
Clinical Characteristics in the Longitudinal Follow-Up of APECED Syndrome in Southern Croatia—Case Series


Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Assessment and Follow-Up
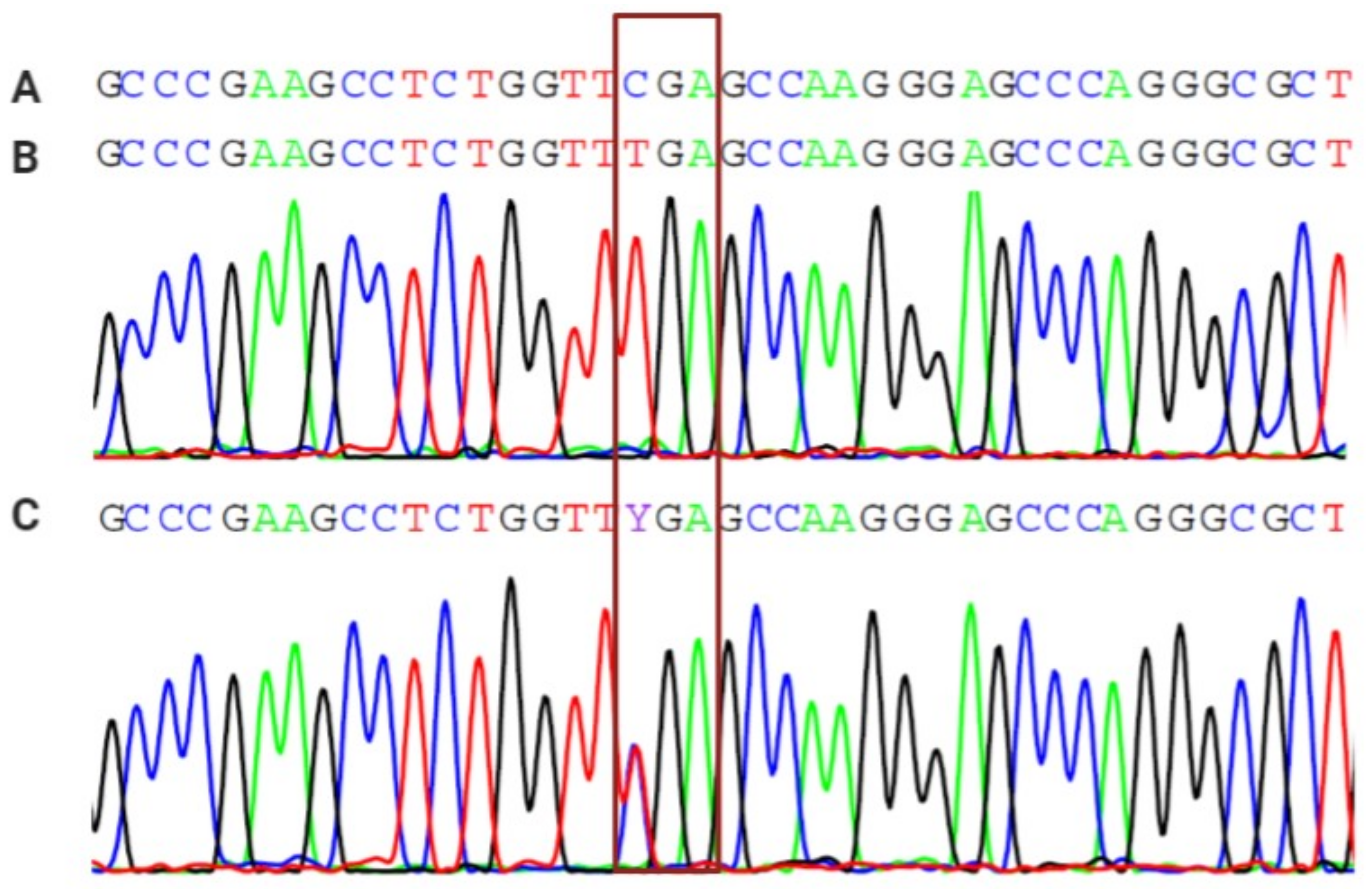
2.2. Genetic Analysis of the AIRE Gene
3. Results
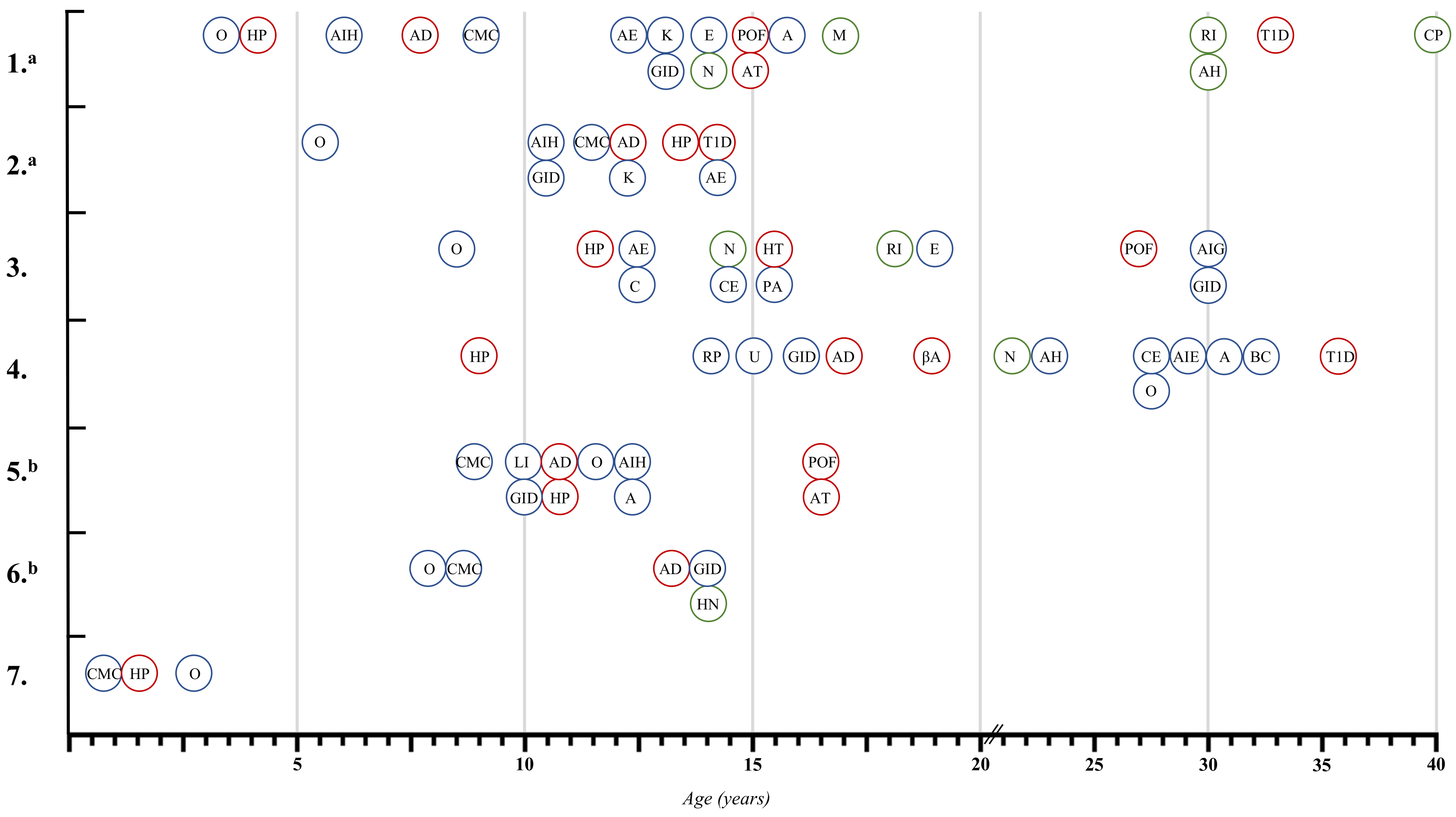
3.1. Initial Clinical Characteristics
3.2. Endocrinological Manifestations
3.3. Non-Endocrinological Manifestations
3.4. Rare Manifestations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahonen, P.; Myllärniemi, S.; Sipilä, I.; Perheentupa, J. Clinical Variation of Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy (APECED) in a Series of 68 Patients. N. Engl. J. Med. 1990, 322, 1829–1936. [Google Scholar] [CrossRef] [PubMed]
- Capalbo, D.; De Martino, L.; Giardino, G.; Di Mase, R.; Di Donato, I.; Parenti, G.; Vajro, P.; Pignata, C.; Salerno, M. Autoimmune Polyendocrinopathy Candidiasis Ectodermal Dystrophy: Insights into Genotype-Phenotype Correlation. Int. J. Endocrinol. 2012, 2012, 353250. [Google Scholar] [CrossRef] [PubMed]
- Perheentupa, J. Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy. J. Clin. Endocrinol. Metab. 2006, 91, 2843–2850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpino, A.; Buganza, R.; Matarazzo, P.; Tuli, G.; Pinon, M.; Calvo, P.L.; Montin, D.; Licciardi, F.; De Sanctis, L. Autoimmune Polyendocrinopathy–Candidiasis–Ectodermal Dystrophy in Two Siblings: Same Mutations but Very Different Phenotypes. Genes 2021, 12, 169. [Google Scholar] [CrossRef] [PubMed]
- Database Human Gene Mutation. Available online: http://www.hgmd.cf.ac.uk/ac/gene.php?gene=AIRE (accessed on 15 December 2021).
- Borchers, J.; Pukkala, E.; Mäkitie, O.; Laakso, S. Patients with APECED Have Increased Early Mortality Due to Endocrine Causes, Malignancies and Infections. J. Clin. Endocrinol. Metab. 2020, 105, dgaa140. [Google Scholar] [CrossRef] [Green Version]
- Kekäläinen, E.; Tuovinen, H.; Joensuu, J.; Gylling, M.; Franssila, R.; Pöntynen, N.; Talvensaari, K.; Perheentupa, J.; Miettinen, A.; Arstila, T.P. A Defect of Regulatory T Cells in Patients with Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy. J. Immunol. 2007, 178, 1208–1215. [Google Scholar] [CrossRef] [Green Version]
- Zlotogora, J.; Shapiro, M.S. Polyglandular Autoimmune Syndrome Type I among Iranian Jews. J. Med. Genet. 1992, 29, 824–826. [Google Scholar] [CrossRef] [Green Version]
- Rosatelli, M.C.; Meloni, A.; Meloni, A.; Devoto, M.; Cao, A.; Scott, H.S.; Peterson, P.; Heino, M.; Krohn, K.J.E.; Nagamine, K.; et al. A Common Mutation in Sardinian Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy Patients. Hum. Genet. 1998, 103, 428–434. [Google Scholar] [CrossRef]
- Podkrajšek, K.T.; Bratanič, N.; Kržišnik, C.; Battelino, T. Autoimmune Regulator-1 Messenger Ribonucleic Acid Analysis in a Novel Intronic Mutation and Two Additional Novel AIRE Gene Mutations in a Cohort of Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy Patients. J. Clin. Endocrinol. Metab. 2005, 90, 4930–4935. [Google Scholar] [CrossRef] [Green Version]
- Dominguez, M.; Crushell, E.; Ilmarinen, T.; McGovern, E.; Collins, S.; Chang, B.; Fleming, P.; Irvine, A.D.; Brosnahan, D.; Ulmanen, I.; et al. Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy (APECED) in the Irish Population. J. Pediatr. Endocrinol. Metab. 2006, 19, 1343–1352. [Google Scholar] [CrossRef]
- Husebye, E.S.; Perheentupa, J.; Rautemaa, R.; Kämpe, O. Clinical Manifestations and Management of Patients with Autoimmune Polyendocrine Syndrome Type I. J. Intern. Med. 2009, 265, 514–529. [Google Scholar] [CrossRef]
- Cervato, S.; Mariniello, B.; Lazzarotto, F.; Morlin, L.; Zanchetta, R.; Radetti, G.; De Luca, F.; Valenzise, M.; Giordano, R.; Rizzo, D.; et al. Evaluation of the Autoimmune Regulator (AIRE) Gene Mutations in a Cohort of Italian Patients with Autoimmune-Polyendocrinopathy-Candidiasis-Ectodermal- Dystrophy (APECED) and in Their Relatives. Clin. Endocrinol. 2009, 70, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Bruserud, Ø.; Oftedal, B.E.; Landegren, N.; Erichsen, M.M.; Bratland, E.; Lima, K.; Jørgensen, A.P.; Myhre, A.G.; Svartberg, J.; Fougner, K.J.; et al. A Longitudinal Follow-up of Autoimmune Polyendocrine Syndrome Type 1. J. Clin. Endocrinol. Metab. 2016, 101, 2975–2983. [Google Scholar] [CrossRef] [PubMed]
- Meloni, A.; Willcox, N.; Meager, A.; Atzeni, M.; Wolff, A.S.B.; Husebye, E.S.; Furcas, M.; Rosatelli, M.C.; Cao, A.; Congia, M. Autoimmune Polyendocrine Syndrome Type 1: An Extensive Longitudinal Study in Sardinian Patients. J. Clin. Endocrinol. Metab. 2012, 97, 1114–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, J.T.; Demarest, B.L.; Bisgrove, B.W.; Su, Y.C.; Smith, M.; Yost, H.J. Poly Peak Parser: Method and Software for Identification of Unknown Indels Using Sanger Sequencing of Polymerase Chain Reaction Products. Dev. Dyn. 2014, 243, 1632–1636. [Google Scholar] [CrossRef] [Green Version]
- Valenzise, M.; Fierabracci, A.; Cappa, M.; Porcelli, P.; Barcellona, R.; De Luca, F.; Barollo, S.; Garelli, S.; Betterle, C. Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy: Report of Seven Additional Sicilian Patients and Overview of the Overall Series from Sicily. Horm. Res. Paediatr. 2014, 82, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Proust-Lemoine, E.; Saugier-Véber, P.; Lefranc, D.; Dubucquoi, S.; Ryndak, A.; Buob, D.; Lalau, J.D.; Desailloud, R.; Weill, J.; Prin, L.; et al. Autoimmune Polyendocrine Syndrome Type 1 in North-Western France: AIRE Gene Mutation Specificities and Severe Forms Needing Immunosuppressive Therapies. Horm. Res. Paediatr. 2010, 74, 275–284. [Google Scholar] [CrossRef]
- Cihakova, D.; Trebusak, K.; Heino, M.; Fadeyev, V.; Tiulpakov, A.; Battelino, T.; Tar, A.; Halsz, Z.; Blmel, P.; Tawfik, S.; et al. Novel AIRE Mutations and P450 Cytochrome Autoantibodies in Central and Eastern European Patients with APECED. Hum. Mutat. 2001, 18, 225–232. [Google Scholar] [CrossRef]
- Myhre, A.G.; Halonen, M.; Eskelin, P.; Ekwall, O.; Hedstrand, H.; Rorsman, F.; Kämpe, O.; Husebye, E.S. Autoimmune Polyendocrine Syndrome Type 1 (APS I) in Norway. Clin. Endocrinol. 2001, 54, 211–217. [Google Scholar] [CrossRef]
- Capalbo, D.; Fusco, A.; Aloj, G.; Improda, N.; Vitiello, L.; Dianzani, U.; Betterle, C.; Salerno, M.; Pignata, C. High Intrafamilial Variability in Autoimmune Polyendocrinopathy- Candidiasis-Ectodermal Dystrophy: A Case Study. J. Endocrinol. Investig. 2012, 35, 77–81. [Google Scholar]
- Meloni, A.; Perniola, R.; Faà, V.; Corvaglia, E.; Cao, A.; Rosatelli, M.C. Delineation of the Molecular Defects in the AIRE Gene in Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy Patients from Southern Italy. J. Clin. Endocrinol. Metab. 2002, 87, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Aaltonen, J.; Björses, P.; Sandkuijl, L.; Perheentupa, J.; Peltonen, L. An Autosomal Locus Causing Autoimmune Disease: Autoimmune Polyglandular Disease Type I Assigned to Chromosome 21. Nat. Genet. 1994, 8, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Stolarski, B.; Pronicka, E.; Korniszewski, L.; Pollak, A.; Kostrzewa, G.; Rowińska, E.; Włodarski, P.; Skórka, A.; Gremida, M.; Krajewski, P.; et al. Molecular Background of Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy Syndrome in a Polish Population: Novel AIRE Mutations and an Estimate of Disease Prevalence. Clin. Genet. 2006, 70, 348–354. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Patient Number | HP | AD | AT | T1D | POF | Laboratory Findings at Diagnosis | Endocrine Complications | Curent Therapy |
|---|---|---|---|---|---|---|---|---|
| I | + | + | + | + | + | ↓Ca, ↓PTH | N, RI, BGC | H, F, C, I, EP |
| II | + | + | + | ↑AST, ↑ALT, ↑GGT | FH | / | ||
| III | + | + | + | ↓Ca, ↓PTH | N, RI, BGC | C, EP | ||
| IV | + | + | + | ↓Ca, ↓PTH | N | H, F, C, I, AE | ||
| V | + | + | + | + | ↓Gluc, ↑ACTH,↓Cort | / | H, F, C, EP, LT4 | |
| VI | + | ↑ACTH,↓Cort | / | H, F | ||||
| VII | + | ↓Ca, ↓PTH | / | C |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skrabic, V.; Skrabic, I.; Skrabic, R.; Roje, B.; Simunovic, M. Clinical Characteristics in the Longitudinal Follow-Up of APECED Syndrome in Southern Croatia—Case Series. Genes 2022, 13, 558. https://doi.org/10.3390/genes13040558
Skrabic V, Skrabic I, Skrabic R, Roje B, Simunovic M. Clinical Characteristics in the Longitudinal Follow-Up of APECED Syndrome in Southern Croatia—Case Series. Genes. 2022; 13(4):558. https://doi.org/10.3390/genes13040558
Chicago/Turabian StyleSkrabic, Veselin, Ivna Skrabic, Roko Skrabic, Blanka Roje, and Marko Simunovic. 2022. "Clinical Characteristics in the Longitudinal Follow-Up of APECED Syndrome in Southern Croatia—Case Series" Genes 13, no. 4: 558. https://doi.org/10.3390/genes13040558
APA StyleSkrabic, V., Skrabic, I., Skrabic, R., Roje, B., & Simunovic, M. (2022). Clinical Characteristics in the Longitudinal Follow-Up of APECED Syndrome in Southern Croatia—Case Series. Genes, 13(4), 558. https://doi.org/10.3390/genes13040558