An Air Quality Health Index (AQHI) with Different Health Outcomes Based on the Air Pollution Concentrations in Stockholm during the Period of 2015–2017

Abstract
1. Introduction
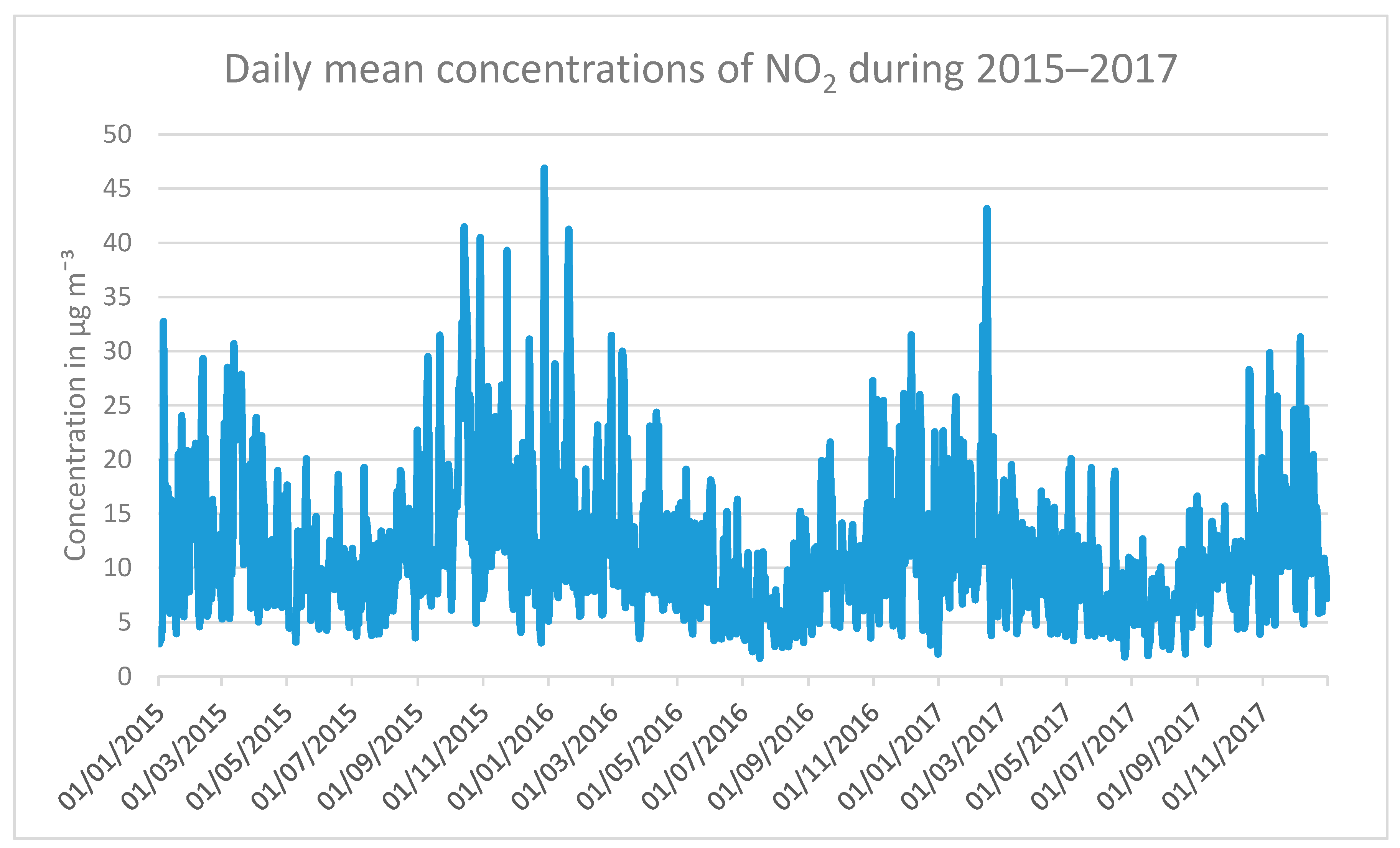
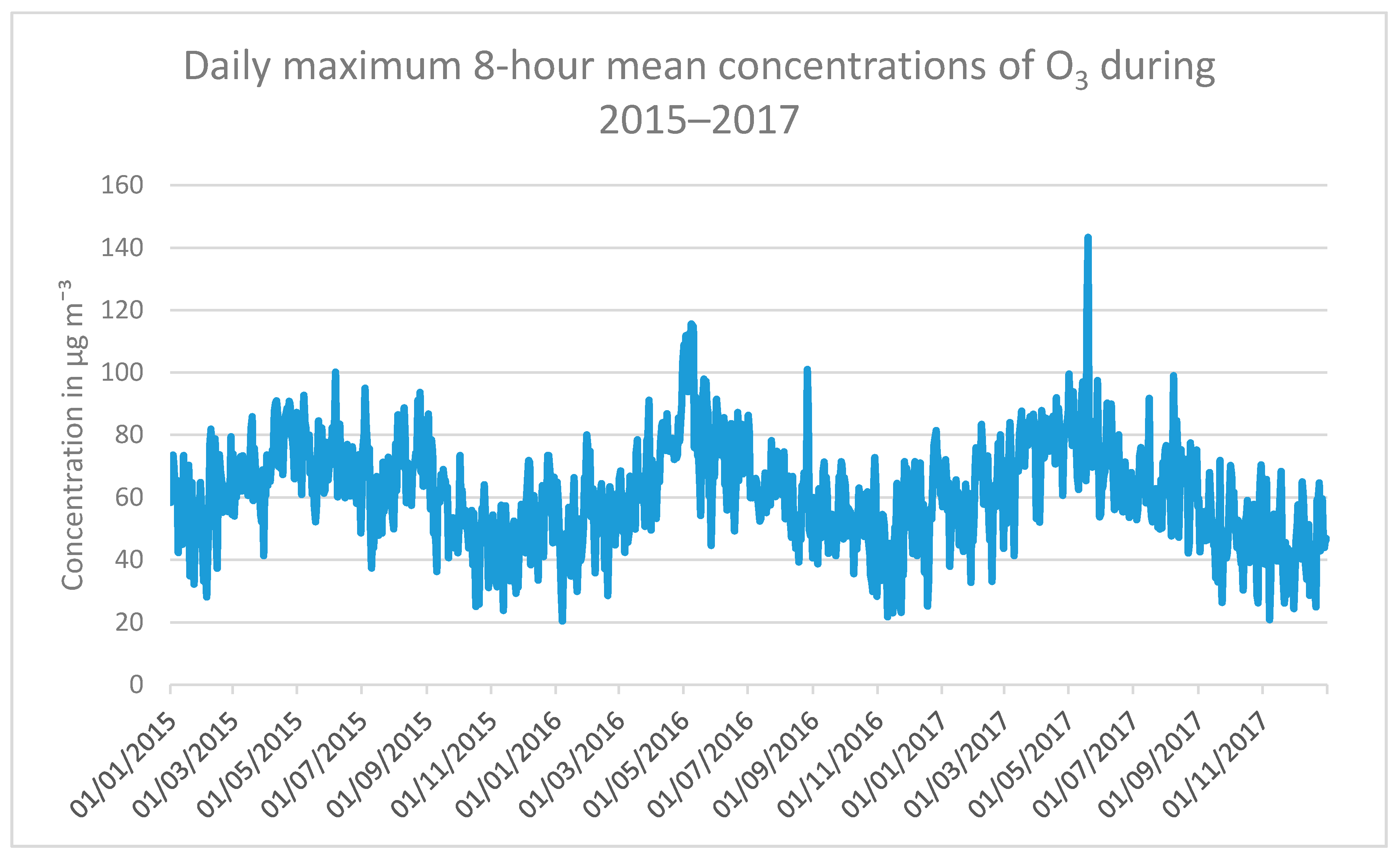
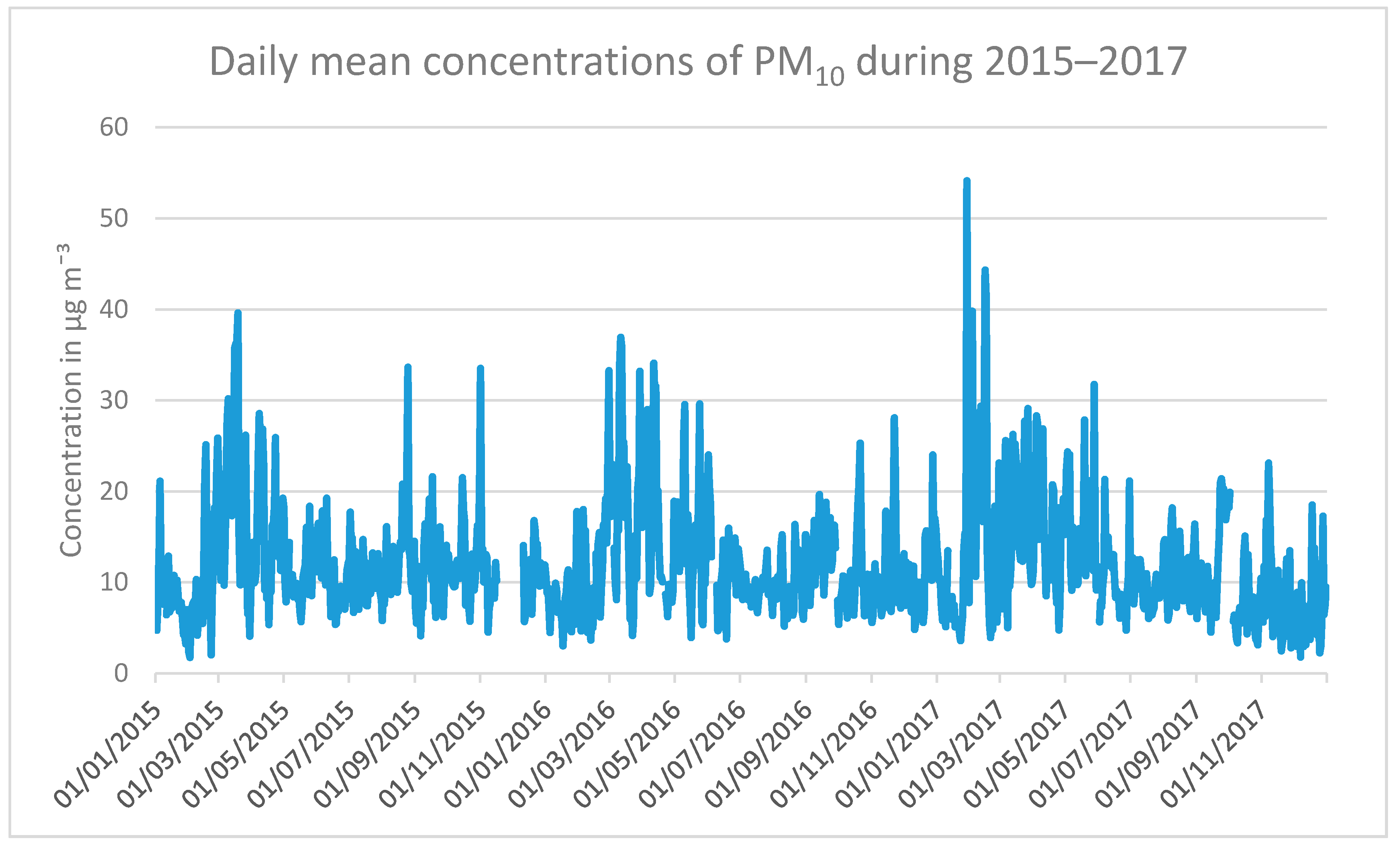
2. Experiments
3. Results
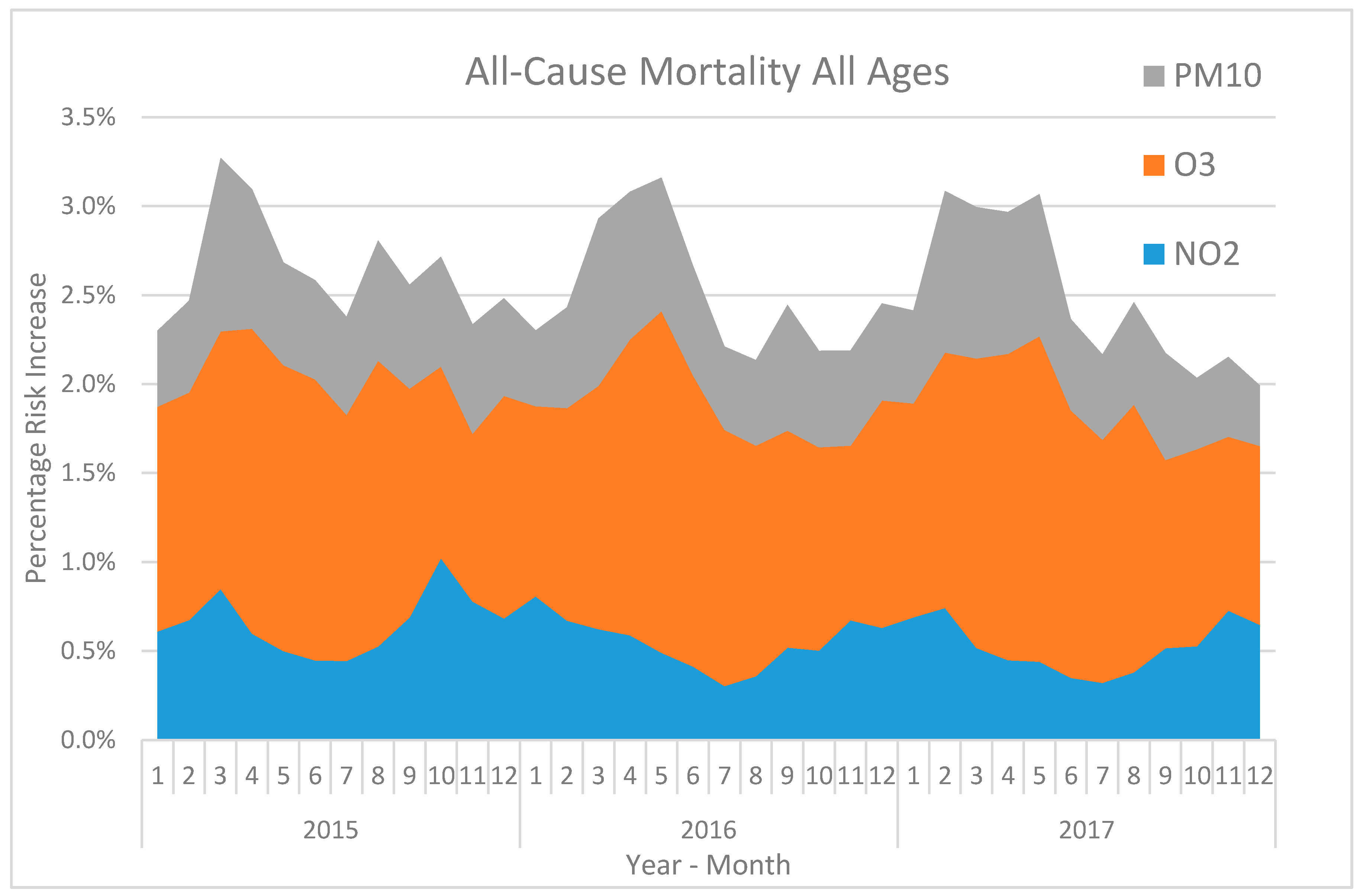
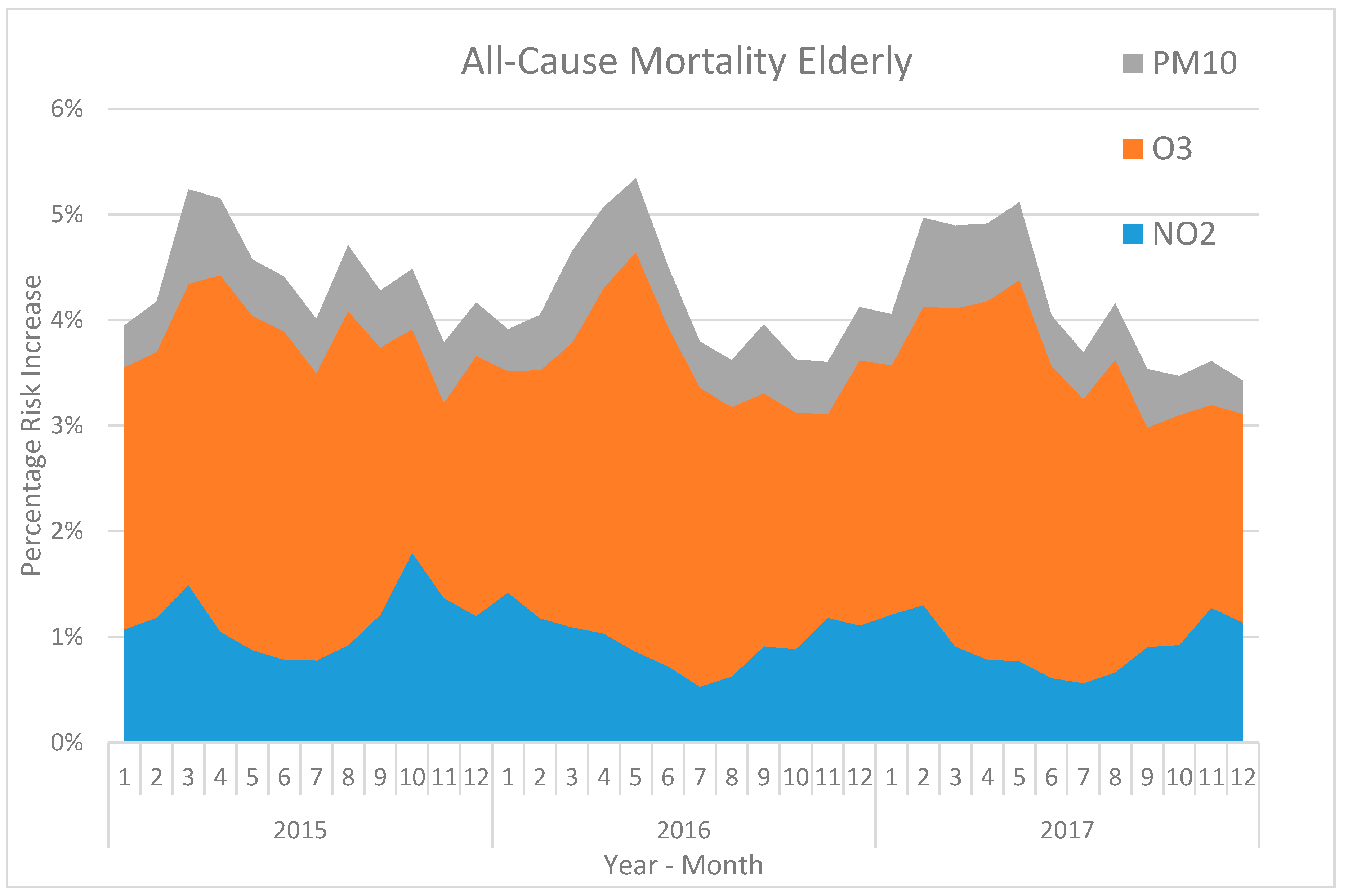
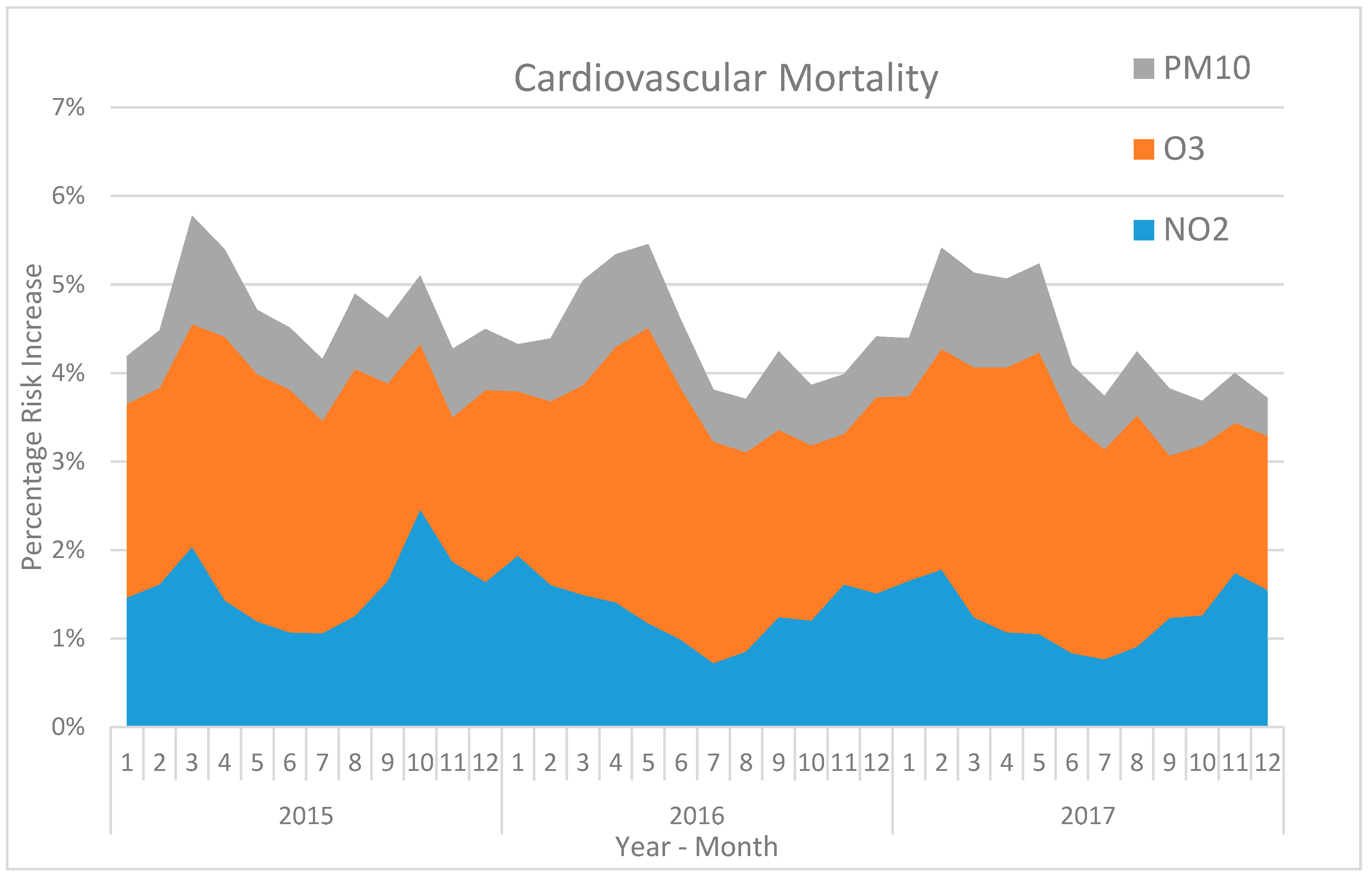
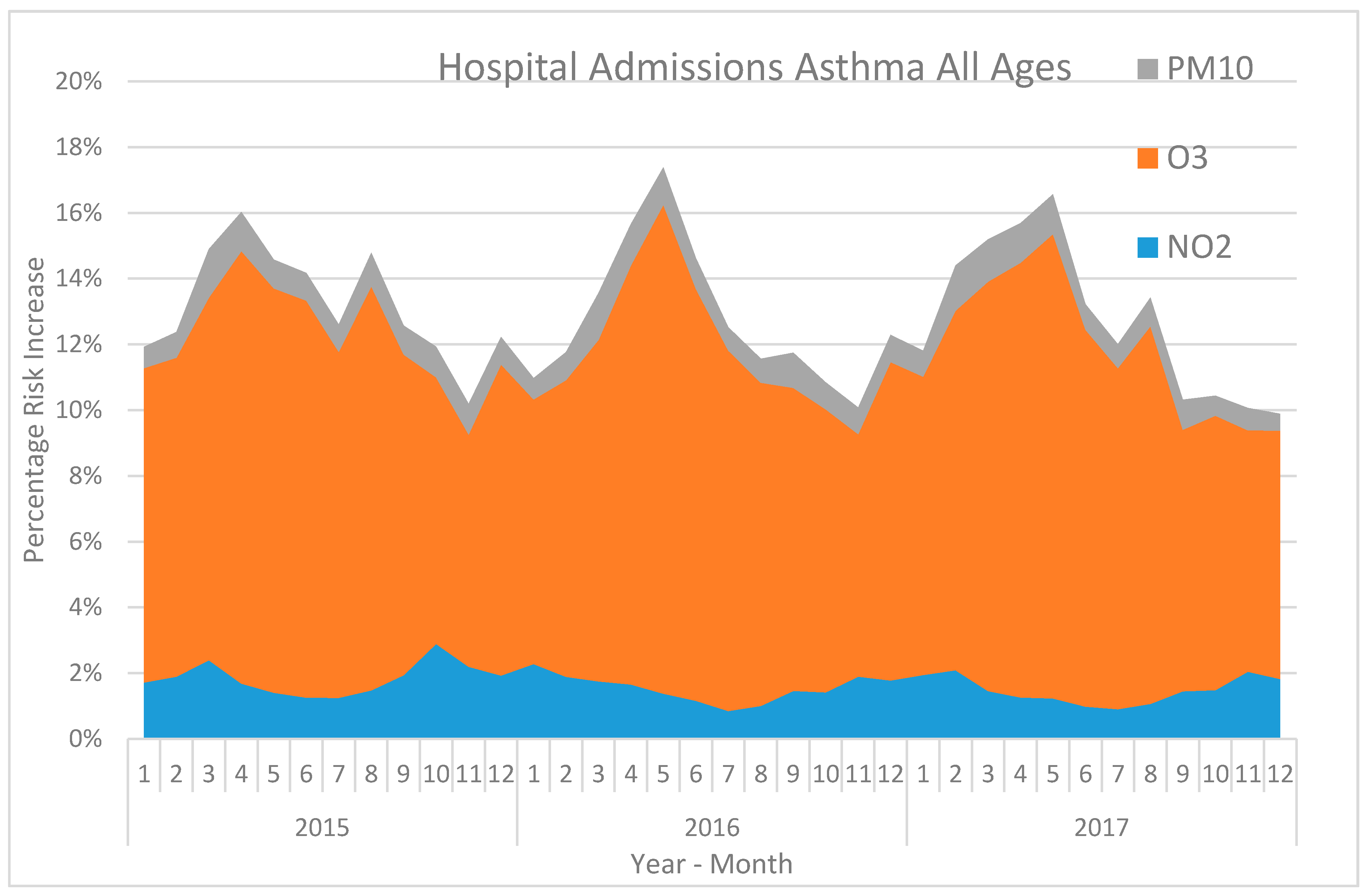
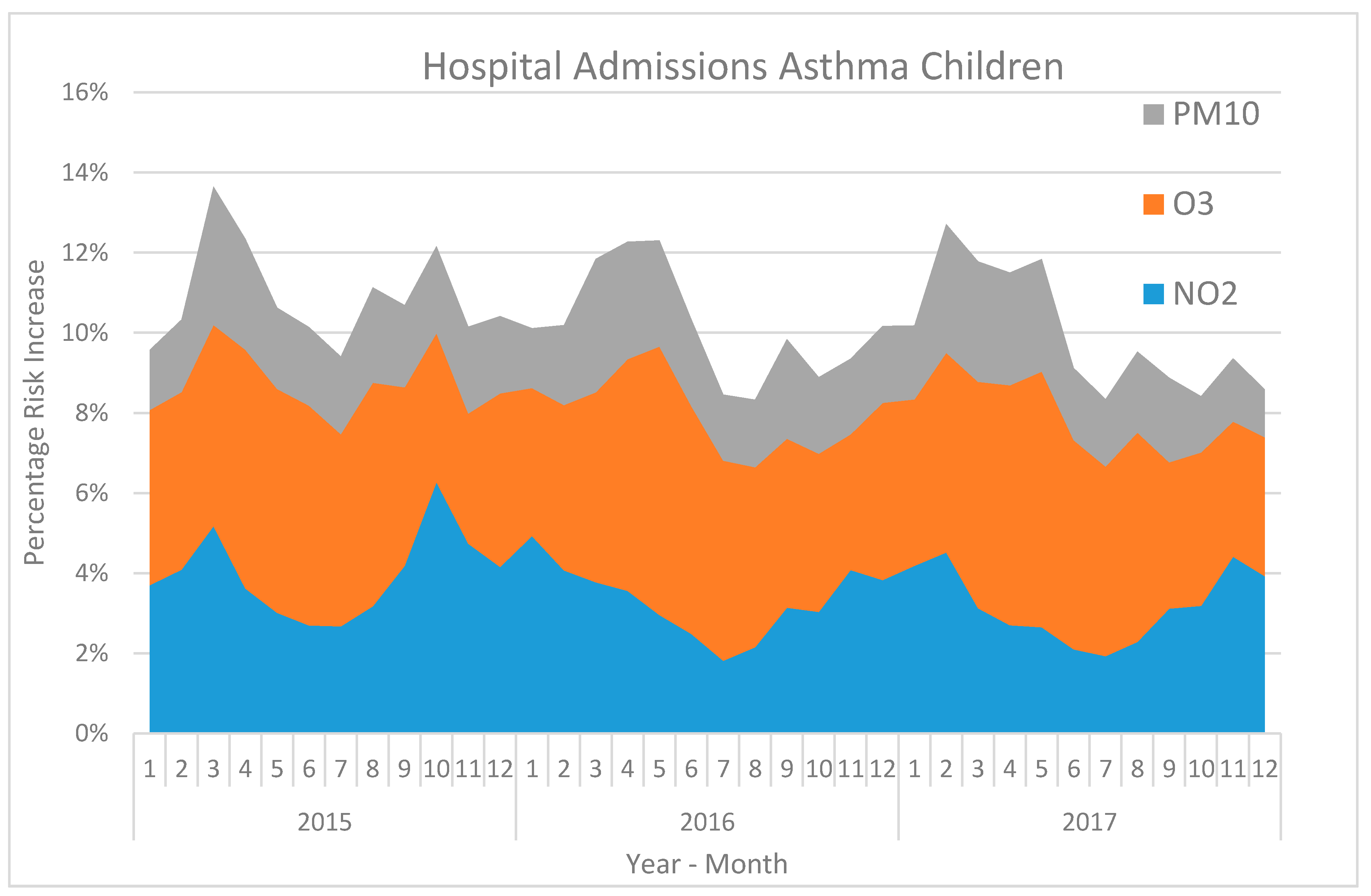
3.1. The Risk Increases for Different Health Outcomes during 2015–2017
3.2. Correlations and Comparisons between Different AQHIs Based on Different Health Outcomes
4. Discussion
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
Appendix A



References
- Stieb, D.M.; Burnett, R.T.; Smith-Doiron, M.; Brion, O.; Shin, H.H.; Economou, V. A new multipollutant, no-threshold air quality health index based on short-term associations observed in daily time-series analyses. J. Air Waste Manag. Assoc. 2008, 58, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xiao, J.; Lin, H.; Liu, T.; Qian, Z.; Zeng, W.; Guo, L.; Ma, W. The construction and validity analysis of AQHI based on mortality risk: A case study in Guangzhou, China. Environ. Pollut. 2017, 220A, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Cairncross, E.K.; John, J.; Zunckel, M. A novel air pollution index based on the relative risk of daily mortality associated with short-term exposure to common air pollutants. Atmos. Environ. 2007, 41, 8442–8454. [Google Scholar] [CrossRef]
- Chen, L.; Villeneuve, P.J.; Rowe, B.H.; Liu, L.; Stieb, D.M. The Air Quality Health Index as a predictor of emergency department visits for ischemic stroke in Edmonton, Canada. J. Expos. Sci. Environ. Epidemiol. 2014, 24, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Szyszkowicz, M.A.; Kousha, T. Emergency department visits for asthma in relation to the Air Quality Health Index: A case-crossover study in Windsor, Canada. Can. J. Public Health 2014, 105, 336–341. [Google Scholar] [CrossRef] [PubMed]
- To, T.; Shen, S.; Atenafu, E.G.; Guan, J.; McLimont, S.; Stocks, B.; Licskai, C. The air quality health index and asthma morbidity: A population-based study. Environ. Health. Perspect. 2013, 121, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Olstrup, H.; Johansson, C.; Forsberg, B.; Tornevi, A.; Ekebom, A.; Meister, K. A Multi-Pollutant Air Quality Health Index (AQHI) Based on Short-Term Respiratory Effects in Stockholm, Sweden. Int. J. Environ. Res. Public Health 2019, 16, 105. [Google Scholar] [CrossRef] [PubMed]
- Anderson, H.R.; Atkinson, R.W.; Bremner, S.A.; Carrinton, J.; Peacock, J. Quantitative Systematic Review of Short Term Associations between Ambient Air Pollution (Particulate Matter, Ozone, Nitrogen Dioxide, Sulphur Dioxide and Carbon Monoxide), and Mortality and Morbidity; Contract number: 0020017; Report to Department of Health revised following first review 2007; Division of Community Health Sciences St George’s, University of London: London, UK, 2007. [Google Scholar]
- Mauderly, J.L.; Samet, J.M. Is There Evidence for Synergy Among Air Pollutants in Causing Health Effects? Environ. Health Perspect. 2009, 117, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Monks, P.S. A review of the observations and origins of the spring ozone maximum. Atmos. Environ. 2000, 34, 3545–3561. [Google Scholar] [CrossRef]
- Johansson, C.A.; Norman, M.; Gidhagen, L. Spatial & temporal variations of PM10 and particle number concentrations in urban air. Environ. Monit. Assess. 2007, 127, 477–487. [Google Scholar] [PubMed]
- Denby, B.R.; Sundvor, I.; Johansson, C.; Pirjola, L.; Ketzel, M.; Norman, M.; Kupiainen, K.; Gustafsson, M.; Blomqvist, G.; Omstedt, G. A coupled road dust surface moisture model to predict non-exhaust road traffic induced particle emissions (NORTRIP). Part 1: Road dust loading and suspension modelling. Atmos. Environ. 2013, 77, 283–300. [Google Scholar] [CrossRef]
- Chen, R.; Wang, X.; Meng, X.; Hua, J.; Zhou, Z.; Chen, B.; Kan, H. Communicating air pollution-related health risks to the public: An application of the Air Quality Health Index in Shanghai, China. Environ. Int. 2013, 51, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Bino, M.; Lefebvre, W.; Walton, H.; Dajnak, D.; Janssen, S.; Williams, M.; Blyth, L.; Beevers, S. Improved Methodologies for NO2 Exposure Assessment in the EU; Contract 070201/2015/SER/717473/C.3; VITO (Belgium), in collaboration with King’s College London (UK); Report no.: 2017/RMA/R/1250; VITO, Belgium, October 2017; University of London: London, UK, 2017. [Google Scholar]
- Daniels, M.J.; Dominici, F.; Samet, J.M.; Zeger, S.L. Estimating particulate matter-mortality dose-response curves and threshold levels: An analysis of daily time-series for the 20 largest US cities. Am. J. Epidemiol. 2000, 152, 397–406. [Google Scholar] [CrossRef]
- Hong, Y.C.; Leem, J.H.; Ha, E.H.; Christiani, D.C. PM10 exposure, gaseous pollutants, and daily mortality in Inchon, South Korea. Environ. Health Perspect. 1999, 107, 873–878. [Google Scholar]
- Chen, K.; Zhou, L.; Chen, X.; Bi, J.; Kinney, P.L. Acute effect of ozone exposure on daily mortality in seven cities of Jiangsu Province, China: No clear evidence for threshold. Environ. Res. 2017, 155, 235–241. [Google Scholar] [CrossRef]
- Le Tertre, A.; Schwartz, J.; Touloumi, G. Empirical Bayes and Adjusted Estimates Approach to Estimating the Relation of Mortality to Exposure of PM10. Risk Anal. 2005, 25, 711–718. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pollutant | Method | Instrument |
|---|---|---|
| NO2 | Chemiluminescence | AC32M, Environment S.A. |
| O3 | UV absorption | O342M, Environment S.A. |
| PM10 | Gravimetric | TEOM 1400A, Thermo Fisher Scientific |
| Health Outcome | NO2 | O3 | PM10 |
|---|---|---|---|
| All-cause mortality, all ages | 0.49 (95% CI: 0.38–0.60) | 0.22 (95% CI: 0.09–0.35) | 0.51 (95% CI: 0.40–0.62) |
| All-cause mortality, elderly | 0.86 (95% CI: 0.50–1.22) | 0.43 (95% CI: 0.18–0.69) | 0.47 (95% CI: 0.35–0.58) |
| Cardiovascular mortality, all ages | 1.17 (95% CI: 0.82–1.53) | 0.38 (95% CI: 0.27–0.49) | 0.64 (95% CI: 0.46–0.81) |
| Hospital admissions (asthma) all ages | 1.37 (95% CI: 0.59–2.15) | 1.60 (95% CI: −0.08–3.30) | 0.77 (95% CI: 0.06–1.48) |
| Hospital admissions (asthma), children | 2.92 (95% CI: 1.15–4.72) | 0.75 (95% CI: −1.72–3.28) | 1.78 (95% CI: 1.01–2.55) |
| Health Outcome | AC mort. AA | AC mort. E | CV mort. AA | HA Asthma AA | HA Asthma C |
|---|---|---|---|---|---|
| AC mort. AA | 1 | 0.98 | 0.98 | 0.85 | 0.96 |
| AC mort. E | 0.98 | 1 | 0.97 | 0.90 | 0.93 |
| CV mort. AA | 0.98 | 0.97 | 1 | 0.77 | 0.99 |
| HA asthma AA | 0.85 | 0.90 | 0.77 | 1 | 0.69 |
| HA asthma C | 0.96 | 0.93 | 0.99 | 0.69 | 1 |
| AQHI Based on Different Health Outcomes from a Meta-Analysis [8] | AQHI Based on Local Risk-Coefficients for AEDV in Stockholm [7] |
|---|---|
| AC mort. AA | 0.95 |
| AC mort. E | 0.87 |
| CV mort. AA | 0.88 |
| HA asthma AA | 0.72 |
| HA asthma C | 0.88 |
| AQHI Based on Different Health Outcomes | Average Daily Percentage Risk Increases During 2015–2017. |
|---|---|
| AC mort. AA | 2.6 |
| AC mort. E | 4.3 |
| CV mort. AA | 4.5 |
| HA asthma AA | 12.9 |
| HA asthma C | 10.4 |
| AEDV AA [7] | 5.8 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olstrup, H. An Air Quality Health Index (AQHI) with Different Health Outcomes Based on the Air Pollution Concentrations in Stockholm during the Period of 2015–2017. Atmosphere 2020, 11, 192. https://doi.org/10.3390/atmos11020192
Olstrup H. An Air Quality Health Index (AQHI) with Different Health Outcomes Based on the Air Pollution Concentrations in Stockholm during the Period of 2015–2017. Atmosphere. 2020; 11(2):192. https://doi.org/10.3390/atmos11020192
Chicago/Turabian StyleOlstrup, Henrik. 2020. "An Air Quality Health Index (AQHI) with Different Health Outcomes Based on the Air Pollution Concentrations in Stockholm during the Period of 2015–2017" Atmosphere 11, no. 2: 192. https://doi.org/10.3390/atmos11020192
APA StyleOlstrup, H. (2020). An Air Quality Health Index (AQHI) with Different Health Outcomes Based on the Air Pollution Concentrations in Stockholm during the Period of 2015–2017. Atmosphere, 11(2), 192. https://doi.org/10.3390/atmos11020192