Abstract
In this paper, an integrative analysis is conducted for both sides of the border of Mexicali B.C. and Imperial Valley, regarding the official procedures and ways in which the collection, organization and disposal of data is carried out for the following: pollutant molecules such as PM2.5, PM10, CO, and O3; meteorological data such as temperature and relative humidity; data produced by epidemiological surveillance of acute respiratory infections; and deaths from all causes minus external ones. Some points around the binational surveillance system, raised in a technical report, are collected, giving continuity to the previous work carried out on this matter. Challenges are identified, recommendations are made, and possible solutions are offered to achieve a binational, unified and integrative system that centralizes meteorological, clinical, and pollution data, and that guarantees the quality and expeditious availability of the data concerning of the effects of air pollution on respiratory diseases and/or natural deaths of the local population. According to our results, air monitoring in Mexicali, clinical data on acute respiratory infections, morbidity, and mortality records must be improved, as well as the cooperation and coordination with the institutions of Imperial Valley. Finally, we show that despite the deficiencies and limitations found in the data generated in the locality, especially data on pollution and clinical data, it is possible, with great effort, to build models that measure and explain the effects of air pollution on health. Examples include the relative risk of death from exposure to PM2.5, PM10, CO, and O3; particulate matter air pollution effects on activation of pulmonary tuberculosis; the association between personal PM10 exposure and pulmonary function; and the estimation of costs and public health benefits by PM10 mitigation, among others.
1. Introduction
Two neighboring countries should establish agreements and programs to solve the problems that affect their populations, such as natural resources, epidemiological surveillance protocols, waste management regulations, and permissible levels of pollution. Projects, agreements, and surveillance systems have been established between Mexico and the United States of America to address different problems, such as the Binational Nogales Wash United States/Mexico groundwater monitoring program [1] for monitoring of water pollution and sharing of water resources. The U.S.-Mexico Border Infectious Disease Surveillance (BIDS) project [2] addresses infectious disease problems that can spread between the inhabitants of both countries with a common border. Other agreements, as reported in the Border Task Force Report of the Paso del Norte region, involving the United States and Mexico, address the needs of southern New Mexico US, western Texas, and northern Chihuahua [3], in addition to research related to water resource management [4], and binational exchange of clinical information [5].
In the Mexicali B.C. and Imperial Valley region, a serious problem that has grown over the years is air pollution. The World Health Organization (WHO) mentions that 58,000 deaths per year are attributable to air pollution in Latin America and the Caribbean [6]. In studies conducted in 2018, the firm IQAir pointed out that Mexicali B.C. is the city with the most pollution in Mexico, as well as being the sixth ranking city in the continent in terms of levels of particulate matter with an aerodynamic diameter less than or equal to 10 and 2.5 μm (i.e., PM10 and PM2.5, respectively). The aforementioned statements are supported by studies conducted in 2015 by the governmental environmental protection agency Secretariat of Environment and Natural Resources (SEMARNAT) [7,8].The report made in 2019 by the National Institute of Ecology and Climate Change (INECC), formerly known as the National Institute of Ecology (INE), mentioned that Mexicali B.C. did not comply with the limits established in the NOM-025-SSA1-2014 for PM10 and PM2.5, placing it among the top three polluted places in the country [9]. Section 3.4 of this document suggests that this pollution has important health repercussions for the inhabitants of Mexicali B.C. and Imperial Valley, and this is supported by local studies on air pollution [10,11,12,13,14,15,16,17]. These studies have included the analysis of contaminants such as CO, O3, PM10, and PM2.5 over time, where reliable data are necessary to be able to establish the relationship between pollutants and the clinical information on diseases and deaths due to exposure of pollution to the inhabitants.
The National Epidemiological Surveillance System in Mexico has a solid structure that has improved over time, seeking to meet the needs arising from the epidemiological transition in the country. However, one of the weaknesses of the system is the time in which the analyses are performed, since currently the analyses are performed weekly instead of daily, as required by the pathologies related to damage caused by air pollution. In addition, there is a time delay of 2 to 3 weeks between the capture time, publication of the results (weekly epidemiological bulletin), and the actual situation. For this reason, it is necessary to have a reliable daily record of information in three areas: (1) pollution and meteorological data, (2) clinical data from health institutions related to acute respiratory infections (ARI), and (3) mortality data.
Currently, there are no binational surveillance agreements involving the cities of Mexicali B.C. and Valle Imperial that involve the three aspects of interest mentioned above. In order to make a proposal for a binational surveillance system, a thorough analysis must be carried out with respect to the methods and procedures involving the collection of data related to air pollution and meteorological monitoring, and protocols and procedures for the exchange and sending of clinical information on ARIs and deaths in both cities.
Therefore, the objective of this paper is to carry out an analysis of the strengths and weaknesses of the surveillance systems for monitoring air pollution, epidemiological control, and mortality on both sides of the border, and to identify the differences and problems that have a negative impact on the health of the population of both countries. We will then propose a unified, binational system that centralizes the collection, organization, analysis, and provision of data.
Based on binational agreements to solve border basin problems between the United States of America and Mexico, such as the Binational Nogales Wash United States/Mexico groundwater monitoring program [1], the U.S.-Mexico Border Infectious Disease Surveillance (BIDS) project [2], and the Border Task Force Report of the Paso del Norte region [3], we propose a unified, binational system that centralizes the collection, organization, analysis, and provision of: (1) epidemiological data on diseases (mainly upper respiratory tracts), and (2) the recording and reporting of daily diseases and deaths. In addition, the system will enable cross-referencing of clinical record data (i.e., respiratory illnesses and deaths) with information on weather conditions and air pollution.
Moreover, according to the opinions of epidemiological surveillance activity experts [18] on both sides of the Mexicali B.C.-Imperial Valley border, the pilot test could be implemented at the Mexicali General Hospital and the Regional Medical Center.
Assignment of responsible physicians who assess, classify, and capture data in the first few hours of patient care would be critically important in initiating the project. Additionally, the union of clinical-epidemiological diagnostic criteria between both border cities (Mexicali B.C. and Imperial Valley), through the operational definitions of case and/or death, as well as the measurement instruments that would be used when questioning the patient about their exposure to risk factors, are also important. Therefore, those responsible for patient care and information capture must have computer equipment, an internet connection, and a telephone line, to allow the issuance and receipt of information from their immediate superior level and with the coordination center, and to enable evaluation and analysis of data with the reference laboratory and binationally, if necessary (see Figure 1).
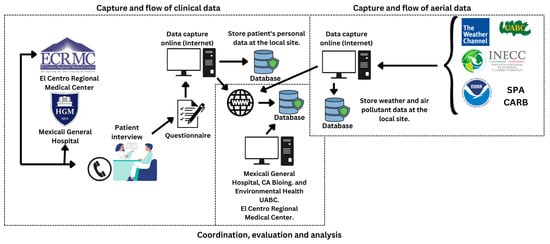
Figure 1.
Binational surveillance system proposed for Mexicali B.C.-Imperial Valley.
Consequently, the daily record would make it possible to carry out tabulations and graphs, and by crossing it with the variables of time and space, their correlation with meteorological data and with air pollution levels would be established, giving the possibility of issuing recommendations for the application of preventive and control measures in a timely manner, focused on the population at risk. After the registration of daily information, the data analysis and feedback could be carried out at the end of the day in the Center for Coordination, Evaluation and Analysis of Data. Later, reports could be generated daily, weekly, monthly, quarterly, semi-annually, and annually, creating a database with information accessible to all levels (see Figure 1).
2. Materials and Methods
We propose a binational surveillance system as summarized in Figure 1. The schematic shows the different elements that would be involved in the implementation of a binational surveillance system, such as the one proposed here. The main objective of this system is to be able to cross-reference data every 24 h on cases of death from all but external causes and new cases of acute respiratory diseases with data on the four main air pollutants (i.e., CO, O3, PM2.5, and PM10), and with two of the main meteorological parameters (i.e., temperature and relative humidity) of this border air basin. In addition, the hospitals recommended as pilots to implement this project are the Mexicali General Hospital and El Centro Regional Medical Center. As shown in Figure 1, the system would be composed of three sections, which are: (1) capture and flow of clinical data, (2) capture and flow of air pollution and meteorological data, and (3) coordination, evaluation and analysis of the information. The clinical data will have to be provided by the Mexicali General Hospital and El Centro Regional Medical Center; the pollution data will have to be sent by CARB, by INECC and by the Secretariat of Environmental Protection (SPA); and the meteorological data could be provided by UABC, and/or by NOAA, and/or by The Weather Channel, and/or by the airports in the area. Meanwhile, the pilot system will have to be coordinated through the participation of the main parties involved: Mexicali General Hospital and El Centro Regional Medical Center. Lastly, the coordinator will also be responsible for the organization, evaluation, analysis, and dissemination of the data and results.
The data are collected on both sides of the border, yet there are no instances that coordinate and manage the responsibility of the filtering, organization, validation, and centralization of the data as a whole in a bilateral way. Figure 2 shows the actors involved in the collection, organization, centralization, analysis, and dissemination of information. In addition, the processes and/or procedures that must be followed to collect the data are described, as well as the way in which they must be organized and how they must be sent to the pilot unit where they would be analyzed, and where the reports would be generated.
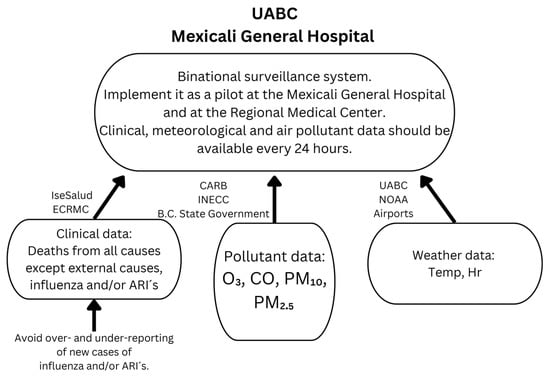
Figure 2.
Main actors in getting data to the pilot station: (1) Clinical data: Secretariat of Health (IseSalud), El Centro Regional Medical Center. (2) Pollutant data: California Air Resources Board (CARB), National Institute of Ecology and Climate Change (INECC), Baja California State Government. (3) Meteorological data: Engineering Institute of the UABC, Mexicali B.C. and Imperial Valley Airports, National Oceanic and Atmospheric Administration (NOAA).
To propose a system like the one suggested by our work, we carried out this methodology in several stages. In the initial phase, research was done on the way that Imperial Valley and Mexicali B.C monitor air pollution and collect meteorological and clinical data. The second stage included an analysis and recommendations to implement the proposal as a binational pilot project between both cities, addressing the deficiencies found in first stage. Finally, the third stage included the impact of the main air pollutants on the population’s health in both cities.
2.1. Data Collection at the Air Monitoring Stations
Mexicali B.C. is considered a non-attainment area in terms of air quality standards for O3, CO, PM2.5, and PM10 [19,20]. It is estimated that nitrogen oxides, grouped in noxes (NOx) and volatile organic compounds (VOCs), which are precursors of O3, contribute 81% and 61% in the production of this gas respectively; these come mainly from automotive emissions, as does the production of CO at 91.1%. Most of the PM10 and PM2.5 (94%) is produced by unpaved roads and soil erosion due to strong winds in the area. In addition, it is presumed that the two thermoelectric plants installed in Mexicali B.C. (i.e., Mexicali B.C. and La Rosita) contribute marginally to air pollution. In addition, it is estimated that when both plants are in operation simultaneously, there is a 0.9% contribution to CO pollution and a 1.3% contribution to PM10 and PM2.5. It is noted that the greatest contribution of the plants to air pollution is given by NOx at 10% [21].
Reports from 2007 [22] indicate that in Mexicali B.C., 25,054 tons of PM10 were emitted into the atmosphere annually, and 70% came from geological sources, of which 29% corresponded to unpaved streets, 16% to paved streets, 47% to wind erosion, and 8% as unexplained. Later, in 2011, SEMARNAT reports increased to 48,826 tons per year [23]. In addition, local media estimated that by 2017 there were emissions of 260,000 tons of waste, increasing air pollution emissions by 30% from 2005 to 2017 [24].
The neighboring city to the north, Imperial County in California, is also considered a non-attainment area for O3, PM10, and PM2.5. The contribution of NOx and VOCs to O3 production is 78% and 63%, respectively, which comes from internal combustion of automotives. The highest air pollution by PM10 is 54%, which is mainly generated by dust raised by strong winds, while the remaining 30% is produced by agricultural activities [22]. All of the aforementioned factors have made the border atmospheric basin between Mexicali B.C. and the Imperial Valley currently one of the most polluted.
As shown in Figure 3, Mexicali B.C. had six air monitoring stations fully financed and operated until 25 March 2007 by the United States Environmental Protection Agency (EPA) and by the company Tracer ES&T contracted by the California Air Resources Board (i.e., CARB), covered by the Border XXI Program. Figure 3 shows the types of pollutants that each station could monitor, the date on which they began to operate, and their geographical location of where these monitoring stations are located [25].
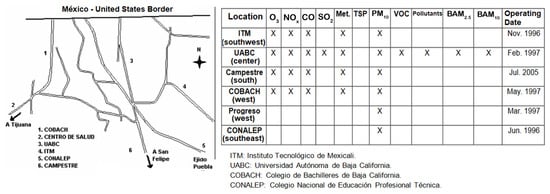
Figure 3.
Geographical location of air monitoring stations in Mexicali B.C. and the pollutants they could monitor until 2008. [x] Indicates that the air monitoring stations have the capability to measure pollutants.
Until June 2008, data from the stations were collected approximately every 15 days by a technician from Tracer, who reviewed and validated the data, finally submitting a quarterly report to CARB; these data were then reviewed and validated. The process of collecting, organizing, analyzing, and validating the data took about three months. As of 25 March 2007, the ambient monitoring stations installed in Mexicali B.C. began to be partially controlled by the state government, due to the Air Quality Monitoring Cooperation Agreement established between EPA, SEMARNAT, Cal/EPA, and the state of Baja California. This agreement, signed in July 2004, establishes the development of an action plan assigning responsibilities for the operation of the monitoring stations once they are transferred to the State of Baja California. In 2007, the Baja California state government contributed approximately 40.12% of the total resources for the sustainability of this project, while the EPA participated with 59.88% [22]. Currently, in 2022, there are only four monitoring stations, one of which is managed by the Municipality of Mexicali. The remaining three are under the administration of the state government: Autonomous University of Baja California (UABC), Baja California State High School (COBACH), and Mexicali Institute of Technology (ITM) [26].
There were seven atmospheric monitoring stations installed in the Imperial Valley in 2007. Figure 4 shows their geographic location, the type of pollutant they record, and the date they began operating.
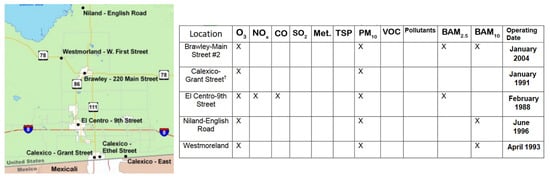
Figure 4.
Geographical location of the air monitoring stations in the Imperial Valley and contaminants that can be monitored. Source: California Air Resources Board (CARB), Imperial County Air Pollution Control District (ICAPCD), U.S. Environmental Protection Agency (EPA). [x] Indicates that the air monitoring stations have the capability to measure pollutants.
Currently, in 2022, the active monitoring stations are: Brawley, Calexico, El Centro, Niland, and Westmorland. There is the possibility of obtaining them in real-time, although these data accessible on the website are unverified and unvalidated [27].
2.2. Meteorological Data
Each air quality monitoring station has a meteorological station that measures temperature, wind direction, and speed. The temperature and relative humidity data recorded by the monitoring stations on both sides of the border are used for internal calculations in some of the equipment. However, this information is complemented by the UABC’s Engineering Institute, which has a meteorology area with a weather station that measures the following: temperature, relative humidity, wind direction, and speed, atmospheric pressure, rainfall, and solar radiation. The station automatically monitors the parameters of temperature, relative humidity, wind speed and direction, and solar radiation every 5 min. Then, the hourly average is obtained automatically [28]. A technician hired by UABC maintains the stations and generates the reports once a week. It is also possible to obtain these meteorological data from the Mexicali B.C. airport and/or The Weather Channel website [28]. For the Imperial Valley, data can be obtained from the National Oceanic and Atmospheric Administration (NOAA) and The Weather Channel [29,30].
2.3. Clinical Data
2.3.1. Epidemiological Surveillance System in México
Information regarding damage and health risks represents an important input for epidemiological surveillance. NOM-017-SSA2-1994 for Mexican Epidemiological Surveillance establishes the illnesses and risks that are subject to notification and investigation, as well as the frequency with which these must be carried out, according to their importance. The purpose of the National Epidemiological Surveillance System (SINAVE) is to obtain timely, uniform, complete, and reliable knowledge regarding the health-disease process in the population, based on the information generated in health services at the local, intermediate, and state level, or their institutional equivalents. The aim is to use the data in planning, training, research, and evaluation of prevention, control, elimination and eradication programs and, if necessary, treatment and rehabilitation. Additionally, it is important to emphasize the interest of this study in ARIs, which belong to the group of respiratory tract infections, since exposure to airborne pollutants is a risk factor for developing ARIs. The conditions registered as ARIs according to the ICD-10 are: (1) Acute nasopharyngitis (common cold); (2) acute sinusitis; (3) acute pharyngitis/Streptococcal pharyngitis; (4) acute tonsillitis/Streptococcal tonsillitis; (5) acute laryngitis/acute tracheitis/acute laryngotracheitis; (6) acute obstructive laryngitis (CRUP) and epiglottitis; (7) acute infections of the upper respiratory tract from multiple and unspecified sites; (8) bronchitis; and (9) acute bronchiolitis [31].
2.3.2. Procedure for Collecting and Submitting Information in México
In the Medical Unit, the procedure for collecting and submitting information is as follows:
- The collection begins at the medical unit with the filling out of the “daily outpatient consultation sheet”, which provides the patient’s age and gender, whether it is a new case or a subsequent case, as well as the diagnostic impression.
- The physician in charge of the first-level unit collects the daily outpatient sheets per week, reviews the diagnostic printout for each day, and records it in the Single Information System for Epidemiological Surveillance (SUIVE-1) format, specifying age group and gender. Subsequent cases are not recorded in the weekly notification.
- The diagnoses of epidemiological interest marked with additional epidemiological surveillance activity are used by the physician responsible for the unit to make the first decision, and, among others, to notify the health jurisdiction so that the corresponding prevention and control activities can be carried out.
- The SUIVE-1 format is submitted from the unit to the immediate superior level no later than Tuesday of the following week after the information is collected.
- If for any reason the information is not sent in the corresponding week, this information is considered untimely and is included in the database of the unit of origin; it is recorded on the original calendar date.
In the Hospital Unit, the process for collecting and submitting information is as follows:
- In the hospital, the “Daily Outpatient Report” is filled out in the Outpatient area and in the Emergency Department.
- The hospital epidemiologist or the IT staff member collects the daily outpatient reports per week, reviews the diagnostic printout for each day and records in the SUIVE-1 format in the line corresponding to the condition, age group, and gender of the new case.
- The diagnoses of epidemiological interest marked with additional epidemiological surveillance activity are used to support the first decision making; in this case, the hospital epidemiologist, in addition to filling out the form, notifies the health jurisdiction so that the necessary field activities can be carried out.
Steps 4 and 5 of the procedure for collecting and submitting information described for the Medical Unit should be repeated.
2.3.3. Epidemiological Surveillance System in Imperial Valley
The health system in the United States of America is a decentralized system, in which each state is governed by its own laws. Therefore, the way of working and capturing information varies from one state to another. The United States has no regulatory obligation to report non-infectious diseases to any level of government. However, all medical units, by regulation, are required to report communicable diseases through the Confidential Morbidity Report. This regulation requires all health facilities to report within 24 h. The report is sent to the local Health Department, where the data are analyzed and confirmed. Then, the information is made public two days after the end of the reporting month. In addition to this process, there is monthly surveillance of respiratory diseases. This report is mandatory for all health units. Once the cases are confirmed and the laboratory results are concordant, the information is returned to all health units through a report called Respiratory Illness Update.
Both El Centro Regional Medical Center and Pioneer’s Health Care District and the satellite rural clinics of both hospitals collect acute respiratory illness data in the Imperial Valley using a computer system called Affinity. This system catalogs all the information, which includes the following: (1) admission date; (2) discharge date; (3) admission diagnosis; (4) discharge diagnosis; (5) birth date; (6) age; (7) sex; (8) patient name; (9) admission time; (10) discharge time; (11) secondary and third-party diagnoses; (12) codes: International Classification of Diseases-9 (ICD9) and Current procedural Terminology (CPT); (13) type of insurance; (14) allergies and medications; (15) name of the family physician and consultants; and finally (16) demographic information.
The Affinity computer system is updated every 24 h (every day at midnight). Affinity also records incoming diagnoses and outgoing diagnoses. The rest of the health centers in the Imperial Valley do not have the technology to catalog such information.
2.3.4. Epidemiological Mortality Surveillance in México
This is done through the System for Epidemiologic Death Statistics (SEED) [32], where the causes of death recorded in the death certificate that is issued at the time of death in the health unit where the incident data are captured. In addition, the causes of death are previously classified according to the International Classification of Diseases in its tenth edition (ICD-10), in which ARIs are classified.
Information on causes of death is published in the mortality yearbooks, since these are validated and compared between the Ministry of Health and National Institute of Statistics and Geography (INEGI). It is feasible to know the causes of death in a preliminary way through the SEED at the local level, particularly those deaths that are subject to epidemiological surveillance and immediate notification, such as maternal deaths, ARIs, and Acute Diarrheal Diseases (ADDs) in children under 5 years of age, whose preventive programs request verbal autopsies. Deaths due to ARIs in the rest of the age groups follow the normal process and are published annually.
2.3.5. Mortality Surveillance in the Imperial Valley
After the death of a person, the only one who can officially declare the death is a physician, and then the person is transferred to the morgue, where an autopsy may or may not be indicated. If an autopsy is performed, a report is generated and then filed along with the medical examiner’s report, which indicates the cause, location, and time of death. An official death certificate is then produced and made public, which remains on file at the county Office of Vital Statistics. California Electronic Death Registration System (CA-EDRS) is the State of California’s system for creating electronic death certificates and the corresponding record. The CA-EDRS web system has the capability for medical examiners, morticians, funeral home operators, doctors, and hospitals to obtain electronic death certificates for legal use 24 h a day, 7 days a week.
3. Results
3.1. Data Collection at Air Monitoring Stations
Once the operation and retrieval of monitoring station data has been analyzed, deficiencies and possible solutions to address them are identified.
Most of the failures that occur in the air monitoring stations in Mexicali B.C. are mainly due to technical problems, derived from the equipment manufactured in 2008, which results in significant data losses during the year. State government makes a series of statements in this regard [33], such as: the inhibitions and possible solutions shown in Table 1.

Table 1.
Inhibitions and solutions for the daily recording of air monitoring stations in Mexicali B.C.
In order to improve data collection and the effectiveness of surveillance networks, some suggestions need to be taken, although some have already been implemented (see Table 1).
3.2. Clinical Data
3.2.1. Inhibitions and Solutions for the Daily Recording of Morbidity Data for Acute Respiratory Infections in Mexicali B.C. and Imperial Valley
Some of the weaknesses identified regarding access to clinical data are: delays and bad practices in the protocols of the health institutions that have been selected as pilots for the implementation of this binational surveillance system.
The main aspects of the current official Mexican epidemiological surveillance procedures that inhibit the possibility of obtaining ARIs data every 24 h are identified below. Possible solutions are also offered, with the objective of abating the identified inhibitions (See Table 2 and Table 3).
Table 2.
Inhibitions and solutions for the daily recording of morbidity data for ARIs in Mexicali B.C.
Table 3.
Inhibitions and solutions for the daily recording of morbidity data for ARIs in the Imperial Valley.
3.2.2. Inhibitions and Solutions for the Daily Recording of Mortality Data for All but External Causes in Mexicali B.C.
A characteristic of the binational system for surveillance proposed in this work is that it can relate the records of deaths with the clinical cases of Acute Respiratory Infections. In addition, it is also relatable to the conditions of exposure to air pollutants, such as NO, O3, PM10, PM2.5 and other contaminants that may be exposed. However, these records, as well as the clinical and air pollution data, have time lags that make it impossible to quickly and expeditiously access them in order to relate them to a cause or exposure. Table 4 and Table 5 show the inhibitions found after analyzing the death systems of Mexicali B.C. and the Imperial Valley.
Table 4.
Inhibitions and solutions for the daily recording of mortality data for all but external causes in Mexicali B.C.
Table 5.
Inhibitions and solutions for the daily recording of mortality data for all but external causes in Imperial Valley.
3.3. Recommendations for Implementing the Proposal as a Binational Pilot Project
3.3.1. Capture and Flow of Clinical Data
- When the patient arrives at the medical unit (i.e., Mexicali General Hospital and El Centro Regional Medical Center and Pioneer’s Memorial), they must be evaluated by the doctor in charge and/or assistant in charge.
- Once an acute respiratory disease is diagnosed, a questionnaire will have to be applied and the data will have to be captured in a local database.
- At the end of the day, a trained person should obtain the information on ARIs for each unit. It will be proposed so that eventually this information can be extracted automatically.
- The data extraction center must be located in each of the pilot hospitals.
- Every morning, a technician dedicated to this project will have to obtain the extracted information and analyze it.
- The information will have to be classified by diagnosis, age, sex, etc.
- Subsequently, the information must be confirmed by an epidemiologist.
- The data and a summary of the information should be sent to the central pilot collection and coordination unit (i.e., Mexicali General Hospital and/or El Centro Regional Medical Center).
- The analyzed and validated data should be available on the Internet.
The participating health units as pilots shall be Mexicali General Hospital, El Centro Regional Medical Center, and Pioneer’s Memorial. Data will be collected, evaluated, and reported every 24 h.
3.3.2. Deaths
- (a)
- In the city of Mexicali B.C., the suggested procedure for the registration and submission of death information is as follows:
- When the person dies in the medical unit (i.e., Mexicali General Hospital), the attending physician will write the medical note of the deceased, and it will be attached to the file.
- The hospital discharge form and the death certificate should be filled out without omissions and sent to the statistics area of the same unit within 24 h of the death; in that way, the data can be entered in the SAEH, where the causes of death will also be assigned a CIE-10 code.
- An assigned epidemiologist will extract the data from the SAEH on deaths from all causes excluding external causes, and will forward them to the pilot central collection and coordination unit (i.e., Hospital General and/or El Centro Regional Medical Center).
- The data analyzed and validated by an epidemiologist should be integrated into the universal database so that they can be accessed via the Internet.
- (b)
- In the city of Imperial Valley, the suggested procedure for death registration is as follows:
- Upon death at the medical facility (i.e., Regional Medical Center and Pioneer’s Memorial), the attending physician will complete a death certificate called a record of death; the original will be kept on record and a copy will be sent to the morgue.
- A technician will have to be trained to collect data on death cases, assign the International Classification of Diseases-10 (ICD-10) code, and send it to the central collection and coordination unit (i.e., Hospital General and/or El Centro Regional Medical Center). For all cases of death, except the external ones, the data will have to be captured digitally within 24 h after the death.
- The analyzed and validated data will be integrated into the universal database so that they can be accessed via the Internet.
3.3.3. Recommendations for the Implementation of a Binational Public Health Administration Model
In relation to the objectives of the project, the purpose of this section is to propose a cross-border management mechanism with the primary objective of addressing public health issues linked to the improvement of binational surveillance that provides lines of action aimed at reducing the effects of air pollution on the environmental health of the border between Mexicali B.C. and the Imperial Valley.
A cross-border management model very similar to that of the Paso del Norte region is proposed, since this mechanism could be adapted to this region, as long as there is political will and citizen approval to establish it. Another similar initiative can be found in the Chihuahua-New México-Texas border region [34].
Before describing the cross-border management proposal for the study region, it is important to mention that the path to follow for its institutionalization would be to generate an inter-institutional agreement entered into between the governments of California and Baja California, including between the governments of the Imperial Valley and Mexicali, in light of the Law on the Celebration of Treaties (published in the Official Gazette of the Federation, on 2 February 1992).
The cross-border management proposal for the study region is represented in the scheme in Figure 5, which could be headed by a citizen committee whose structure and operation are described below.
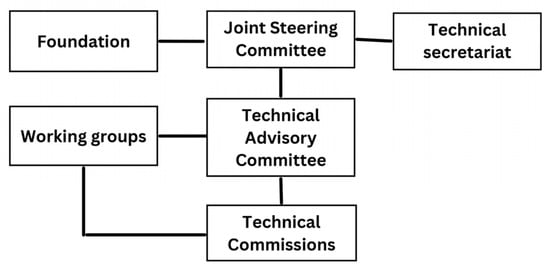
Figure 5.
Organizational model for cross-border management in Mexicali B.C.-Imperial Valley.
Joint Steering Committee
The transboundary nature of this management proposal requires a high degree of institutional commitment and support at the federal, state, and local levels. Therefore, it is proposed that the transboundary management mechanism be led by a Joint Steering Committee (JSC). The purpose of the Centers for Disease Control and Prevention (CDC) will be to develop and approve action plans, develop, manage, and administer the budget necessary for its operation, and submit recommendations to the public health working group, derived from the actual U.S.-México Border Environmental Program Agreements, or directly to the governments of the states of California and Baja California. The JSC will be chaired by two co-chairs, who will be the representatives of the federal governments, through the U.S. Health Agency and the Mexican Secretariat of Health (SS).
Technical Secretariat
It may be composed of two persons, one for each party, to be appointed by the co-chairs upon proposal of the members of the JSC. The functions of the technical secretariat could be, among others, to (1) give notice of the JSC meetings to the members and the public; (2) to prepare and keep the minutes of the meetings; (3) to prepare and present reports; and (4) to follow up on the activities defined in the work programs.
Technical Advisory Committee
At first, the JSC may establish technical commissions for the fulfillment of its objectives at any time and whenever it deems necessary, but they could not make final decisions as that will be an attribution of the JSC. Secondly, the technical commissions become working groups in charge of carrying out specific tasks at the request of the JSC; they shall be headed by a member of the JSC. Lastly, the work of the technical commissions could be organized through regional working groups, based in the border communities of San Diego and Tijuana, and in the Imperial Valley and Mexicali B.C., as per the actual Border Environmental Program Agreement, for example.
Foundation
The management and research of funding, technical assistance, and international co-operation will be the subject of the work of a foundation. Consequently, its function will be the management of financing, approach, and alliances of technical support and cooperation with international institutions related to Environmental Health care, among which the following organizations stand out: World Health Organization (WHO), Pan American Health Organization (OPS), World Bank (BM), U.S.-Mexico Border Health Association (AFMES), United Nations Environment Programme (PNUMA), United Nations Development Programme (PNUD), and Canadian International Development Agency (CIDA).
3.4. Impact of Air Quality on the Mexicali B.C.-Imperial Valley Atmospheric Basin’s Health and on the Mexicali’s Economy
This section contains a summary of the most important scientific articles that have been carried out in the last four decades. As a result, the main factors that endanger the health of both Mexicali B.C. and Imperial Valley residents are identified and analyzed. The first of the works published in the scientific literature reported a high composition of toxic pollutants (85% aluminosilicates) associated with the death of a young resident of Mexicali B.C. The sample was analyzed by X-ray spectrometry. In this way, they related the presence of aluminum and silicon to interstitial granulomatous disease. The alarming results were that particles composed of aluminum and silicon were found, which coincided with samples taken from the patient’s home environment [10]. In the study [11], the composition of the Mexicali’s soil was analyzed to demonstrate its toxicity, as well as showing that it can lead to the development of multifocal interstitial lung disease. In addition, the study proposed that deposits of aluminum silicates as well as asbestos and silica could be an etiological agent in pulmonary fibrosis in exposed individuals. It was also demonstrated in experiments with rats that the particles were deposited preferentially in bifurcations of the alveolar duct, triggering mechanisms that have repercussions on health.
Results on Mexicali’s soil composition for PM10 and PM2.5, collected from a semi-urban and urban area, were presented in [12]. Sixteen elements were identified in the monthly samples (except Ni, which was absent in some monthly samples): Mg, Al, Si, P, S, S, Cl, K, Ca, Ti, V, Cr, Mn, Fe, Ni, Cu, and Zn.
By the 2010s, it was already established as fact that the air breathed at the Mexicali B.C.-Imperial Valley border is highly toxic and represents a health risk, and thus an interesting change in the focus of the published scientific articles can be observed. Once the health effects are known, the next observed in the literature is the estimation of relative risk (RR) of death using statistics. In other studies [13,14], Poisson regression models were used with data on exposures to PM10, PM2.5, CO, O3, sulfur dioxide SO2, and nitrogen dioxide NO2, and the effect of temperature (winter and summer season), to relate the effect of these pollutants to the health of the Mexicali population. As results of these studies, an increase in RR of death was found in the general population and by gender analysis [13], as well as a relationship between particle matter air pollution and the incidence of pulmonary tuberculosis [14].
In 2017, there was a clearly identified need for a more in-depth study to remotely monitor the inhabitants of Mexicali B.C. as they went about their daily activities; therefore, a study was conducted [15] to monitor 97 healthy adults every 5 min for 24-h lapses to demonstrate the relationship between PM10 exposures and pulmonary function. The results of this study showed that there is a small but significant decrease in forced expiratory volume (FEV) capacity.
With this scientific evidence, it is clear that the health problem in the inhabitants due to exposure to pollutants such as PM10, PM2.5, O3, and CO mainly, is a matter of interest and concern for experts in the field of the environment, and also in the health sector, that it has not been resolved in at least four decades. In addition, it seems that it has been getting worse over the years. However, proposals such as in the work of [16], where an evaluation of the health benefits and costs that would have to be carried out in order to have a significant impact on the reduction of PM10 and PM2.5 pollutants have not been implemented by the local government. Therefore, a binational system between both cities could work to have impact in the coming years if this proposal was to be implemented.
4. Discussion
This paper analyzed the institutionalized and non-institutionalized ways, modes, and customs of recording clinical data (i.e., epidemiological surveillance), air pollutants, and meteorological data, both in Mexicali B.C., México, and in the Imperial Valley, California, USA. Deficiencies and differences between the two border cities in data recording were identified and possible solutions were proposed. Challenges were identified and recommendations were made for the construction of a unified binational system whose main function would be the quality assurance, analysis, and centralization of clinical, meteorological, and air pollutant data from the Mexicali B.C.–Imperial Valley air basin. We also analyzed the most relevant local scientific articles dealing with the associations between the main air pollutants and population health. All of them showed statistically significant associations. An integrated, binational, institutionalized monitoring system that centralizes and assures the quality of the data would provide greater certainty in the results of these types of studies in the future.
If this proposed surveillance system was to be implemented at a trinational or multinational level, it would be an interesting challenge. The results of this study would not be fully replicable because only the cities of interest have been analyzed. The main requirement for binational or multinational application is that the countries involved have a common land border; as such, common problems or interests could be analyzed in a similar way to the binational systems studied in this paper. However, another very similar situation that could arise is where countries are very close but do not share the same border, as in the case of Europe and Latin America. Problems such as waste management, natural resources, air pollution, or epidemiological surveillance could apply in these cases, and it would be necessary to analyze the strengths of each country involved and sign agreements and create multinational agencies to solve common problems and issues. This work could serve as a starting point to analyze and propose a multi-national system.
Some of the most relevant aspects found in this work are as follows. First, the meteorological data generated in Mexicali B.C. and Imperial Valley have very good quality. Second, the data generated by the environmental monitoring stations in Mexicali B.C. are not the most adequate; it needs to be improved with our proposed recommendations. Therefore, it is not possible to know the effects of air pollutants on the health of the inhabitants by zones of the city, since there is a large amount of missing data in the time-series generated by the environmental monitoring stations in Mexicali B.C. Furthermore, the analysis of pollutants and their effects on health cannot be carried out in an expeditious manner, as a report with validated data from the stations is not submitted until after three months.
The poor quality of clinical data generated in Mexicali B.C. is a concern, in the sense that influenza is not recorded as such, and ARIs are over- and under-reported. In addition, ARIs are being over- and under-reported; this is done weekly rather than daily. This results in unavailability of data at hand. In other words, it takes a year for the data to become available. Deaths are not reported on a daily basis, but they can be extracted from the official files, since the date and time of death are recorded. There is no coordination between the Imperial Valley and Mexicali B.C. to generate this type of database jointly and integrally. None of the current official epidemiological surveillance systems in Mexicali B.C. and/or Imperial Valley investigate whether the cause of death may have been air pollution exposure or exposure to other sources of pollution.
In order to achieve models that explain the effects in the most reliable way possible, in an expeditious manner, and in a local binational manner, it is necessary to correct the aspects mentioned above, among others. The region does not have an integrated, binational surveillance system that addresses morbidity and mortality cases due to exposure to air pollution, as proposed in this paper.
With the realization of this project, it would result in making the data more practical for conducting research studies and knowing the effects on mortality from all causes except external ones due to the exposure of the local population to the most relevant air pollutants (see Section 3.4).
If an integral, binational, unified system were established (such as the one proposed in this work), it would be possible to know the effects of each pollutant and how they affect the health of the local population, by the features such as the city areas, age groups, sex, type of disease, or cause of death, etc., giving reliable results 365 days a year, since the collection, organization, provision, and communication of the data would be carried out on a daily basis throughout the year. After the first three years of implementing this binational, unified system, there would be enough information to be able to estimate, with quality, the first effects of air pollution on the health of our population.
Finally, it is necessary to emphasize the importance of the administrative and management parts to achieve this type of action. Cooperation and planning are necessary between local organizations and institutions that exist as independent entities; there is a need to build relationships to focus on the purpose of addressing problems that, due to their complexity, cannot be addressed unilaterally. At the same time, the aim is to eliminate the barriers imposed by not having differentiated legal systems and institutional procedures, despite sharing the same geographic region, as well as all the environmental and public health implications.
A limitation of this work is that it requires huge cooperation and organization from both border cities in order to accomplish the goal. Logistical problems and protocols concerning data quality and availability have been addressed. However, costs and economic logistics have not been considered for the implementation of this project.
5. Conclusions
This paper has made it possible to carefully examine both the air quality monitoring information system, as well as the health conditions that occur in the population of both border cities. In the same way, suggestions have been made objectively, thinking about the integration of a binational system between both countries. The challenges faced in realizing a binational integrated system with the features proposed here are not impossible to resolve, if a panel of multidisciplinary experts in the environment, health, legal, and regulatory fields can be formed, to show the virtues of this system to environmental health decision-makers on both sides of the border. Mexicali B.C. must improve its data acquisition system at the monitoring stations, in addition to speeding up the access time to the data. It should also improve protocols for recording clinical data in health units to provide real-time access through publicly available databases. Even more, the statistical results obtained in the reviewed published articles reinforce the effect of the main pollutants analyzed (O3, CO, PM10, and PM2.5, among others) on the population’s health registered in Mexicali B.C.; however, with the implementation of a binational system with the characteristics proposed in this work, the reliability of the results in this type of study (i.e., air pollution vs. population’s health) would improve even more. Most importantly, the contribution of this work has a positive impact on improvements and care for the environment to reduce the emission of pollutants and the harmful damage that they can have on the population on both sides of the border. In terms of future work, an economic analysis may be needed to assess the feasibility of its implementation in subsequent years. It could also help as a starting point for implementation in other countries with binational or multinational borders to solve problems other than air pollution.
Author Contributions
Conceptualization, M.A.R. and D.C.-G.; methodology, M.A.R. and D.C.-G.; validation, E.C.N., J.V.M. and M.L.N.; formal analysis, M.A.R., D.C.-G. and R.L.A.; investigation, M.A.R., D.C.-G., R.L.A., E.C.N., J.V.M. and M.L.N.; writing—original draft preparation, M.A.R. and D.C.-G.; writing—review and editing, M.A.R., D.C.-G. and R.L.A.; visualization, R.L.A., E.C.N., J.V.M. and M.L.N.; supervision, M.A.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Binational Nogales Wash United States/Mexico Groundwater Monitoring Program. International Boundary and Water Commission between Mexico and the U.S.A. Nogales, Arizona-Sonora, U.S.A.–Mexico. 18 January 2000. Available online: https://ibwc.gov/Files/Bi_Nogales_Wash_US_MX_GW_%20Monitoring_Program_082001.pdf (accessed on 3 February 2023).
- Michelle, W.; Stephen, W.; Carlos, A.; Veronica, C.; Pablo, K.; Luis, A.; Chris, P.; Alejandro, E.; Ernesto, R.; Ana, F.; et al. The U.S.-Mexico Border Infectious Disease Surveillance project: Establishing binational border surveillance. Emerg. Infect. Dis. 2003, 9, 97–102. Available online: https://investigadores.unison.mx/es/publications/the-us-mexico-border-infectious-disease-surveillance-project-esta (accessed on 3 February 2023).
- Border Task Force Report. Arrowhead Center, New Mexico, U.S.A. July 2022. Available online: https://arrowheadcenter.nmsu.edu/reports/border-report/border-tasks-force-report-paso-del-norte-region.pdf (accessed on 3 February 2023).
- Luzma, N. The Transboundary Paso del Norte Region: Stakeholders’ Preferences Allowing Water Resources Adaptation. Integrated Water Resource Management, 1st ed.; Edson, O., Samuel, S., Valmir, A., Pablo, O.J., Eds.; Springer: Cham, Switzerland, 2020; pp. 73–84. Available online: https://www.researchgate.net/publication/333756936_The_Transboundary_Paso_del_Norte_Region_Stakeholders%27_Preferences_Allowing_Water_Resources_Adaptation (accessed on 3 February 2023).
- Rogelio, R.; Kristin, E.; Melissa, L.; Purnima, M. Arizona–Sonora binational data sharing: The missing piece to the cervical cancer puzzle. Int. J. Gynecol. Cancer 2022, ijgc-2022. Available online: https://ijgc.bmj.com/content/early/2022/12/21/ijgc-2022-004181 (accessed on 3 February 2023).
- Horacio, R.; Agnes, S.; José, T.; Grea, M. Air pollution management and control in Latin America and the Caribbean: Implications for climate change. Rev. Panam. Salud Pública 2016, 40, 150–159. Available online: https://iris.paho.org/bitstream/handle/10665.2/31229/v40n3a2_150-%2059.pdf?sequence=1&isAllowed=y (accessed on 24 December 2022).
- World’s Most Polluted Cities in 2021—PM2.5 Ranking. Available online: https://www.iqair.com/world-most-polluted-cities (accessed on 24 December 2022).
- Mexican Goverment. Ley General del Equilibrio Ecológico y la Protección al Ambiente. 28 January 2012. Available online: https://biblioteca.semarnat.gob.mx/janium/Documentos/Ciga/agenda/DOFsr/148.pdf (accessed on 4 March 2023).
- Informe Nacional de la Calidad del Aire 2019. National Institute of Ecology and Climate Change, Ciudad de México, México. 2020. Available online: https://sinaica.inecc.gob.mx/archivo/informes/Informe2019.pdf (accessed on 2 February 2023).
- Alvaro, O.; Mario, S.; Adriana, Y. Progressive Interstitial Lung Disease Associated with Non Occupational Inhalation of Mineral Dusts. Rev. Investig. Clin.-Clin. Transl. Investig. 1986, 38, 59–63. [Google Scholar]
- Alvaro, O.; Norma, H.; Adriana, Y.; William, U.; Lila, O.; Arnold, B. Lung cell toxicity experimentally induced by a mixed dust from Mexicali, Baja California, México. Environ. Res. 1991, 56, 31–47. [Google Scholar]
- Alvaro, O.; Jesús, S.; Leonora, R.; Javier, M.; Claudia, G.; Marco, R.; Geraldine, F.; Miriam, Z.; Margarita, Q.; Inez, V.; et al. In Vitro biological effects of airborne PM2.5 and PM10 from a semi-desert city on the México–US border. Chemosphere 2011, 83, 618–626. [Google Scholar]
- Marco, R.; Miguel, B.; Roberto, L.; Efrain, C.; Martha, L. Relative risk of death from exposure to air pollutants: A short-term (2003–2007) study in Mexicali, Baja California, México. Int. J. Environ. Health Res. 2012, 22, 370–386. [Google Scholar]
- Marco, R.; Stephan, S.; Roberto, L.; Miguel, B.; Myrtha, R.; Martha, L.; Miriam, S.; Alvaro, O. Particulate matter air pollution effects on pulmonary tuberculosis activation in a semi-desert city on the US-Mexican border. Atmósfera 2020, 35, 545–556. [Google Scholar]
- Marco, R.; Mérida, J.V.; Alvaro, O.; Claudia, L.; Miguel, B.; Roberto, L.; Efrain, C. Association between personal PM10 exposure and pulmonary function in healthy volunteers from a semi-arid city on the US-Mexican border. Rev. Int. Contam. Ambient. 2018, 34, 583–595. [Google Scholar]
- Marco, R.; Efrain, N.; Martha, N.; Esmeralda, T. An estimation of costs and public-health benefits by the PM10 mitigation in Mexicali, Baja California, México. Rev. Int. Contam. Ambient. 2017, 33, 117–129. [Google Scholar]
- Marco, R. Un Sistema de Vigilancia Binacional como Indicador de los Efectos de la Contaminación Aérea Sobre la Salud Ambiental del Municipio de Mexicali y Valle Imperial; Technical Report; LASPAU, Academic and Professional Programs for the Americas: Mexicali, Mexico, 2015. [Google Scholar] [CrossRef]
- Katherine, D.; Marco, R. Binational Surveillance of Air Pollution Related Illnesses in Imperial County and the Municipality of Mexicali; Border Environmental Research Report, Baja California and Imperial County, California. October 2005. Available online: https://archive.epa.gov/ehwg/web/pdf/binational_surveillance.pdf (accessed on 30 January 2023).
- Marco, R.; Margarito, Q.; Kimberly, C. Correlation Study of the Association of PM10 with the Main Respiratory Diseases in the Populations of Mexicali. Rev. Mex. Ing. Biomed. 2005, 26, 22–36. [Google Scholar]
- Margarito, Q.; Marco, R.; Kimberly, C.; Saul, G.; Bill, P.; Alberto, M. Issues Related to Air Quality and Health in the California–Baja California Border Region; San Diego State University Press: San Diego, CA, USA, 2006; Volume 14, pp. 1–46. Available online: https://www.researchgate.net/publication/236672882_Issues_Related_to_Air_Quality_and_Health_in_the_California-Baja_California_Border_Region (accessed on 30 January 2023).
- Julio, L. Air Quality and Economic Development along the California/Baja California Border: Can We Have Both? In Proceedings of the San Diego Dialogue’s Forum Fronterizo, San Diego, CA, USA, 22 October 2002; Available online: https://drive.google.com/file/d/1ELDi9sNnoDg23tyTFQRJy7xMMaKPITUn/view?usp=share_link (accessed on 30 January 2023).
- Government of the State of Baja California. Baja California/California: Boletín del Grupo de Trabajo Regional. Programa Ambiental Frontera 2012 México–Estados Unidos, Autumn of 2007. pp. 1–10. Available online: https://drive.google.com/file/d/14EzRy2ddoM3TktynSGaoIe0ThbDdBGNc/view (accessed on 30 January 2023).
- Programa para Mejorar la Calidad del Aire en Mexicali. Government of the State of Baja California, Mexicali Baja California, México. 2011. Available online: http://www.spabc.gob.mx/wp-content/uploads/2017/10/PROGRAMA-PARA-MEJORAR-LA-CALIDAD-DEL-AIRE-EN-MEXICALI-PROAIRE-MEXICALI-2011-2020.pdf (accessed on 24 December 2022).
- En 12 años, Contaminación del Aire creció 30%. El Sol de Tijuana. 21 February 2019. Available online: https://www.elsoldetijuana.com.mx/local/en-12-anos-contaminacion-del-aire-en-mexicali-crecio-30-3087687.html (accessed on 24 December 2022).
- Análisis de la Calidad del Aire en cuanto a PM2.5 y datos Meteorológicos: Calexico, California y Mexicali, Baja California. California Air Resources Board, CA, USA. 2019. Available online: https://www.bajacalifornia.gob.mx/Documentos/sest/desarrollo_sustentable/Programas_Proyectos/Calidad_Aire/Analisis-de-la-calidad-del-aire-Mexicali-Calexico-2019.PDF (accessed on 24 December 2022).
- Calidad del Aire en Tijuana y Mexicali. Government of the State of Baja California. Available online: https://www.bajacalifornia.gob.mx/Prensa/Noticia/8861 (accessed on 24 December 2022).
- Imperial Valley Air Quality. Available online: http://www.imperialvalleyair.org/ (accessed on 24 December 2022).
- The Weather Channel. Available online: https://weather.com/ (accessed on 24 December 2022).
- National Weather Service: National Oceanic and Atmospheric Administration. Available online: http://www.wrh.noaa.gov (accessed on 24 December 2022).
- The Weather Channel. Available online: http://espanol.weather.com/weather/climatology/USCA0508 (accessed on 24 December 2022).
- Manual de Procedimientos Estandarizados para la Notificación Semanal de Casos Nuevos (SUIVE). Federal Government of Mexico, City of México, México, September 2012. Available online: https://epidemiologiatlax.files.wordpress.com/2013/08/28_2012_manual_suive.pdf (accessed on 3 February 2023).
- Manual de Procedimientos Estandarizados para el Sistema Estadístico Epidemiológico de las Defunciones (SEED). Federal Government of Mexico, City of Mexico, México. September 2012. Available online: https://epidemiologiatlax.files.wordpress.com/2013/08/26_2012_manual_seed.pdf (accessed on 3 February 2023).
- Reporte Anual: 2006 Programa Fronterizo de Monitoreo del Aire California–México. Government of the State of Baja California, Tijuana, Baja California, México. 2006. Available online: https://web.archive.org/web/20090411000743/http://www.bajacalifornia.gob.mx:80/spa/doctos/Reporte_Anual_2006.pdf (accessed on 3 February 2023).
- PAHO and EPA (2004–2005), Bi-National Tracking Network of Environmentally Related Diseases. Available online: https://web.archive.org/web/20170210223345/https://archive.epa.gov/ehwg/web/pdf/binational_tracking_network_of_environmentally_related_diseases.pdf (accessed on 24 December 2022).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).