
Impacts of Air Pollution and Dampness on Occupant Respiratory Health in Unplanned Houses: A Case Study of Bandung, Indonesia



Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire Survey: Household Attributes and Self-Reported Health Conditions
2.2. Field Measurement: Indoor and Outdoor Air Quality
2.3. Statistical Analysis
3. Results and Discussion
3.1. Household Survey
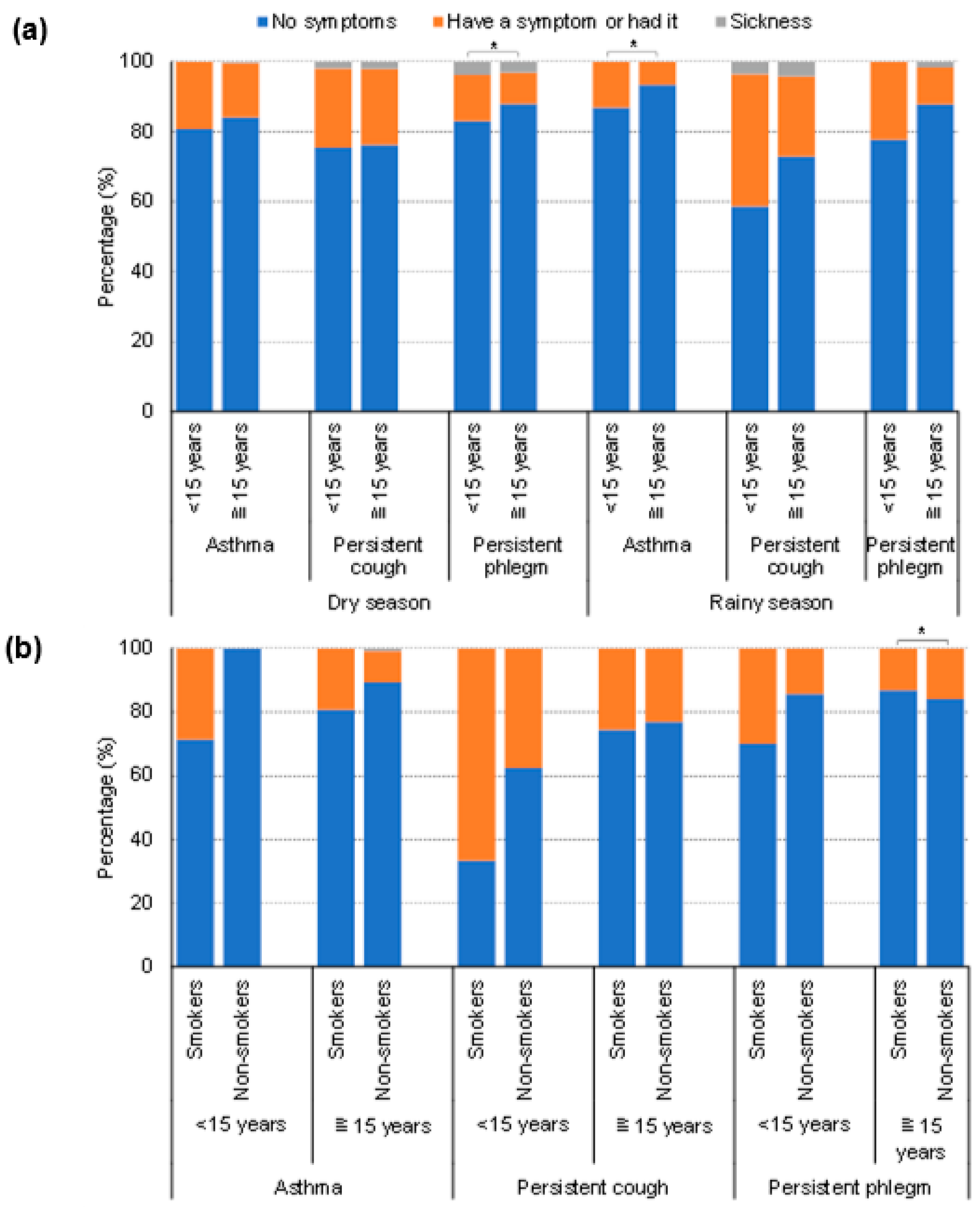
3.2. Self-Reported Respiratory Health
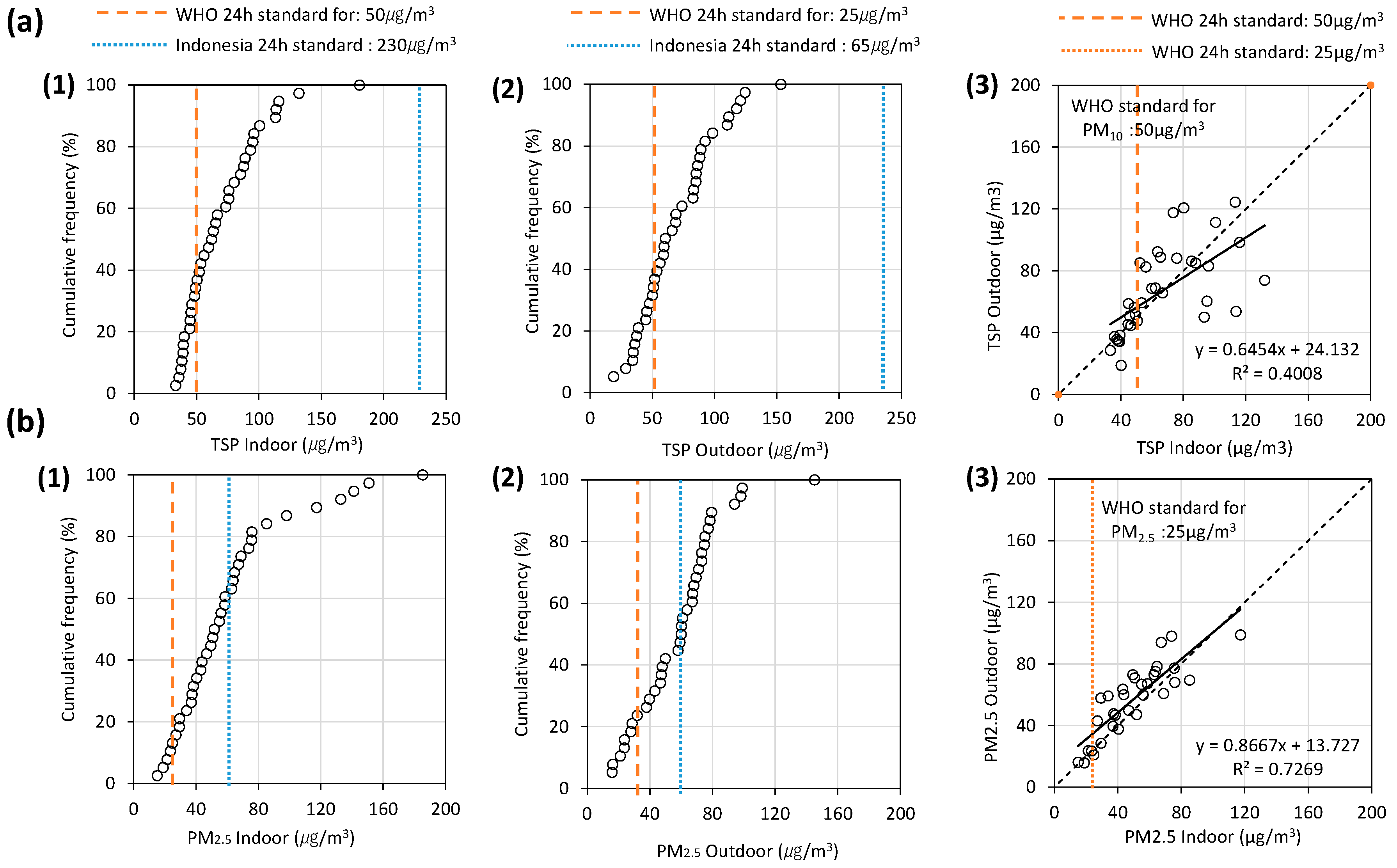
3.3. Field Measurement
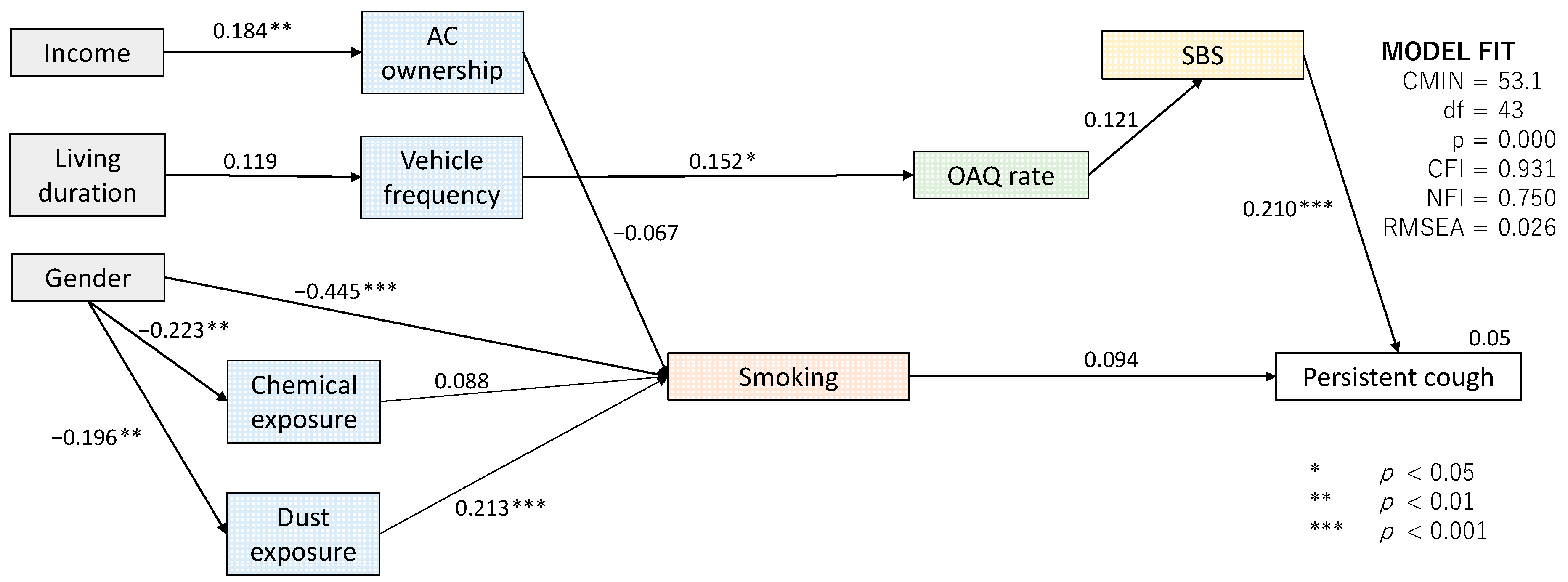
3.4. Factors Impacting Occupant Respiratory Health Symptoms
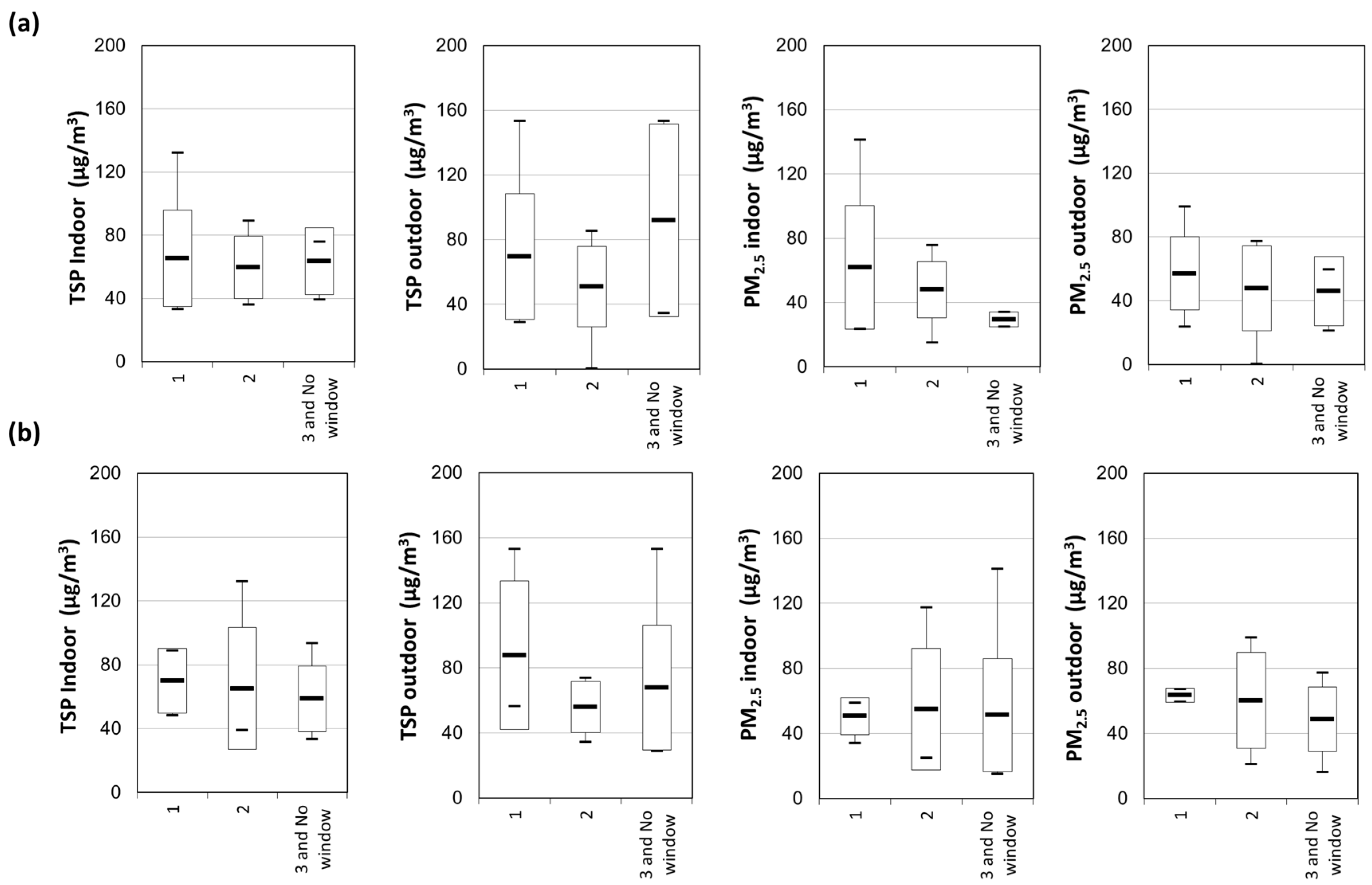
3.5. Window-Opening Behavior in Kampung Houses
4. Conclusions
- The symptoms of respiratory health problems were higher among children, particularly in the rainy season. The percentage of persistent cough symptoms was found to be more than 40% among those under 15 years old during the rainy season, whereas that of 15 years and over was 27%.
- Kampung houses were observed to suffer from severe mold risk. More than 97% of the houses were highly likely to have a mold propagation in the rainy season. Even in the dry season, the outdoor RH can be as high as 80% on average and approximately 79% of houses had a mold risk, and 68% was considered a high possibility of propagation. The outdoor RH averaged at 83%, while the corresponding indoor RH averaged at 82% during the rainy season. Water leakages were reported by 50% and 60% of the respondents in the dry and rainy seasons, respectively.
- The concentrations of indoor TSP and PM2.5 far exceeded the WHO standards in more than 50% of the kampung houses, whereas the outdoor air pollution within kampungs contributed to the degraded IAQ.
- Opening windows in the bedroom negatively affected mite occurrence and humidity rate. Furthermore, a longer duration of opening windows in the bedroom showed a lower concentration of PM2.5, while that in the living room was the other way around, i.e., a longer duration of opening windows showed a higher concentration of PM2.5.
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Lueker, J.; Bardhan, R.; Sarkar, A.; Norford, L. Indoor air quality among Mumbai’s resettled populations: Comparing Dharavi slum to nearby rehabilitation sites. Build. Environ. 2019, 167, 106419. [Google Scholar] [CrossRef]
- Romieu, I.; Samet, J.M.; Smith, K.R.; Bruce, N. Outdoor air pollution and acute respiratory infections among children in developing countries. J. Occup. Environ. Med. 2002, 44, 640–649. [Google Scholar] [CrossRef] [PubMed]
- Bornehag, C.-G.; Sundell, J.; Sigsgaard, T. Dampness in buildings and health (DBH): Report from an ongoing epidemiological investigation on the association between indoor environmental factors and health effects among children in Sweden. Indoor Air 2004, 14, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Sundell, J. Reflections on the history of indoor air science, focusing on the last 50 years. Indoor Air 2017, 27, 708–724. [Google Scholar] [CrossRef]
- Takaoka, M.; Norback, D. The Home Environment of Japanese Female University Students—Association with Respiratory Health and Allergy. Indoor Built Environ. 2011, 20, 369–376. [Google Scholar] [CrossRef]
- Wang, L.; Qu, F.; Zhang, Y.; Weschler, L.B.; Sundell, J. Home environment in relation to allergic rhinitis among preschool children in Beijing, China: A cross-sectional study. Build. Environ. 2015, 93, 54–63. [Google Scholar] [CrossRef]
- WHO. WHO Guidelines for Air Quality Dempess and Mould; WHO Regional Office for Europe: Scherfigsvej, Denmark, 2009; p. 248. [Google Scholar]
- Choi, J.; Chun, C.; Sun, Y.; Choi, Y.; Kwon, S.; Bornehag, C.; Sundell, J. Associations between building characteristics and children’s allergic symptoms—A cross-sectional study on child’s health and home in Seoul, South Korea. Build. Environ. 2014, 75, 176–181. [Google Scholar] [CrossRef]
- Hägerhed-Engman, L.; Bornehag, C.-G.; Sundell, J. Building characteristics associated with moisture related problems in 8,918 Swedish dwellings. Int. J. Environ. Health Res. 2009, 19, 251–265. [Google Scholar] [CrossRef]
- Hu, Y.; Liu, W.; Huang, C.; Zou, Z.J.; Zhao, Z.H.; Shen, L.; Sundell, J. Home dampness, childhood asthma, hay fever, and airway symptoms in Shanghai, China: Associations, dose-response relationships, and lifestyle’s influences. Indoor Air 2014, 24, 450–463. [Google Scholar] [CrossRef]
- Sun, Y.; Zhang, Y.; Sundell, J.; Fan, Z.; Bao, L. Dampness in dorm rooms and its associations with allergy and airways infections among college students in China: A cross-sectional study. Indoor Air 2009, 19, 348–356. [Google Scholar] [CrossRef]
- Larsson, M.; Weiss, B.; Janson, S.; Sundell, J.; Bornehag, C.-G. Associations between indoor environmental factors and parental-reported autistic spectrum disorders in children 6–8 years of age. NeuroToxicology 2009, 30, 822–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisk, W.J.; Lei-Gomez, Q.; Mendell, M.J. Meta-analyses of the associations of respiratory health effects with dampness and mold in homes. Indoor Air 2007, 17, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Gunnbjörnsdottir, M.; Norbäck, D.; Plaschke, P.; Norrman, E.; Björnsson, E.; Janson, C. The relationship between indicators of building dampness and respiratory health in young Swedish adults. Respir. Med. 2003, 97, 302–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ignatavičius, Č.; Ignatavičius, G. Investigation of Damage and Microclimate Deterioration Caused by Dampness in the Palace of Signatories to the Declaration of Independence. Indoor Built Environ. 2005, 14, 89–95. [Google Scholar] [CrossRef]
- Jaakkola, J.J.K.; Hwang, B.-F.; Jaakkola, N. Home Dampness and Molds, Parental Atopy, and Asthma in Childhood: A Six-Year Population-Based Cohort Study. Environ. Health Perspect. 2005, 113, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Sahlberg, B.; Wieslander, G.; Janson, C.; Gislason, T.; Norback, D. Dampness and moulds in workplace buildings: Associations with incidence and remission of sick building syndrome (SBS) and biomarkers of inflammation in a 10year follow-up study. Sci. Total Environ. 2012, 430, 75–81. [Google Scholar] [CrossRef]
- Hsu, N.-Y.; Lee, C.-C.; Wang, J.-Y.; Li, Y.-C.; Chang, H.-W.; Chen, C.-Y.; Bornehag, C.-G.; Wu, P.-C.; Sundell, J.; Su, H.-J. Predicted risk of childhood allergy, asthma, and reported symptoms using measured phthalate exposure in dust and urine. Indoor Air 2011, 22, 186–199. [Google Scholar] [CrossRef]
- Naydenov, K.; Melikov, A.; Markov, D.; Stankov, P.; Bornehag, C.-G.; Sundell, J. A comparison between occupants’ and inspectors’ reports on home dampness and their association with the health of children: The ALLHOME study. Build. Environ. 2008, 43, 1840–1849. [Google Scholar] [CrossRef]
- Smedje, G.; Norbäck, D. Asthmatic Symptoms in School Children in Relation to Building Dampness and Atopy. Indoor Built Environ. 2003, 12, 249–250. [Google Scholar] [CrossRef]
- Sun, Y.; Sundell, J. Life style and home environment are associated with racial disparities of asthma and allergy in Northeast Texas children. Sci. Total Environ. 2011, 409, 4229–4234. [Google Scholar] [CrossRef]
- Sun, Y.; Sundell, J. On Associations between Housing Characteristics, Dampness and Asthma and Allergies among Children in Northeast Texas. Indoor Built Environ. 2013, 22, 678–684. [Google Scholar] [CrossRef]
- Tham, K.W.; Zuraimi, M.S.; Koh, D.; Chew, F.T.; Ooi, P.L. Associations between home dampness and presence of molds with asthma and allergic symptoms among young children in the tropics. Pediatr. Allergy Immunol. 2007, 18, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Haq, G.; Han, W.; Kim, C.; Vallack, H. Benchmarking Urban Air Quality Management and Practice in Major and Mega Cities of Asia; Air Pollution in the Megacities of Asia (APMA): Seoul, Korea, 2002. [Google Scholar]
- Deng, T.; Shen, X.; Cheng, X.; Liu, J. Investigation of window-opening behaviour and indoor air quality in dwellings situated in the temperate zone in China. Indoor Built Environ. 2020, 30, 938–956. [Google Scholar] [CrossRef]
- Lin, H.H.; Ezzati, M.; Murray, M. Tobacco smoke, indoor air pollution and tuberculosis: A systematic review and meta-analysis. PLoS Med. 2007, 4, 0173–0189. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Hu, Z.; Liu, M.; Yang, H.; Kong, Q.; Liu, Y. Review of research on air-conditioning systems and indoor air quality control for human health. Int. J. Refrig. 2008, 32, 3–20. [Google Scholar] [CrossRef]
- Demographia. Demographia World Urban Areas. 2017. Available online: http://www.demographia.com/db-worldua.pdf (accessed on 18 January 2022).
- Funo, S.; Yamamoto, N.; Silas, J. Typology of Kampung Houses and Their Transformation Process—A Study on Urban Tissues of an Indonesian City. J. Asian Archit. Build. Eng. 2018, 7581, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Parisi, C.D.A.; Kubota, T.; Surahman, U. Affordable modifications for sustainable houses in urban informal settlements: A case study of Bandung, Indonesia. Int. J. Urban Sustain. Dev. 2021, 13, 659–689. [Google Scholar] [CrossRef]
- Paramita, B.; Suparta, W. Alteration of Urban Microclimate in Bandung, Indonesia Based on Urban Morphology. Geogr. Tech. 2019, 14, 213–220. [Google Scholar] [CrossRef]
- Tarigan, A.; Sagala, S.; Samsura, D.A.; Fiisabiilillah, D.F.; Simarmata, H.A.; Nababan, M. Bandung City, Indonesia. Cities 2016, 50, 100–110. [Google Scholar] [CrossRef]
- Paramita, B.; Fukuda, H. Building Groups Design Strategies in Hot-humid Climate: A Dense Residential Planning in Bandung, Indonesia. In PLEA 2013: Sustainable Architecture for a Renewable Future; IRB-Verlag: Stuttgart, Germany, 2013. [Google Scholar]
- Indonesia’s Kampung Improvement Program: Policy Issues and Local Impacts for Secondary Cities. J. Plan. Educ. Res. 1989, 9, 79–83. [CrossRef]
- BRE. Condensation and Dampness; IHS BRE Press: London, UK, 2007. [Google Scholar]
- Bai, L.; Li, C.; Yu, C.W.; He, Z. Air pollution and health risk assessment in Northeastern China: A case study of Jilin Province. Indoor Built Environ. 2021, 30, 1857–1874. [Google Scholar] [CrossRef]
- Fu, X.; Norbäck, D.; Yuan, Q.; Li, Y.; Zhu, X.; Hashim, J.H.; Hashim, Z.; Ali, F.; Zheng, Y.-W.; Lai, X.-X.; et al. Indoor microbiome, environmental characteristics and asthma among junior high school students in Johor Bahru, Malaysia. Environ. Int. 2020, 138, 105664. [Google Scholar] [CrossRef] [PubMed]
- Norbäck, D.; Hashim, J.H.; Hashim, Z.; Cai, G.-H.; Sooria, V.; Ismail, S.A.; Wieslander, G. Respiratory symptoms and fractional exhaled nitric oxide (FeNO) among students in Penang, Malaysia in relation to signs of dampness at school and fungal DNA in school dust. Sci. Total Environ. 2017, 577, 148–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norbäck, D.; Hashim, Z.; Ali, F.; Hashim, J.H. Asthma symptoms and respiratory infections in Malaysian students-associations with ethnicity and chemical exposure at home and school. Environ. Res. 2021, 197, 111061. [Google Scholar] [CrossRef]
- Yap, J.; Toh, Z.A.; Goh, V.; Ng, L.C.; Vesper, S. Assessment of mold concentrations in Singapore shopping centers using mold-specific quantitative PCR (MSQPCR) analysis. Indian J. Microbiol. 2009, 49, 290–293. [Google Scholar] [CrossRef] [Green Version]
- Zuraimi, M.; Tham, K. Indoor air quality and its determinants in tropical child care centers. Atmos. Environ. 2007, 42, 2225–2239. [Google Scholar] [CrossRef]
- Hu, J.; Li, N.; Zou, S.; Yoshino, H.; Yanagi, U.; Yu, C.W.; Qu, H. Indoor environmental conditions in schoolchildren’s homes in central-south China. Indoor Built Environ. 2019, 29, 956–971. [Google Scholar] [CrossRef]
- Manivannan, S.; Venugopal, V.; Kindo, A.J.; Kuppuswamy, R. Method for assessment of indoor household dampness for its use in epidemiological studies in tropical settings. Ann. Trop. Med. Public Health 2017, 10, 966. [Google Scholar] [CrossRef]
- Bandung, B. Bandung City Figure; BPS: Bandung, Indonesia, 2016. Available online: https://bandungkota.bps.go.id/subject/151/iklim.html#subjekViewTab3 (accessed on 31 January 2022).
- Portal Data Kota Bandung. Tahun 2017—Data Jumlah Unit Bangunan dan Keteraturan Bangunan Hunian Per RT; Dinas Perumahan dan Kawasan Permukiman, Pertanahan dan Pertamanan: Bandung, Indonesia, 2019. [Google Scholar]
- Ferris, B.G. Epidemiology Standardization Project (American Thoracic Society). Am. Rev. Respir. Dis. 1978, 118 Pt 2, 1–120. [Google Scholar]
- Enright, P.L.; Kronmal, R.A.; Higgins, M.W.; Schenker, M.B.; Haponik, E.F. Prevalence and Correlates of Respiratory Symptoms and Disease in the Elderly. Chest 1994, 106, 827–834. [Google Scholar] [CrossRef]
- Langkulsen, U.; Jinsart, W.; Karita, K.; Yano, E. Respiratory symptoms and lung function in Bangkok school children. Eur. J. Public Health 2006, 16, 676–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nkosi, V.; Voyi, K. Reliability of an adult respiratory symptom questionnaire in a community located near a mine dump in South Africa: Pilot study. South. Afr. J. Infect. Dis. 2016, 31, 103–105. [Google Scholar] [CrossRef]
- Abe, K. A Method For Numerical Characterization Of Indoor Climates By A Biosensor Using A Xerophilic Fungus. Indoor Air 1993, 3, 344–348. [Google Scholar] [CrossRef]
- Abe, K. Assessment of the environmental conditions in a museum storehouse by use of a fungal index. Int. Biodeterior. Biodegrad. 2010, 64, 32–40. [Google Scholar] [CrossRef]
- Abe, K. Assessment of home environments with a fungal index using hydrophilic and xerophilic fungi as biologic sensors. Indoor Air 2011, 22, 173–185. [Google Scholar] [CrossRef]
- Hildebrandt, S.; Kubota, T.; Sani, H.A.; Surahman, U. Indoor Air Quality and Health in Newly Constructed Apartments in Developing Countries: A Case Study of Surabaya, Indonesia. Atmosphere 2019, 10, 182. [Google Scholar] [CrossRef] [Green Version]
- Using a Protimeter Moisture Meter to Check Damp within a Building Using a Protimeter Moisture Meter. 2015. Available online: https://www.damp-meter-direct.co.uk (accessed on 7 July 2022).
- Chicea, D.; Leca, C.; Olaru, S.; Chicea, L. An Advanced Sensor for Particles in Gases Using Dynamic Light Scattering in Air as Solvent. Sensors 2021, 21, 5115. [Google Scholar] [CrossRef]
- Sinclair, D. Light Scattering Instruments as an Aid in Air Pollution Measurements. Air Repair 1953, 3, 51–56. [Google Scholar] [CrossRef]
- Olobatuyi, M.E. A User’s Guide to Path Analysis; University Press of America: Lanham, MD, USA, 2006. [Google Scholar]
- Kota Bandung Dalam Angka; Badan Pusat Statistik Kota Bandung Bps-Statistics of Bandung Municipality: Bandung, Indonesia, 2020.
- Statistik Indonesia 2020. Bandan Pusat Statistik Indonesia. 2020. ISSN 0126-2912. Available online: https://www.bps.go.id/publication/2020/04/29/e9011b3155d45d70823c141f/statistik-indonesia-2020.html (accessed on 19 July 2022).
- Provinsi Jawa Barat Dalam Angka Jawa Barat Province in Figures 2020 Penyediaan Data untuk Perencanaan Pembangunan Delivering Data to Inform Development Planning. 2020. Available online: https://jabar.bps.go.id/publication/2020/04/27/cfab9a400cf304f800182a5f/provinsi-jawa-barat-dalam-angka-2020.html (accessed on 17 July 2022).
- Schramm, S.; Carré, V.; Scheffler, J.-L.; Aubriet, F. Active and passive smoking—New insights on the molecular composition of different cigarette smoke aerosols by LDI–FTICRMS. Atmos. Environ. 2014, 92, 411–420. [Google Scholar] [CrossRef]
- Smoking Rates by Country. 2022. Available online: https://worldpopulationreview.com/country-rankings/smoking-rates-by-country (accessed on 11 May 2022).
- Gent, J.F.; Kezik, J.M.; Hill, M.E.; Tsai, E.; Li, D.-W.; Leaderer, B.P. Household mold and dust allergens: Exposure, sensitization and childhood asthma morbidity. Environ. Res. 2012, 118, 86–93. [Google Scholar] [CrossRef] [Green Version]
- Fabi, V.; Andersen, R.V.; Corgnati, S.; Olesen, B.W. Occupants’ window opening behaviour: A literature review of factors influencing occupant behaviour and models. Build. Environ. 2012, 58, 188–198. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Samples | Dry Season (September–November 2018) | Rainy Season (March–April 2019) | Dry Season (September–November 2019) | Total | |
|---|---|---|---|---|---|
| Questionnaires | ATS-DLD-78 | 333 | 266 | - | 599 |
| Measurements | Mold risk | 34 | 34 | 34 | 102 |
| TSP and PM2.5 | 38 | 38 |
| Questionnaire | Factors/Scales | Details |
|---|---|---|
| House’s and respondent’s information | Personal attributes | Age, gender, occupation, asthma (past/present), eczema (past/present), allergic symptoms (past/present), stress level (10-point scale), other diseases |
| Household attributes | Established year, living duration, cleaning habits, furniture conditions, household income | |
| Indoor air quality | Smell sensation (past/present), humidity sensation (10-point scale), mold and water leakage occurrence (past/present), mite observation (past/present), air quality sensation (indoor and outdoor, 10-point scale) | |
| Detailed cooling behavior | Windows-opening behavior, AC and fan availability and usage |
| Measured Variable | Instrument Model | Accuracy |
|---|---|---|
| Air temperature, relative humidity | T&D TR-72Ui | Accuracy: ±0.3 °C, ±5% RH Resolution: 0.1 °C, 1% RH Range: 0~50 °C, 10~95% |
| Air temperature, relative humidity, air pressure | T&D TR-73U | Accuracy: ±0.3 °C, ±5% RH Resolution: 0.1 °C, 1% RH, 1 hpa Range: 0~50 °C, 10~95%, 750~1100 hpa |
| TSP, PM2.5 | SIBATA LD-5R cyclone granulator for PM2.5 | Accuracy: ±10% (relative to standard particles) Range: 0.001~10,000 mg/m3 (for standard particles) |
| Mold risk | Fungal risk detector | The error range for mold index measurement at constant temperature and humidity is a few percent (up to 20 percent). Measurable range: fungal index from 8 to 70.5 for one week 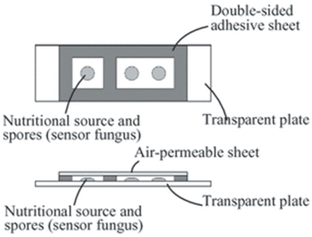 Source: Abe [52] |
| Whole | <15 Years | ≥15 Years | Sig. | Dry Season | Rainy Season | Sig. | |||
|---|---|---|---|---|---|---|---|---|---|
| n = 599 | n = 101 | n = 497 | n = 333 | n = 266 | |||||
| Personal attributes | Age | Years (mean) | 36.3 | 6.9 | 42.4 | 0.000 | 35.9 | 36.9 | 0.617 |
| Duration | Years (mean) | 26.4 | 22.9 | 26.8 | 0.036 | 28.3 | 23.6 | 0.005 | |
| Gender (%) | Male/Female | 45.8/53.5 | 52.3/47.7 | 44.7/54.5 | 0.020 | 45.1/53.6 | 46.7/53.3 | 0.824 | |
| Income (US$) (%) | <150 | 27.9 | 23.1 | 28.8 | 0.076 | 34.9 | 18.8 | 0.984 | |
| 150–450 | 56.3 | 60.0 | 55.7 | 48.3 | 67.0 | ||||
| 450–750 | 10.3 | 9.2 | 10.4 | 8.8 | 12.2 | ||||
| >750 | 5.5 | 7.7 | 5.1 | 8.0 | 2.0 | ||||
| Occupation (%) | Government | 0.9 | 1.1 | 0.082 | 0.9 | ||||
| Private | 18.9 | 21.6 | 18.9 | ||||||
| Entrepreneur | 15.5 | 18.3 | 15.5 | ||||||
| Student | 20.1 | 81.6 | 10.6 | 20.1 | |||||
| Housewife | 26.9 | 31.1 | 26.9 | ||||||
| Retired | 6.5 | 7.7 | 6.5 | ||||||
| Other | 10.5 | 18.4 | 9.2 | 10.5 | |||||
| Worked for a year or more in dusty job | (%) | 39.9 | 39.9 | 0.439 | 29.1 | 49.0 | 0.001 | ||
| Exposed to gas or chemical fumes in work | (%) | 19.7 | 19.7 | 0.616 | 16.9 | 22.3 | 0.299 | ||
| Behavior | Window opening in bedroom | Hours (Average) | 9.0 | 8.3 | 9.1 | 0.424 | 8.6 | 9.6 | 0.234 |
| Window opening in living room | Hours (Average) | 12.1 | 13.5 | 11.8 | 0.301 | 13.8 | 9.0 | 0.000 | |
| Smoking behavior (%) | Active | 39.7 | 38.5 | 35.9 | 32.3 | 49.7 | 0.000 | ||
| Passive | 13.6 | 30.8 | 15.4 | 13.9 | 13.2 | 0.018 | |||
| Non-smoker | 46.7 | 30.8 | 48.7 | 53.8 | 37.1 | ||||
| Frequency of cleaning rooms (%) | Every day | 90.8 | 92.6 | 90.5 | 0.630 | 87.3 | 96.6 | 0.057 | |
| Several times per week | 5.3 | 2.5 | 5.8 | 7.9 | 1.0 | ||||
| Every week | 0.8 | 1.2 | 0.7 | 1.2 | 0.0 | ||||
| 2–3 times per month | 1.7 | 2.5 | 1.5 | 2.7 | 0.0 | ||||
| Once per month or less | 1.5 | 1.2 | 1.5 | 0.9 | 2.5 | ||||
| Frequency of cleaning bathroom (%) | Every day | 63.2 | 72.7 | 62.3 | 0.118 | 62.2 | 64.0 | 0.060 | |
| Several times per week | 25.9 | 27.3 | 25.8 | 20.5 | 30.0 | ||||
| Every week | 8.6 | 9.5 | 12.8 | 5.4 | |||||
| 2–3 times per month | 1.1 | 1.2 | 2.6 | ||||||
| Once per month or less | 1.1 | 1.2 | 1.9 | 0.5 | |||||
| Health | Asthma | (%) | 13.8 | 15.7 | 13.5 | 0.878 | 13.8 | ||
| Hay fever | (%) | 30.8 | 20.7 | 33.0 | 0.199 | 30.8 | |||
| Eczema | (%) | 13.5 | 10.9 | 14.1 | 0.433 | 13.5 | |||
| Allergy | (%) | 13.6 | 9.4 | 14.4 | 0.468 | 13.6 | |||
| None | (%) | 55.2 | 61.0 | 49.5 | 55.2 | ||||
| Disease | (%) | 18.0 | 1.8 | 21.6 | 0.000 | 18.0 | |||
| SBS | (%) | 4.3 | 0.0 | 5.2 | 0.148 | 4.3 | |||
| Stress | (mean: 0 = no stress, 10 = very stressful) | 1.5 | 0.4 | 1.8 | 0.000 | 1.5 | |||
| Whole | <15 Years | ≥15 Years | Sig. | Dry Season | Rainy Season | Sig. | |||
|---|---|---|---|---|---|---|---|---|---|
| n = 599 | n = 101 | n = 498 | n = 333 | n = 266 | |||||
| Building attributes | Building age | Average age (years) | 40.7 | 39.7 | 40.8 | 0.264 | 39.0 | 41.9 | 0.305 |
| No. of windows in master bedroom (%) | 0 | 24.8 | 20.9 | 25.6 | 0.339 | 29.9 | 16.8 | 0.630 | |
| 1 | 51.6 | 58.2 | 50.3 | 48.0 | 57.1 | ||||
| >1 | 23.6 | 20.9 | 24.1 | 22.0 | 26.1 | ||||
| No. of windows in living room (%) | 0 | 32.1 | 34.4 | 31.7 | 0.141 | 37.6 | 22.5 | 0.000 | |
| 1 | 38.3 | 46.9 | 36.6 | 41.6 | 32.4 | ||||
| >1 | 29.6 | 18.8 | 31.7 | 20.4 | 43.0 | ||||
| HVAC system (%) | AC | 6.7 | 8.7 | 6.4 | 0.789 | 4.7 | 10.6 | 0.015 | |
| Fan in bedroom | 65.7 | 66.7 | 65.6 | 65.7 | |||||
| Ceiling/stand fan | 47.3 | 45.7 | 47.7 | 0.125 | 47.3 | ||||
| Exhaust fan | 17.9 | 27.3 | 19.7 | 0.062 | 17.9 | ||||
| Number of furniture in living room (%) | 0 | 4.3 | 2.0 | 4.8 | 0.975 | 4.3 | |||
| 1–5 | 86.2 | 88.2 | 85.7 | 86.2 | |||||
| >5 | 9.6 | 9.8 | 9.5 | 9.6 | |||||
| Number of furniture in bedroom (%) | 0 | 1.1 | 2.2 | 0.9 | 0.574 | 1.1 | |||
| 1–5 | 90.6 | 84.4 | 91.9 | 90.6 | |||||
| >5 | 8.2 | 13.3 | 7.2 | 8.2 | |||||
| Vehicle frequency (%) | Constantly | 22.7 | 22.7 | 0.013 | 13.0 | 31.9 | 0.000 | ||
| Frequency | 46.0 | 46.0 | 56.7 | 39.3 | |||||
| Seldom | 29.1 | 29.1 | 27.9 | 27.4 | |||||
| Never | 2.2 | 2.2 | 2.3 | 1.5 | |||||
| Dampness | Visual mold | (%) | 49.8 | 64.0 | 47.3 | 0.039 | 55.9 | 39.2 | 0.000 |
| Mite | (%) | 17.9 | 23.8 | 16.9 | 0.933 | 19.9 | 15.0 | 0.110 | |
| Water leakage | (%) | 53.7 | 58.4 | 52.8 | 0.344 | 50.2 | 59.9 | 0.033 | |
| Smell/Odor | (%) | 47.8 | 57.5 | 46.1 | 0.098 | 39.8 | 60.6 | 0.000 | |
| Humidity (%) | 0–3: (rather) dry | 21.6 | 19.4 | 22.0 | 0.045 | 21.4 | 22.1 | 0.544 | |
| 4–6: neutral | 46.6 | 43.1 | 47.2 | 44.3 | 50.3 | ||||
| 7–10: (rather) humid | 31.7 | 37.5 | 30.8 | 34.3 | 27.7 | ||||
| Perceived IAQ | IAQ (%) | 0–3: (rather) clean | 38.2 | 34.7 | 38.7 | 0.374 | 35.6 | 42.3 | 0.937 |
| 4–6: neutral | 46.1 | 46.7 | 45.9 | 47.1 | 44.4 | ||||
| 7–10: (rather) dirty | 15.8 | 18.7 | 15.3 | 17.3 | 13.3 | ||||
| OAQ (%) | 0–3: (rather) clean | 30.2 | 24.0 | 31.2 | 0.682 | 28.0 | 33.8 | 0.391 | |
| 4–6: neutral | 50.4 | 57.3 | 49.2 | 49.7 | 51.5 | ||||
| 7–10: (rather) dirty | 19.2 | 12.0 | 19.3 | 22.0 | 9.1 | ||||
| Annoyance from outdoor air pollution (%) | 0–3: not annoyed | 63.8 | 63.8 | 0.689 | 57.6 | 69.4 | 0.326 | ||
| 4–6: neutral | 26.0 | 26.0 | 34.3 | 18.7 | |||||
| 7–10: annoyed | 10.1 | 10.1 | 8.1 | 11.9 | |||||
| (a) | |||||
| Water Leakage | Mold Growth | Sig. | |||
| Yes | No | ||||
| Yes | 160 (60.6%) | 104 (39.4%) | 0.000 | ||
| No | 98 (39.2%) | 152 (60.8%) | |||
| (b) | |||||
| Mold Growth | Persistent Cough | Sig. | |||
| No Symptoms | Have a Symptom of Had It | Sickness | |||
| Yes | 166 (77.2%) | 46 (21.3%) | 3 (1.4%) | 0.696 | |
| No | 155 (73.5%) | 49 (23.2%) | 7 (3.3%) | ||
| Gender | Smoking Habits | Persistent Cough | Sig. | ||
|---|---|---|---|---|---|
| No Symptoms | Have a Symptom or Had It | Sickness | |||
| Male | Active | 53 (76.8%) | 16 (23.2%) | 0 (0%) | 0.775 |
| Passive | 10 (71.4%) | 4 (28.6%) | 0 (0%) | 0.437 | |
| None | 22 (81.5%) | 5 (18.5%) | 0 (0%) | - | |
| Female | Active | 23 (76.7%) | 7 (23.3%) | 0 (0%) | 0.703 |
| Passive | 19 (70.4%) | 8 (29.6%) | 0 (0%) | 0.891 | |
| None | 68 (75.6%) | 22 (24.4%) | 0 (0%) | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sani, H.; Kubota, T.; Sumi, J.; Surahman, U. Impacts of Air Pollution and Dampness on Occupant Respiratory Health in Unplanned Houses: A Case Study of Bandung, Indonesia. Atmosphere 2022, 13, 1272. https://doi.org/10.3390/atmos13081272
Sani H, Kubota T, Sumi J, Surahman U. Impacts of Air Pollution and Dampness on Occupant Respiratory Health in Unplanned Houses: A Case Study of Bandung, Indonesia. Atmosphere. 2022; 13(8):1272. https://doi.org/10.3390/atmos13081272
Chicago/Turabian StyleSani, Hanief, Tetsu Kubota, Jumpei Sumi, and Usep Surahman. 2022. "Impacts of Air Pollution and Dampness on Occupant Respiratory Health in Unplanned Houses: A Case Study of Bandung, Indonesia" Atmosphere 13, no. 8: 1272. https://doi.org/10.3390/atmos13081272
APA StyleSani, H., Kubota, T., Sumi, J., & Surahman, U. (2022). Impacts of Air Pollution and Dampness on Occupant Respiratory Health in Unplanned Houses: A Case Study of Bandung, Indonesia. Atmosphere, 13(8), 1272. https://doi.org/10.3390/atmos13081272