
An Unclassified Deletion Involving the Proximal Short Arm of Chromosome 10: A New Syndrome?

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Report
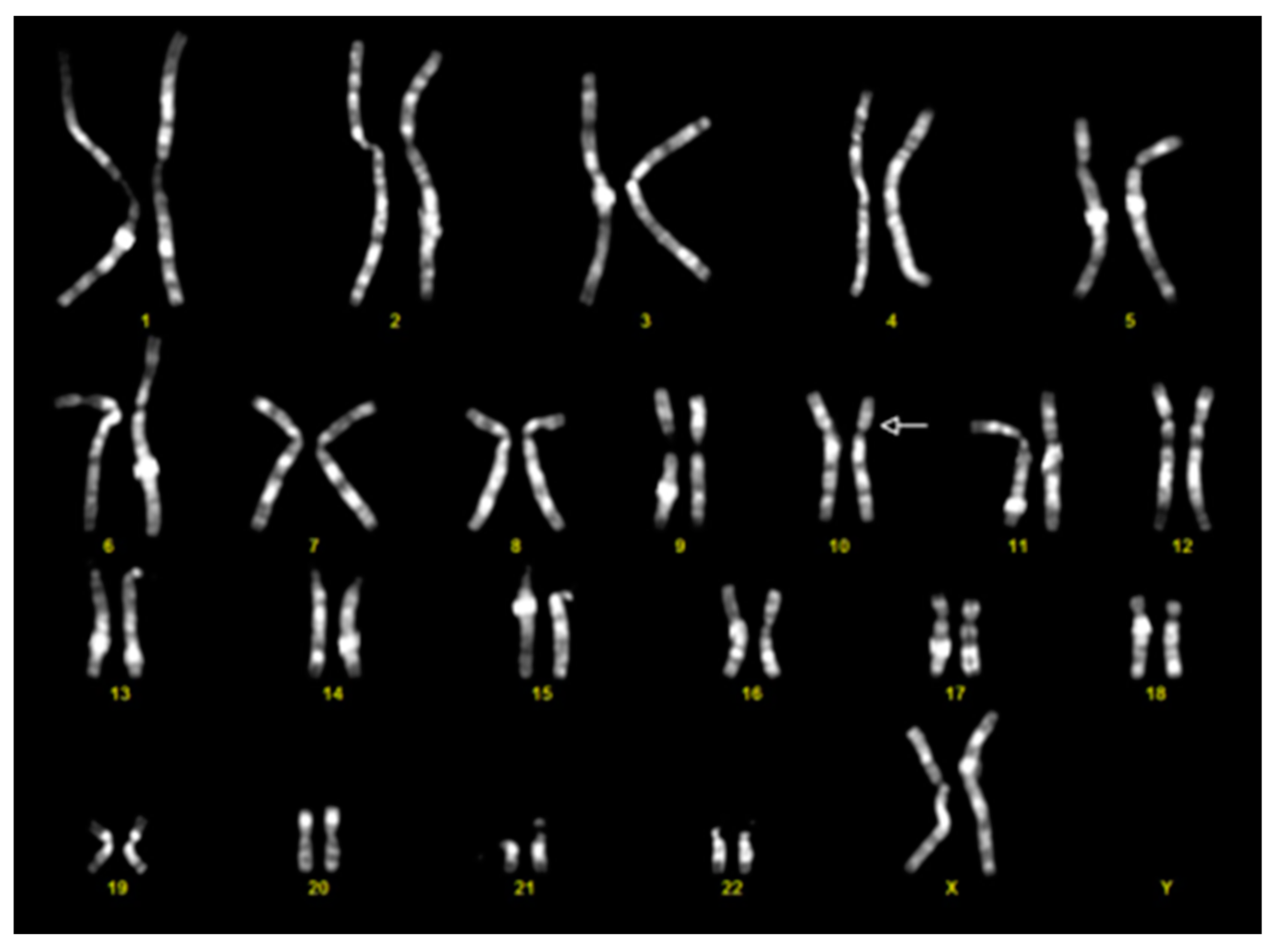
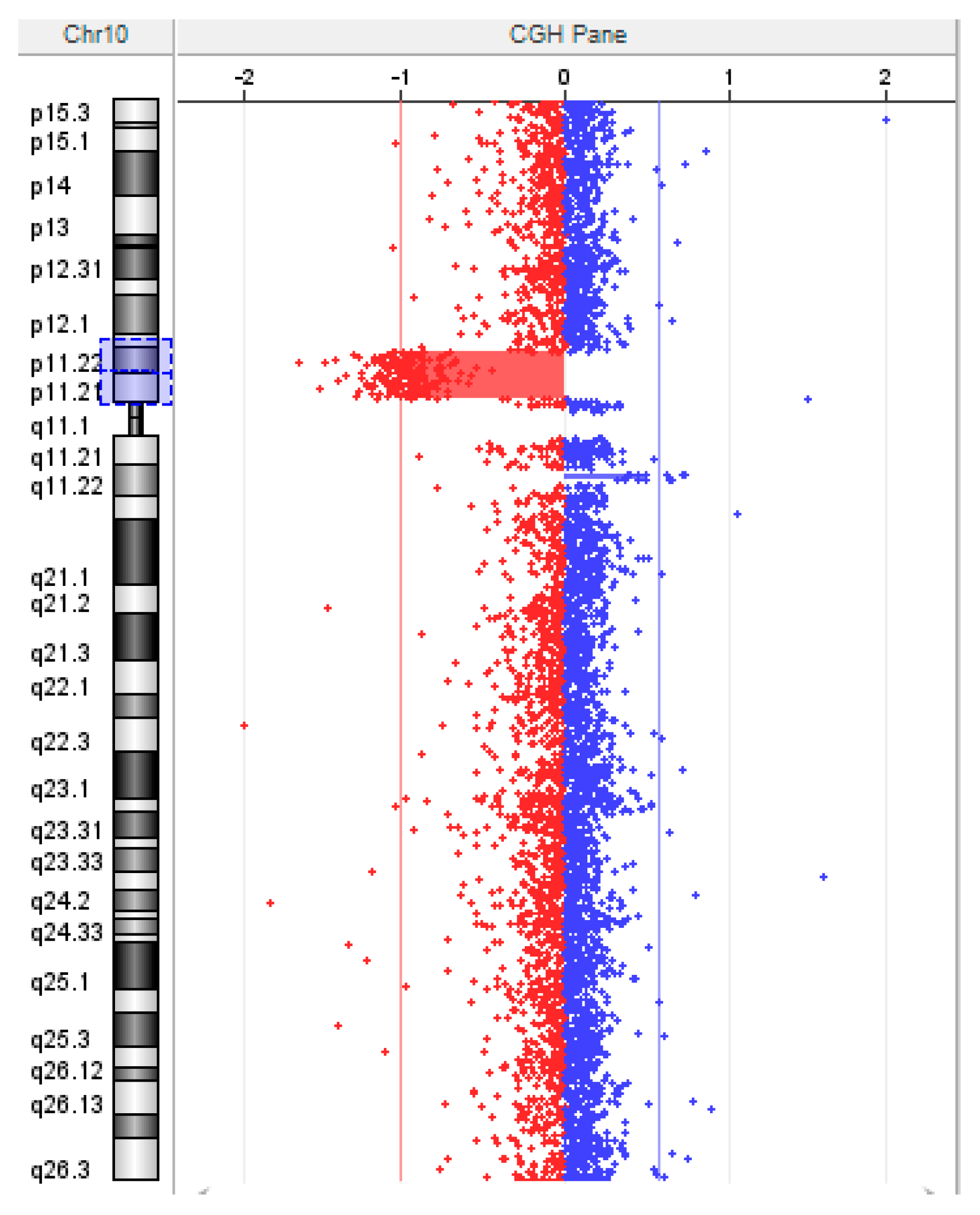
2.2. Cytogenetic Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
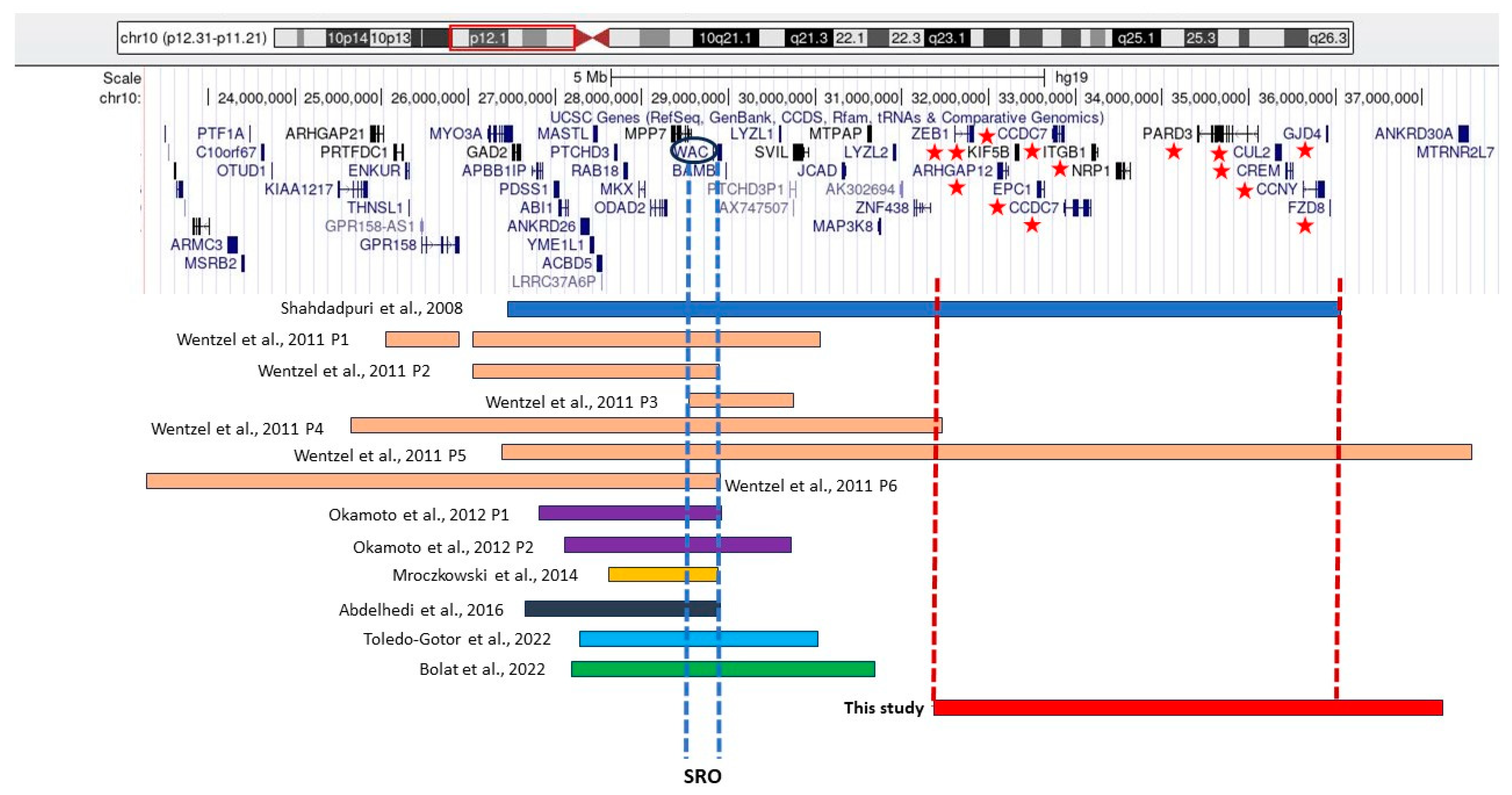
- Shahdadpuri, R.; de Vries, B.; Pfundt, R.; de Leeuw, N.; Reardon, W. Pseudoarthrosis of the clavicle and copper beaten skull associated with chromosome 10p11.21p12.1 microdeletion. Am. J. Med. Genet. A 2008, 146A, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Wentzel, C.; Rajcan-Separovic, E.; Ruivenkamp, C.A.; Chantot-Bastaraud, S.; Metay, C.; Andrieux, J.; Annerén, G.; Gijsbers, A.C.; Druart, L.; Hyon, C.; et al. Genomic and clinical characteristics of six patients with partially overlapping interstitial deletions at 10p12p11. Eur. J. Hum. Genet. 2011, 19, 959–964. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, N.; Hayashi, S.; Masui, A.; Kosaki, R.; Oguri, I.; Hasegawa, T.; Imoto, I.; Makita, Y.; Hata, A.; Moriyama, K.; et al. Deletion at chromosome 10p11.23-p12.1 defines characteristic phenotypes with marked midface retrusion. J. Hum. Genet. 2012, 57, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Mroczkowski, H.J.; Arnold, G.; Schneck, F.X.; Rajkovic, A.; Yatsenko, S.A. Interstitial 10p11.23-p12.1 microdeletions associated with developmental delay, craniofacial abnormalities, and cryptorchidism. Am. J. Med. Genet. A 2014, 164A, 2623–2626. [Google Scholar] [CrossRef] [PubMed]
- Abdelhedi, F.; El Khattabi, L.; Essid, N.; Viot, G.; Letessier, D.; Lebbar, A.; Dupont, J.-M. A de novo 10p11.23-p12.1 deletion recapitulates the phenotype observed in WAC mutations and strengthens the role of WAC in intellectual disability and behavior disorders. Am. J. Med. Genet. A 2016, 170A, 1912–1917. [Google Scholar] [CrossRef] [PubMed]
- Toledo-Gotor, C.; García-Muro, C.; García-Oguiza, A.; Poch-Olivé, M.L.; Ruiz-Del Prado, M.Y.; Domínguez-Garrido, E. Phenotypic comparison of patients affected with DeSanto-Shinawi syndrome: Point mutations in WAC gene versus a 10p12.1 microdeletion including WAC. Mol. Genet. Genom. Med. 2022, 10, e1910. [Google Scholar] [CrossRef] [PubMed]
- Bolat, H.; Derin, H.; Ünsel-Bolat, G. Phenotypic and Brain Imaging Findings Associated With a 10p Proximal Deletion Including the WAC Gene: Case Report and Literature Review. Cogn. Behav. Neurol. 2022, 35, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Berisha, S.Z.; Shetty, S.; Prior, T.W.; Mitchell, A.L. Cytogenetic and molecular diagnostic testing associated with prenatal and postnatal birth defects. Birth Defects Res. 2020, 112, 293–306. [Google Scholar] [CrossRef] [PubMed]
- Alsahlawi, Z.; Jailani, M.; Alaradi, H.; AlAbbad, A. A Case of DeSanto-Shinawi Syndrome in Bahrain with a Novel Mutation. Case Rep. Pediatr. 2020, 2020, 8820966. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Gene | Protein Name | Protein Function | Gene Ontology |
|---|---|---|---|
| ZEB1 (OMIM #189909) | Zinc Finger E-Box-Binding Homeobox | The encoded protein seems to contribute to the transcriptional inhibition of interleukin 2. Pathogenic variants in this gene have been linked to late-onset Fuchs endothelial corneal dystrophy and posterior polymorphous corneal dystrophy-3. | Nucleic acid binding and chromatin binding |
| LOC100505502 | POM121 Transmembrane Nucleoporin-Like Protein | This is a pseudogene. | None |
| ARHGAP1 | Rho-GTPase-Activating Protein 1 | This protein, belonging to a large family, activates enzymes involved in GTP metabolism and may suppress tumour formation by regulating cellular invasion and adhesion. | GTPase activator activity and obsolete SH3/SH2 adaptor activity |
| KIF5B | Kinesin Family Member 5B | This protein participates in various processes, such as lysosome positioning, natural-killer-cell-mediated cytotoxicity, and the promotion of protein localization to the plasma membrane. | ATP hydrolysis activity and microtubule motor activity |
| EPC1 | Enhancer of Polycomb Homolog 1 | This protein works as a transcriptional activator and repressor. It is associated with various processes, like apoptosis, DNA repair, skeletal muscle differentiation, gene silencing, and adult T-cell leukaemia/lymphoma. | Histone acetyltransferase activity |
| LOC102031319 | Uncharacterized | Uncharacterized. | None |
| LOC101929431 | Uncharacterized | Uncharacterized. | None |
| CCDC7 | Coiled-Coil Domain-Containing 7 | This is a coiled-coil domain-containing protein that is specifically expressed in the testis and may play a role in tumorigenesis. | None |
| ITGB1 | Integrin Subunit β 1 | This protein plays an important role in cell adhesion and signalling by serving as a receptor for extracellular matrix proteins. It mediates various cellular processes, such as embryogenesis, haemostasis, tissue repair, immune response, and the metastatic diffusion of tumour cells. | Protein heterodimerization activity and signalling receptor binding |
| SNORA86 | Small Nucleolar RNA and H/ACA Box 86 | The small nucleolar RNAs, like SNORA86, are involved in the post-transcriptional modification of ribosomal RNAs and gene expression regulation. | None |
| IATPR | ITGB1 Adjacent-Tumour-Promoting LncRNA | This is an RNA gene and is affiliated with the lncRNA class. Diseases associated with IATPR include hepatocellular carcinoma. | None |
| NRP1 | Neuropilin 1 | This gene encodes one of two neuropilins involved in diverse signalling pathways regulating cell migration, survival, and attraction through interactions with various ligands, such as vascular endothelial growth factor (VEGF) and semaphorins. | Heparin binding and growth factor binding |
| LINC00838 | Long Intergenic Non-Protein-Coding RNA 838 | This is an RNA gene and is affiliated with the lncRNA class. | None |
| PARD3 | Par-3 Family Cell Polarity Regulator | This gene encodes for a member of the PARD protein family. They affect asymmetrical cell division and direct polarized cell growth. | Protein phosphatase binding and phosphatidylinositol-4,5-bisphosphate binding |
| PARD3-AS1 | PARD3-Divergent Transcript | This is an RNA gene and is affiliated with the lncRNA class. | None |
| CUL2 | Cullin 2 | A part of Cul2-RING ubiquitin ligase complex. It is predicted to be involved in SCF-dependent proteasomal ubiquitin-dependent protein catabolic processes and protein ubiquitination. It is also predicted to act upstream of, or within, the protein catabolic process. | Ubiquitin protein ligase binding and protein-containing complex binding |
| MIR3611 | MicroRNA 3611 | It is an RNA gene and is affiliated with the miRNA class. | None |
| CREM | CAMP-Responsive Element Modulator | This gene codes for a bZIP transcription factor crucial in cAMP-mediated signal transduction during the spermatogenetic cycle and other processes. | DNA-binding transcription factor activity and core promoter sequence-specific DNA binding |
| CCNY | Cyclin Y | This protein is the CDK14/PFTK1 and CDK16 cyclin-dependent kinase’s positive regulatory subunit that functions as a Wnt signalling pathway cell-cycle regulator. | Protein kinase binding and cyclin-dependent protein serine/threonine kinase regulator activity |
| GJD4 | Gap Junction Protein Delta 4 | The encoded protein participates in creating gap junctions, which are intercellular channels that directly link the cytoplasms of contacting cells. | Not known |
| FZD8 | Frizzled Class Receptor 8 | This intronless gene, belonging to the frizzled gene family, encodes a seven-transmembrane domain protein acting as a receptor for wingless-type MMTV integration site family signalling proteins, which are commonly linked to the β-catenin canonical signalling pathway. | G-protein-coupled receptor activity and transmembrane signalling receptor activity |
| MIR4683 | MicroRNA 4683 | This is a non-coding RNA RNA gene involved in vitamin-D-dependent rickets (type 2A). | None |
| PCAT5 | Prostate-Cancer-Associated Transcript 5 | This is a long non-coding RNA. Diseases associated with PCAT5 include prostate cancer and meningeal hemangiopericytoma. | None |
| Shahdapuri et al. (2008), [1] | Wentzel et al. (2011), [2] | Okamoto et al. (2012), [3] | Mroczkowski et al. (2014), [4] | Abdelhedi et al. (2016), [5] | Toledo-Gotor et al. (2022), [6] | Bolat et al. (2022), [7] | This Case | |
|---|---|---|---|---|---|---|---|---|
| N of cases | 1 | 6 | 2 | 1 | 1 | 1 | 1 | 1 |
| Gender | M | 4F;2M | 1F;1M | 1M | M | F | M | F |
| Age at last follow up | 1 year | 3 to 14 years | 6 and 7 years | 6 years | 3 years | 6 years | 9 years | 5 years |
| Genetic | ||||||||
| Chromosomal band | 10p12.1p11.21 | 10p12.1p11.23 (P1, P2, P3) 10p12.1p11.22 (P4) 10p12.1p11.21 (P5) 10p12.31p11.23 (P6) | 10p12.1p11.23 | 10p12.1p11.23 | 10p12.1p11.23 | 10p12.1p11.23 | 10p12.1p11.23 | 10p11.22p11.21 |
| Size (Mb) | 10 | 1–10.7 | 2–2.4 | 0.85 | 1.39 | 2.49 | 2.8 | 5.7 |
| Inheritance | De novo | De novo | 1 De novo; 1 NR | NR | De novo | NR | NR | De novo |
| Dysmorphic facial features | ||||||||
| Downlslanted palpebral fissures | NR | 2/6 | 2/2 | + | + | + | − | − |
| Synophrys | NR | 5/6 | 2/2 | − | + | + | − | − |
| Deep set eyes | + | 4/6 | 2/2 | − | + | + | + | − |
| Epicanthus | + | NR | 2/2 | NR | + | NR | − | + |
| Depressed nasal bridge | NR | 1/6 | 2/2 | NR | + | + | − | + |
| Bulbous nose | + | 4/6 | 1/2 | − | + | + | − | + |
| Other features | ||||||||
| Cardiac abnormalities | + | 5/6 | 1/2 | − | − | NR | − | − |
| Motor delay | + | 6/6 | 2/2 | + | + | + | + | − |
| Learning difficulties | + | 5/6 | 1/2 | + | + | + | + | + |
| Hearing impairments | + | 2/6 | 1/2 | NR | − | − | NR | − |
| Visual impairment | + | 6/6 | NR | + | − | − | + | + |
| Hyperactivity | NR | 4/6 | NR | NR | + | + | + | + |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santoro, G.; Incoronato, M.; Spagnoli, E.; Gabbiato, I.; Contini, S.; Piovan, M.; Ferrari, M.; Lapucci, C.; Zuccarello, D. An Unclassified Deletion Involving the Proximal Short Arm of Chromosome 10: A New Syndrome? Genes 2024, 15, 650. https://doi.org/10.3390/genes15060650
Santoro G, Incoronato M, Spagnoli E, Gabbiato I, Contini S, Piovan M, Ferrari M, Lapucci C, Zuccarello D. An Unclassified Deletion Involving the Proximal Short Arm of Chromosome 10: A New Syndrome? Genes. 2024; 15(6):650. https://doi.org/10.3390/genes15060650
Chicago/Turabian StyleSantoro, Graziano, Mariarosaria Incoronato, Edoardo Spagnoli, Ilaria Gabbiato, Simona Contini, Marta Piovan, Maurizio Ferrari, Cristina Lapucci, and Daniela Zuccarello. 2024. "An Unclassified Deletion Involving the Proximal Short Arm of Chromosome 10: A New Syndrome?" Genes 15, no. 6: 650. https://doi.org/10.3390/genes15060650
APA StyleSantoro, G., Incoronato, M., Spagnoli, E., Gabbiato, I., Contini, S., Piovan, M., Ferrari, M., Lapucci, C., & Zuccarello, D. (2024). An Unclassified Deletion Involving the Proximal Short Arm of Chromosome 10: A New Syndrome? Genes, 15(6), 650. https://doi.org/10.3390/genes15060650