are other techniques for sperm obtained from a paralysed patient. The principle of electroejaculation is to induce reflective ejaculation while using an alternating current of voltage up to 15 V with paraplegics and up to 5 V with tetraplegics; the current ranges between 100–600 mA [3]. PVS appears as a safer and less demanding method for the patient.
The current market offers other variants of the PVS device: FertiCare and FertiCare 2, or Viberect- Penile vibrator/stimulator. The competitive devices, however, do not allow a precise amplitude setting and electronic maintenance of the set frequency. The designed device FertEx CM also provides an interface for recording one’s heart rate and blood pressure for a potential cessation of the procedure before any succeeding complications could be observed. Another advantage of the FertEx CM PVS device is the continuous storing of information of the selected mode of stimulation. The data obtained this way can be later analysed or imported into the patient’s database for further use. Devices of this nature are not currently available on the market. In a similar device operating on a similar principle, production was discontinued and replaced by a less effective device that stimulates nerve endings on both sides. Thanks to this step, the demand on the Czech market has increased significantly and doctors are practically waiting for the development of the FertEx CM device to be completed.
When designing the solution, the safety of the patient was the highest priority and both the prevention of the mechanical and electric malfunction of the device were taken into account. The basic technical requirements were: Reaching the maximum load of 10 N, securing the amplitude with a 1–4 mm range and oscillation frequency between 60–120 Hz, and maintaining the selection of a safe electric power source, which is a source with a direct current of 5–12 V voltage [12]. Other technical requirements were the possibility of wireless inductive charging and securing compliance with the electric norm stated by the ordinance about electric devices. The final requirement was to secure the watertight integrity corresponding with the integrity of the device in 5 metres depth and controlling functions of the device regarding the priority of securing the safety of the patient [13]. The construction of the device complies with the set requirements for the construction of medical devices according to the EU norm. The mechanical parts of the device were checked by numerical calculations for stress, cutting, pressure, thrust, and bruising. Considering the very insignificant applied forces, it was verified by a second calculation check and the device complied with the mentioned kinds of load. Charging was provided by a secure direct electric source, the accumulator, which can be charged repeatedly. The type of accumulator has a long lifespan and does not have a memory effect. The electronics which are in charge of the automatic device control were designed regarding the safety of the patient. The body of the medical device met the requirements for the mechanical load by vibrations generated by the device and the lifespan of the prototype [6]. The protection against foreign elements and water was solved so that it is possible to wash the device under running water without danger of water contamination, which could subsequently damage the electronic parts. The device is protected from overload, in other words against misapplication and a violent cessation of the electronic nondestructive protection, which in case of malfunction would safely disconnect the power supply without endangering the patient.
5. Conclusions
Penile vibrostimulation is a safe and efficient method for sperm retrieval from males with a spinal cord injury. The designed device for PVS offers a higher range of amplitudes and frequency vibrations in all five variants of the constructional solutions. In regard to the serial manufacturing of the device, feedback from the patient is assumed while being stimulated, and the electronics are therefore designed with an option to connect blood pressure and heart rate monitoring. In case of recording nonstandard values, it is then possible to prevent the development of autonomous dysreflexia or other complications while using the device. After that, there is always an emergency cessation of the device and an alarm alert. The course of the stimulation is automatically recorded into the memory of the device for further data analysis or the patient’s database information for doctors. Data transfer is done by a Bluetooth standard or by a USB cable. It is safe to state that low production costs and a more affordable device are achieved by the designed vibration mechanism [4,6,7,14].
Technical parameters of the FertEX CM device are as follows in Figure 9—reachable frequency 60–120 Hz and amplitude 1–5 mm; charging from a safe source from built-in accumulator; recording of the course during stimulation into the memory of the device; emergency cessation and alarm alert functions; Bluetooth or USB data transfer; and watertight integrity to the depth of 5 m.
Figure 9.
Final form of the body of the device called FertEx CM.
Author Contributions
Investigation, A.S.; Supervision, M.C. and T.Š. T.Š.: All medical contributions based on her research, professional practice and experience of a doctor at the Faculty Hospital in Brno in the Czech Republic. M.C.: Technical experience mentioned in the introduction of the article based on his professional practice of the University of Defense in Brno in the Czech Republic and the Army of the Czech Republic. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Statistics 2010. Available online: https://www.who.int/whosis/whostat/2010/en/ (accessed on 30 December 2020).
- Sramkova, T.; Fajtova, R. Sex life after Spinal Cord Injury. In Handbook of Spinal Cord Injuries: Types, Treatments and Prognosis; Berkovsky, T.C., Ed.; Nova Science Publishers: New York, NY, USA, 2010; pp. 133–166. [Google Scholar]
- Šrámková, T. Andrological care of a patient after spinal cord trauma. Urol. Pract. 2019, 20, 85–88. [Google Scholar]
- Šrámková, T. Poruchy Sexuality u Somatických Onemocnění a Jejich Léčba; Grada-Publishing: Prague, Czech Republic, 2013; pp. 140–156. [Google Scholar]
- Anderson, R.E.; Moses, R.; Lenherr, S.; Hotaling, J.M.; Myers, J. Spinal cord injury and male infertility–A review of current literature, knowledge gaps, and future research. Transl. Androl. Urol. 2018, 7, S373–S382. [Google Scholar] [CrossRef] [PubMed]
- Benaroya, H. Mechanical Vibration, 3rd ed.; Marcel Dekker: New York, NY, USA; CRC Press: Boca Raton, FL, USA, 2004. [Google Scholar]
- Vejrosta, V. Konstrukce Zdravotnických Přístrojů; Česká Společnost pro Zdravotnickou Techniku: Staré Město, Czech Republic, 1995. [Google Scholar]
- Juliš, K.; Brepta, R. Mechanika I.–Statika a Kinematika; SNTL: Prague, Czechoslovakia, 1986. [Google Scholar]
- Svoboda, A. Mechanický Přístroj pro Stimulaci Nervových Drah. Ph.D. Thesis, Univerzita Jana Evangelisty Purkyně v Ústí nad Labem, Ústí nad Labem-město, Czech Republic, 2015. [Google Scholar]
- Dejl, Z. Konstrukce Strojů a Zařízení I. Spoje; Montanex: Ostrava, Czech Republic, 2000. [Google Scholar]
- Degree of Protection IP–Water Protection and Penetration of Objects. Available online: https://www.nemaenclosures.com/blog/ingress-protection-ratings/ (accessed on 30 December 2020).
- Sapieta, M.; Šulka, P.; Svoboda, M. Using a numerical model to verification of thermoelastic analysis of flat specimen. Manuf. Technol. 2018, 18, 482–486. [Google Scholar] [CrossRef]
- Bittner, V.; Tuček, R.; Panská, Š.; Svoboda, M.; Jelen, K. Using the fourier transform in the analysis of vibration load tests of heterogeneous mechanical systems. Manuf. Technol. 2017, 17, 836–841. [Google Scholar] [CrossRef]
- Durga, A.; Sepahpanah, F.; Regozzi, M.; Hastings, J.; Crane, D.A. Prevalence of Testosterone Deficiency After Spinal Cord Injury. PM&R 2011, 3, 929–932. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).