Abstract
Illness and poverty have been identified to be mutually influential, thereby forming a vicious cycle. Cutting off this vicious circle will be of great significance in the long-term planning of rural poverty reduction. Most of the existing studies have been conducted in proposing medical policies. Thus, these policies neglect the ability of the poor themselves. In oasis agricultural areas, the land is the critical resource, and improving land-use efficiency has been proposed as the key entry point for breaking the vicious cycle of poverty and illness. This article summarizes the success achieved in fighting health-related poverty in South Xinjiang, China, which can be attributed to a three-pronged approach that addresses the construction of the living, production, and ecological spaces. (1) Construction of the living space should be the first step in breaking the vicious cycle of poverty and illness since it can improve the medical and basic living infrastructure. (2) Construction of the production space is critical for breaking the vicious cycle since it can directly increase the income of the poor. Specifically, the profit can be improved by increasing crop yields, developing animal husbandry, and participating in land circulation and rural cooperatives. Additionally, the construction of township enterprises can provide employment to the poor. (3) In regard to the construction of the ecological space, preventing and controlling desertification, as well as renovating the village environment, is essential for providing a good living environment that is conducive to the improvement of physical fitness. Constructing the multi-spaces of “living–production–ecological” has important implications in terms of transforming the vicious cycle into a virtuous one, which is crucial for designing national poverty reduction policies.
1. Introduction
Poverty has been a worldwide problem, especially in developing countries [1,2,3]. Ending poverty in all its forms everywhere is the first goal of the 17 Sustainable Development Goals (SDGs) of the United Nations 2030 Agenda [4]. The situation worsens further when poverty is accompanied by illness because illness and poverty are interconnected—each a cause for and a consequence of the other. Specifically, poor households are particularly vulnerable to illnesses, and illness aggravates poverty by increasing the cost of treatment and decreasing the income. An illness affects both the individual and the household, and it may have repercussions for the wider community. This link has been eloquently documented in the positive correlation between poverty and illness, which revealed that good physical and mental health is essential for effective production as well as life [5].
The current policy for improving the lives of poor people suffering from an illness has been studied in the existing literature. In general, three main research agendas have been followed in previous studies. First, most of the literature focused on designing policies by controlling certain diseases, such as HIV [6], AIDS [7], malaria [8], and breast cancer [9], since those serious diseases can lead to huge disasters for one family. Moreover, WHO favors the utilization of the services of family health nurses as a means of controlling the sequelae of poverty [10]. Second, strategies were also formulated from the employment perspective [11,12]. Third, the examination of the policies from other surrounding perspectives such as educational inequities also suggested that the issue of poverty should be addressed [13,14]. Most of the policies were proposed from either the medical or the social support perspective. For instance, by proposing a policy from a single medical view, the support program assumed that people with illnesses cannot work instead of helping and encouraging the poor with illnesses to use their abilities to get rid of poverty. However, considering the challenges caused by the intersection of poverty and illness, no single force can help extract the poor from an illness-induced poverty cycle. Only policies and interventions that take into account all the components can control the sequelae of illness-induced poverty.
Most of the poverty-stricken counties in China are concentrated in the mountainous areas, border areas, and minority areas, and the communities residing in these areas depend on land for their wealth creation [15]. In the case of oasis agricultural areas, land use is an even more important factor for rural social and economic development [16]. In recent years, oasis agricultural areas have witnessed one of the most transformative trends of converting cultivated land to multi-functional landscapes. For instance, many projects proposed by the local government have attempted to improve the land-use profits, which has assisted the poor with illness in increasing their income. Despite the spectacular progress in reducing health-related poverty achieved by these projects, the intervention strategies have not been comprehensively documented.
There is a lacuna of research on the impact of land use on health-related poverty in oasis agricultural areas. The knowledge gap has prevented a complete understanding of how to break the vicious cycle of illness and poverty in oasis agricultural areas. In this context, this study selected South Xinjiang, China to acquire a deeper understanding of the role of land use in solving the issues of health-related poverty in oasis agricultural areas. The paper is divided into four sections. The Section 2 introduces the methodology applied in this analysis where the characteristics of the study area, method, and data source are addressed. The Section 3 outlines different definitions of poverty and addresses how the vicious cycle of poverty and illness presents itself in the study area. The Section 4 presents the empirical evidence of breaking the vicious cycle of illness and poverty in the study area. Then, the theoretical base is summarized at the end of this section. The Section 5 concludes the main findings, provides recommendations for future research, and discusses the policy implications.
2. Methodology
2.1. Study Area
South Xinjiang includes three prefectures, which are located in the southwest of the Taklimakan Desert. Bounded by water resources, few pieces of land are cultivable. This region is a typical and traditional oasis agricultural region located on the edge of the Taklimakan Desert. In particular, South Xinjiang is one of the 14 contiguous and concentrated poverty-stricken areas in China. The poverty in this area presented the following characteristics: (1) the high incidence of poverty with a proportion of 18.8%; (2) the deepest poverty-stricken degree with an annual income of less than 4626 yuan/per capita, compared to the national average of 11,442 yuan/per capita [17]; (3) a wide coverage of poverty with all the 24 counties being key counties for poverty alleviation and development and 75% of the administrative villages being the key villages for poverty alleviation and development. In sum, the aforementioned factors have led to South Xinjiang becoming a typical contiguous and concentrated poverty-stricken area in China. In general, poverty in this area is caused by certain regional factors to some extent.
2.1.1. Land-Use Characteristics
Most of the land is mountainous and constitutes the Gobi Desert, and the oasis area accounts for less than 3.7% of the total land surface. Most of the residents are concentrated in a limited oasis, and the continuously growing population is making the contradiction between increasing people and decreasing land in South Xinjiang more and more prominent. The agricultural area of the three prefectures in southern Xinjiang accounts for 18.8% of the total agricultural area in Xinjiang, while the population accounts for 34% of the total population of Xinjiang [18]. At the average level of 0.22 ha per capita arable land in Xinjiang, only 0.15 ha is available per person in Kashgar, 0.09 ha per person in Kizilsu Kirghiz Autonomous, and less than 0.09 ha per person in Hotan [18].
2.1.2. Limited Economic Activities
The area can be included under the categories of arid and extremely arid areas with an average annual precipitation of less than 100 mm, and the annual average evaporation is more than 2100 mm [19]. However, because it is far away from eastern China, where both population and economy are concentrated, the level of industrial activity is relatively low. For instance, in 2017, the proportion of the secondary industry was only 25.6%, which was much lower than the national level of 40.5% [18,20]. Thus, the three states are mostly engaged in agricultural activities. Agricultural productivity in some areas is relatively low. The average yield of wheat is 5583 kg per ha (Figure 1).
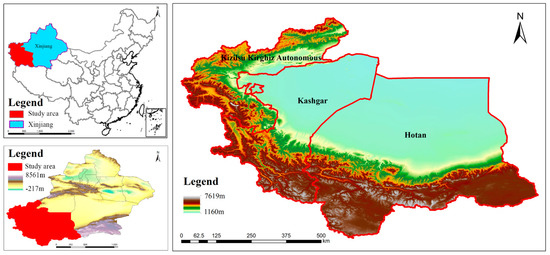
Figure 1.
Study area.
2.2. Method and Data Source
To explore the ways of breaking the vicious cycle of poverty and illness, the actual cycle in the study area needed to be explored beforehand. Besides, in response to the prevalence of illness-induced poverty in South Xinjiang, a series of strategies were adopted to change the status quo. Focusing on the aim, interviews of the members of poor households, as well as the local government staff, were conducted for this analysis. Then, the data collection stages were divided into three research stages.
First, during the pre-field stage, the selection of research fields was conducted. Specifically, villages with a certain number of the poor with illness were selected as the case studies. As a result, five villages were selected. Second, during the field work stage, interviews of the staff members working for the local government were conducted in order to acquire an overview of illness-induced poverty and the regional policies issued by the local government. Data collected through the interviews include the general situation of illness-induced poverty and how the local government designs the set of practices to be implemented to deal with the same. The staff included cadres from villages and towns. A total of five interviews with more than 20 respondents were conducted, and each interview lasted more than 2 h. The data were recorded using field notes. Then, the household survey was conducted among the poor who were affected by an illness (as well as disability) in 2018. As a result, 80 respondents covering five villages were included. The data were also recorded using field notes. The questions were related to the illness of members of the household, economic activities, and household characteristics. For instance, what kind of disease the family member suffered from, the source of income, what the government had done in the process, whether those policies worked, etc., were some of the questions included in the survey. Moreover, to ensure the authenticity of the survey, the questions were phrased as simply as possible. Additionally, persons proficient in the local language were hired as surveyors. Third, during the data analysis stage, the inductive research approach was applied to summarize the common information gained from interviews and the survey.
3. The Vicious Cycle of Poverty and Illness in Oasis Agricultural Areas
3.1. What Is Poverty?
In general, poverty has been defined in three ways based on different approaches, which are the basic needs approach, the capability approach, and the economic resources approach [21,22]. First, it was stated that poverty, which was originally considered as an economic phenomenon, indicates such a condition where the individual or household income is under the basic line of living. As a result, poverty was defined as the inability to purchase necessities [23] and insufficient means to obtain the minimum necessities for the maintenance of merely physical efficiency [24]. Second, poverty was defined as the lack of availability of minimal resources for participating in the activities, customs, and diets commonly approved by society [25]. Third, the definition of poverty was simplified as absolute deprivation in terms of a person’s capabilities, which are associated with relative deprivation in terms of commodities, incomes, and resources [26]. Additionally, poverty was also described from a symbolic dimension, which related it to a lack of voice, a loss of rights, and diminished citizenship [27]. Furthermore, it should be stated that poverty is caused not only by economic factors but also social deprivation, such as missing opportunities and exclusion from them. In particular, it was observed that irrespective of whether poverty is understood as the deprivation of basic needs, capabilities, or economic resources, a lack of food and hunger is core to the understanding of poverty [28], (p. 35). The overview of the multidimensional definitions of poverty reminded us that poverty refers to the low level of household assets, thereby providing the background for the explanation of the mechanism of the vicious cycle of poverty and illness. In our study, the poor residents were identified based on their income, and a household member with an average income lower than 2800 yuan per capita per year is defined by the local government as poor in South Xinjiang, China.
3.2. Components in the Vicious Cycle—Households’ Characteristics
For the poor suffering from diseases and their household members, poverty is a seemingly thorny issue since people with certain illnesses cannot work. As a result, the two-way relationship between disease and poverty is described as a vicious cycle that makes families comprising members with illnesses face poverty. According to the household survey, all the households were identified as poor following the definition of poverty. Most of the poor are generally weak, seriously ill, and suffer from chronic conditions. The proportion of poverty caused by illness and disability was found to be 77.8% and 22.2%, respectively. What makes illness-induced poverty worse is that it is generally accompanied by a lack of land, labor, and development funds. It was found that 30.93% of the poor have excessive burdens due to medical treatment. The household survey enabled us to know more about the characteristics of illness-induced poverty, which helped construct the conceptual framework for analyzing the vicious cycle of poverty and illness in South Xinjiang, China. The household survey revealed some primary components of the vicious cycle, which are described in the following sections (Figure 2).
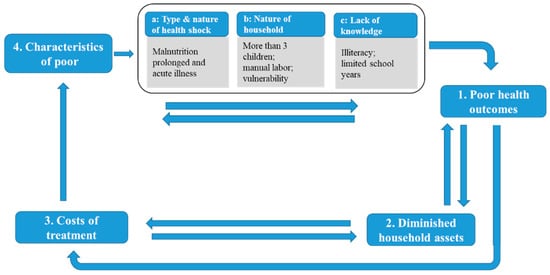
Figure 2.
Conceptual framework for the vicious cycle of poverty and illness in South Xinjiang, China.
3.2.1. Poor Health Outcomes
Poor health outcomes are mainly caused by the condition of poverty, which is also referred to as the deterioration of health caused by poverty. In most occurrences, this component determines whether the household steps into the vicious cycle. The following three reasons helped us understand this component.
First, as defined earlier, poverty refers to the lack of income and wealth. The poor lack the ability to acquire basic elements necessary for sustenance, leading to malnutrition and imbalanced diets that directly affect people’s health. For instance, a mother’s healthy state may affect an infant’s physical condition to a great extent, which has a significant impact on the future state of the body [29].
Second, the poor families in South Xinjiang always exhibit the following characteristics: high fertility with at least three children and engaged in manual labor (Figure 2).
Third, according to the theory of poverty culture, the poor form inherent norms and values in their minds [30]. What is worse is that the occlusion of the region has made it more difficult for the poor to obtain the required information. As a result, their norms and values are often backward and incorrect, which is even worse. For instance, due to the limited years of schooling, the poor lack the necessary knowledge on how to prevent and deal with diseases.
3.2.2. Diminished Household Assets
The second major component in the vicious cycle is the diminishing of household assets caused by poor health outcomes. The diminished household assets include the financial asset, physical asset, human asset, and social asset.
First, it was observed that the financial asset, which refers to income and savings, directly decreased once the disease emerged. The disease indirectly affected the income level of the family through the following: (1) the decrease in income caused by the loss of working time for patients and family caregivers; (2) the economic loss caused by the decreased ability of the sick [31], such as the absence from work and reduced productivity costs.
Second, it was observed that the human asset, which refers to the number of laborers and the education level of the household members, also decreased directly once the disease emerged. For patients, the disease itself is a reduction in healthy capital, and a decline in health is bound to affect their access to education or training. Moreover, some diseases may have intergenerational inheritance such that the initial health capital of the next generation lags behind that of other people, further increasing the medical burden of the family. In addition, due to the low level of wealth and income, farmers have a weak self-risk ability. Once family members suffer health shocks without insurance compensation, they reduce the overall living standard of the family. Some families may not even be able to meet the basic needs of life. As a result, decision-making behavior on human investment (e.g., education) for household members can be impacted.
Third, it was observed that the physical asset, which refers to the livestock, equipment, etc., decreased if the poor suffered from serious diseases. Specifically, the family’s major medical expenses for health crowded out the investment in other productive physical assets. When household cash is not enough to pay for high medical expenses, families use savings, borrow money, and sell livestock, agricultural tools, and durable consumer goods to deal with the risks associated with the disease. If household goods are sold, resources are redirected to meet short-term consumption or survival needs, thereby damaging the long-term investments (such as productive assets and education) that have an impact on the future of the family. It was observed that long-term illnesses increased the vulnerability of families or individuals quickly. Therefore, initiatives to get rid of poverty must be provided enough long-term support; otherwise, the poor will remain very fragile [32].
Fourth, the social asset refers to the informal risk-sharing mechanisms, such as relatives and neighborhoods. However, such an asset is based on a mutual aid network, which emphasizes “reciprocity”. It was observed that families that suffered from long-term health shocks were gradually marginalized over time. As a result, the scale of the relationship network was narrowed, the frequency of communication decreased, and social support was weakened.
3.2.3. Costs of Treatment
The third key component is the cost of treatment incurred as a result of poor health outcomes as well as diminished assets. The impact of the disease on the family is directly reflected in the medical loss caused by illness, including direct medical expenses such as outpatient fees, hospitalization fees, inspection fees, and medical expenses, as well as other related expenses such as transportation, nutrition, rehabilitation, and health supplies.
Some indicators in previous studies revealed not only the low quality of treatment of the conditions but also the availability of few support options [17].
- ⮚
- Treatment costs account for 6.1% of total consumption expenditure;
- ⮚
- In the case of poor households where poverty was caused by an illness, 82% are in extreme poverty;
- ⮚
- About 80% of poor households are in debt of more than 10,000 yuan.
3.2.4. Characteristics of the Poor
The final key component of the poverty trap is the aggravated poverty caused by the treatment costs. In general, people can respond to disease and poverty in different ways. How they respond is largely influenced by their ability and the opportunities available in terms of various assets, which might be physical, human, and social assets. However, these assets decrease over time. Once the poor households become incapable of rebuilding their assets, they become increasingly vulnerable to poverty and are ultimately forced to rely on highly unsafe and even harmful strategies. As a result, poverty persists.
3.3. Mechanism of the Vicious Cycle
In general, poverty in this area is caused by certain regional factors and household factors. Once the disease emerges, it directly affects the patient as well as their household members. Meanwhile, the household characteristics, i.e., having more than three children and engaging in manual labor, make their recovery more difficult. Notably, short-term illnesses are at risk of becoming prolonged and acute illnesses due to negligence, thereby resulting in catastrophic losses for the household. The poor health outcomes lead to poverty by altering the physical asset, the human asset, and the social asset. In terms of time series, a disease not only affects the family’s assets in the short term but also results in long-term poverty. Moreover, it was observed that the deep-rooted self-satisfying expectation of the poor made people with diseases unable to support themselves or, perhaps worse, unwilling to support themselves [33].
4. Land-Use Policies Adopted by Local Government
This section summarized the results gained from the interviews of the local government staff, strategies that aimed to ensure the fulfillment of the basic needs, increase in income, and improvement of physical fitness that were adopted. Then, the series of strategies were discussed in a theoretical manner.
4.1. Basic Requirements for Disease Control
Strengthening the prevention and control of diseases is an effective way of reducing the incidence of diseases. Most of the poor people in the oasis agricultural area are engaged in manual labor and have at least three children in their family. Once the disease emerges, it directly affects the living conditions as well as other household members. Therefore, central to the idea of breaking this vicious cycle is the prevention of the occurrence of diseases and ensuring the supply of nutrients. Thus, strategies formulated by the local government include the construction of township health centers and village clinics to improve the health care infrastructure, the prevention of communicable diseases and endemic diseases, free testing for early detection of chronic and acute illnesses, and volunteer medical consultation. Moreover, the local government takes various measures to reduce non-productive expenditures and avoid exemptions. The strategies include the following:
- ⮚
- Ensuring full coverage of medical insurance to reduce the personal cost incurred for the treatment of the disease;
- ⮚
- Establishing a reimbursement system for chronic diseases;
- ⮚
- Strengthening medical insurance for acute illnesses;
- ⮚
- Increasing the proportion of reimbursement: 90% in township hospitals and 70% in tertiary hospitals;
- ⮚
- Reducing complex procedures for reimbursement.
For instance, if family members spend more than 10,000 yuan at their own expense due to illness, they are exempted from the self-raised expenses for the following year. Moreover, the reimbursement rate is increased appropriately. Additionally, the pension for the elderly, i.e., those over 60 years of age, is appropriately increased. Specifically, 1440 yuan/month is received by the people between the ages of 60 and 70, 1500 yuan by those between 70 and 80, and 1800 yuan by those aged above 80. Furthermore, free and compulsory education is provided for the poor to reduce children’s enrollment costs. Moreover, living allowances are also provided for children in the education stage.
Diet, drinking water, sanitation, and housing safety are closely related to health. A problem in any of those aspects has an impact on health. In South Xinjiang, the emergence of diseases, especially chronic diseases, is closely related to family habits and personal lifestyles. For instance, the local diet culture, which is a high-sugar and high-fat diet structure, increases the rate of diseases to some extent. The local government issues strategies by providing clean water and safe food for ensuring basic public services.
4.2. Various Approaches for Increasing Income
First, agriculture should be developed to increase land profit. The poor households with member(s) suffering from diseases do not have much energy and ability to engage in agricultural production. Moreover, they have a low level of education and lack agricultural planting skills. Therefore, poverty is expected to be alleviated through science and technology in order to improve the planting environment, increase crop yields, and promote agricultural development in arid regions. Additionally, the saline-alkali land and new desert land have been re-cultivated (see Figure 3). Moreover, being affected by the local diet culture, there is a large demand for beef and mutton, and thus, planting pasture has become one of the ways of developing oasis agricultural areas. One of the most important attempts was the forage planting experiments where the animal feed was planted. Based on the interviews conducted, it was found that the land profit has been increased.

Figure 3.
Almond planted in South Xinjiang.
Second, the non-agriculturalization industry was developed to promote employment and improve economic profit. Essentially, the poor were encouraged to participate in land circulation as well as rural cooperatives. Under the premise of ensuring that farmers’ land contract rights remained unchanged and planting benefits were not reduced, their lands were invested in rural land stock cooperatives. The cooperative regularly distributes dividends to farmers. In this way, the poor not only share in the achievements of modern agricultural technology but also increase their family income. As a result, the poor gained high rents and moved away from agricultural production.
Then, the township enterprises were constructed to provide employment. Moreover, certain employment training sessions, including those on language and skill, were provided for the poor for free. The poor were also encouraged to develop a courtyard economy, which involves planting and raising small livestock in their own yard since most of the poor have a big yard (see Figure 4).
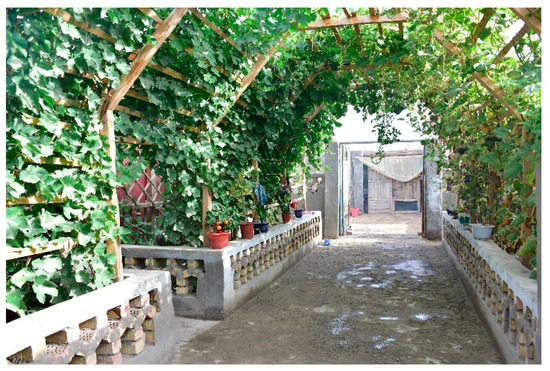
Figure 4.
Courtyard economy.
4.3. Good Living Environment to Strengthen Physical Fitness
A good ecological environment is essential to strengthen physical fitness. In arid areas, desertification has always been a problem that plagues people’s lives. Various approaches have been adopted to prevent and control desertification. Between the five years from 2015 to 2020, 165.22 million ha of desertified land in Xinjiang has been rehabilitated [34]. Desertification control has increased the efficiency of land utilization to a large extent.
Moreover, the village environment has been renovated through the village renovation programs. Specifically, rubbish in the countryside was cleaned up, and the perennial mess in rural areas was rectified. Besides, the local government issued fruit trees to the poor for free, and these fruit trees were planted in and around the yards of poor households. To ensure the survival of the fruit trees, technicians inspected the fruit trees regularly to ensure growth. As a result, the village has transformed significantly (see Figure 5).

Figure 5.
Comparison (a) before and (b) after village renovation.
4.4. Extracting Land-Use Policies from Experiences
In the oasis agricultural area, there are increasing land-use conflicts, and the provision of infrastructure has become prohibitively expensive [16]. Previous studies have shown that land planning policies significantly contributed to the transformation of poverty-stricken counties [35,36]. Thus, in-depth insights from the perspective of land-use advance the debate on the vicious cycle between them in oasis agricultural areas. The successful outcomes witnessed in South Xinjiang were reviewed systematically. The successful policies in South Xinjiang not only enabled the poor with illness to escape from the vicious cycle but also shed new light on rethinking the ways of breaking the path of the poverty spiral.
In sum, these strategies were observed to be related to the exercising of land functions fully by constructing the multi-space in oasis agricultural areas. Specifically, the construction of the living space ensured that the basic needs (e.g., medical and basic living infrastructure) for controlling diseases were met. Therefore, it was regarded as the first step in breaking the vicious cycle. The previous studies showed that ensuring a health outcome is critical, and thus, the medical care system has been focused on individual-level health-related outcomes [37,38]. The successful strategies in South Xinjiang were built on the recognition that ill-health should not be responded to only in terms of its medical components but must be seen and, therefore, treated as part of the wider socio-economic and political response to poverty reduction. Thus, the construction of the living space by equipping the area with essential medical and living infrastructure was highlighted to ensure the health outcome in the vicious cycle. Besides, the ecological space has been constructed to provide a good living environment in order to improve physical fitness. As addressed in previous studies, the poor are both the agents and victims of environmentally degrading activities [39].
Last but not the least, the production function, which aims to increase household income, is critical for improving the household’s economic level. In this support program, the poor with illnesses are encouraged to exercise their own abilities to get rid of poverty rather than assuming that people with illnesses cannot work. In the oasis agricultural area, the land resources are quite scarce. Therefore, the improvement of land-use efficiency was highlighted in particular. Besides, the non-agriculturalization industry has also developed and provided employment. As a result, the economic income of the poor has improved to a large extent. Under the multi-sectoral collaboration in various spaces, the poor with illnesses were able to escape the vicious cycle. In sum, tracking illness-induced poverty by constructing the multi-spaces of “living–production–ecological” (see Figure 6) would provide great support in approving interventions.
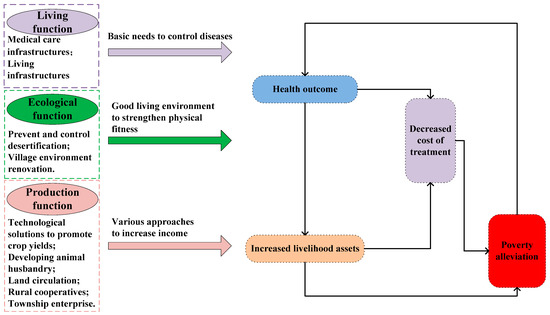
Figure 6.
Constructing the “living–production–ecological” space to break the vicious cycle of illness and poverty.
5. Conclusions
Illness-induced poverty has been one of the serious problems affecting the sustainable development of the rural economy. Affected by regional poverty and the characteristics of households, the vicious cycle of poverty and illness will be exacerbated without any interventions. Despite the spectacular progress in reducing health-related poverty achieved in China, the intervention strategies adopted to break the vicious cycle have not been comprehensively documented. In oasis agricultural areas, land use is much more critical than in any other region. This paper extracted the multi-spaces of “living–production–ecological” from the strategies, which has transformed the vicious cycle into a virtuous one. In sum, success in fighting health-related poverty can be attributed to a three-pronged approach: (1) Construction of the living space should be the first step in breaking the vicious cycle of poverty and illness since it can improve the medical and basic living infrastructure. (2) Construction of the production space is critical for breaking the vicious cycle since it can increase the income of the poor directly. Specifically, the profit can be improved by increasing crop yields, developing animal husbandry, and participating in land circulation and rural cooperatives. Additionally, township enterprises should be constructed to provide working positions and increase the income for the poor. (3) In regard to the construction of the ecological space, preventing and controlling desertification and renovating the village environment will provide a good living environment conducive to the strengthening of physical fitness.
This article summarized the main strategies implemented in South Xinjiang, which significantly helped the poor with illnesses lift themselves out of poverty by using their own abilities and resources. For arid lands, the land is critical for the sustainability of the poor with illnesses; therefore, exercising land function fully was considered as the entry point for breaking the vicious cycle of poverty and illness. By highlighting the economic and production functions of land use, the income of the poor with illnesses has been increased largely. The experiences in South Xinjiang have also transformed society’s unrealistically low expectations about the ability of the poor with illnesses to participate successfully in the labor market.
Our study first discussed the complex relationship between illness and poverty in oasis agricultural areas, which has remarkably been extremely poor because of its regional and household factors. We outlined the knowledge acquired from studying the strategies that intended to address poverty among people with illnesses in arid regions, implying that an appreciation of the structural forces shapes the illness–disease patterns. As evident from this paper, addressing poverty in oasis agricultural areas requires land use through the construction of the multi-spaces of “living–production–ecological”. We discussed how land-use functions should be well-positioned to break the poverty spiral and what actions should be taken to address poverty.
The special resource endowment in oasis agricultural areas has increased the difficulty and particularity of breaking the vicious cycle of poverty and illness. This article extracted the experiences from the success story in South Xinjiang, China, indicating that targeted policies for constructing living, production, and ecological spaces are important for transforming the vicious cycle into a virtuous one. The land-use policies extracted in our analysis permit practical applications in other arid regions. Additionally, this article has a couple of limitations, which simultaneously suggest avenues for conducting further research on sustainable rural development. One of the limitations is that the strategies addressed in this article were developed by the local government. Therefore, we assumed that once the poor are trapped in a vicious cycle of poverty and illness, they cannot break the cycle without the intervention of an external force. Therefore, this study ignored the initiative of the poor to break the cycle to a certain extent. Moreover, though the issue of illness-induced poverty is not a new topic, the lack of an appropriate dataset has always been one of the obstacles affecting research progress. In the absence of existing data, this article interviewed the poor and the local government staff who know the local situation the best. The methodology of collecting detailed information from all households was challenging and can be improved in future studies.
Author Contributions
Conceptualization, L.Z. and Y.Z.; methodology, L.Z.; software, L.Z.; validation, L.Z. and Y.Z.; formal analysis, L.Z.; investigation, L.Z.; resources, L.Z.; data curation, L.Z.; writing—original draft preparation, L.Z. and Y.Z.; writing—review and editing, L.Z.; visualization, Y.Z.; supervision, L.Z.; project administration, Y.Z.; funding acquisition, L.Z. and Y.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Research Foundation for Youth Scholars of Beijing Technology and Business University (QNJJ2021-56) and China Postdoctoral Science Foundation (2020M680660).
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We are thankful for all participants who contributed their ideas to this study. We also appreciate greatly the constructive comments and suggestions from the anonymous reviewers.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Haushofer, J.; Fehr, E. On the psychology of poverty. Science 2014, 344, 862–867. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, J.; Zhou, Y. Spatio-temporal patterns of rural poverty in China and targeted poverty alleviation strategies. J. Rural Stud. 2017, 52, 66–75. [Google Scholar] [CrossRef]
- Carr, S.C.; Sloan, T.S. Poverty and Psychology: From Global Perspective to Local Practice; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2003. [Google Scholar]
- Nations, U. Transforming Our World: The 2030 Agenda for Sustainable Development. General Assembley 70 Session 2015. Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld (accessed on 1 March 2020).
- Macinko, J.A.; Shi, L.; Starfield, B.; Wulu, J.T., Jr. Income inequality and health: A critical review of the literature. Med. Care Res. Rev. 2003, 60, 407–452. [Google Scholar] [CrossRef]
- Stratford, D.; Mizuno, Y.; Williams, K.; Courtenay-Quirk, C.; O’leary, A. Addressing poverty as risk for disease: Recommendations from CDC’s consultation on microenterprise as HIV prevention. Public Health Rep. 2008, 123, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Gillies, P.; Tolley, K.; Wolstenholme, J. Is AIDS a disease of poverty? AIDS Care 1996, 8, 351–364. [Google Scholar] [CrossRef] [PubMed]
- Worrall, E.; Basu, S.; Hanson, K. Is malaria a disease of poverty? A review of the literature. Trop. Med. Int. Health 2005, 10, 1047–1059. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N. Is breast cancer a disease of affluence, poverty, or both? The case of African American women. Am. J. Public Health 2002, 92, 611–613. [Google Scholar] [CrossRef] [PubMed]
- Schubert, K. Poverty causes illness. WHO favors the family health nurse as a means for controlling the sequelae of poverty. Pflege Aktuell 2002, 56, 273. [Google Scholar] [PubMed]
- Hughes, C.; Avoke, S.K. The elephant in the room: Poverty, disability, and employment. Res. Pract. Pers. Sev. Disabil. 2010, 35, 5–14. [Google Scholar] [CrossRef][Green Version]
- Livermore, G.A.; Goodman, N. A Review of Recent Evaluation Efforts Associated with Programs and Policies Designed to Promote the Employment of Adults with Disabilities; Report; Rehabilitation Research and Training Center on Employment Policy for Persons with Disabilities: Princeton, NJ, USA, 2009.
- Flores, G.; Bauchner, H.; Feinstein, A.R.; Nguyen, U.S. The impact of ethnicity, family income, and parental education on children’s health and use of health services. Am. J. Public Health 1999, 89, 1066–1071. [Google Scholar] [CrossRef]
- Hughes, C. Poverty and disability: Addressing the challenge of inequality. Career Dev. Transit. Except. Individ. 2013, 36, 37–42. [Google Scholar] [CrossRef]
- Zhou, L.; Xiong, L.Y. Natural topographic controls on the spatial distribution of poverty-stricken counties in China. Appl. Geogr. 2018, 90, 282–292. [Google Scholar] [CrossRef]
- Zhang, L.; Zhao, Y.; Zhang, X.; Du, H. Effect Mechanisms of Peasant Relocation Decision-making Behaviours in the Process of Rural Spatial Restructuring: The case of Hotan region, China. Sustain. Cities Soc. 2020, 63, 102429. [Google Scholar] [CrossRef]
- Mengxia, H. The Precise Identification about Poverty Population and Influence Mechanism of the Three Southern Prefectures in Xinjiang, in University of Chinese Academy of Sciences; University of Chinese Academy of Sciences: Urumqi, China, 2017. [Google Scholar]
- National Bureau of Statistics of the People’s Republic of China. Xinjiang Statistical Yearbook; National Bureau of Statistics of the People’s Republic of China: Beijing, China, 2018.
- Han, S.; Hu, H. Spatial variations and temporal changes in potential evaporation in the Tarim Basin, northwest China (1960–2006): Influenced by irrigation? Hydrol. Process. 2012, 26, 3041–3051. [Google Scholar] [CrossRef]
- National Bureau of Statistics of the People’s Republic of China. China Statistical Yearbook; National Bureau of Statistics of the People’s Republic of China: Beijing, China, 2018.
- Sylvestre, J.; Notten, G.; Kerman, N.; Polillo, A.; Czechowki, K. Poverty and serious mental illness: Toward action on a seemingly intractable problem. Am. J. Community Psychol. 2018, 61, 153–165. [Google Scholar] [CrossRef]
- Spicker, P. The Idea of Poverty; Policy Press: Bristol, UK, 2007. [Google Scholar]
- Smith, A. An Inquiry into the Nature and Causes of the Wealth of Nations; Liberty Fund, Inc.: Carmel, CA, USA, 1817; Volume 2. [Google Scholar]
- Rowntree, B.S. Poverty: A Study of Town Life; Macmillan: London, UK, 1901. [Google Scholar]
- Townsend, P. Poverty in the United Kingdom: A Survey of Household Resources and Standards of Living; University of California Press: Berkeley, CA, USA, 1979. [Google Scholar]
- Sen, A. Development as freedom. Dev. Pract. Oxf. 2000, 10, 258. [Google Scholar]
- Lister, R. ‘Power, not Pity’: Poverty and Human Rights. Ethics Soc. Welf. 2013, 7, 109–123. [Google Scholar] [CrossRef]
- Narayan-Parker, D.; Patel, R. Voices of the Poor: Can Anyone Hear Us? World Bank Publications; World Bank: Washington, DC, USA, 2000; Volume 1. [Google Scholar]
- Rahman, A.; Lovel, H.; Bunn, J.; Iqbal, Z.; Harrington, R. Mothers’ mental health and infant growth: A case-control study from Rawalpindi, Pakistan. Child Care Health Dev. 2004, 30, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Michael, D.L.; Reed, M.H. The Culture of Poverty: An Ideological Analysis. Sociol. Perspect. 1996, 39, 465–495. [Google Scholar]
- Pauwels, R.A.; Rabe, K.F. Burden and clinical features of chronic obstructive pulmonary disease (COPD). Lancet 2004, 364, 613–620. [Google Scholar] [CrossRef]
- Ruthven, O.; Kumar, S. Making & Breaking Poverty in Koraon, Utter Pradesh. Presented at Staying Poor: Chronic Poverty and Development Policy, Institute for Development Policy and Management, University of Manchester, Manchester, UK, 7–9 April 2003; Chronic Poverty Research Centre (CPRC): Manchester, UK, 2003. [Google Scholar]
- Stapleton, D.C.; O’DAY, B.L.; Livermore, G.A.; Imparato, A. Dismantling the poverty trap: Disability policy for the twenty-first century. Milbank Q. 2006, 84, 701–732. [Google Scholar] [CrossRef]
- Liu, X. The Desertification Control in Xinjiang Is Getting Better. 2020. Available online: http://www.forestry.gov.cn/main/5115/20200703/084843703230645.html (accessed on 5 March 2020).
- Herwirawan, F.X.; Kusmana, C.; Suhendang, E.; Widiatmaka, W. Changes in Land Use/Land Cover Patterns in Indonesia’s Border and their Relation to Population and Poverty. J. Manaj. Hutan Trop. (J. Trop. For. Manag.) 2017, 23, 90–101. [Google Scholar] [CrossRef][Green Version]
- Li, Y.; Yi, L.; Karácsonyi, D.; Liu, Z.; Wang, Y.; Wang, J. Spatio-temporal pattern and driving forces of construction land change in a poverty-stricken county of China and implications for poverty-alleviation-oriented land use policies. Land Use Policy 2019, 91, 104267. [Google Scholar] [CrossRef]
- Wang, Y.P.; Zhou, X.N. The year 2020, a milestone in breaking the vicious cycle of poverty and illness in China. Infect. Dis. Poverty 2020, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Narasimhan, L.; Gopikumar, V.; Jayakumar, V.; Bunders, J.; Regeer, B. Responsive mental health systems to address the poverty, homelessness and mental illness nexus: The Banyan experience from India. Int. J. Ment. Health Syst. 2019, 13, 54. [Google Scholar] [CrossRef] [PubMed]
- Etongo, D.; Djenontin, I.N.S.; Kanninen, M. Poverty and Environmental Degradation in Southern Burkina Faso: An Assessment Based on Participatory Methods. Land 2016, 5, 20. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).