
Evaluation of Hormonal Factors in Acne Vulgaris and the Course of Acne Vulgaris Treatment with Contraceptive-Based Therapies in Young Adult Women

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Selection Criteria
2.1.1. Study Groups and Treatment Regimens
- -
- Subgroup OC was treated with an oral contraceptive agent,
- -
- Subgroup OC + A was treated with an oral contraceptive agent + cyproterone acetate,
- -
- Subgroup OC + R was treated with an oral contraceptive agent + isotretinoin.
2.1.2. Inclusion Criteria for the Study
- -
- Age 18–31 years;
- -
- Caucasian women;
- -
- A history of normal sexual maturation;
- -
- No history of permanent medication use;
- -
- No significant abnormalities on physical examination;
- -
- The patient consents to participate in the study.
- -
- Disorders of growth and weight gain;
- -
- Endocrine diseases (e.g., thyroid disease, diabetes mellitus, polycystic ovary syndrome (PCOS), congenital adrenal hyperplasia (CAH), premature expiration of ovarian function (POF)), which were diagnosed based on history, gynecological examination, and laboratory tests;
- -
- Performance of competitive sports;
- -
- Long-term use of stimulants;
- -
- Incomplete follow-up period;
- -
- Application of a different acne treatment regimen.
2.2. Instruments
2.3. Statistical Methods
2.4. Ethics
3. Results
3.1. Descriptive Statistics of Variables
3.2. Relationships between Hormonal Factors and Acne Severity before Treatment
3.3. The Significance of Differences between Selected Parameters in Subjects from the Pre- and Post-Treatment Group by the Type of Agents Used
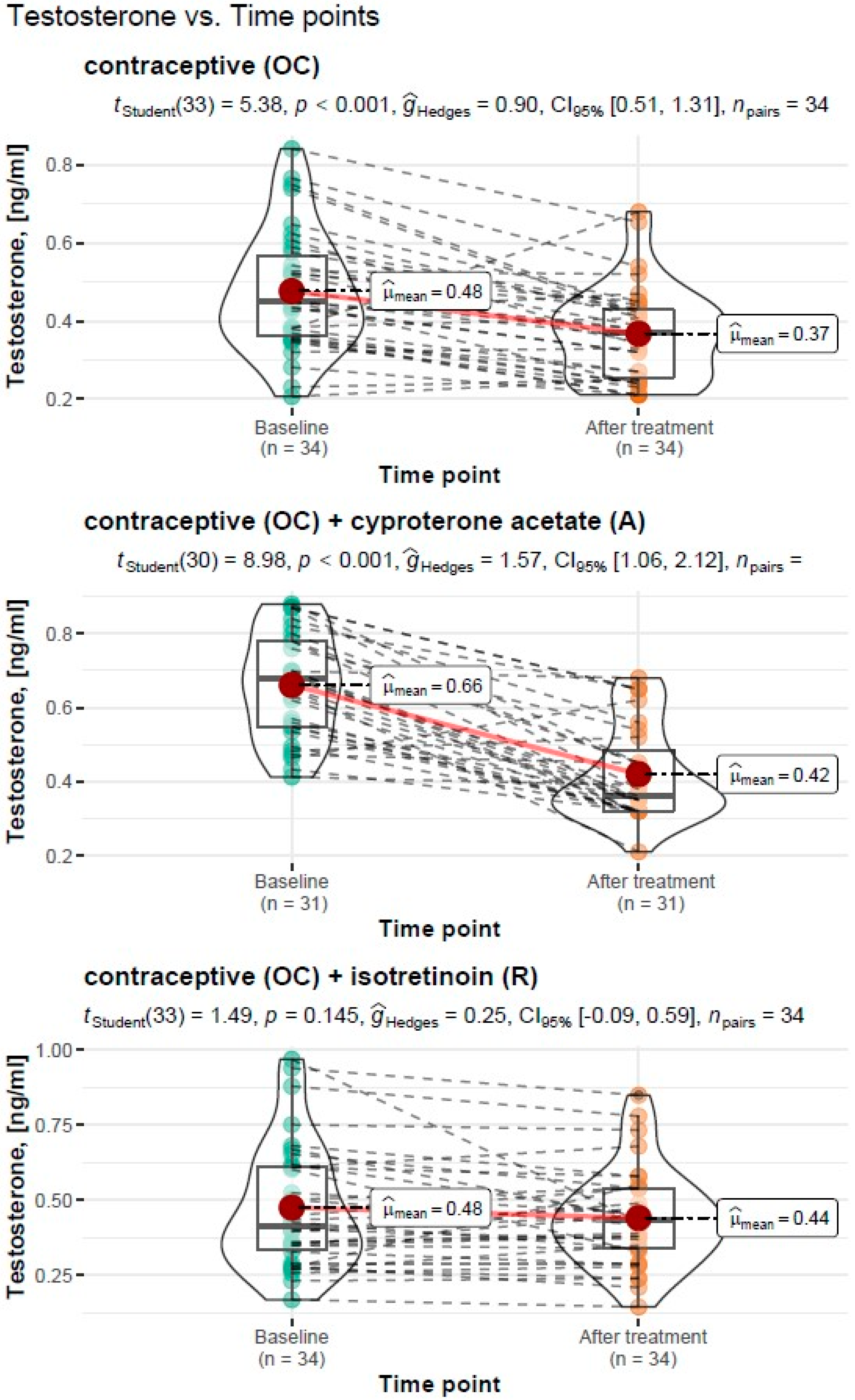
3.3.1. Assessment of Testosterone Levels before and after Treatment
Treatment Type: Oral Contraceptive (OC)
Treatment Type: Oral Contraceptive (OC) + Cyproterone Acetate (A)
Treatment Type: Oral Contraceptive (OC) + Isotretinoin (R)
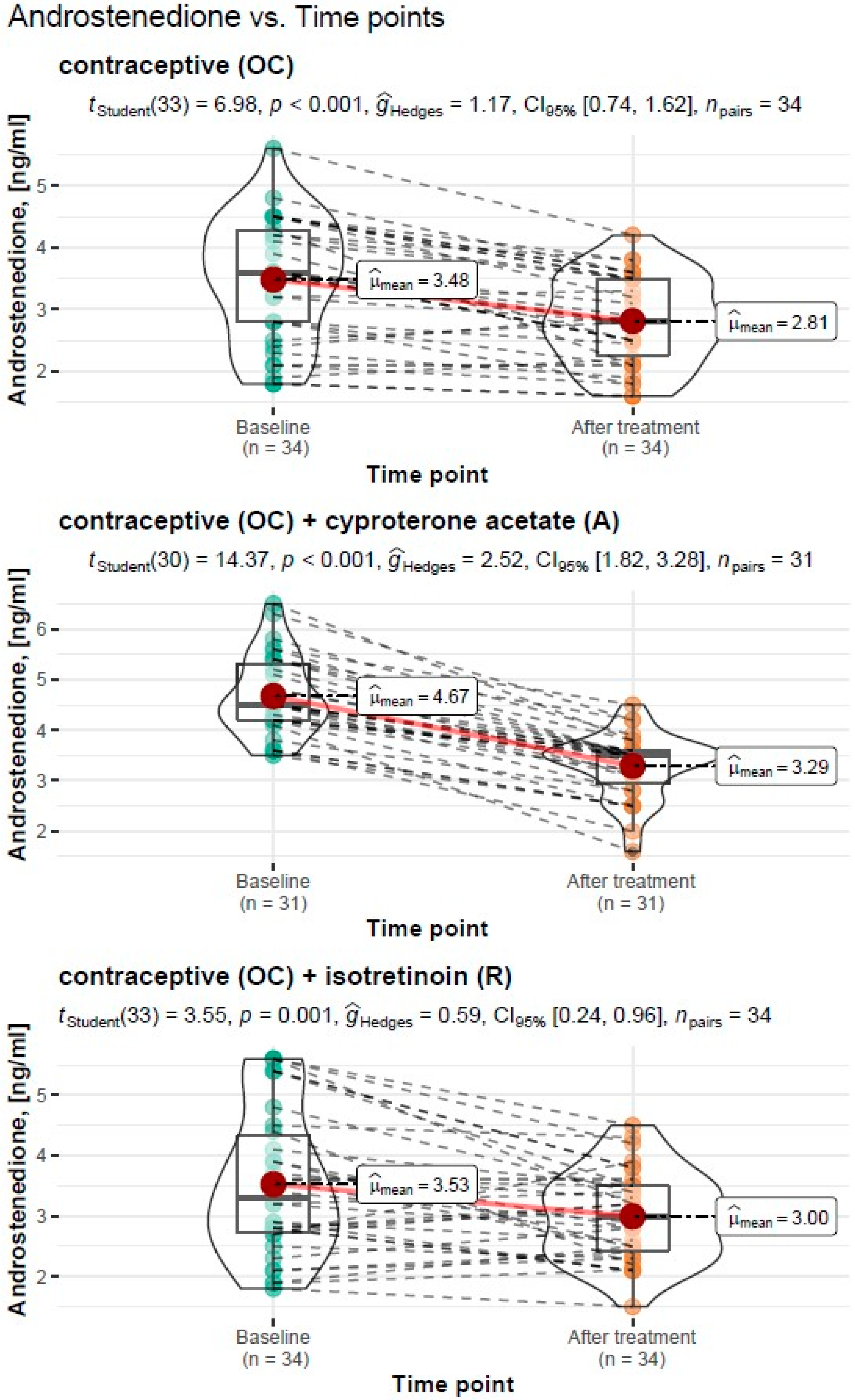
3.3.2. Assessment of Androstendione Levels before and after Treatment
Treatment Type: Oral Contraceptive (OC)
Treatment Type: Oral Contraceptive (OC) + Cyproterone Acetate (A)
Treatment Type: Oral Contraceptive (OC) + Isotretinoin (R)
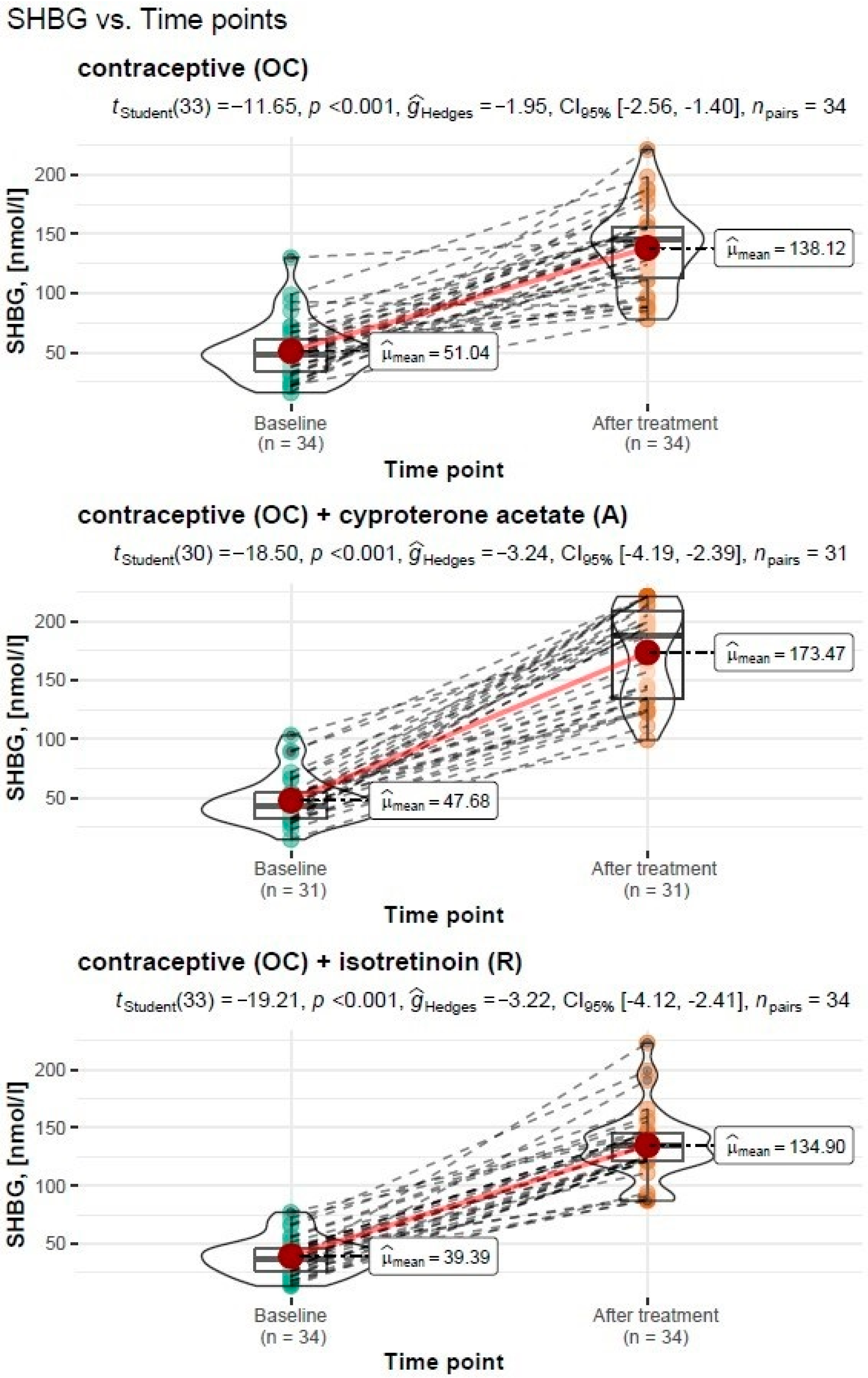
3.3.3. Assessment of SHBG Levels before and after Treatment
Treatment Type: Oral Contraceptive (OC)
Treatment Type: Oral Contraceptive (OC) + Cyproterone Acetate (A)
Treatment Type: Oral Contraceptive (OC) + Isotretinoin (R)
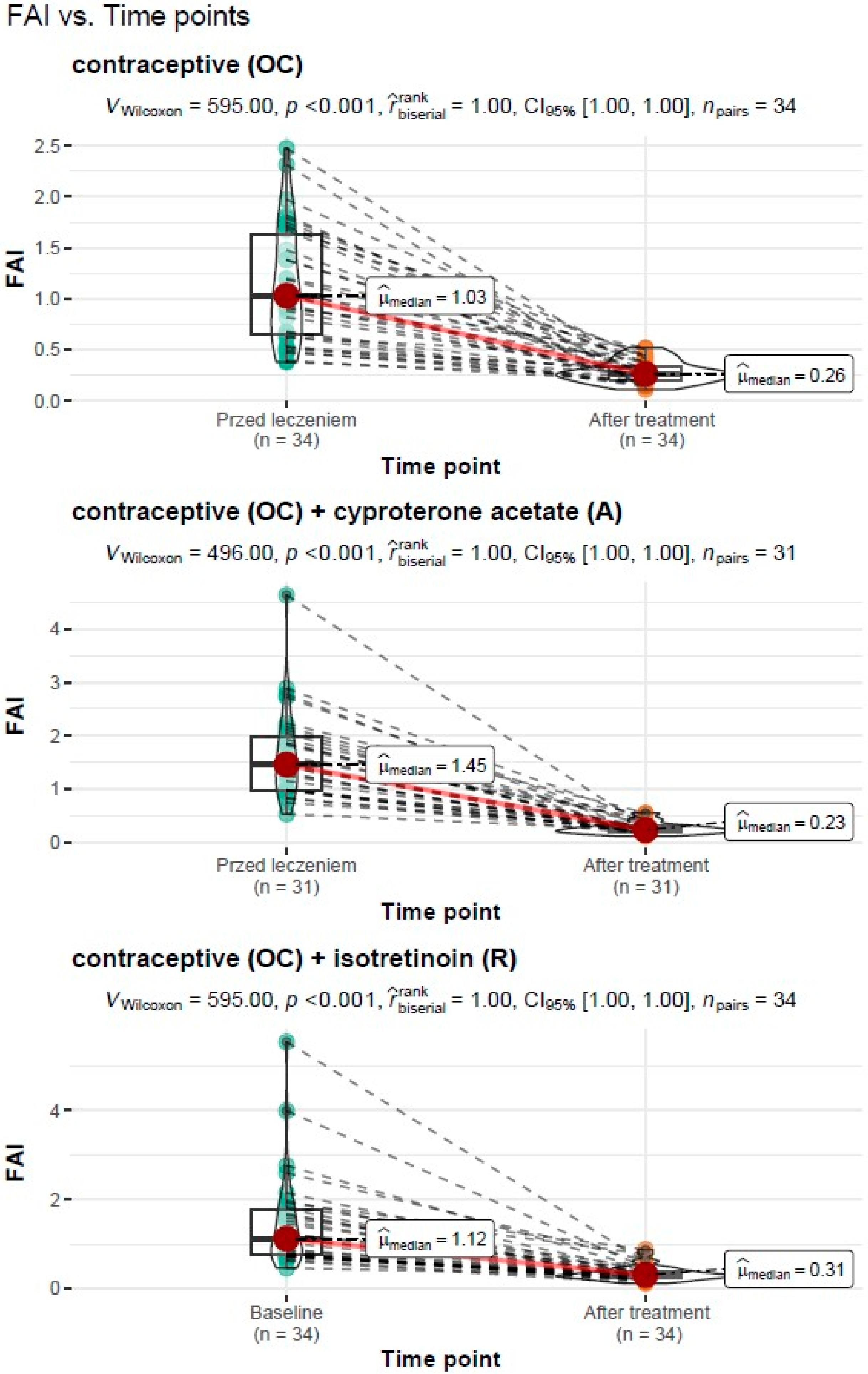
3.3.4. Assessment of FAI before and after Treatment
Treatment Type: Oral Contraceptive (OC)
Treatment Type: Oral Contraceptive (OC) + Cyproterone Acetate (A)
Treatment Type: Oral Contraceptive (OC) + Isotretinoin (R)
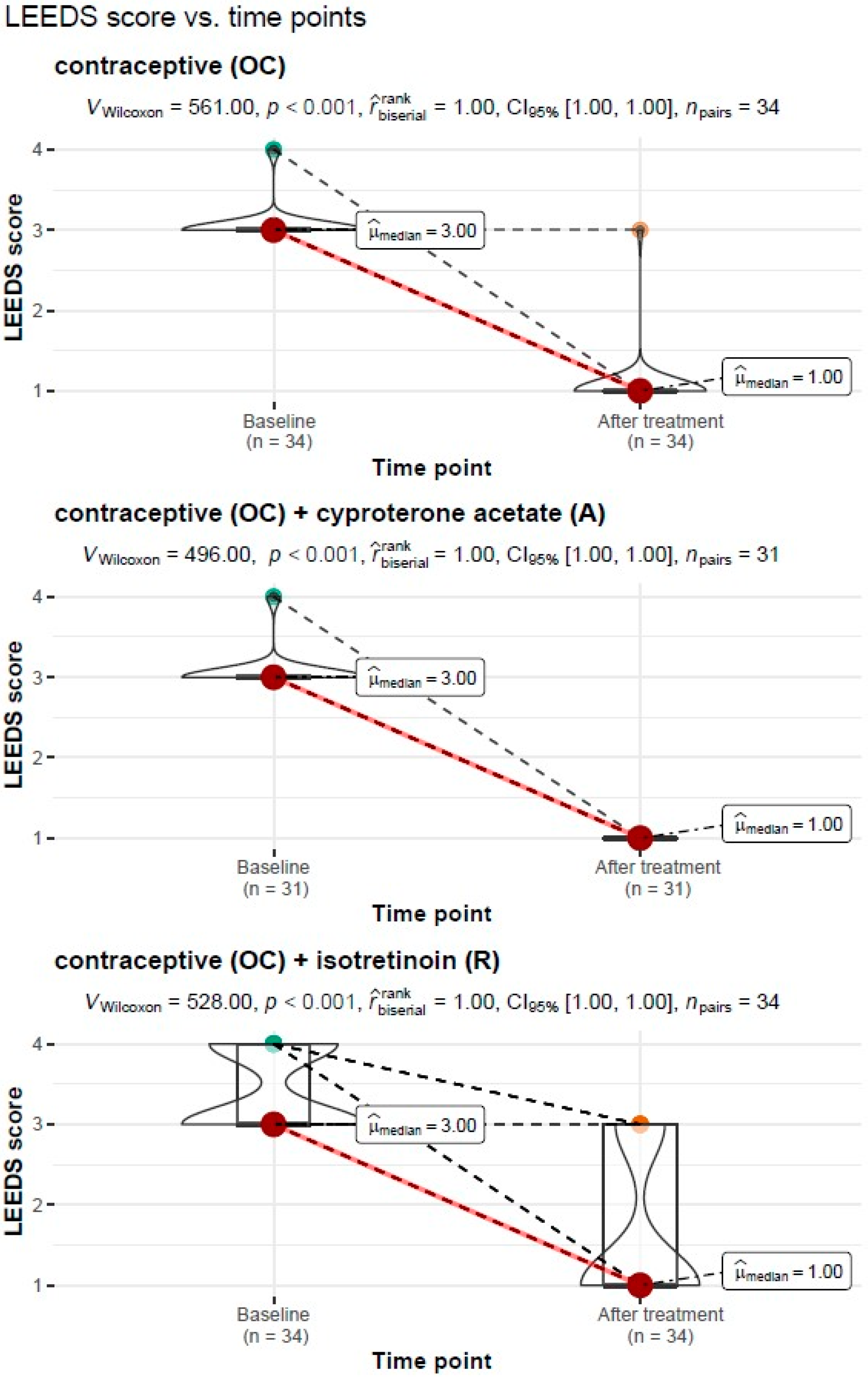
3.3.5. LEEDS Acne Severity Scores before and after Treatment
Treatment Type: Oral Contraceptive (OC)
Treatment Type: Oral Contraceptive (OC) + Cyproterone Acetate (A)
Treatment Type: Oral Contraceptive (OC) + Isotretinoin (R)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, H.; Zhang, T.; Yin, X.; Man, J.; Yang, X.; Lu, M. Magnitude and temporal trend of acne vulgaris burden in 204 countries and territories from 1990 to 2019: An analysis from the Global Burden of Disease Study 2019. Br. J. Dermatol. 2022, 186, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Lynn, D.; Umari, T.; Dellavalle, R.; Dunnick, C. The epidemiology of acne vulgaris in late adolescence. Adolesc. Health Med. Ther. 2016, 7, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Zhang, X.; Jones, E.; Bulger, L. Correlation of photographic images from the Leeds revised acne grading system with a six-category global acne severity scale. J. Eur. Acad. Dermatol. Venereol. 2013, 27, e414–e419. [Google Scholar] [CrossRef] [PubMed]
- Tuchayi, S.M.; Makrantonaki, E.; Ganceviciene, R.; Dessinioti, C.; Feldman, S.R.; Zouboulis, C. Acne vulgaris. Nat. Rev. Dis. Prim. 2015, 1, 15029. [Google Scholar] [CrossRef]
- Rao, A.; Douglas, S.; Hall, J. Endocrine Disrupting Chemicals, Hormone Receptors, and Acne Vulgaris: A Connecting Hypothesis. Cells 2021, 10, 1439. [Google Scholar] [CrossRef] [PubMed]
- Dréno, B. What is new in the pathophysiology of acne, an overview. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 8–12. [Google Scholar] [CrossRef]
- Preneau, S.; Dreno, B. Female acne—A different subtype of teenager acne? J. Eur. Acad. Dermatol. Venereol. 2012, 26, 277–282. [Google Scholar] [CrossRef]
- Dréno, B. Treatment of adult female acne: A new challenge. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 14–19. [Google Scholar] [CrossRef]
- Koo, J.Y.M.; Smith, L.L. Psychologic Aspects of Acne. Pediatr. Dermatol. 1991, 8, 185–188. [Google Scholar] [CrossRef]
- Kantor, J. This month in JAAD International: March 2022: The psychological impact of acne scarring. J. Am. Acad. Dermatol. 2022, 86, 532. [Google Scholar] [CrossRef]
- Heng, A.H.S.; Chew, F.T.; Heng, A.H.S.; Chew, F.T. Systematic review of the epidemiology of acne vulgaris. Sci. Rep. 2020, 10, 5754. [Google Scholar] [CrossRef] [PubMed]
- Kanitakis, J. Anatomy, histology and immunohistochemistry of normal human skin. Eur. J. Dermatol. 2002, 12, 390–399. [Google Scholar]
- Zouboulis, C.C. Human Skin: An Independent Peripheral Endocrine Organ. Horm. Res. Paediatr. 2000, 54, 230–242. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Reyero, N. The clandestine organs of the endocrine system. Gen. Comp. Endocrinol. 2018, 257, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Zouboulis, C.C. The human skin as a hormone target and an endocrine gland. Hormones 2004, 3, 9–26. [Google Scholar] [CrossRef]
- Zouboulis, C.C.; Degitz, K. Androgen action on human skin—From basic research to clinical significance. Exp. Dermatol. 2004, 13, 5–10. [Google Scholar] [CrossRef]
- Pace, S.; Werz, O. Impact of Androgens on Inflammation-Related Lipid Mediator Biosynthesis in Innate Immune Cells. Front. Immunol. 2020, 11, 1356. [Google Scholar] [CrossRef]
- Traish, A.; Bolanos, J.; Nair, S.; Saad, F.; Morgentaler, A. Do Androgens Modulate the Pathophysiological Pathways of Inflammation? Appraising the Contemporary Evidence. J. Clin. Med. 2018, 7, 549. [Google Scholar] [CrossRef]
- Zhang, R.; Zhou, L.; Lv, M.; Yue, N.; Fei, W.; Wang, L.; Liu, Z.; Zhang, J. The Relevant of Sex Hormone Levels and Acne Grades in Patients with Acne Vulgaris: A Cross-Sectional Study in Beijing. Clin. Cosmet. Investig. Dermatol. 2022, 15, 2211–2219. [Google Scholar] [CrossRef]
- Gratton, R.; Del Vecchio, C.; Zupin, L.; Crovella, S. Unraveling the Role of Sex Hormones on Keratinocyte Functions in Human Inflammatory Skin Diseases. Int. J. Mol. Sci. 2022, 23, 3132. [Google Scholar] [CrossRef]
- Thiboutot, D.; Gilliland, K.; Cong, Z.; Jabara, S.; McAllister, J.M.; Sivarajah, A.; Clawson, G. Human Skin is a Steroidogenic Tissue: Steroidogenic Enzymes and Cofactors Are Expressed in Epidermis, Normal Sebocytes, and an Immortalized Sebocyte Cell Line (SEB-1). J. Investig. Dermatol. 2003, 120, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Zawiślak, B.; Marchlewicz, M.; Świder-Al-Amawi, M.; Wenda-Rózewicka, L.; Wiszniewska, B. Skóra i jej udział w syntezie hormonów steroidowych. Postep. Biol. Komórki 2010, 37, 783–793. [Google Scholar]
- Poreba, R.; Debski, R.; Kotarski, J.; Paszkowski, T.; Pertyn, T.; Stachowiak, G. Complex hormonal therapy in women with acne—Recommendations of the polish gynecologic society expert panel-2011. Ginekol. Pol. 2012, 83, 229–232. [Google Scholar]
- Akpolat, D. Unexpected Effects of Oral Isotretinoin in Adolescents With Acne Vulgaris. Cureus 2021, 13, e17115. [Google Scholar] [CrossRef]
- Chilicka, K.; Rogowska, A.M.; Szyguła, R.; Rusztowicz, M.; Nowicka, D. Efficacy of Oxybrasion in the Treatment of Acne Vulgaris: A Preliminary Report. J. Clin. Med. 2022, 11, 3824. [Google Scholar] [CrossRef] [PubMed]
- Chilicka, K.; Rusztowicz, M.; Rogowska, A.M.; Szyguła, R.; Asanova, B.; Nowicka, D. Efficacy of Hydrogen Purification and Cosmetic Acids in the Treatment of Acne Vulgaris: A Preliminary Report. J. Clin. Med. 2022, 11, 6269. [Google Scholar] [CrossRef] [PubMed]
- Burke, B.M.; Cunliffe, W.J. The assessment of acne vulgaris—The Leeds technique. Br. J. Dermatol. 1984, 111, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Slayden, S.M.; Moran, C.; Sams, W.; Boots, L.R.; Azziz, R. Hyperandrogenemia in patients presenting with acne. Fertil. Steril. 2001, 75, 889–892. [Google Scholar] [CrossRef]
- Timpatanapong, P.; Rojanasakul, A. Hormonal Profiles and Prevalence of Polycystic Ovary Syndrome in Women with Acne. J. Dermatol. 1997, 24, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Bunker, C.; Newton, J.A.; Kilborn, J.; Patel, A.; Conway, G.; Jacobs, H.; Greaves, M.; Dowd, P.M. Most women with acne have polycystic ovaries. Br. J. Dermatol. 1989, 121, 675–680. [Google Scholar] [CrossRef]
- Levell, M.; Cawood, M.; Burke, B.; Cunliffe, W. Acne is not associated with abnormal plasma androgens. Br. J. Dermatol. 1989, 120, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Lucky, A.W.; Biro, F.M.; Simbartl, L.A.; Morrison, J.A.; Sorg, N.W. Predictors of severity of acne vulgaris in young adolescent girls: Results of a five-year longitudinal study. J. Pediatr. 1997, 130, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Lucky, A.W.; Cullen, S.I.; Funicella, T.; Jarratt, M.T.; Jones, T.; Reddick, M.E. Double-blind, vehicle-controlled, multicenter comparison of two 0.025% tretinoin creams in patients with acne vulgaris. J. Am. Acad. Dermatol. 1998, 38, S24–S30. [Google Scholar] [CrossRef]
- Harper, J.C. Evaluating hyperandrogenism: A challenge in acne management. J. Drugs Dermatol. 2008, 7, 527–530. [Google Scholar] [PubMed]
- Walton, S.; Cunliffe, W.; Keczkes, K.; Early, A.; McGarrigle, H.; Katz, M.; Reese, R. Clinical, ultrasound and hormonal markers of androgenicity in acne vulgaris. Br. J. Dermatol. 1995, 133, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Cibula, D.; Hill, M.; Vohradnikova, O.; Kuzel, D.; Fanta, M.; Zivny, J. The role of androgens in determining acne severity in adult women. Br. J. Dermatol. 2000, 143, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Cannavò, S.P.; Vaccaro, M.; Guarneri, B.; Borgia, F.; Cannavò, S.; Guarneri, F. Correlation between Endocrinological Parameters and Acne Severity in Adult Women. Acta Derm. Venereol. 2004, 84, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Koulianos, G.; Thorneycroft, I. Abnormal sex hormone-binding globulin. In Decision-Making in Reproductive Endocrinology and Infertility; Schlaff, W.D., Rock, J.A., Eds.; MedicalEconomicsBooks: Oradell, NJ, USA, 1993; pp. 240–245. [Google Scholar]
- Kurnaz-Gomleksiz, O.; Akadam-Teker, B.; Bugra, Z.; Omer, B.; Yilmaz-Aydogan, H. Genetic polymorphisms of the SHBG gene can be the effect on SHBG and HDL-cholesterol levels in Coronary Heart Disease: A case–control study. Mol. Biol. Rep. 2019, 46, 4259–4269. [Google Scholar] [CrossRef]
- Xita, N.; Tsatsoulis, A. Genetic variants of sex hormone-binding globulin and their biological consequences. Mol. Cell. Endocrinol. 2010, 316, 60–65. [Google Scholar] [CrossRef][Green Version]
- Lolis, M.S.; Bowe, W.P.; Shalita, A.R. Acne and Systemic Disease. Med. Clin. N. Am. 2009, 93, 1161–1181. [Google Scholar] [CrossRef]
- Imperato-McGinley, J.; Gautier, T.; Cai, L.Q.; Yee, B.; Epstein, J.; Pochi, P. The androgen control of sebum production. Studies of subjects with dihydrotestosterone deficiency and complete androgen insensitivity. J. Clin. Endocrinol. Metab. 1993, 76, 524–528. [Google Scholar] [CrossRef]
- Tehrani, F.R.; Behboudi-Gandevani, S.; Yarandi, R.B.; Naz, M.S.G.; Carmina, E. Prevalence of acne vulgaris among women with polycystic ovary syndrome: A systemic review and meta-analysis. Gynecol. Endocrinol. 2021, 37, 392–405. [Google Scholar] [CrossRef]
- Carmina, E.; Lobo, R. Hirsutism, alopecia, and acne. In Principles and Practice of Endocrinology and Metabolism; Lip-pincott Williams and Wilkins: Philadelphia, PA, USA, 2001; pp. 991–1008. [Google Scholar]
- Reingold, S.B. The Relationship of Mild Hirsutism or Acne in Women to Androgens. Arch. Dermatol. 1987, 123, 209. [Google Scholar] [CrossRef]
- Carmina, E. Cutaneous manifestations of polycystic ovary syndrome. Curr. Opin. Endocr. Metab. Res. 2020, 12, 49–52. [Google Scholar] [CrossRef]
- Sardana, K.; Bansal, P.; Sharma, L.K.; Garga, U.C.; Vats, G. A study comparing the clinical and hormonal profile of late onset and persistent acne in adult females. Int. J. Dermatol. 2020, 59, 428–433. [Google Scholar] [CrossRef]
- Carmina, E.; Dreno, B.; Lucky, W.A.; Agak, W.G.; Dokras, A.; Kim, J.J.; Lobo, R.A.; Tehrani, F.R.; Dumesic, D. Female Adult Acne and Androgen Excess: A Report From the Multidisciplinary Androgen Excess and PCOS Committee. J. Endocr. Soc. 2022, 6, bvac003. [Google Scholar] [CrossRef]
- Gáspár, E.; Hardenbicker, C.; Bodó, E.; Wenzel, B.; Ramot, Y.; Funk, W.; Kromminga, A.; Paus, R. Thyrotropin releasing hormone (TRH): A new player in human hair-growth control. FASEB J. 2010, 24, 393–403. [Google Scholar] [CrossRef]
- Foitzik, K.; Krause, K.; Conrad, F.; Nakamura, M.; Funk, W.; Paus, R. Human Scalp Hair Follicles Are Both a Target and a Source of Prolactin, which Serves as an Autocrine and/or Paracrine Promoter of Apoptosis-Driven Hair Follicle Regression. Am. J. Pathol. 2006, 168, 748–756. [Google Scholar] [CrossRef]
- Langan, E.A.; Hinde, E.; Paus, R.R. Prolactin as a candidate sebotrop(h)ic hormone? Exp. Dermatol. 2018, 27, 729–736. [Google Scholar] [CrossRef]
- Clayton, R.W.; Langan, E.A.; Ansell, D.; de Vos, I.; Göbel, K.; Schneider, M.R.; Picardo, M.; Lim, X.; Van Steensel, M.A.M.; Paus, R. Neuroendocrinology and neurobiology of sebaceous glands. Biol. Rev. 2020, 95, 592–624. [Google Scholar] [CrossRef]
- Cussen, L.; McDonnell, T.; Bennett, G.; Thompson, C.J.; Sherlock, M.; O’Reilly, M.W. Approach to androgen excess in women: Clinical and biochemical insights. Clin. Endocrinol. 2022, 97, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Sheely, D.; Pujare, D. Endocrinopathies. Med. Clin. N. Am. 2022, 106, 495–507. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Group | n | M | SD | Mdn | IQR | Min | Max | p |
|---|---|---|---|---|---|---|---|---|---|
| Age | Study | 99 | 25.93 | 5.95 | 25.00 | 9.00 | 18.00 | 31.00 | 0.6122 |
| Control | 69 | 23.84 | 1.15 | 24.00 | 1.00 | 21.00 | 28.00 | ||
| Weight | Study | 99 | 67.29 | 14.02 | 63.00 | 12.50 | 54.00 | 89.00 | 0.6688 |
| Control | 69 | 60.46 | 7.06 | 60.00 | 9.00 | 58.00 | 85.00 | ||
| Height | Study | 99 | 163.07 | 13.13 | 164.00 | 8.50 | 158.00 | 173.00 | 0.1949 |
| Control | 69 | 164.58 | 5.45 | 164.00 | 8.00 | 155.00 | 176.00 | ||
| BMI | Study | 99 | 25.00 | 5.00 | 24.00 | 5.05 | 18.69 | 30.72 | 0.5312 |
| Control | 69 | 22.28 | 1.94 | 22.31 | 2.34 | 18.42 | 28.40 |
| Variable | Group | n | M | SD | Mdn | IQR | Min | Max | p |
|---|---|---|---|---|---|---|---|---|---|
| testosterone (T1) | Study | 99 | 0.53 | 0.19 | 0.52 | 0.30 | 0.17 | 0.97 | 0.001 |
| Control | 69 | 0.31 | 0.10 | 0.32 | 0.13 | 0.13 | 0.54 | ||
| testosterone (T2) | Study | 99 | 0.41 | 0.14 | 0.38 | 0.14 | 0.14 | 0.85 | 0.001 |
| androstendione (T1) | Study | 99 | 3.87 | 1.14 | 3.90 | 1.60 | 1.80 | 6.50 | 0.001 |
| Control | 69 | 2.36 | 0.58 | 2.47 | 0.73 | 1.19 | 3.83 | ||
| androstendione (T2) | Study | 99 | 3.03 | 0.71 | 3.10 | 1.00 | 1.50 | 4.50 | 0.026 |
| SHBG (T1) | Study | 99 | 45.99 | 20.97 | 44.80 | 21.92 | 13.55 | 129.90 | 0.001 |
| Control | 69 | 104.79 | 94.83 | 66.90 | 48.70 | 5.00 | 414.00 | ||
| SHBG (T2) | Study | 99 | 148.08 | 38.94 | 145.10 | 55.70 | 78.10 | 223.10 | 0.001 |
| FAI (T1) | Study | 99 | 1.40 | 0.86 | 1.20 | 0.99 | 0.38 | 5.55 | 0.001 |
| Control | 69 | 0.60 | 1.22 | 0.40 | 0.36 | 0.05 | 10.22 | ||
| FAI (T2) | Study | 99 | 0.30 | 0.14 | 0.27 | 0.17 | 0.11 | 0.88 | 0.001 |
| LH (T1) | Study Control | 99 69 | 8.26 9.31 | 3.88 5.22 | 8.50 10.2 | 4.26 5.11 | 1.07 1.02 | 15.10 14.3 | 0.621 |
| FSH (T1) | Study | 99 | 5.63 | 1.81 | 5.47 | 2.51 | 1.64 | 9.95 | 0.820 |
| Control | 69 | 5.61 | 1.84 | 5.82 | 2.53 | 0.30 | 9.69 | ||
| PRL (T1) | Study | 99 | 20.66 | 7.99 | 19.60 | 13.03 | 6.75 | 37.91 | 0.001 |
| Control | 69 | 17.91 | 8.33 | 16.30 | 8.60 | 6.16 | 44.00 | ||
| DHEA-S (T1) | Study | 99 | 258.51 | 81.79 | 254.10 | 119.15 | 45.60 | 413.00 | 0.348 |
| Control | 69 | 239.70 | 98.19 | 211.00 | 151.00 | 58.40 | 487.00 | ||
| ACTH (T1) | Study | 99 | 16.57 | 11.95 | 15.20 | 13.35 | 4.27 | 89.20 | 0.001 |
| Control | 69 | 21.21 | 11.52 | 18.70 | 12.90 | 1.66 | 67.90 | ||
| cortisol (T1) | Study | 99 | 22.25 | 9.61 | 21.00 | 11.90 | 8.02 | 49.10 | 0.001 |
| Control | 69 | 15.79 | 7.51 | 14.30 | 9.30 | 5.63 | 39.50 |
| Variables | LEEDS Scale | |
|---|---|---|
| Correlations (τb, φc) | p | |
| testosterone | 0.14 | 0.013 |
| androstendione | 0.15 | 0.014 |
| SHBG | 0.07 | 0.369 |
| FAI | 0.05 | 0.531 |
| LH | 0.10 | 0.243 |
| FSH | 0.01 | 0.996 |
| PRL | 0.01 | 0.874 |
| DHEA-S | 0.01 | 0.870 |
| ACTH | 0.18 | 0.051 |
| cortisol | 0.20 | 0.017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borzyszkowska, D.; Niedzielska, M.; Kozłowski, M.; Brodowska, A.; Przepiera, A.; Malczyk-Matysiak, K.; Cymbaluk-Płoska, A.; Sowińska-Przepiera, E. Evaluation of Hormonal Factors in Acne Vulgaris and the Course of Acne Vulgaris Treatment with Contraceptive-Based Therapies in Young Adult Women. Cells 2022, 11, 4078. https://doi.org/10.3390/cells11244078
Borzyszkowska D, Niedzielska M, Kozłowski M, Brodowska A, Przepiera A, Malczyk-Matysiak K, Cymbaluk-Płoska A, Sowińska-Przepiera E. Evaluation of Hormonal Factors in Acne Vulgaris and the Course of Acne Vulgaris Treatment with Contraceptive-Based Therapies in Young Adult Women. Cells. 2022; 11(24):4078. https://doi.org/10.3390/cells11244078
Chicago/Turabian StyleBorzyszkowska, Dominika, Mirela Niedzielska, Mateusz Kozłowski, Agnieszka Brodowska, Adam Przepiera, Kinga Malczyk-Matysiak, Aneta Cymbaluk-Płoska, and Elżbieta Sowińska-Przepiera. 2022. "Evaluation of Hormonal Factors in Acne Vulgaris and the Course of Acne Vulgaris Treatment with Contraceptive-Based Therapies in Young Adult Women" Cells 11, no. 24: 4078. https://doi.org/10.3390/cells11244078
APA StyleBorzyszkowska, D., Niedzielska, M., Kozłowski, M., Brodowska, A., Przepiera, A., Malczyk-Matysiak, K., Cymbaluk-Płoska, A., & Sowińska-Przepiera, E. (2022). Evaluation of Hormonal Factors in Acne Vulgaris and the Course of Acne Vulgaris Treatment with Contraceptive-Based Therapies in Young Adult Women. Cells, 11(24), 4078. https://doi.org/10.3390/cells11244078