Abstract
This study examines air quality in Polish health resorts (HR) and its potential health risks, challenging the belief that these environments always provide safe air for recovery. Over five years, air quality was evaluated by measuring concentrations of PM10 and benzo(a)pyrene (B(a)P) in seven resorts with varying environmental conditions. Using data from 3781 daily samples, both non-carcinogenic and carcinogenic risks were assessed for visitors (various age groups) and employees to determine health risks from prolonged exposure. The findings show frequent exceedances of national B(a)P limits, with some resorts, such as HR2 in Rabka-Zdrój and HR3 in Polanica-Zdrój, surpassing permissible levels by up to 320% and 373%, especially in winter. Non-carcinogenic risks exceeded safe limits by up to 40% for visitors in HR2 and 18% for employees in HR6 (Szczawno-Zdrój). Carcinogenic risks were up to 3.74 times higher than acceptable levels for visitors in HR2 and 3.15 times higher for employees in HR5 (Latoszyn), indicating a continuous risk from long-term exposure. These findings underscore the urgent need for measures to improve air quality in HRs. Given the global implications, similar risks could affect resorts worldwide. Therefore, future research should focus on cross-border studies and innovative strategies to manage pollution and protect health.
1. Introduction
Air as a mixture of gases is a component of the natural environment that determines the continuation of life on Earth. At present, industrial development, the increase in the number of cars, and the combustion of fossil fuels are the main causes of declining air quality [1]. Air pollution and its forecasting are of interest to many scientists internationally [2,3,4,5]. This major environmental problem affects the lives of people in societies. Associated with the industrial revolution, the increase in coal combustion and the smog problem has become a cause of increased morbidity and mortality [1].
Priority air pollutants include carbon monoxide (CO), particulate matter (PM), sulfur dioxide (SO2), ozone (O3), nitrogen oxides (NOx), volatile organic compounds (VOCs), and polycyclic aromatic hydrocarbons (PAHs) [6,7]. There is a strong correlation between exposure to air pollution and pathogenic effects on human health [8].
Poland is one of the European Union countries facing a serious air pollution problem, due to the widespread use of coal for residential heating, industrial emissions, and the persistence of low-level emission [4]. Particularly in autumn and winter, there are numerous exceedances of current air quality standards, in particular for PM10 particulate matter with a diameter of less than 10 μm, PM2.5 fine particulate matter with a particle diameter of less than 2.5 μm, and for polycyclic aromatic hydrocarbons [9]. PM10 and PM2.5 particulate matter can penetrate the respiratory system, leading to serious health issues such as respiratory and cardiovascular diseases, and have been linked to increased mortality rates [10,11,12,13,14]. Polycyclic aromatic hydrocarbons (PAHs) constitute a group of chemical substances of particular significance to the environment. A significant factor in PAH pollution is human activity. Many PAHs are classified as mutagenic and carcinogenic substances [15]. Benzo(a)pyrene (B(a)P), due to the frequency of its testing, has been recognized as a marker for PAHs in the air. B(a)P pollution is a significant problem, especially in areas where coal and wood are commonly burned in heating systems [16]. Low-level emissions are the most important factor influencing B(a)P emissions, not only in Poland but also in Europe [17]. The issue of poor air quality in Poland applies to a large part of the country. The analyzed problem also concerns the area of health resorts (HR), which are obliged to maintain high environmental quality [18]. The climate of HRs should in particular be characterized by first-rate air quality. Patients of HRs during their stay are treated in HR facilities [19]. During their leisure time, they spend time outside the indoor facilities. When staying outside the buildings, patients are potentially exposed to air pollution [18]. The presence of pollutants in the air poses a threat both to residents but also undermines the viability of a HR treatment [20]. Similar challenges have already been observed in Poland [21,22,23,24], where authors highlighted the impact of air pollution on HRs, especially in terms of PM10 and other pollutants. Furthermore, Tammekivi et al. [25] identified comparable issues in northern Europe, where small towns with winter resorts experiencing seasonal peaks in pollution due to increased traffic and heating during winter also face significant air quality problems. These studies confirm that air quality challenges are not limited to urban areas but also affect HRs and small towns across Europe.
Therefore, this study aimed to provide a comprehensive assessment of air quality in Polish HRs by evaluating the health risks associated with B(a)P exposure via inhalation. This study focused on analyzing concentrations of PM10 and B(a)P across seven HRs: Konstancin-Jeziorna, Rabka-Zdrój, Polanica-Zdrój, Kołobrzeg, Latoszyn, Szczawno-Zdrój, and Swoszowice; each represent different environmental conditions and operational practices across Poland. The research aimed to assess whether current air quality standards are adequate. The investigation differentiated between intermittent exposure for resort staff and prolonged exposure for patients, to better understand the potential health risks and the effectiveness of the therapeutic environments provided. The hypothesis underlying this study was that the air quality in these resorts may not consistently meet the necessary standards, which could compromise the intended health benefits of the resorts’ climates. Although the research focused on a specific set of locations, its implications are of profound global significance. The findings offer critical insights that can be extrapolated to similar health-focused facilities worldwide, informing global strategies for air quality management and patient safety. By addressing a crucial gap in understanding and offering actionable recommendations, this study has the potential to enhance global public health practices and contribute to improved environmental standards in HRs globally.
2. Materials and Methods
2.1. Study Area
The study was conducted in 7 HRs located in different parts of Poland (Figure 1). The first (HR1) is located in Konstancin-Jeziorna (52°04′09.2″ N 21°07′17.1″ E), the central part of the Mazowieckie voivodship. It borders on the north-eastern side with the capital city of Warsaw and belongs to the Warsaw agglomeration. HR1 is suitable for patients with upper respiratory conditions, cardiovascular disease, hypertension, orthopedic and trauma issues, rheumatological diseases, and lower respiratory conditions, excluding asthma sufferers.
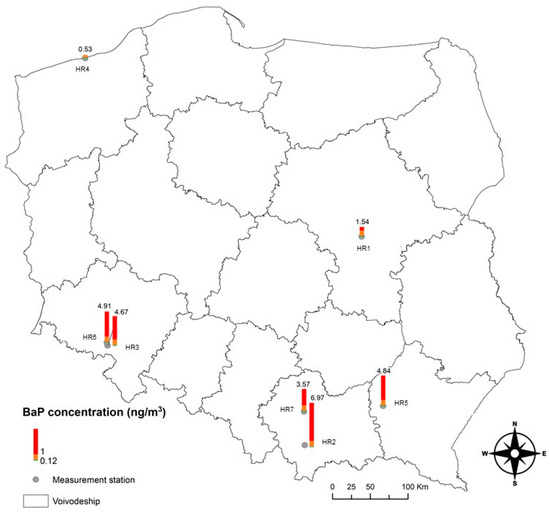
Figure 1.
Location of studied health resorts in Poland, with average annual B(a)P concentrations measured from 2018 to 2022.
The second (HR2) is located in the Rabka-Zdrój, a Nowy Targ district (49°36′05.7″ N 19°58′11.1″ E). The territory of the municipality is surrounded by two mountain ranges: Gorce and Beskid Wyspowy. HR2 provides treatment for both adults and children, specializing in pulmonology, diabetology, cardiology, orthopedics, laryngology, and rheumatology.
The third (HR3) is located in Polanica-Zdrój, a Kłodzko County (50°24′35.6″ N 16°30′34.9″ E), is referred to as the pearl of Polish HRs. It is located at an altitude of 380 to 410 m above sea level. This HR is particularly suited for patients with heart disease, hypertension, peripheral vascular diseases, digestive system disorders, orthopedic–traumatic conditions, rheumatological diseases, and upper respiratory tract ailments.
The fourth (HR4) is located in Kołobrzeg (54°11′09.3″ N 15°33′59.1″ E). Its location and its maritime climate create favorable conditions for the use of climatic stimuli for therapeutic purposes. Kolobrzeg is one of the most popular spa resorts on the Baltic Sea and treats both children and adults with conditions such as respiratory diseases, motor organ disorders, cardiovascular issues, and rheumatological diseases.
The fifth (HR5) is located in Latoszyn, within the municipality of Debica (50°01′10.2″ N 21°22′10.6″ E). It is relatively new as HR status was granted to it in 2022. The HR5 has at its disposal waters of sulfide and sulfurous waters. HR5 specializes in treating patients with rheumatic diseases, cardiovascular conditions, nervous system disorders, and orthopedic and post-traumatic conditions, utilizing its sulfide and sulfurous waters.
The sixth (HR6) is located in Szczawno-Zdrój (50°48′22.0″ N 16°15′13.5″ E) and is famous for its mineral waters, which are used for drinking and bathing. The extracted waters are certified by the National Institute of Hygiene. The awarding of the certificate was based on many years of research, which confirmed the therapeutic properties of at least one pharmacologically active component contained in the mineral water. The municipality is located in the Central Sudetes range and borders the city of Walbrzych. HR6, in accordance with the characteristics of the climate and natural resources, serves patients suffering from diabetes, obesity, osteoporosis, and both upper and lower respiratory tract diseases.
The seventh (HR7) is located in Swoszowice (49°59′32.2″ N 19°56′04.8″ E) and is the only place of its kind in Poland and one of the few in Europe that operates within a large urban agglomeration. It is located in the south-eastern part of Krakow. HR7 caters to patients with orthopedic and traumatic diseases, nervous system disorders, rheumatological diseases, osteoporosis, and skin conditions.
The study analyzed 24 h concentrations of PM10 and B(a)P from 2018 to 2022, examining a total of 3781 daily samples to assess these pollutants. PM10 levels were determined using a medium-volume sampler (2.3 m3/h, Twin PM; Zambelli, Milan, Italy), fitted with a PM2.5 and PM10 sampling head (TSI Incorporated; Shoreview, MN, USA) and quartz fiber filters (Whatman, Maidstone, UK, Ø 47 mm). The B(a)P bound to particulate matter was extracted from the quartz fiber filters using dichloromethane (DCM) as the solvent. The extraction process was carried out in two steps: first, the filters were subjected to ultrasonic treatment in a bath for 30 min to release B(a)P. This was followed by a second extraction phase, where the extract was redissolved in DCM and treated again with ultrasound. The combined extracts were concentrated under a nitrogen stream and then purified using a 0.45 µm polytetrafluoroethylene (PTFE) filter. For the analysis, HPLC was employed, utilizing a C18 chromatographic column (250 mm, 4.6 mm ID, 5 µm particles) with a gradient of acetonitrile and water as the mobile phase. The detection was performed using a UV/Vis detector based on retention times.
The measurement methods employed were rigorously validated to ensure data reliability. The measurements followed the N 12341:2023 standard [26], aligning with the European Union Directive on air quality and cleaner air [27] and the Polish Regulation of the Ministry of the Environment on air quality assessments [28,29]. Both the N 12341:2023 standard and the European Union Directive are consistent with the Federal Reference Methods (FRM) and Federal Equivalent Methods (FEMs). All samples, including blanks, were subjected to strict QA/QC protocols, ensuring rigorous conditioning, weighing, storage, and transportation. Calibration of the instruments was conducted both at the beginning and end of the experiment, with additional checks using a DryCal Defender 530 (Mesa Laboratories Inc., Colorado, USA) during sampling to ensure stable flow. The limit of quantification (LOQ) for the method was set at 0.05 µg/sample, and the repeatability of the method was 5%, with an expanded uncertainty of 25% (k = 2). Recovery values for the analyzed constituents ranged from 94 ± 4% to 101 ± 3% (n = 10). The accuracy of the applied methodology was verified by determining the recovery of standard reference material SRM 1649b (NIST). The recovery rates for PM10 samples and B(a)P ranged from 88% to 107%, further confirming the robustness of the method.
2.2. Human Health Exposure Assessment
Given that B(a)P is recognized as a Group 1 carcinogen by the International Agency for Research on Cancer, a comprehensive assessment of human health exposure was imperative [16,30]. This evaluation, motivated by the necessity to uphold stringent environmental quality standards, particularly in air quality, specifically addressed the carcinogenic and non-carcinogenic risks associated with inhalation exposure to B(a)P. The analysis was stratified across three distinct age groups of HR residents—infants (0–2 years), children (2–16 years), and adults (over 16 years). This division was based on the varying levels of susceptibility to air pollution across these age groups. Infants and young children are particularly vulnerable due to their developing respiratory and immune systems, as well as higher inhalation rates relative to their body size. Although adults are generally less sensitive, they still face significant health risks from long-term exposure to air pollutants [31]. Given that health resorts cater to both children and adults, this stratification allowed for a more accurate assessment of the health risks posed to each group.
The analysis was conducted in two scenarios: (1) for patients seeking health rehabilitation, who reside at the resort continuously for 24 h per day over a 30-day period each year; (2) for adult residents, e.g., staff and medical professionals, who spend an average of 8 h per day at the resort for 20 days each month.
The human health exposure assessment was conducted by analyzing the potential carcinogenic risk via carcinogenic risk indicator (CR) (Equation (1) alongside the potential non-carcinogenic risk through a hazard quotient (HQ) (Equation (2) [32,33]. Both indicators are based on the analysis of the exposure concentration (ECi) of B(a)P (Equation (3), calculated as follows:
Here, IUR represents the inhalation unit risk, specified in μg/m3 by the US EPA [34]. RfC indicates the reference concentration, expressed in mg/m3 [34]. The variable Ci denotes the B(a)P concentration in μg/m3. ET stands for exposure time, set at 8 h per day for scenario 1 and 24 h per day for scenario 2. EF signifies the exposure frequency, set at 240 days per year for scenario 1 and 30 days per year for scenario 2. ED refers to the exposure duration for three distinct age groups: 2 years for infants, 14 years for children, and 62 years for adults. The parameter ATn, representing the average time, is calculated differently depending on the type of risk; for non-carcinogenic substances, it is the product of ED multiplied through 365 days and 24 h. For carcinogens, it is based on 70 years, multiplied by 365 days per year and 24 h per day.
The CRi values derived from this assessment can be evaluated using a scale where a CRi of 1 × 10−6 is considered to represent a negligible risk. CRi values ranging from 1 × 10−6 to 1 × 10−4 are generally deemed acceptable within regulatory standards, whereas a CRi exceeding 1 × 10−4 may signal a substantial health risk, potentially requiring corrective measures [35]. The HQ serves to evaluate the potential health risks posed by non-carcinogenic exposures. An HQ value greater than 1 indicates a likely risk associated with exposure to the non-carcinogenic substance in question, while an HQ value below 1 suggests that adverse health effects are unlikely [36].
2.3. Statistical Analysis
The work was based on daily averages. Monthly and annual averages were then calculated based on these. Statistical analysis was carried out using the Statisica 13.3 program. Scatter diagrams of pollutant concentrations were made of pollutants with a trend line in relation to the entire analyzed period. All data from the spas were checked to assess the normality of distribution. The Shapiro–Wilk test was used for this purpose. Non-parametric tests were also used to analyze the data from the spas. The tests above were chosen because the data analyzed did not have a normal distribution. The Wilcoxon paired rank order test and the sign test were used to compare the values of the concentrations from the selected HR. The non-parametric tests, as opposed to the parametric tests, did not focus on the data values, but on the order of the data.
3. Results and Discussion
3.1. PM10 Concentrations
The analysis of PM10 concentrations across seven HRs from 2018 to 2022 revealed significant variability in daily levels, highlighting ongoing challenges in maintaining air quality within acceptable standards. In 2018, the most pronounced fluctuations in daily PM10 concentrations were observed at HR4, ranging from as low as 2 µg/m3 to as high as 106.1 µg/m3 (Table 1). These fluctuations were likely influenced by the coastal location of HR4, where meteorological factors such as wind speed, direction, and temperature inversions can significantly affect the dispersion of pollutants. Additionally, increased traffic and heating demand during the colder months likely contributed to the peaks in PM10 concentrations. By contrast, in 2022, HR5 experienced the most notable variations, with concentrations ranging from 3.3 µg/m3 to 125.7 µg/m3. These fluctuations indicate that PM10 pollution levels can vary greatly within the same resort over different periods, reflecting both seasonal influences and local environmental factors that affect air quality [37,38].

Table 1.
The measurement series of PM10 concentrations in the analyzed health resorts in the period 2018–2022.
Table 2 complements this analysis by presenting the number of days each year when the PM10 daily concentration limit (50 µg/m3) was exceeded. According to the Regulation of the Minister of Environment, the permissible daily PM10 concentration should not be exceeded more than 35 times per year. In 2018, two resorts, HR1 and HR4, did not record exceedances above this limit, suggesting relatively better air quality management or less pollution exposure in these areas (Table 2). However, HR7 experienced 93 days of exceedances, amounting to a quarter of the year, indicating a significant challenge in controlling PM10 levels. This pattern of exceedance was consistent with HR7’s location near a large urban area, such as Krakow, which contributes to higher levels of particulate matter due to urban and industrial emissions, as supported by the findings from Kuchcik [9]. According to the World Health Organization’s [6] recommended standards for PM10 concentrations, none of the analyzed HRs met the criteria for annual average PM10 levels, underscoring a pervasive issue with air quality across these facilities. Additionally, significant exceedances of the WHO-recommended daily average values were noted in all the resorts, further highlighting the persistent air quality challenges faced by these HRs. The health effects of PM10 exposure are significant, as inhalation of these particles can penetrate deep into the lungs, causing respiratory problems, exacerbating conditions such as asthma and bronchitis, and increasing the risk of cardiovascular diseases [39,40]. Long-term exposure to elevated PM10 levels has also been linked to increased mortality from heart and lung diseases, as well as a reduction in life expectancy [37,41].
Table 2.
The number of days with exceedances of the limit value PM10 (L > 50) in the health resort surveyed in 2018–2022.
The data also revealed a general trend towards improvement in some HR over the analyzed period. For instance, HR7, which had the highest number of exceedance days in 2018 (93 days), showed a reduction to 40 days by 2022 (Table 2). This decline suggests the implementation of more effective air quality management strategies or changes in external factors influencing pollution levels. Similarly, HR5, which recorded the highest 24 h average PM10 concentration of 256 µg/m3 in 2019, saw a reduction in the number of exceedance days from 68 in 2018 to 27 in 2022 (Table 1 and Table 2). However, not all resorts showed consistent improvement; HR3, for example, continued to experience significant exceedances, peaking at 47 days in 2022 (Table 2), indicating persistent challenges in managing air quality.
Particulate matter concentrations showed some seasonality (Supplementary Materials (SM), Figure S1). With the start of the heating season from the beginning of November until the end of April, significant exceedances in PM10 concentrations occurred in the analyzed HR.
Also, the Chief Inspectorate for Environmental Protection in its report on air quality in HR in Poland in 2022 identified emissions at lower altitudes below the boundary layer height as the main reason for the extremely high concentrations of PM10 particulate matter [42,43]. In the winter half of the year, the accumulations of pollutants from low emissions are also influenced by meteorological conditions. Low temperatures, weak winds, and inversion have a negative impact on air quality [22]. According to studies and analyses of air quality, an important factor affecting air quality not only in Europe but also worldwide was the COVID-19 pandemic. Preventive measures against virus contamination taken by national governments had a positive effect on reducing pollutant concentrations in the atmosphere [44].
The issue of PM10 air pollution is also faced by other countries. Based on data from the global particulate matter model, there has been a 22% decrease in global PM10 levels over the past two decades, primarily driven by reductions in developed countries. However, certain countries in Asia and Africa have experienced significant increases in PM10 levels during the same period, including Bangladesh (31.4%), Kenya (26.3%), and Nepal (24.6%) [37].
3.2. Benzo(a)pyrene
Over the period from 2018 to 2022, the analysis of B(a)P concentrations in seven HRs revealed significant exceedances of both national and international air quality standards [29]. As indicated in Table 3, annual average B(a)P concentrations consistently surpassed the Polish National Standard [29] of 1 ng/m3 in six of the seven HRs analyzed. In 2022, HR2 and HR3 reported concentrations exceeding the annual average norm by 320% and 373%, respectively. Such levels are concerning given the strong carcinogenic properties of B(a)P, which can pose serious health risks to patients and staff alike, especially in environments expected to promote health and well-being [9,45]. The problem with the concentration of B(a)P in the air is also highlighted by Anioł et al. [21]. Authors emphases that contrary to the general downward trend persisting since the 1990s for B(a)P concentrations in the air, there are exceedances of national standards and WHO recommendations not only in HRs but throughout the country.
Table 3.
The measurement series of B(a)P concentrations in the analyzed health resorts in the period 2018 to 2022.
Furthermore, the data clearly demonstrate that the average annual concentrations of BaP in the analyzed HR across Poland significantly exceeded the WHO recommended limit of 0.12 ng/m3. This threshold is established by the WHO to minimize health risks associated with long-term exposure to this carcinogenic compound. Alarmingly high B(a)P concentrations were found in HR such as HR2 at 6.97 ng/m3, HR6 at 4.91 ng/m3, and HR3 at 4.67 ng/m3. These values were over 50 times higher than the WHO’s recommended limit. The data highlight a serious public health concern, as all analyzed locations exceeded the WHO guideline for safe B(a)P levels. Persistent exposure to such elevated concentrations of B(a)P in these HR—which are typically sought after for their clean air and therapeutic environment—could lead to increased risks of cancer and other health problems among the local population and visitors [18,22]. The stark contrast between the observed B(a)P levels and the WHO recommendations underscores the urgent need for targeted interventions to reduce pollution and protect public health in these areas.
Two of the seven HR analyzed (HR3 and HR6) are located near the Czech Republic. The Czech–Polish project ‘Air Silesia’ assessed the transboundary transport of pollutants in the Czech–Polish border region (between the Moravian–Silesian and Silesian regions) in central Europe [46]. This study provides an assessment of the transboundary transport of PM10 and B(a)P in this border area. The entire region is heavily affected by BaP and PM10 air pollution, with limits still being exceeded. Annual concentrations of B(a)P are even several times higher than the established annual limits. The Czech residential sector is identified as the primary contributor to B(a)P emissions. Data from 48 sites within the National Air Quality Monitoring Network indicate that the annual average concentration of BaP varies significantly, ranging from 0.4 ng/m3 at a rural regional station to as high as 7.7 ng/m3 at an industrial station. Moreover, short-term measurement campaigns conducted in small settlements have revealed elevated daily concentrations of BaP during the winter months, with values ranging from 0.1 ng/m3 to 13.6 ng/m3, largely due to local household heating practices [47].
The summer months of May, June, July, and August are characterized by low levels of B(a)P air pollution (SM, Table S1). Air quality starts to change dramatically with decreasing outdoor temperatures from October and continues until April. During the winter months, unbelievable monthly average concentrations of B(a)P are recorded. Two HRs in particular lead the way in reaching unbelievable levels. The monthly average in January for the analyzed period took the value of 19.9 ng/m3 in HR2. In the same month, the monthly average in HR5 was 12.1 ng/m3. Also, Szulc and Tomaszewska [48], indicate a significant relationship between the heating period and B(a)P concentrations in HR2. In 2017, concentrations of the analyzed pollutant remained at a significant level for 9 months of the year. Only in the period from June to August was a decreasing trend observed [40]. The problem of B(a)P pollution is not only associated with large agglomerations. In the case of the pollution under consideration, it is the villages and small towns that suffer from the problem of B(a)P air pollution. In small towns and cities, such as HRs, heating is based on stoves that do not meet emission standards, are furnaces that do not meet emission standards [49].
The main Inspectorate for Environmental Protection also points out the seasonality of concentrations of B(a)P in the calendar year. In the months from October 2021 to March 2022, concentrations of B(a)P were on average from 3.1 to 12.2 times higher than concentrations for the months of the summer half-year [22]. Values above the European Union target level for B(a)P of 1 ng/m3 was recorded in 12 of the 27 reporting countries. As with particulate matter PM10. the problem of meeting air quality standards for B(a)P concerns the central and eastern European countries [50]. This article analyzed the concentration of B(a)P in one of the Baltic locations (HR4). Similar analyses were carried out for the coastal zone in the Gulf of Gdansk [51], where it was observed that average daily concentrations of B(a)P frequently exceeded 1 ng/m3 for 50% to 65% of the monitoring period. These elevated levels were primarily recorded during the heating season, when low temperatures and poor ventilation conditions, combined with air masses from residential areas, contributed to the high B(a)P concentrations.
3.3. Health Effects from Benzo(a)pyrene Exposure
This health risk assessment evaluates the potential impacts of B(a)P exposure on the health in Polish HR, focusing on both carcinogenic and non-carcinogenic risks. The evaluation was structured around two primary scenarios to capture the most vulnerable groups typically found in HR: Scenario 1 examined patients undergoing health rehabilitation, who are continuously exposed to B(a)P for 24 h a day over a 30-day period annually, which is the standard duration of stay for patients in these resorts [52,53]. Patients represent the core group these facilities are designed to serve, and their prolonged exposure, even if limited to a shorter time frame, poses significant health risks, especially given their potential underlying health conditions [54]. Scenario 2 focused on HR staff and medical professionals, who are exposed to B(a)P for approximately 8 h a day over 20 days each month, reflecting a typical full-time work schedule in Poland [55]. While these individuals are not the primary focus of the health services provided, they remain in the resort environment year-round, making them a significant high-risk group due to their continuous exposure over extended periods [53,54].
3.3.1. Risk for Patients
Patients represent the core group for whom HRs are primarily designed. These resorts cater to individuals seeking health restoration, often visiting frequently to maintain or improve their well-being. At the end of 2022, resort facilities operating in Poland collectively served 819.9 thousand patients over the year [56]. This high demand is driven by several factors, including an increasing number of people in the post-productive age group, a growing trend towards a healthy lifestyle, affluence, and heightened health awareness across various age demographics, including families with infants and children seeking preventive care and therapeutic services [57]. HRs offer valuable preventive and rehabilitative services, particularly through natural therapeutic treatments, which are essential in today’s society to combat lifestyle-related diseases and promote overall health and longevity [53,57]. The rising need for such services is not only evident among those requiring medical rehabilitation but also among individuals seeking to enhance their psychophysical condition and prevent the onset of chronic illnesses associated with modern civilization [58].
For the patient group, who remained continuously exposed to B(a)P throughout their stay at the resort, the non-carcinogenic risk fluctuated across different months and years (Figure 2 and SM, Table S2). The highest non-carcinogenic risks, as indicated by the HQ, were observed during the winter months, particularly in January. For instance, in January 2020 at HR2, the HQ for patients reached 0.98, and at HR6, it reached 1.18, indicating a risk level that exceeded the threshold of 1, where non-carcinogenic health effects are considered possible. Similarly high values were observed in December 2020, with HQ values around 1.40 at HR2 and 1.18 at HR6, reflecting persistent high-risk periods during colder months. These elevated levels are primarily due to increased heating activities and lower atmospheric dispersion during the colder months, which contribute to higher concentrations of B(a)P [45]. In addition to the overall analysis for patients, a closer examination of non-carcinogenic risks for different age groups—children (2–16 years) and adults (over 16 years)—revealed important distinctions. While the non-carcinogenic risks for children generally remained low throughout the assessment period, certain months and resorts presented elevated risks for adults. For instance, in January 2021, the HQ for adults at HR6 reached 1.18, indicating a significant potential health risk due to prolonged exposure to B(a)P. In contrast, the HQ values for children during the same period and location were substantially lower, typically remaining well below the threshold of concern. However, despite lower HQ values for children, it is important to note that their developing respiratory and immune systems make them more susceptible to even low levels of environmental pollutants [59]. The observed trend in the data suggests that while children are less exposed than adults, they are not completely free from risk. The most recent data from 2022 indicates some improvement, with HQ values for both children and adults showing a downward trend, particularly in the winter months, with a maximum of 0.73 observed at HR5 in January. This suggests that ongoing measures to improve air quality, such as the adoption of low-emission heating technologies, may be starting to have a positive impact on reducing non-carcinogenic health risks across all age groups in HR environments [48,51].
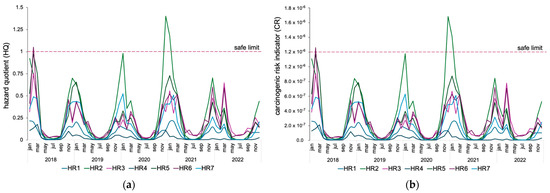
Figure 2.
Monthly distribution of cumulative non-carcinogenic (a) and carcinogenic (b) risks for patients in seven health resorts.
While non-carcinogenic risks seem to be manageable and do not pose a significant threat to patient health, the carcinogenic risk from exposure to radon and its progeny is a more serious concern (Figure 2). The assessment of carcinogenic risk indicated that adults consistently faced the highest risk across all months at HRs, primarily because of their longer cumulative exposure to B(a)P over their lifetimes. For example, in December 2020, the CR for adults at HR6 was 7.21 × 10−7. Although this value is still below the regulatory threshold of concern (1 × 10−4), it suggests a persistent risk, especially with prolonged exposure. For children and infants, the calculated CR values were significantly lower due to their reduced exposure time and lower inhalation rates. However, their developing bodies are more susceptible to carcinogenic substances, which makes even low CR values a potential concern. In December 2020 at HR6, the CR for children (2–16 years) was 5.01 × 10−9, and for infants, it was 7.16 × 10−10. These values, while lower than those for adults, still warrant attention due to the heightened sensitivity of younger populations to carcinogens [45,60]. Prolonged exposure, even at these lower levels, could potentially lead to an increased risk of developing cancer later in life, as children’s developing organs and tissues are more vulnerable to the harmful effects of carcinogens. Additionally, early-life exposure to such toxic substances can disrupt normal growth and development, potentially leading to other adverse health outcomes, such as respiratory issues, immune system deficiencies, and developmental delays [61,62]. Recent data from 2022 show a slight reduction in carcinogenic risk across all age groups, particularly during winter months, suggesting some improvement in air quality and exposure controls. However, these findings underscore the need for continued vigilance and mitigation strategies to further reduce exposure and protect vulnerable groups such as children and infants in HR environments.
3.3.2. Risk for Resort Employees
Resort employees, including medical staff and other workers, represent a significant group vulnerable to the effects of air pollution due to their regular, year-round presence in these environments [53,54]. Although their exposure is intermittent, the cumulative effect over time could lead to serious health implications, especially during months with elevated pollution levels, such as the winter season [62].
The non-carcinogenic risks included concerning levels of exposure in several HRs (Figure 3 and SM, Table S2). In particular, resorts HR2, HR3, HR5, and HR6 showed HQ values exceeding 1 in multiple instances, especially during the winter months. For example, in HR2, HQ values were as high as 2.47 in January 2018 and 3.74 in November 2020, more than double or triple the safe limit. Similarly, in HR5, the HQ reached 2.60 in February 2018, and in HR6, HQ values peaked at 2.80 in January 2018. These elevated HQ values suggest a significant likelihood of non-carcinogenic health effects, especially during the colder months when resort workers are exposed to higher levels of B(a)P due to increased emissions from individual and collective heating installations using solid fuels. The use of solid fuel stoves, characterized by low energy efficiency and high emissions of pollutants, including particulates and B(a)P, exacerbates this risk [47,63,64]. The primary health concerns associated with such exposures include respiratory issues, such as chronic bronchitis and asthma, cardiovascular problems, and potential impacts on the immune system [16,30,61]. In more recent years, 2021–2022, HQ values for HR workers in HR2, HR3, HR5, and HR6 have shown a downward trend compared to previous years. This trend may reflect improvements in air quality due to the implementation of more effective mitigation measures, such as air protection programs introduced by local authorities in Poland and across Europe, including upgrades to heating systems and stricter emissions controls. For example, in HR2, HQ values in January 2021 dropped to 1.88, which is lower than the value of 2.47 recorded in January 2018. Similarly, in HR5, the HQ in February 2022 was 1.73, a decrease from the value of 2.60 in February 2018. These lower HQ values indicate that the health risk associated with non-carcinogenic exposures may have decreased, although it has not been completely eliminated. Continuous exposure to elevated B(a)P levels can lead to an accumulation of toxic effects over time, potentially worsening pre-existing conditions or contributing to the development of new health issues [65,66]. The data indicate that HR workers are at risk not only during peak pollution months but potentially throughout the year if air quality management is not consistently maintained.
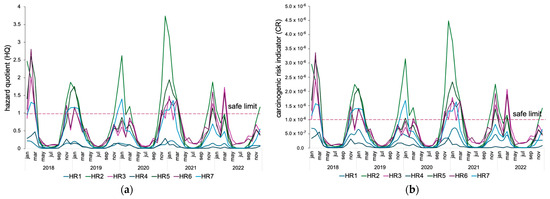
Figure 3.
Monthly trends in non-carcinogenic (a) and carcinogenic (b) risks among health resort employees in seven health resorts.
The carcinogenic risk analysis further underscores the potential long-term health dangers for HR workers (Figure 3). In resorts HR2, HR3, HR5, and HR6, CR values frequently approached or surpassed the acceptable risk threshold, particularly during months with higher pollution levels. For example, HR2 recorded CR values of 2.96 × 10−6 in January 2018, 3.15 × 10−6 in December 2019, and a peak of 3.74 × 10−6 in November 2020. HR5 also exhibited elevated CR values, such as 3.12 × 10−6 in February 2018. A downward trend is evident in the data for the years 2021 to 2022. In HR2, CR values in December 2021 were 1.29 × 10−6, a significant improvement compared to 3.15 × 10−6 in December 2019. In HR6, the CR value in November 2021 was 1.92 × 10−6, which also indicates a reduction compared to earlier peaks from 2018 to 2020. Although CR values still exceed the acceptable limit, suggesting the presence of some carcinogenic risk, their decline suggests a positive trend toward improving exposure conditions. However, prolonged exposure to even low concentrations of carcinogenic pollutants like B(a)P can increase the likelihood of developing lung cancer and other malignancies [30]. The risks are particularly pronounced for workers with extended tenures at the resorts, where cumulative exposure could significantly elevate their lifetime cancer risk.
4. Conclusions
This study shows that air quality in Polish health resorts often fails to meet required standards, with six out of seven resorts experiencing significant exceedances of PM10 and B(a)P levels. Resorts located near industrial areas or dense residential zones, such as HR1 and HR6, are particularly affected by local heating and traffic emissions, while coastal areas like HR4 suffer from meteorological factors like temperature inversions during colder months.
The non-carcinogenic and carcinogenic risk assessments indicate that risks are significantly higher during the winter heating season, with values frequently exceeding safe thresholds. Although Poland has implemented antismog resolutions and stricter emissions standards, further targeted actions are necessary, especially in regions affected by transboundary pollution, to ensure health resorts can support recovery and well-being.
Future initiatives should focus on upgrading heating systems, increasing public awareness, and fostering international cooperation to tackle pollution. Continued research into innovative mitigation technologies and cross-border studies will be essential to protect the health of resort visitors and staff, as well as to address similar challenges globally.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/atmos15101147/s1, Figure S1. Scatter plots showing the relationship between daily concentrations of particulate matter (PM10) and the study period (2018–2022) in the analyzed health resorts: (a) HR1, (b) HR2, (c) HR3, (d) HR4, (e) HR5, (f) HR6, (g) HR7; Table S1. Benzo(a)pyrene Monthly Average Concentrations (ng/m3) in the Seven Health Resorts Over the Period 2018–2022; Table S2. Monthly Distribution of Non-Carcinogenic and Carcinogenic Risks for Patients in Seven Health Resorts for different age groups—infants (0–2 years), children (2–16 years), and adults (over 16 years).
Author Contributions
Conceptualization, G.M.; methodology, W.N.; software, B.K. and W.N.; validation, B.K.; formal analysis, W.N.; investigation, B.K.; resources, B.K.; data curation, B.K.; writing—original draft preparation, B.K. and W.N.; writing—review and editing, G.M., W.N. and B.K.; visualization, B.K.; supervision, B.K.; project administration, B.K.; funding acquisition, G.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Institute of Environmental Engineering of WULS basic (statutory) research projects.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bai, L.; Wang, J.; Ma, X.; Lu, H. Air Pollution Forecasts: An Overview. Int. J. Environ. Res. Public Health 2018, 15, 780. [Google Scholar] [CrossRef]
- Borck, R.; Schrauth, P. Population Density and Urban Air Quality. Reg. Sci. Urban. Econ. 2021, 86, 103596. [Google Scholar] [CrossRef]
- Xu, K.; Cui, K.; Young, L.H.; Wang, Y.F.; Hsieh, Y.K.; Wan, S.; Zhang, J. Air Quality Index, Indicatory Air Pollutants and Impact of COVID-19 Event on the Air Quality near Central China. Aerosol Air Qual. Res. 2020, 20, 1204–1221. [Google Scholar] [CrossRef]
- Koolen, C.D.; Rothenberg, G. Air Pollution in Europe. ChemSusChem 2019, 12, 164–172. [Google Scholar] [CrossRef]
- Juginović, A.; Vuković, M.; Aranza, I.; Biloš, V. Health Impacts of Air Pollution Exposure from 1990 to 2019 in 43 European Countries. Sci. Rep. 2021, 11, 22516. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; World Health Organization: Geneva, Switzerland, 2021; Volume xxi, pp. 1–273. [Google Scholar]
- Cheng, Y.H.; Yan, J.W. Comparisons of Particulate Matter, CO, and CO2 Levels in Underground and Ground-Level Stations in the Taipei Mass Rapid Transit System. Atmos. Environ. 2011, 45, 4882–4891. [Google Scholar] [CrossRef]
- Sofia, D.; Gioiella, F.; Lotrecchiano, N.; Giuliano, A. Mitigation Strategies for Reducing Air Pollution. Environ. Sci. Pollut. Res. 2020, 27, 19226–19235. [Google Scholar] [CrossRef]
- Kuchcik, M. Air Pollution in Polish Health Resorts—A Problem for Both Local Authorities and Patients. Geogr. Rev. 2020, 92, 109–134. [Google Scholar] [CrossRef]
- Lansford, J.L.; Vlachos, D.G. Infrared Spectroscopy Data- and Physics-Driven Machine Learning for Characterizing Surface Microstructure of Complex Materials. Nat. Commun. 2020, 11, 1513. [Google Scholar] [CrossRef]
- Victor, F.S.; Kugarajah, V.; Bangaru, M.; Ranjan, S.; Dharmalingam, S. Electrospun Nanofibers of Polyvinylidene Fluoride Incorporated with Titanium Nanotubes for Purifying Air with Bacterial Contamination. Environ. Sci. Pollut. Res. 2021, 28, 37520–37533. [Google Scholar] [CrossRef]
- Li, L.; Hu, J.; Li, J.; Gong, K.; Wang, X.; Ying, Q.; Qin, M.; Liao, H.; Guo, S.; Hu, M.; et al. Modelling Air Quality during the EXPLORE-YRD Campaign—Part II. Regional Source Apportionment of Ozone and PM2.5. Atmos. Environ. 2021, 247, 118063. [Google Scholar] [CrossRef]
- Liu, H.; Yu, J.; Zhang, S.; Ding, B. Air-Conditioned Masks Using Nanofibrous Networks for Daytime Radiative Cooling. Nano Lett. 2022, 22, 9485–9492. [Google Scholar] [CrossRef]
- Liu, C.; Hu, H.; Zhou, S.; Chen, X.; Hu, Y.; Hu, J. Change of Composition, Source Contribution, and Oxidative Effects of Environmental PM2.5 in the Respiratory Tract. Environ. Sci. Technol. 2023, 57, 11605–11611. [Google Scholar] [CrossRef]
- Gupta, A.D.; Soni, A.; Gupta, T. Synergistic Cancer Risk Assessment from PM1 Bound Metals and PAHs in the Indo-Gangetic Region. Sustain. Chem. Environ. 2023, 1, 100002. [Google Scholar] [CrossRef]
- Bukowska, B.; Mokra, K.; Michałowicz, J. Benzo[a]Pyrene—Environmental Occurrence, Human Exposure, and Mechanisms of Toxicity. Int. J. Mol. Sci. 2022, 23, 6348. [Google Scholar] [CrossRef] [PubMed]
- Aquilina, N.J.; Harrison, R.M. Evaluation of the Cancer Risk from PAHs by Inhalation: Are Current Methods Fit for Purpose? Environ. Int. 2023, 177, 107991. [Google Scholar] [CrossRef]
- Mallah, M.A.; Changxing, L.; Mallah, M.A.; Noreen, S.; Liu, Y.; Saeed, M.; Xi, H.; Ahmed, B.; Feng, F.; Mirjat, A.A.; et al. Polycyclic Aromatic Hydrocarbon and Its Effects on Human Health: An Overeview. Chemosphere 2022, 296, 133948. [Google Scholar] [CrossRef]
- Merenda, B.; Maciejewski, P.; Bezyk, Y.; Sówka, I. Indoor Air Quality in a Selected Health Resort Facility: Analysis of PM10, PM2.5 and 222Rn Concentrations. J. Ecol. Eng. 2022, 23, 202–215. [Google Scholar] [CrossRef]
- Pacín, C.; Martínez-Abaigar, J.; Núñez-Olivera, E.; Aboal, J.R.; De Nicola, F.; Fernández, J.Á. Polycyclic Aromatic Hydrocarbons (PAHs) Levels in PM10 and Bulk Deposition Using Mosspheres: A Pilot Study in an Urban Environment. Environ. Res. 2023, 223, 115406. [Google Scholar] [CrossRef]
- Anioł, E.; Suder, J.; Bihałowicz, J.S.; Majewski, G. The Quality of Air in Polish Health Resorts with an Emphasis on Health on the Effects of Benzo(a)Pyrene in 2015–2019. Climate 2021, 9, 74. [Google Scholar] [CrossRef]
- Kobus, D.; Merenda, B.; Sówka, I.; Chlebowska-Styś, A.; Wroniszewska, A. Ambient Air Quality as a Condition of Effective Healthcare Therapy on the Example of Selected Polish Health Resorts. Atmosphere 2020, 11, 882. [Google Scholar] [CrossRef]
- Radziemska, M.; Mazur, Z. Content of Selected Heavy Metals in Ni-Contaminated Soil Following the Application of Halloysite and Zeolite. J. Ecol. Eng. 2016, 17, 125–133. [Google Scholar] [CrossRef]
- Wyszkowski, M.; Radziemska, M. Assessment of Tri- and Hexavalent Chromium Phytotoxicity on Oats (Avena sativa L.) Biomass and Content of Nitrogen Compounds. Water Air Soil. Pollut. 2013, 224, 1619. [Google Scholar] [CrossRef]
- Tammekivi, T.; Kaasik, M.; Hamer, P.; Santos, G.S.; Šteinberga, I. Air Pollution Situation in Small Towns, Including Winter Resorts: A Comparative Study of Three Cases in Northern Europe. Air Qual. Atmos. Health 2023, 16, 945–961. [Google Scholar] [CrossRef]
- EN 12341:2023; Ambient Air—Standard Gravimetric Measurement Method for the Determination of the PM10 or PM2,5 Mass Concentration of Suspended Particulate Matter. European Committee for Standarization: Brussels, Belgium, 2023.
- E.C. of the European Parliament and of the Council. Directive 2008/50/EC of the European Parliament and of the Council of 21 May 2008 on Ambient Air Quality and Cleaner Air for Europe; Official Journal of the European Union: Brussels, Belgium, 2008. [Google Scholar]
- Minister of Climate and Environment. Ordinance of the Minister of Environment Regulation on Levels of Certain Substances in Ambient Air. J. Laws 2021, 845, 4–6. [Google Scholar]
- Minister of the Environment. Regulation of the Ministry of Environment Environment Safety Law Concerning Evaluation of Substances Levels in the Air. J. Laws 2012, 1032, 5–8. [Google Scholar]
- Myers, J.N.; Harris, K.L.; Rekhadevi, P.V.; Pratap, S.; Ramesh, A. Benzo(a)Pyrene-Induced Cytotoxicity, Cell Proliferation, DNA Damage, and Altered Gene Expression Profiles in HT-29 Human Colon Cancer Cells. Cell Biol. Toxicol. 2021, 37, 891–913. [Google Scholar] [CrossRef] [PubMed]
- Pulster, E.L.; Johnson, G.; McCluskey, J.; Harbison, R.D. Public Health Risk Analysis for Ambient Polycyclic Aromatic Hydrocarbon Exposure Surrounding a Petrochemical Complex in Curaçao. Hum. Ecol. Risk Assess. Int. J. 2020, 26, 2173–2188. [Google Scholar] [CrossRef]
- Penkała, M.; Bihałowicz, J.S.; Rogula-Kozłowska, W.; Rogula-Kopiec, P.; Klik, B.; Bihałowicz, J.; Lewicka, S.; Olszowski, T.; Majewski, G. Health Hazard Related to Fine Road Dust in Poland. Chem. Didact. Ecol. Metrol. 2023, 28, 79–92. [Google Scholar] [CrossRef]
- Sówka, I.; Kobus, D.; Skotak, K.; Zathey, M.; Merenda, B.; Paciorek, M. Assessment of the Health Risk Related to Air Pollution in Selected Polish Health Resorts. J. Ecol. Eng. 2019, 20, 132–145. [Google Scholar] [CrossRef]
- U.S. Environmental Protection Agency. Toxicological Review of Benzo[a]Pyrene; Integrated Risk Information System: Washington, DC, USA, 2017.
- Rybak, J.; Wróbel, M.; Pieśniewska, A.; Rogula-Kozłowska, W.; Majewski, G. Possible Health Effects of Road Dust in Winter: Studies in Poland. Appl. Sci. 2023, 13, 7444. [Google Scholar] [CrossRef]
- Majewski, G.; Klik, B.; Rogula-Kozłowska, W.; Rogula-Kopiec, P.; Rybak, J.; Radziemska, M.; Liniauskienė, E. Assessment of Heavy Metal Inhalation Risks in Urban Environments in Poland: A Case Study. J. Ecol. Eng. 2023, 24, 330–340. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, A.; Agrawal, M. World Air Particulate Matter: Sources, Distribution and Health Effects. Environ. Chem. Lett. 2017, 15, 283–309. [Google Scholar] [CrossRef]
- Majewski, G.; Rogula-Kozłowska, W.; Szeląg, B.; Anioł, E.; Rogula-Kopiec, P.; Brandyk, A.; Walczak, A.; Radziemska, M. New Insights into Submicron Particles Impact on Visibility. Environ. Sci. Pollut. Res. 2022, 29, 87969–87981. [Google Scholar] [CrossRef]
- Fallahizadeh, S.; Kermani, M.; Esrafili, A.; Asadgol, Z.; Gholami, M. The Effects of Meteorological Parameters on PM10: Health Impacts Assessment Using AirQ+ Model and Prediction by an Artificial Neural Network (ANN). Urban Clim. 2021, 38, 100905. [Google Scholar] [CrossRef]
- Badyda, A.; Gayer, A.; Czechowski, P.O.; Majewski, G.; Dąbrowiecki, P. Pulmonary Function and Incidence of Selected Respiratory Diseases Depending on the Exposure to Ambient PM10. Int. J. Mol. Sci. 2016, 17, 1954. [Google Scholar] [CrossRef]
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou, E. Environmental and Health Impacts of Air Pollution: A Review. Front. Public Health 2020, 8, 505570. [Google Scholar] [CrossRef]
- Maring, T.; Kumar, S.; Jha, A.K.; Kumar, N.; Pandey, S.P. Airborne Particulate Matter and Associated Heavy Metals: A Review. Macromol. Symp. 2023, 407, 2100487. [Google Scholar] [CrossRef]
- EEA Air Quality in Europe 2022; Report No. 05/2022; European Environmental Agency: Copenhagen, Denmark, 2022.
- Filonchyk, M.; Hurynovich, V.; Yan, H. Impact of COVID-19 Lockdown on Air Quality in the Poland, Eastern Europe. Environ. Res. 2021, 198, 110454. [Google Scholar] [CrossRef]
- Guerreiro, C.B.B.; Horálek, J.; De Leeuw, F.; Couvidat, F. Benzo(a)Pyrene in Europe: Ambient Air Concentrations, Population Exposure and Health Effects. Environ. Pollut. 2016, 214, 657–667. [Google Scholar] [CrossRef]
- Volná, V.; Hladký, D.; Seibert, R.; Krejčí, B. Transboundary Air Pollution Transport of PM10 and Benzo[a]Pyrene in the Czech–Polish Border Region. Atmosphere 2022, 13, 341. [Google Scholar] [CrossRef]
- Schreiberová, M.; Vlasáková, L.; Vlček, O.; Šmejdířová, J.; Horálek, J.; Bieser, J. Benzo[a]Pyrene in the Ambient Air in the Czech Republic: Emission Sources, Current and Long-Term Monitoring Analysis and Human Exposure. Atmosphere 2020, 11, 955. [Google Scholar] [CrossRef]
- Szulc, A.; Tomaszewska, B. The Concept of Using Local Renewable Energy Sources as Possibility to Reduce Low Emission in Health Resort Rabka-Zdrój. Geol. Explor. Tech. 2018, 57, nr2. [Google Scholar]
- Widziewicz, K.; Rogula-Kozłowska, W.; Majewski, G. Lung Cancer Risk Associated with Exposure to Benzo(A)Pyrene in Polish Agglomerations, Cities, and Other Areas. Int. J. Environ. Res. 2017, 11, 685–693. [Google Scholar] [CrossRef]
- Targa, J.; Ripoll, A.; Banyuls, L.; González Ortiz, A.; Soares, J. Status Report of Air Quality in Europe for Year 2022, Using Validated and Up-to-Date Data; ETC-HE Report; ETC Human Health and the Environment (ETC HE): Germany, Norway, 2023; Volume 2. [Google Scholar]
- Lewandowska, A.U.; Staniszewska, M.; Witkowska, A.; Machuta, M.; Falkowska, L. Benzo(a)Pyrene Parallel Measurements in PM1 and PM2.5 in the Coastal Zone of the Gulf of Gdansk (Baltic Sea) in the Heating and Non-Heating Seasons. Environ. Sci. Pollut. Res. 2018, 25, 19458–19469. [Google Scholar] [CrossRef]
- Brusco, N.K.; Watts, J.J.; Shields, N.; Taylor, N.F. Are Weekend Inpatient Rehabilitation Services Value for Money? An Economic Evaluation alongside a Randomized Controlled Trial with a 30 Day Follow Up. BMC Med. 2014, 12, 89. [Google Scholar] [CrossRef]
- Zajączkowski, M.; Cegliński, P. Analysis of Development Potential of Health Resort Enterprises on the Example of Przedsiębiorstwo Uzdrowisko Ciechocinek S.A. in Aleksandrów County. J. Educ. Health Sport 2018, 8, 699–710. [Google Scholar] [CrossRef]
- Wisnom, M.; Gallagher, K. Quality of Work Life in the Resort Spa Industry. Int. J. Spa Wellness 2018, 1, 159–177. [Google Scholar] [CrossRef]
- Working Time Setting and Settlement—Your Europe in Poland—Gov.Pl Website. Available online: https://www.gov.pl/web/your-europe/working-time-setting-and-settlement (accessed on 31 August 2024).
- Statistical Centre in Poland Therapeutic Activities of Health Resort Facilities and Inpatient Rehabilitation Facilities in 2022; Central Statistical Library: Warsaw, Poland, 2022.
- Królak, S. Spa tourism in Poland—Reflections on the essence, determinants and future. Reg. Dev. Reg. Policy 2021, 2, 125–146. [Google Scholar] [CrossRef]
- Kupcewicz, E.; Bentkowska, A. Health and Its Significance in the Modern Concept of Wellness and Spa. J. Educ. Health Sport 2023, 49, 44–55. [Google Scholar] [CrossRef]
- Garg, A.; Gupta, N.C.; Kumar, A. Spatio-Temporal Variability and Health Risk Assessment of Benzo[a]Pyrene in Different Population Through Ambient Air Exposure in Delhi, India. Expo. Health 2022, 14, 111–127. [Google Scholar] [CrossRef]
- Zhang, Y.; Tao, S.; Shen, H.; Ma, J. Inhalation Exposure to Ambient Polycyclic Aromatic Hydrocarbons and Lung Cancer Risk of Chinese Population. Proc. Natl. Acad. Sci. USA 2009, 106, 21063–21067. [Google Scholar] [CrossRef]
- Kasala, E.R.; Bodduluru, L.N.; Barua, C.C.; Sriram, C.S.; Gogoi, R. Benzo(a)Pyrene Induced Lung Cancer: Role of Dietary Phytochemicals in Chemoprevention. Pharmacol. Rep. 2015, 67, 996–1009. [Google Scholar] [CrossRef]
- Liao, K.; Yu, J.Z. Abundance and Sources of Benzo[a]Pyrene and Other PAHs in Ambient Air in Hong Kong: A Review of 20-Year Measurements (1997–2016). Chemosphere 2020, 259, 127518. [Google Scholar] [CrossRef]
- Kargulewicz, I. Air Emissions of Selected Substances from Particular Sectors Including Metallurgy in Poland. Arch. Foundry Eng. 2017, 17, 83–86. [Google Scholar] [CrossRef]
- Pepłowska, M.; Kryzia, D. Examining Pollution Emissions in Relation to Atmospheric Conditions: A Case Study on Air-Quality Management in Kraków. Polityka Energetyczna–Energy Policy J. 2023, 26, 117–130. [Google Scholar] [CrossRef]
- Majewski, G.; Rogula-Kozłowska, W.; Rozbicka, K.; Rogula-Kopiec, P.; Mathews, B.; Brandyk, A. Concentration, Chemical Composition and Origin of PM1: Results from the First Long-Term Measurement Campaign in Warsaw (Poland). Aerosol Air Qual. Res. 2018, 18, 636–654. [Google Scholar] [CrossRef]
- Romanova, A.; Porowski, A.; Zielski, T.; Dancewicz, A. Origin and Evolution of Chemical Composition of Mineral Waters of Szczawno-Zdrój Inferred from Long-Term Variation of Ionic Ratios, Sudetes Mts. (SW Poland). Environ. Earth Sci. 2021, 80, 374. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).