

Technologies Supporting Screening Oculomotor Problems: Challenges for Virtual Reality


Abstract
1. Introduction
2. Literature Background
3. The C&Look Application
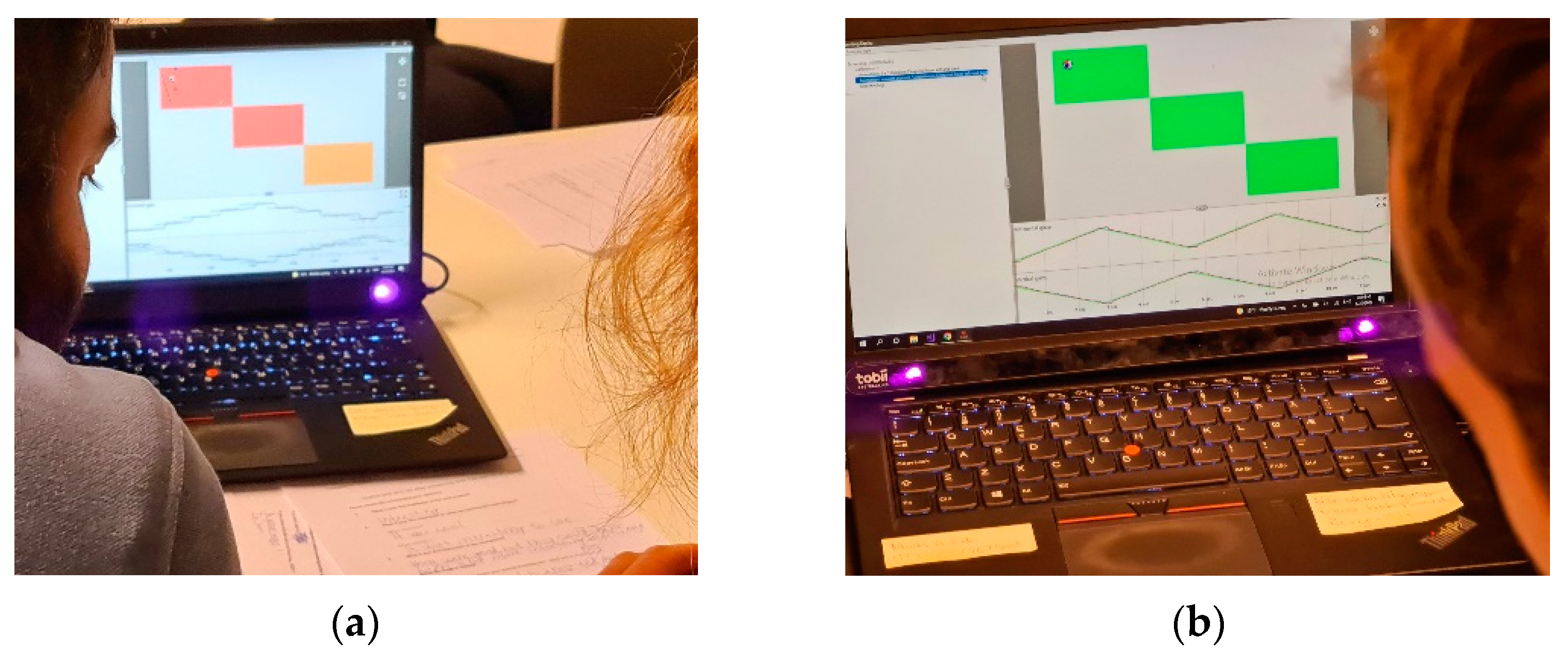
3.1. Developing a Laptop-Based Application
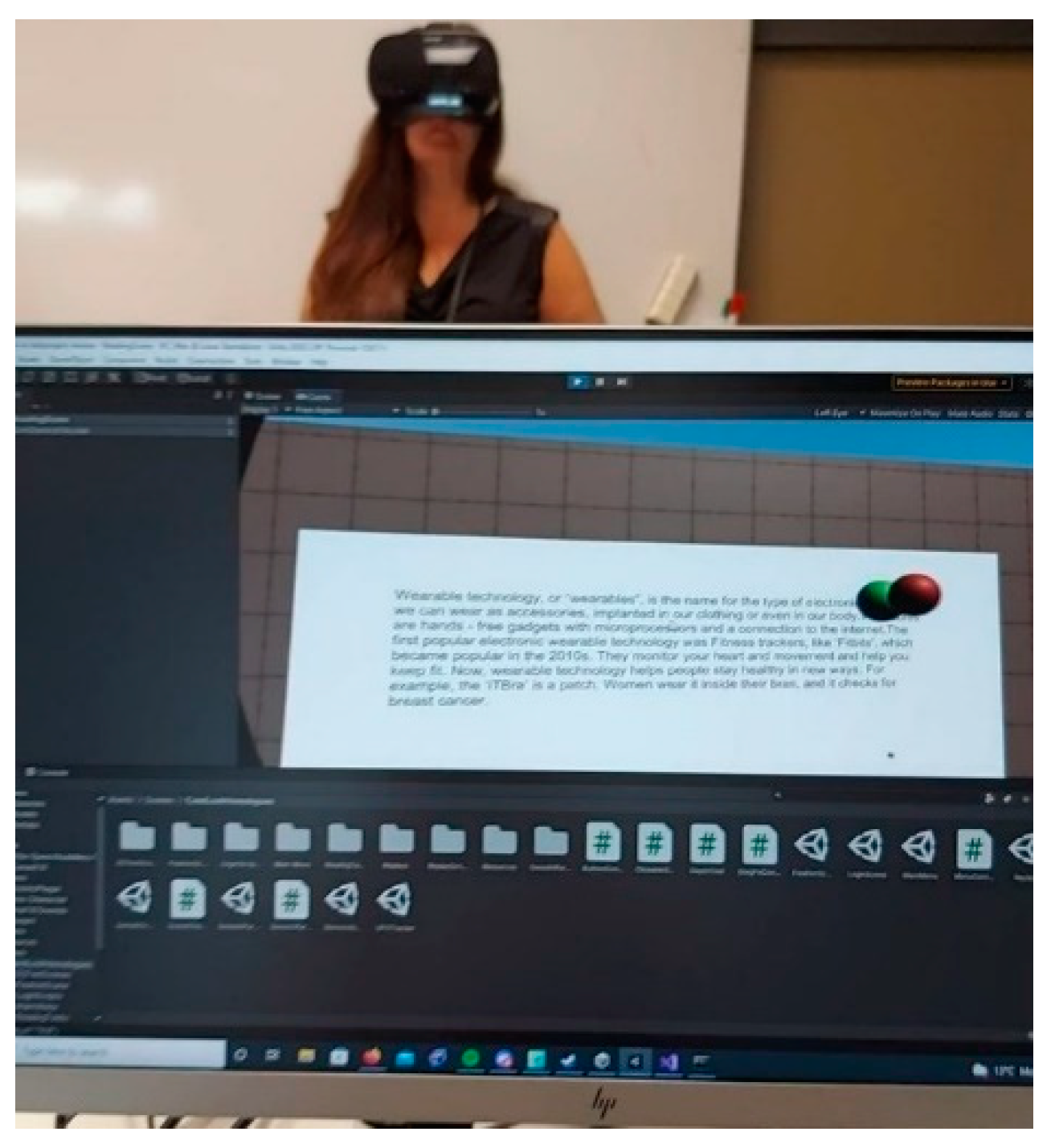
3.2. Development of a VR Application
4. Study Design
- Information about this study (written and oral information).
- Consent for participation.
- Background information about the participant’s familiarity with vision control and their familiarity with new technologies (ET, VR, and serious games).
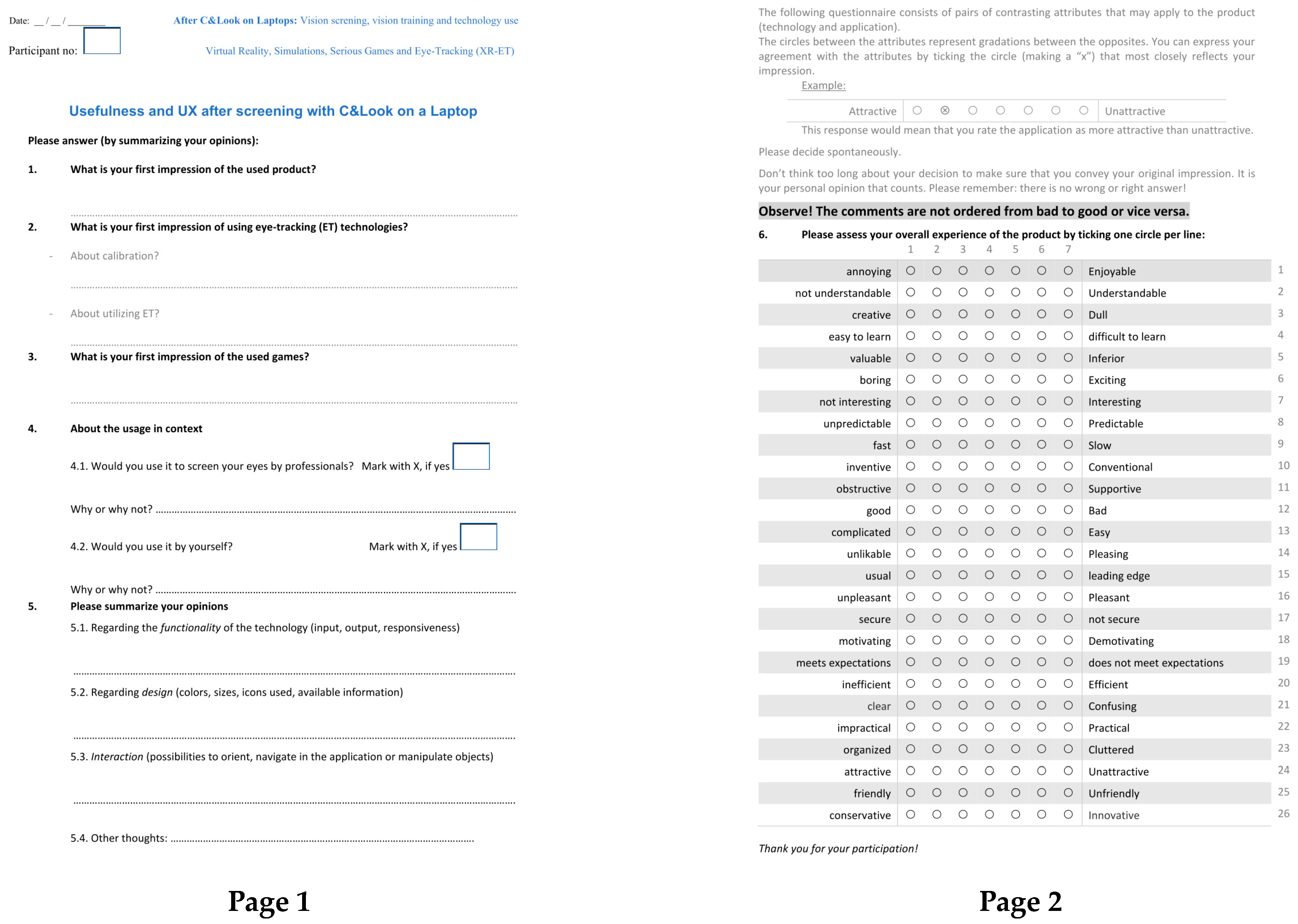
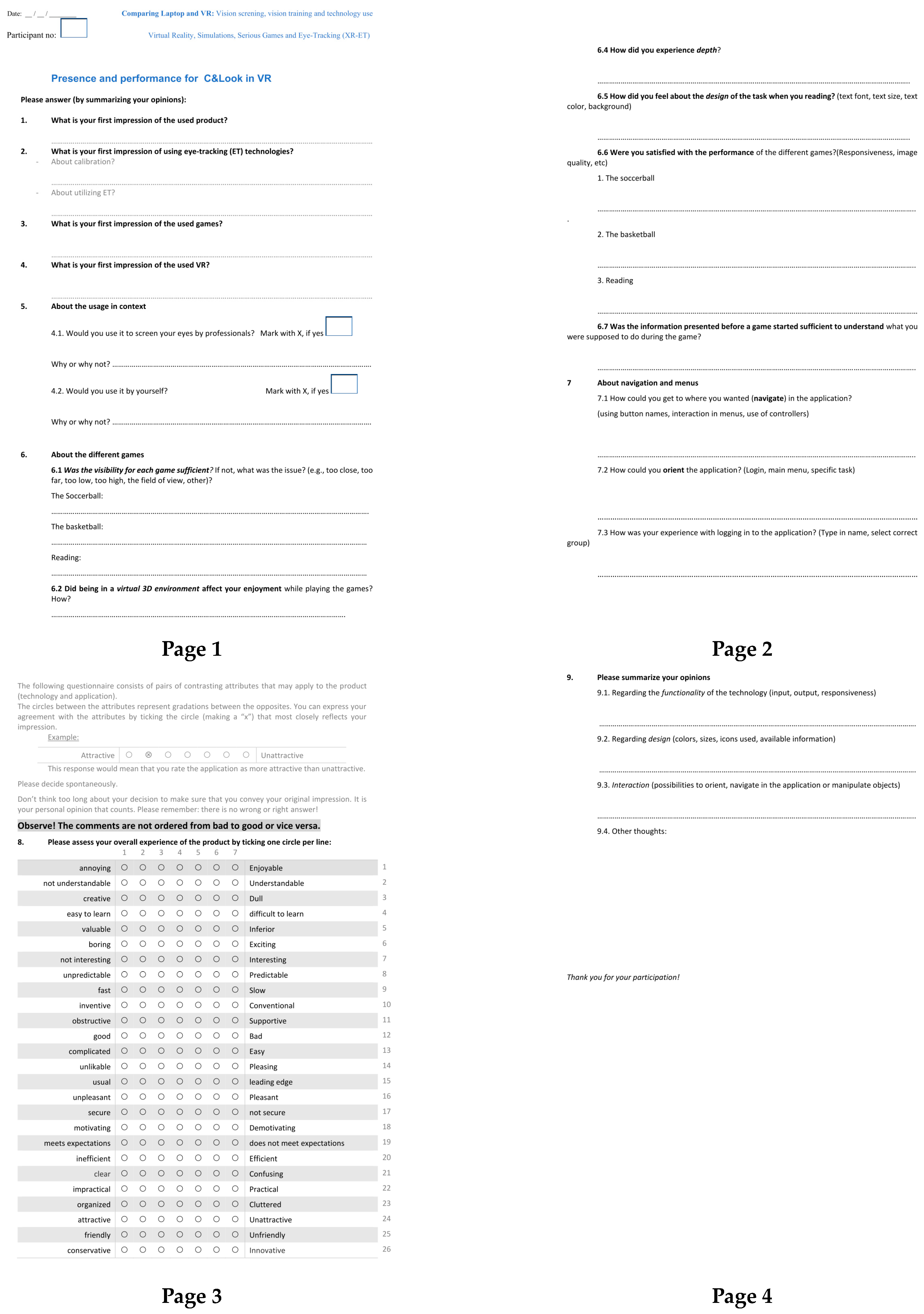
- Questionnaire about experiencing the laptop version of C&Look.
- Questionnaire about experiencing the VR version of C&Look.
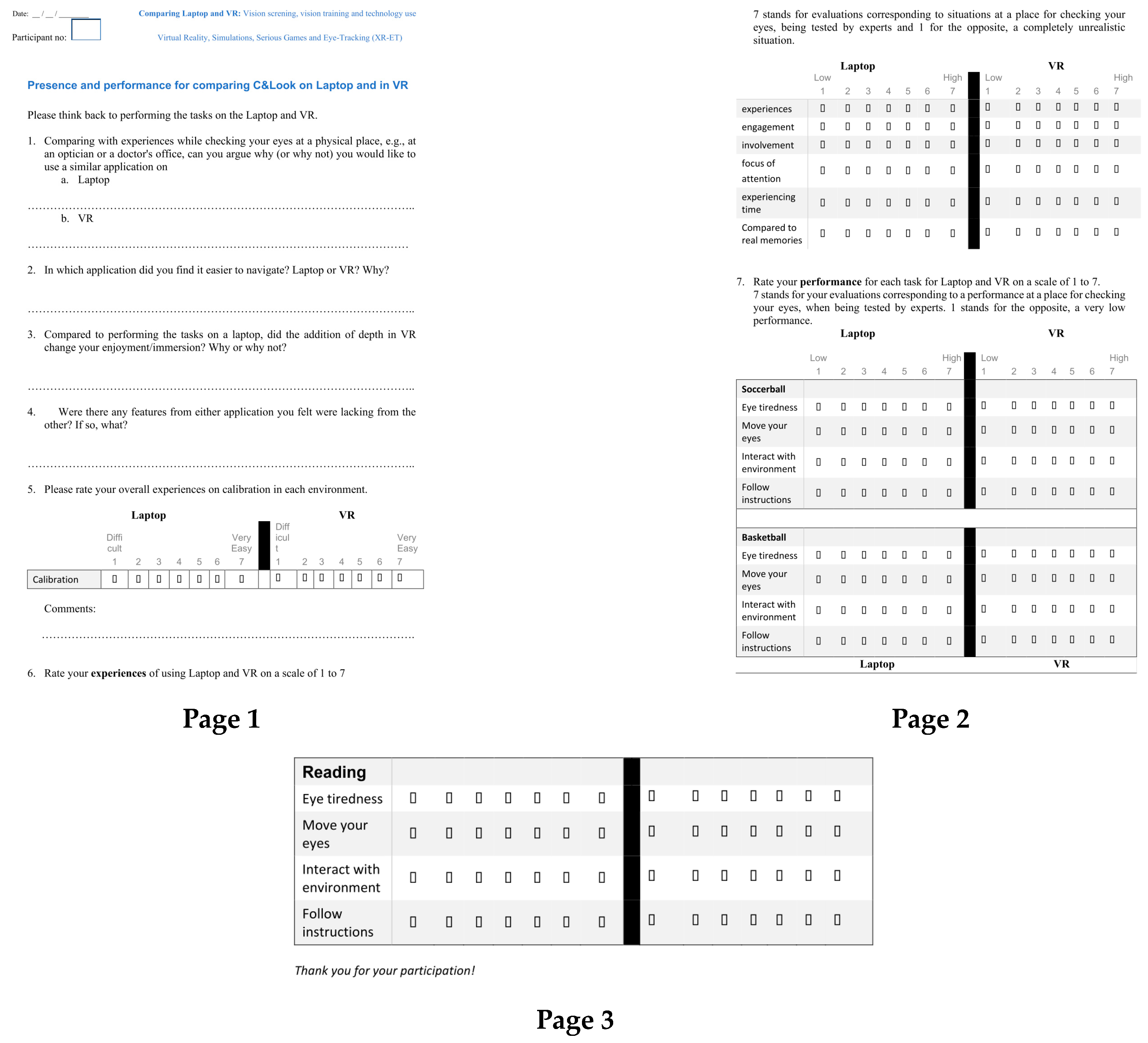
- Comparison questionnaire for the laptop and the VR application.
- Open-ended questions related to the feeling of presence and comparative elements of both applications.
- ET calibration experience questionnaire.
- Presence questionnaire for the laptop and the VR application.
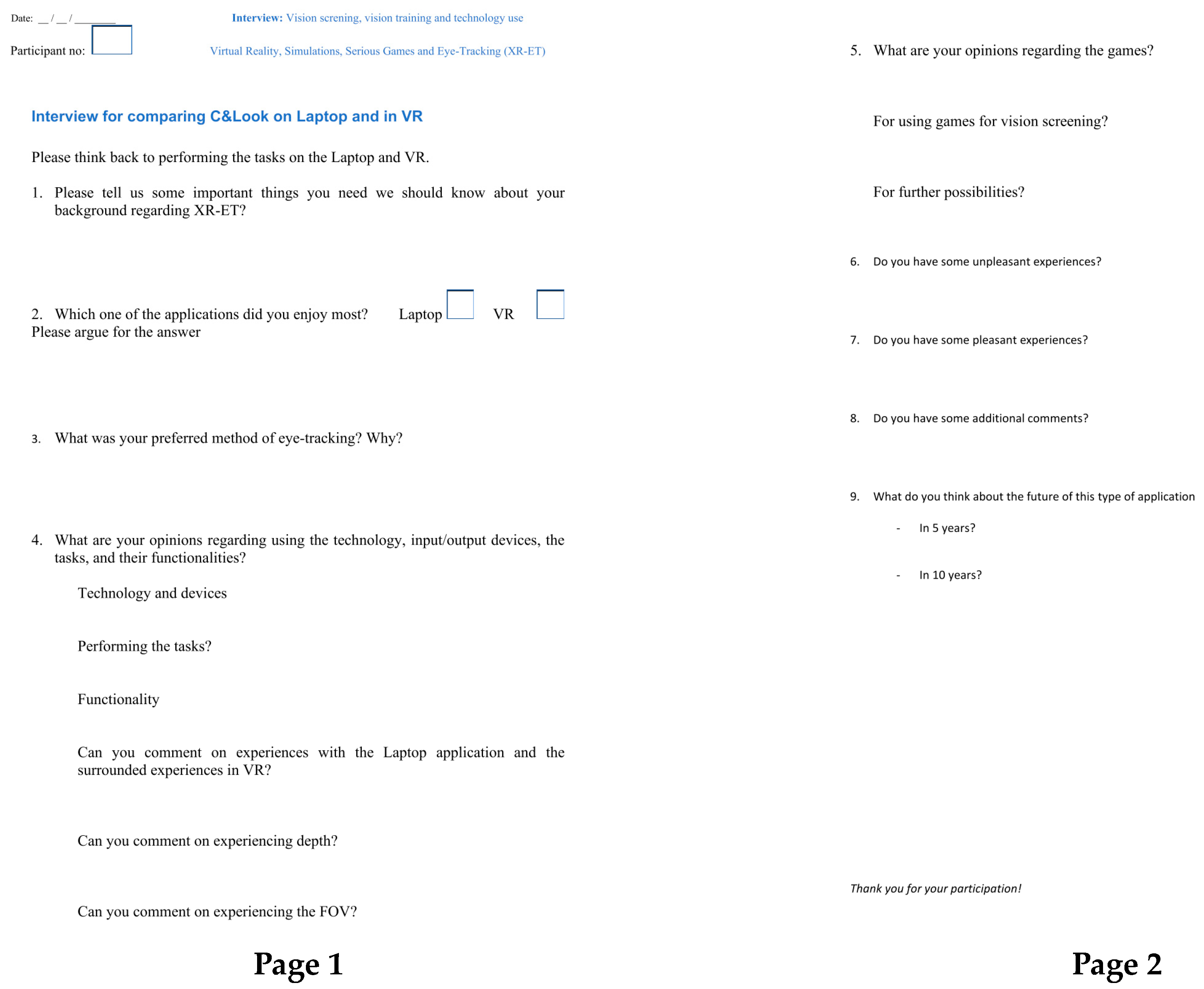
- Nine interview questions, with, after each, the possibility to discuss comparatively evaluating their presence and experiencing the technologies and serious games.
5. Results
5.1. Calibration Experience Results
5.2. Open-Ended Questionnaire Results
- Q: Comparing with experiences while checking your eyes at a physical place, e.g., at an optician or a doctor’s office, can you argue why (or why not) you would like to use a similar application on a laptop?
- Laptop:
- VR:
- Q: In which application did you find it easier to navigate? Laptop or VR? Why?
- Q: Compared to performing the tasks on a laptop, did the addition of depth in VR change your enjoyment/immersion? Why or why not?
- Q: Were there any features from either application that you felt were lacking from the other? If so, what?
- “Laptop is easier to understand/use”: indicated that participants found the laptop application easier to use, especially those with limited technological background or prior knowledge of the system.
- “Higher confidence in laptop results”: indicated an interest in better data representation and collection for the VR environment, leading to higher confidence in the laptop application’s results.
- “VR is more fun/exciting”: highlighted the additional immersive elements that VR brings, with an emphasis on enjoyment.
- “VR helps with focus”: included mentions of participants finding task performance easier or more motivating with fewer outside disturbances in VR.
- “VR is easier to navigate” and “Laptop is easier to navigate”: described preferences for different user interfaces and navigation options.
- “VR performance issues”: included responses that mentioned optimization issues in the VR application.
- “No Answer”: contained answers that were non-existent or completely unrelated.
5.3. Task Performance Similarity
5.4. Participant Opinions on Using Serious Games for Vision Screening
6. Discussion, Limitations, and Future Work
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Testing Battery







References
- Goldstand, S.; Koslowe, K.C.; Parush, S. Vision, visual-information processing, and academic performance among seventh-grade schoolchildren: A more significant relationship than we thought? Am. J. Occup. 2005, 59, 377–389. [Google Scholar] [CrossRef]
- Wilhelmsen, G.B.; Wankel, V.D. Friske øyne–svekket syn. English: Healthy eye-reduced vision. In Å Kartlegge Synsforstyrrelser Av Nevrol. Årsak. Bergen/Moss: Høgskolen I Bergen; English: Mapping vision problems of neurological cause; The University of Western Norway: Bergen, Norway, 2014. [Google Scholar]
- Eide, M.G.; Heldal, I.; Helgesen, C.G.; Birkeland Wilhelmsen, G.; Watanabe, R.; Geitung, A.; Soleim, H.; Costescu, C. Eye-tracking Complementing Manual Vision Screening for Detecting Oculomotor Dysfunction. In Proceedings of the 2019 E-Health and Bioengineering Conference (EHB), Iasi, Romania, 21–23 November 2019. [Google Scholar]
- Delazer, M.; Sojer, M.; Ellmerer, P.; Boehme, C.; Benke, T. Eye-tracking provides a sensitive measure of exploration deficits after acute right MCA stroke. Front. Neurol. 2018, 9, 359. [Google Scholar] [CrossRef]
- Rowe, F.; Brand, D.; Jackson, C.A.; Price, A.; Walker, L.; Harrison, S.; Eccleston, C.; Scott, C.; Akerman, N.; Dodridge, C.; et al. Visual impairment following stroke: Do stroke patients require vision assessment? Age Ageing 2009, 38, 188–193. [Google Scholar] [CrossRef]
- Ciuffreda, K.J.; Kapoor, N.; Rutner, D.; Suchoff, I.B.; Han, M.E.; Craig, S. Occurrence of oculomotor dysfunctions in acquired brain injury: A retrospective analysis. Optom. J. Am. Optom. Assoc. 2007, 78, 155–161. [Google Scholar] [CrossRef]
- Ambrosino, C.; Dai, X.; Antonio Aguirre, B.; Collins, M.E. Pediatric and School-Age Vision Screening in the United States: Rationale, Components, and Future Directions. Children 2023, 10, 490. [Google Scholar] [CrossRef]
- Heldal, I.; Helgesen, C.; Ali, Q.; Patel, D.; Geitung, A.B.; Pettersen, H. Supporting school aged children to train their vision by using serious games. Computers 2021, 10, 53. [Google Scholar] [CrossRef]
- WHO. Global Diffusion of eHealth: Making Universal Health Coverage Achievable: Report of the Third Global Survey on eHealth; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Ali, Q.; Heldal, I.; Helgesen, C.G.; Krumina, G.; Costescu, C.; Kovari, A.; Katona, J.; Thill, S. Current Challenges Supporting School-Aged Children with Vision Problems: A Rapid Review. Appl. Sci. 2021, 11, 9673. [Google Scholar] [CrossRef]
- Ali, Q.; Heldal, I.; Eide, M.G.; Helgesen, C. Using Eye-tracking Technologies in Vision Teachers’ Work–a Norwegian Perspective. In Proceedings of the 2020 E-Health and Bioengineering Conference (EHB), Iasi, Romania, 29–30 October 2020. [Google Scholar]
- Slater, M.; Usoh, M.; Steed, A. Depth of Presence in Virtual Environments. Presence Teleoperators Virtual Environ. 1994, 3, 130–144. [Google Scholar] [CrossRef]
- Slater, M.; Usoh, M. Presence in immersive virtual environments. In Proceedings of the Proceedings of IEEE Virtual Reality Annual International Symposium, Seattle, WA, USA, 18–22 September 1993; pp. 90–96. [Google Scholar]
- Loetscher, T.; Barrett, A.M.; Billinghurst, M.; Lange, B. Immersive medical virtual reality: Still a novelty or already a necessity? J. Neurol. Neurosurg. Psychiatry 2023, 94, 499–501. [Google Scholar] [CrossRef]
- Tang, Y.M.; Chau, K.Y.; Kwok, A.P.K.; Zhu, T.; Ma, X. A systematic review of immersive technology applications for medical practice and education–Trends, application areas, recipients, teaching contents, evaluation methods, and performance. Educ. Res. Rev. 2022, 35, 100429. [Google Scholar] [CrossRef]
- Adhanom, I.B.; MacNeilage, P.; Folmer, E. Eye Tracking in Virtual Reality: A Broad Review of Applications and Challenges. Virtual Real. 2023, 27, 1481–1505. [Google Scholar] [CrossRef]
- Ma, M.K.I.; Saha, C.; Poon, S.H.L.; Yiu, R.S.W.; Shih, K.C.; Chan, Y.K. Virtual reality and augmented reality—Emerging screening and diagnostic techniques in ophthalmology: A systematic review. Surv. Ophthalmol. 2022, 67, 1516–1530. [Google Scholar] [CrossRef] [PubMed]
- Lam, A.K.N.; To, E.; Weinreb, R.N.; Yu, M.; Mak, H.; Lai, G.; Chiu, V.; Wu, K.; Zhang, X.; Cheng, T.P.H.; et al. Use of Virtual Reality Simulation to Identify Vision-Related Disability in Patients with Glaucoma. JAMA Ophthalmol. 2020, 138, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Goh, R.L.Z.; Kong, Y.X.G.; McAlinden, C.; Liu, J.; Crowston, J.G.; Skalicky, S.E. Objective Assessment of Activity Limitation in Glaucoma with Smartphone Virtual Reality Goggles: A Pilot Study. Transl. Vis. Sci. Technol. 2018, 7, 10. [Google Scholar] [CrossRef] [PubMed]
- Gopalakrishnan, S.; Jacob, C.E.; Kumar, M.; Karunakaran, V.; Raman, R. Development of Immersive Virtual Reality Environment for Assessment of Functional Vision in people with Low Vision: A Pilot Study. J. Ophthalmol. 2022, 14, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Sargur, K.; Kartha, A.; Sadeghi, R.; Bradley, C.; Dagnelie, G. Functional Vision Assessment in People with Ultra-Low Vision using Virtual Reality: A Reduced Version. Investig. Ophthalmol. Vis. Sci. 2022, 63, 4055-F0019. [Google Scholar]
- Falkenberg, H.K.; Mathisen, T.S.; Ormstad, H.; Eilertsen, G. “Invisible” visual impairments. A qualitative study of stroke survivors’ experience of vision symptoms, health services and impact of visual impairments. BMC Health Serv. Res. 2020, 20, 302. [Google Scholar] [CrossRef]
- Wilhelmsen, G.B.; Felder, M. Structured Visual Learning and Stimulation in School: An Intervention Study. Creat. Educ. 2021, 12, 757–779. [Google Scholar] [CrossRef]
- Nazir, M.; Nabeel, T. Effects of Training of Eye Fixation Skills on the Reading Fluency of Children with Oculomotor Dysfunction. Pak. J. Educ. 2019, 36, 61–80. [Google Scholar]
- Dæhlen, A.; Heldal, I.; Katona, J. Towards Developing an Immersive Virtual Reality Applications for Supporting Vision Screening–A User Study. J. Appl. Tech. Educ. Sci. 2022, 12, 330. [Google Scholar]
- Ali, Q.; Heldal, I.; Helgesen, C.G.; Dæhlen, A. Serious Games for Vision Training Exercises with Eye-Tracking Technologies: Lessons from Developing a Prototype. Information 2022, 13, 569. [Google Scholar] [CrossRef]
- Niehorster, D.C.; Hessels, R.S.; Benjamins, J.S.; Nyström, M.; Hooge, I.T.C. GlassesValidator: A data quality tool for eye tracking glasses. Behav. Res. Methods 2023. [Google Scholar] [CrossRef] [PubMed]
- Heldal, I. The Usability of Collaborative Virtual Environments: Towards an Evaluation Framework; Chalmers: Gothenburg, Sweden, 2004. [Google Scholar]
- Safikhani, S.; Keller, S.; Schweiger, G.; Pirker, J. Immersive virtual reality for extending the potential of building information modeling in architecture, engineering, and construction sector: Systematic review. Int. J. Digit. Earth 2022, 15, 503–526. [Google Scholar] [CrossRef]
- Lin, J.; Zhu, R.; Li, N.; Becerik-Gerber, B. Do people follow the crowd in building emergency evacuation? A cross-cultural immersive virtual reality-based study. Adv. Eng. Inform. 2020, 43, 13. [Google Scholar] [CrossRef]
- Radianti, J.; Majchrzak, T.A.; Fromm, J.; Wohlgenannt, I. A systematic review of immersive virtual reality applications for higher education: Design elements, lessons learned, and research agenda. Comput. Educ. 2020, 147, 103778. [Google Scholar] [CrossRef]
- Mao, R.Q.; Lan, L.; Kay, J.; Lohre, R.; Ayeni, O.R.; Goel, D.P.; Sa, D.d. Immersive Virtual Reality for Surgical Training: A Systematic Review. J. Surg. Res. 2021, 268, 40–58. [Google Scholar] [CrossRef]
- Garrett, B.; Taverner, T.; Masinde, W.; Gromala, D.; Shaw, C.; Negraeff, M. A rapid evidence assessment of immersive virtual reality as an adjunct therapy in acute pain management in clinical practice. Clin. J. Pain 2014, 30, 1089–1098. [Google Scholar] [CrossRef]
- Zhao, J.; Xu, X.; Jiang, H.; Ding, Y. The effectiveness of virtual reality-based technology on anatomy teaching: A meta-analysis of randomized controlled studies. BMC Med. Educ. 2020, 20, 127. [Google Scholar] [CrossRef]
- Makransky, G.; Petersen, G.B. The Cognitive Affective Model of Immersive Learning (CAMIL): A Theoretical Research-Based Model of Learning in Immersive Virtual Reality. Educ. Psychol. Rev. 2021, 33, 937–958. [Google Scholar] [CrossRef]
- Žiak, P.; Holm, A.; Halička, J.; Mojžiš, P.; Piñero, D.P. Amblyopia treatment of adults with dichoptic training using the virtual reality oculus rift head mounted display: Preliminary results. BMC Ophthalmol. 2017, 17, 105. [Google Scholar] [CrossRef]
- Li, S.; Tang, A.; Yang, B.; Wang, J.; Liu, L. Virtual reality-based vision therapy versus OBVAT in the treatment of convergence insufficiency, accommodative dysfunction: A pilot randomized controlled trial. BMC Ophthalmol. 2022, 22, 182. [Google Scholar] [CrossRef]
- Nixon, N.; Thomas, P.B.; Jones, P.R. Feasibility study of an automated Strabismus screening Test using Augmented Reality and Eye-tracking (STARE). Eye 2023. Epub ahead of print. [Google Scholar] [CrossRef]
- Panachakel, J.T.; Ramakrishnan, A.G.; Manjunath, K.P. VR Glasses based Measurement of Responses to Dichoptic Stimuli: A Potential Tool for Quantifying Amblyopia? In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 5106–5110. [Google Scholar]
- Black, J.M.; Hess, R.F.; Cooperstock, J.R.; To, L.; Thompson, B. The measurement and treatment of suppression in amblyopia. J. Vis. Exp. 2012, 70, e3927. [Google Scholar] [CrossRef]
- Yeh, P.-H.; Liu, C.-H.; Sun, M.-H.; Chi, S.-C.; Hwang, Y.-S. To measure the amount of ocular deviation in strabismus patients with an eye-tracking virtual reality headset. BMC Ophthalmol. 2021, 21, 246. [Google Scholar] [CrossRef] [PubMed]
- Economides, J.R.; Adams, D.L.; Horton, J.C. Variability of Ocular Deviation in Strabismus. JAMA Ophthalmol. 2016, 134, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Pascal, J.I. The Angle of Deviation in Strabismus. Ophthalmologica 2010, 127, 184–189. [Google Scholar] [CrossRef]
- Leong, D.F.; Master, C.L.; Messner, L.V.; Pang, Y.; Smith, C.; Starling, A.J. The Effect of Saccadic Training on Early Reading Fluency. Clin. Pediatr. 2014, 53, 858–864. [Google Scholar] [CrossRef]
- Gallaway, M.; Scheiman, M.; Mitchell, G.L. Vision Therapy for Post-Concussion Vision Disorders. Optom. Vis. Sci. 2017, 94, 68–73. [Google Scholar] [CrossRef]
- Piccione, J.; Collett, J.; De Foe, A. Virtual skills training: The role of presence and agency. Heliyon 2019, 5, e02583. [Google Scholar] [CrossRef]
- Vaughn, W.; Maples, W.C.; Hoenes, R. The association between vision quality of life and academics as measured by the College of Optometrists in Vision Development Quality of Life questionnaire1 1OPTOMETRY VOLUME 77/NUMBER 3/MARCH 2006. Optom. J. Am. Optom. Assoc. 2006, 77, 116–123. [Google Scholar] [CrossRef]
- McClelland, M.M.; Acock, A.C.; Piccinin, A.; Rhea, S.A.; Stallings, M.C. Relations between preschool attention span-persistence and age 25 educational outcomes. Early Child. Res. Q. 2013, 28, 314–324. [Google Scholar] [CrossRef]
- Kiili, K.; Ketamo, H.; Kickmeier-Rust, M.D. Eye tracking in game-based learning research and game design. Int. J. Serious Games 2014, 1, 51–65. [Google Scholar] [CrossRef]
- Wong, C.L.; Lui, M.M.W.; Choi, K.C. Effects of immersive virtual reality intervention on pain and anxiety among pediatric patients undergoing venipuncture: A study protocol for a randomized controlled trial. Trials 2019, 20, 369. [Google Scholar] [CrossRef]
- Eide, G.M.; Watanabe, R. Detecting Oculomotor Problems in Children Using Eye-Tracking; University of Bergen: Bergen, Norway; Western Norway University of Applied Sciences: Bergen, Norway,, 2017. [Google Scholar]
- Deepa, B.M.S.; Valarmathi, A.; Benita, S. Assessment of stereo acuity levels using random dot stereo acuity chart in college students. J. Fam. Med. Prim. Care 2019, 8, 3850–3853. [Google Scholar] [CrossRef]
- Eide, M.G.; Watanabe, R.; Heldal, I.; Helgesen, C.; Geitung, A.; Soleim, H. Detecting oculomotor problems using eye tracking: Comparing EyeX and TX300. In Proceedings of the 2019 10th IEEE International Conference on Cognitive Infocommunications (CogInfoCom), Naples, Italy, 23–25 October 2019; pp. 381–388. [Google Scholar]
- Schrepp, M.; Thomaschewski, J.; Hinderks, A. Construction of a benchmark for the user experience questionnaire (UEQ). Int. J. Interact. Multimed. Artif. Intell. 2017, 4, 40–44. [Google Scholar] [CrossRef]
- Usoh, M.; Catena, E.; Arman, S.; Slater, M. Using Presence Questionnaires in Reality. Presence 2000, 9, 497–503. [Google Scholar] [CrossRef]
- Schroeder, R.; Heldal, I.; Tromp, J. The Usability of Collaborative Virtual Environments and Methods for the Analysis of Interaction. Presence 2006, 15, 655–667. [Google Scholar] [CrossRef]
- Holmqvist, K.; Örbom, S.L.; Hooge, I.T.C.; Niehorster, D.C.; Alexander, R.G.; Andersson, R.; Benjamins, J.S.; Blignaut, P.; Brouwer, A.-M.; Chuang, L.L.; et al. Eye tracking: Empirical foundations for a minimal reporting guideline. Behav. Res. Methods 2023, 55, 364–416. [Google Scholar] [CrossRef]
- Blignaut, P.; van Rensburg, E.J.; Oberholzer, M. Visualization and quantification of eye tracking data for the evaluation of oculomotor function. Heliyon 2019, 5, e01127. [Google Scholar] [CrossRef]
- Grassini, S.; Laumann, K.; Rasmussen Skogstad, M. The Use of Virtual Reality Alone Does Not Promote Training Performance (but Sense of Presence Does). Front. Psychol. 2020, 11, 1743. [Google Scholar] [CrossRef] [PubMed]
- Makransky, G.; Terkildsen, T.S.; Mayer, R.E. Adding immersive virtual reality to a science lab simulation causes more presence but less learning. Learn. Instr. 2019, 60, 225–236. [Google Scholar] [CrossRef]
- Ping, J.; Liu, Y.; Weng, D. Comparison in Depth Perception between Virtual Reality and Augmented Reality Systems. In Proceedings of the 2019 IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Osaka, Japan, 23–27 March 2019; pp. 1124–1125. [Google Scholar]
- Backus, B.T. Standardized Stereoacuity Testing in VR: The Vivid Vision Stereoacuity Test: Conference presentation. In Proceedings of the I Heart VT 2020, Online, 1–7 July 2020. [Google Scholar]
- Dæhlen, A. Towards Developing an Eye-Tracker Based Virtual Reality Application for Supporting Vision Screening; The University of Bergen: Bergen, Norway, 2022. [Google Scholar]
- Mees, L.; Upadhyaya, S.; Kumar, P.; Kotawala, S.; Haran, S.; Rajasekar, S.; Friedman, D.S.; Venkatesh, R. Validation of a head-mounted virtual reality visual field screening device. J. Glaucoma 2020, 29, 86–91. [Google Scholar] [CrossRef]
- Miao, Y.; Jeon, J.Y.; Park, G.; Park, S.W.; Heo, H. Virtual reality-based measurement of ocular deviation in strabismus. Comput. Methods Programs Biomed. 2020, 185, 105132. [Google Scholar] [CrossRef]
- David, E.J.; Beitner, J.; Võ, M.L.-H. The importance of peripheral vision when searching 3D real-world scenes: A gaze-contingent study in virtual reality. J. Vis. 2021, 21, 3. [Google Scholar] [CrossRef] [PubMed]
- Sauer, Y.; Sipatchin, A.; Wahl, S.; García García, M. Assessment of consumer VR-headsets’ objective and subjective field of view (FoV) and its feasibility for visual field testing. Virtual Real. 2022, 26, 1089–1101. [Google Scholar] [CrossRef]
- Diniz-Filho, A.; Boer, E.R.; Gracitelli, C.P.B.; Abe, R.Y.; van Driel, N.; Yang, Z.; Medeiros, F.A. Evaluation of Postural Control in Patients with Glaucoma Using a Virtual Reality Environment. Ophthalmology 2015, 122, 1131–1138. [Google Scholar] [CrossRef]
- Colenbrander, A. Assessment of functional vision and its rehabilitation. Acta Ophthalmol. 2010, 88, 163–173. [Google Scholar] [CrossRef]
- Schuetz, I.; Fiehler, K. Eye tracking in virtual reality: Vive pro eye spatial accuracy, precision, and calibration reliability. J. Eye Mov. Res. 2022, 15. [Google Scholar] [CrossRef]
- Bangay, S.; Preston, L. An investigation into factors influencing immersion in interactive virtual reality environments. Stud. Health Technol. Inform. 1998, 58, 43–51. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Task | Fixation | Smooth Pursuit | Reading |
|---|---|---|---|
| Eye tiredness | 4 | 3.85 | 3.86 |
| Move your eyes | 5 | 5.28 | 5.85 |
| Interact with environment | 4 | 4.28 | 4.57 |
| Follow instructions | 4 | 5.85 | 6.28 |
| Task | Fixation | Smooth Pursuit | Reading |
|---|---|---|---|
| Eye tiredness | 4.28 | 4.28 | 4.14 |
| Move your eyes | 4.85 | 5.28 | 5.85 |
| Interact with environment | 5.14 | 5.28 | 5.28 |
| Follow instructions | 6.14 | 5.85 | 6.42 |
| P Nr. | Experience with Vision Screening/Testing | Opinions about the Used Games |
|---|---|---|
| 1 | Has some previous experience with regular vision checkups from school. | “[The VR] worked well for the things we would like to accomplish…Changing the size of the objects was fun.” The participant also expressed that she enjoyed the fixation game more in VR for the enjoyment alone. She also mentioned appreciating the analysis application after screening on a laptop. She wished to have the possibility to screen the children’s eyes alone with a trustable gamified application. |
| 2 | Wears spectacles and undergoes eye tests every second year. | “A fun way to do screening, I think. I felt that when I am performing an eye test, I focus on the games, which is good. Here the eyes may work normally, as in reality.” He explained that his son is aged 5 and, as a parent, he would like to ensure that he has no vision problems. “This is an innovative way for vision testing. Although, elderly people may experience this otherwise.” |
| 3 | Has regular checkups at least every second year. | The games “were well designed. Most important is to see how my vision is moving when I follow objects.” “I also believe that the games are not only useful for doctors and opticians, but also for schools, universities, or other workplaces needing to measure the employees’ focus or help children to learn better by showing them eventual problems with their eyes.” |
| 4 | Had vision problems at a younger age, so they have experience with regular vision controls. No longer has any vision problems today. | “It is an entertaining way to test, especially in VR. I liked the easy applications. Maybe to construct an environment with more games and being able, maybe, to change the figures would be fun.” “If I know the game is trustable and cost and time effective, I may test my eyes in this way rather than go to the optician. However, I believe this also has several ethical questions behind it.” |
| 5 | Wears spectacles and undergoes regular controls (frequency not specified). | “I like the idea to test your eyes with games. I [also liked experiencing] more depth in ‘games’, which should be exploited for more traditional games as well, adding more experience.” He also “believes that depth perception can be measured on laptops”. |
| 6 | Wears spectacles and undergoes regular controls (frequency not specified). | “I prefer ET and games on laptop because it is faster and takes up info better. VR [was] more difficult.” While it was “cooler with VR, [it was] more practical on laptops”. VR was “a bit more like in reality, but it is moving from a distance”. “The reading tasks was better on a laptop.” It was “a bit boring to read in VR […] you should put more interesting text there”. |
| 7 | Wears spectacles and undergoes eye tests every year. | “Games easy to understand and intuitive, except that the VR had some lagging for basketball … framerate drops. Overall, a nice experience to see and to understand how things [the eyes] are focusing … maybe we can avoid eye specialists.” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dæhlen, A.; Heldal, I.; Ali, Q. Technologies Supporting Screening Oculomotor Problems: Challenges for Virtual Reality. Computers 2023, 12, 134. https://doi.org/10.3390/computers12070134
Dæhlen A, Heldal I, Ali Q. Technologies Supporting Screening Oculomotor Problems: Challenges for Virtual Reality. Computers. 2023; 12(7):134. https://doi.org/10.3390/computers12070134
Chicago/Turabian StyleDæhlen, Are, Ilona Heldal, and Qasim Ali. 2023. "Technologies Supporting Screening Oculomotor Problems: Challenges for Virtual Reality" Computers 12, no. 7: 134. https://doi.org/10.3390/computers12070134
APA StyleDæhlen, A., Heldal, I., & Ali, Q. (2023). Technologies Supporting Screening Oculomotor Problems: Challenges for Virtual Reality. Computers, 12(7), 134. https://doi.org/10.3390/computers12070134