
Low Rates of Intrapulmonary Local Recurrence After Laser Metastasectomy: A Single-Center Retrospective Cohort Study of Colorectal Cancer Metastases †

 , , , and
, , , and
Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients and Data Collection
2.2. Operative Procedure
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
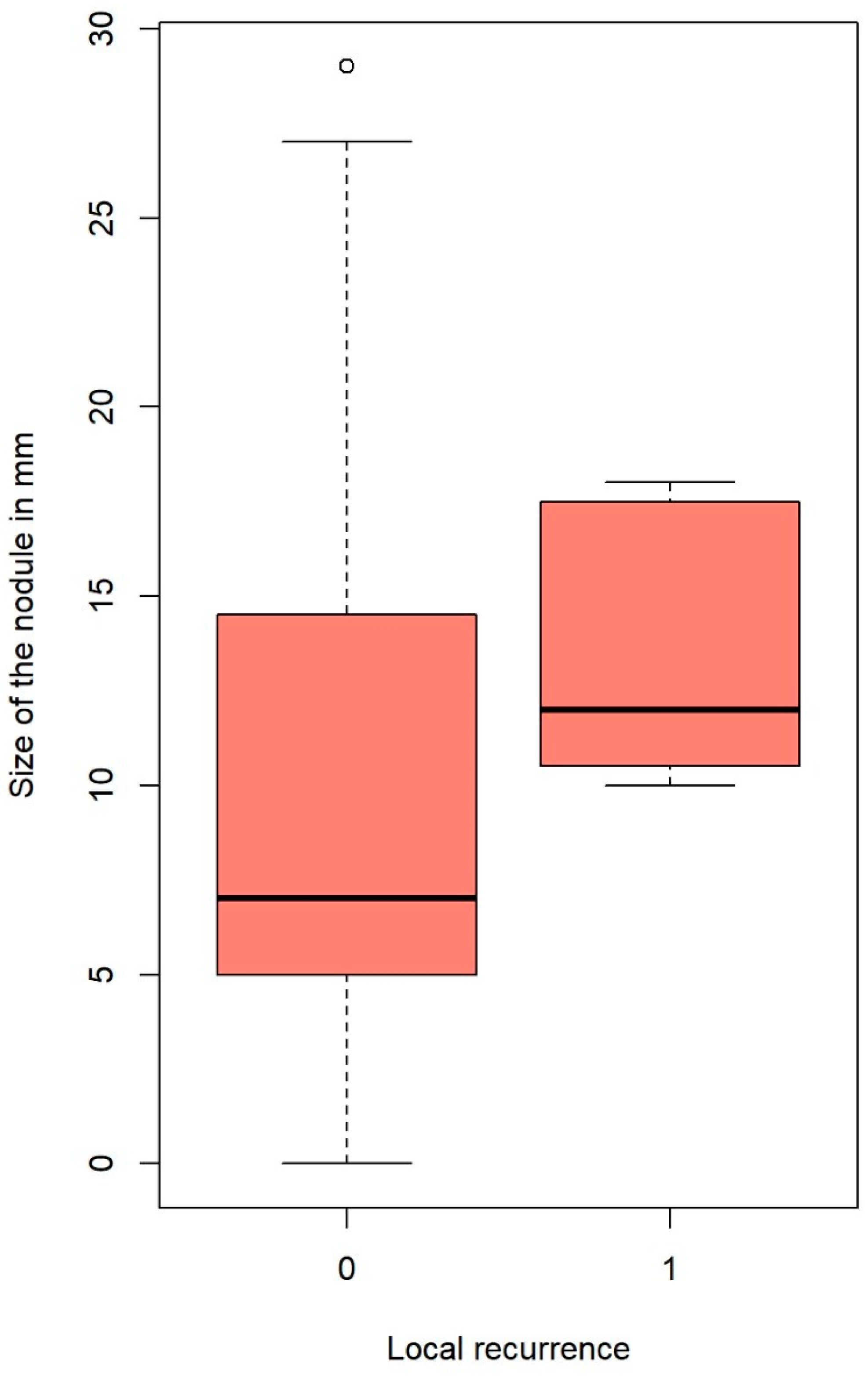
3.2. Local Recurrence and Associated Factors
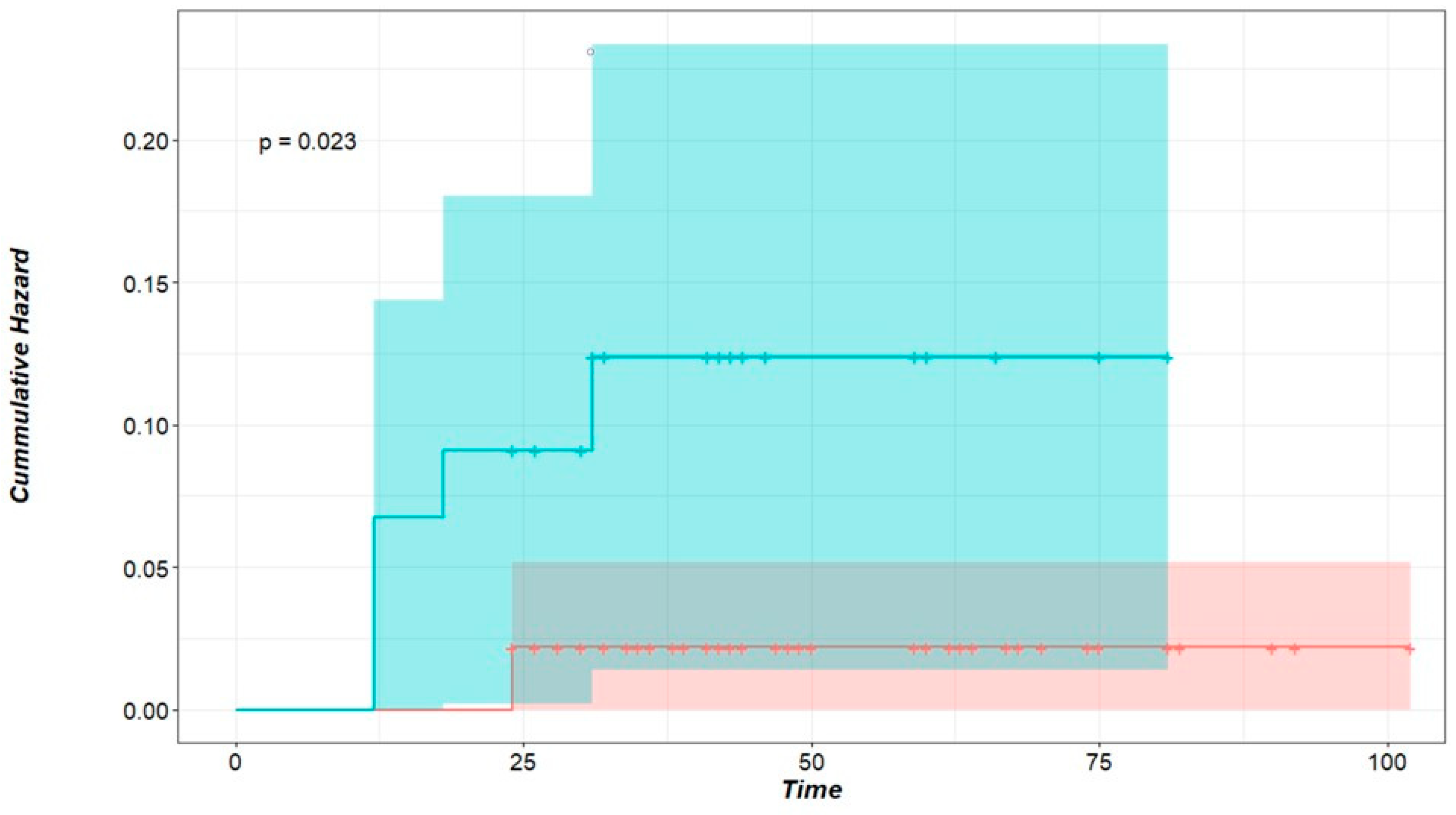
3.3. Survival Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CT | Computed tomography |
| CRC | Colorectal cancer |
| DFI | Disease-free interval |
| LL | Lower lobe |
| LR | Local recurrence |
| LPM | Laser-assisted pulmonary metastasectomy |
| ML | Middle lobe |
| Nd:YAG | Neodymium-doped yttrium aluminum garnet |
| PM | Pulmonary metastasectomy |
| R | Resection state |
| STAS | Spread through air spaces |
| SD | Standard deviation |
| SEM | Standard error of mean |
| UL | Upper lobe |
| VATS | Video-assisted thoracic surgery |
References
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aguilar, E.A.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, S.; Bouvier, A.M.; Lepage, C.; Hatem, C.; Dancourt, V.; Faivre, J. Incidence and patterns of recurrence after resection for cure of colonic cancer in a well defined population. J. Br. Surg. 2006, 93, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Gerull, W.D.; Puri, V.; Kozower, B.D. The epidemiology and biology of pulmonary metastases. J. Thorac. Dis. 2021, 13, 2585. [Google Scholar] [CrossRef]
- Panagiotopoulos, N.; Patrini, D.; Lawrence, D.; Scarci, M.; Mitsos, S. Pulmonary metastasectomy and laser-assisted resection. J. Thorac. Dis. 2018, 10 (Suppl. 17), S1930. [Google Scholar] [CrossRef]
- Shishido, Y.; Ishii, M.; Maeda, T.; Kokado, Y.; Masuya, D.; Kusama, T.; Fujimoto, K.; Higashiyama, H. Survival outcomes of lung metastases from colorectal cancer treated with pulmonary metastasectomy or modern systemic chemotherapy: A single institution experience. J. Cardiothorac. Surg. 2023, 18, 327. [Google Scholar] [CrossRef]
- Matsuguma, H.; Mun, M.; Sano, A.; Yoshino, I.; Hashimoto, H.; Shintani, Y.; Iida, T.; Shiono, S.; Chida, M.; Kuroda, H.; et al. Time to incurable recurrence for patients treated with pulmonary metastasectomy for colorectal cancer. Ann. Surg. Oncol. 2022, 29, 6909–6917. [Google Scholar] [CrossRef]
- Prisciandaro, E.; Bertolaccini, L.; Fieuws, S.; Cara, A.; Spaggiari, L.; Huang, L.; Petersen, R.H.; Ambrogi, M.C.; Sicolo, E.; Barbarossa, A.; et al. Multicentre retrospective analysis on pulmonary metastasectomy: An European perspective. Eur. J. Cardio-Thorac. Surg. 2024, 65, ezae141. [Google Scholar] [CrossRef]
- Gonzalez, M.; Brunelli, A.; Szanto, Z.; Passani, S.; Falcoz, P.E. Report from the European Society of Thoracic Surgeons database 2019: Current surgical practice and perioperative outcomes of pulmonary metastasectomy. Eur. J. Cardio-Thorac. Surg. 2021, 59, 996–1003. [Google Scholar] [CrossRef]
- Brandi, G.; Derenzini, E.; Falcone, A.; Masi, G.; Loupakis, F.; Pietrabissa, A.; Pinna, A.D.; Ercolani, G.; Pantaleo, M.A.; Di Girolamo, S.; et al. Adjuvant systemic chemotherapy after putative curative resection of colorectal liver and lung metastases. Clin. Color. Cancer 2013, 12, 188–194. [Google Scholar] [CrossRef]
- Handy, J.R.; Bremner, R.M.; Crocenzi, T.S.; Detterbeck, F.C.; Fernando, H.C.; Fidias, P.M.; Firestone, S.; Johnstone, C.A.; Lanuti, M.; Litle, V.R.; et al. Expert consensus document on pulmonary metastasectomy. Ann. Thorac. Surg. 2019, 107, 631–649. [Google Scholar] [CrossRef]
- Higashiyama, M.; Tokunaga, T.; Nakagiri, T.; Ishida, D.; Kuno, H.; Okami, J. Pulmonary metastasectomy: Outcomes and issues according to the type of surgical resection. Gen. Thorac. Cardiovasc. Surg. 2015, 63, 320–330. [Google Scholar] [CrossRef]
- Welter, S.; La Raia, R.B.; Gupta, V. Pursuit of an optimal surgical margin in pulmonary metastasectomy. J. Vis. Surg. 2019, 5, 39. [Google Scholar] [CrossRef]
- Welter, S.; Jacobs, J.; Krbek, T.; Poettgen, C.; Stamatis, G. Prognostic impact of lymph node involvement in pulmonary metastases from colorectal cancer. Eur. J. Cardio-Thorac. Surg. 2007, 31, 167–172. [Google Scholar] [CrossRef]
- Claramunt, N.P.; Hwang, D.; de Perrot, M.; Yasufuku, K.; Darling, G.; Pierre, A.; Donahoe, L.; Yeung, J.; Tomlinson, G.; Englesakis, M.; et al. Incidence of ipsilateral side recurrence after open or video-assisted thoracic surgery resection of colorectal lung metastases. Ann. Thorac. Surg. 2020, 109, 1591–1597. [Google Scholar] [CrossRef]
- Forster, C.; Ojanguren, A.; Perentes, J.Y.; Zellweger, M.; Krueger, T.; Abdelnour-Berchtold, E.; Gonzalez, M. Survival prognostic and recurrence risk factors after single pulmonary metastasectomy. J. Cardiothorac. Surg. 2021, 16, 357. [Google Scholar] [CrossRef]
- Mammana, M.; Baldi, M.; Melan, L.; Dell’Amore, A.; Rea, F. Laser-assisted lung metastasectomy: A systematic review. Updates Surg. 2023, 75, 1783–1793. [Google Scholar] [CrossRef]
- Rolle, A.; Kozłowski, M. Laser resection of lung parenchyma--a new technical and clinical approach. Rocz. Akad. Med. W Bialymst. 2005, 50, 193–196. [Google Scholar]
- Welter, S.; Theegarten, D.; Trarbach, T.; Maletzki, F.; Stamatis, G.; Tötsch, M. Safety distance in the resection of colorectal lung metastases: A prospective evaluation of satellite tumor cells with immunohistochemistry. J. Thorac. Cardiovasc. Surg. 2011, 141, 1218–1222. [Google Scholar] [CrossRef]
- Shiono, S.; Ishii, G.; Nagai, K.; Yoshida, J.; Nishimura, M.; Murata, Y.; Tsuta, K.; Kim, Y.H.; Nishiwaki, Y.; Kodama, T.; et al. Predictive factors for local recurrence of resected colorectal lung metastases. Ann. Thorac. Surg. 2005, 80, 1040–1045. [Google Scholar] [CrossRef]
- Welter, S.; Arfanis, E.; Christoph, D.; Hager, T.; Roesel, C.; Aigner, C.; Weinreich, G.; Theegarten, D. Growth patterns of pulmonary metastases: Should we adjust resection techniques to primary histology and size? Eur. J. Cardio-Thorac. Surg. 2017, 52, 39–46. [Google Scholar] [CrossRef]
- Nelson, D.B.; Tayob, N.; Mitchell, K.G.; Correa, A.M.; Hofstetter, W.L.; Sepesi, B.; Walsh, G.L.; Vaporciyan, A.A.; Swisher, S.G.; Antonoff, M.B.; et al. Surgical margins and risk of local recurrence after wedge resection of colorectal pulmonary metastases. J. Thorac. Cardiovasc. Surg. 2019, 157, 1648–1655. [Google Scholar] [CrossRef]
- Chung, J.H.; Lee, S.H.; Yi, E.; Lim, J.Y.; Jung, J.S.; Son, H.S.; Sun, K. Impact of resection margin length and tumor depth on the local recurrence after thoracoscopic pulmonary wedge resection of a single colorectal metastasis. J. Thorac. Dis. 2019, 11, 1879. [Google Scholar] [CrossRef]
- Hermanek, P.; Wittekind, C. The pathologist and the residual tumor (R) classification. Pathol. Res. Pract. 1994, 190, 115–123. [Google Scholar] [CrossRef]
- Rolle, A.; Koch, R.; Alpard, S.K.; Zwischenberger, J.B. Lobe-sparing resection of multiple pulmonary metastases with a new 1318-nm Nd: YAG laser—First 100 patients. Ann. Thorac. Surg. 2002, 74, 865–869. [Google Scholar] [CrossRef]
- Franzke, K.; Natanov, R.; Zinne, N.; Rajab, T.K.; Biancosino, C.; Zander, I.; Lodziewski, S.; Ricklefs, M.; Kropivnitskaya, I.; Schmitto, J.D.; et al. Pulmonary metastasectomy–A retrospective comparison of surgical outcomes after laser-assisted and conventional resection. Eur. J. Surg. Oncol. 2017, 43, 1357–1364. [Google Scholar] [CrossRef]
- Treasure, T.; Farewell, V.; Macbeth, F.; Monson, K.; Williams, N.R.; Brew-Graves, C.; Lees, B.; Grigg, O.; Fallowfield, L. Pulmonary metastasectomy versus continued active monitoring in colorectal cancer (PulMiCC): A multicentre randomised clinical trial. Trials 2019, 20, 718. [Google Scholar] [CrossRef]
- Stefani, A.; Oricchio, F.; Cinquepalmi, A.; Aramini, B.; Morandi, U. Is laser-assisted resection preferable to lobectomy for pulmonary metastasectomy? Lasers Med. Sci. 2020, 35, 611–620. [Google Scholar] [CrossRef]
- Baum, D.; Rolle, A.; Koschel, D.; Rostock, L.; Decker, R.; Sombati, M.; Öhme, F.; Plönes, T. Long-Term Follow-Up after Laser-Assisted Pulmonary Metastasectomy Shows Complete Lung Function Recovery. Cancers 2024, 16, 1762. [Google Scholar] [CrossRef]
- Pastorino, U.; Buyse, M.; Friedel, G.; Ginsberg, R.J.; Girard, P.; Goldstraw, P.; Johnston, M.; McCormack, P.; Pass, H.; Putna, J.B., Jr. Long-term results of lung metastasectomy: Prognostic analyses based on 5206 cases. J. Thorac. Cardiovasc. Surg. 1997, 113, 37–49. [Google Scholar] [CrossRef]
- Prisciandaro, E.; Ceulemans, L.J.; Van Raemdonck, D.E.; Decaluwe, H.; De Leyn, P.; Bertolaccini, L. Impact of the extent of lung resection on postoperative outcomes of pulmonary metastasectomy for colorectal cancer metastases: An exploratory systematic review. J. Thorac. Dis. 2022, 14, 2677. [Google Scholar] [CrossRef]
- Ambrogi, M.C.; Aprile, V.; Sanna, S.; Forti Parri, S.N.; Rizzardi, G.; Fanucchi, O.; Valentini, L.; Italiani, A.; Morganti, R.; Cartia, C.F.; et al. Lung Metastasectomy: Where Do We Stand? Results from an Italian Multicentric Prospective Database. J. Clin. Med. 2024, 13, 3106. [Google Scholar]
- Pfannschmidt, J.; Dienemann, H.; Hoffmann, H. Surgical resection of pulmonary metastases from colorectal cancer: A systematic review of published series. Ann. Thorac. Surg. 2007, 84, 324–338. [Google Scholar] [CrossRef]
- Vogelsang, H.; Haas, S.; Hierholzer, C.; Berger, U.; Siewert, J.R.; Präuer, H. Factors influencing survival after resection of pulmonary metastases from colorectal cancer. J. Br. Surg. 2004, 91, 1066–1071. [Google Scholar] [CrossRef]
- Shiono, S.; Okumura, T.; Boku, N.; Hishida, T.; Ohde, Y.; Sakao, Y.; Yoshiya, K.; Hyodo, I.; Mori, K.; Kondo, H. Outcomes of segmentectomy and wedge resection for pulmonary metastases from colorectal cancer. Eur. J. Cardio-Thorac. Surg. 2017, 51, 504–510. [Google Scholar] [CrossRef]
- Macherey, S.; Doerr, F.; Wahlers, T.; Hekmat, K. Role of laser resection in pulmonary metastasectomy. Pneumologie 2017, 71, 475–479. [Google Scholar]
- Ojanguren, A.; Karenovics, W.; Dackam, S.; Demarchi, M.; Triponez, F. Laser pulmonary metastasectomy by video-assisted thoracic surgery. J. Vis. Surg. 2019, 5, 40. [Google Scholar] [CrossRef]
- Sassorossi, C.; Chiappetta, M.; Nachira, D.; Campanella, A.; Santoro, G.; Calabrese, G.; Scognamiglio, C.; Napolitano, A.G.; Senatore, A.; Petracca Ciavarella, L.; et al. Uniportal Laser-Assisted Video-Assisted Thoracoscopy (U-LA-VATS) for Lung Metastasectomy: Technical Description, Peri-Operative Results and Pertinent Literature Review. J. Clin. Med. 2024, 13, 5346. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Patients/Percent | Local Recurrence Patients (Percent) | ||
|---|---|---|---|
| Gender | Male | 33 (67.3%) | 4 (12.1%) |
| Female | 16 (32.6%) | 1 (6.2%) | |
| Age group | ≤35 Years | 2 (4.8%) | 0 |
| 35–55 Years | 5 (10.2%) | 0 | |
| ≥55 Years | 42 (85.7%) | 5 (11.3%) | |
| Disease spread | Unilateral | 25 (51.0%) | 2 (8.0%) |
| Bilateral | 24 (49.0%) | 3 (12.0%) | |
| DFI in months (n = 45) | <36 | 35 (77.8%) | 3 (8.5%) |
| ≥36 | 10 (22.2%) | 2 (20%) | |
| Extrapulmonary invasion | Yes | 0 | 0 |
| No | 49 | 5 (10.2%) | |
| Single nodule | Yes | 14 | 2 (14.2%) |
| No | 35 | 3 (8.5%) | |
| Surgical access | VATS | 4 | 0 |
| Thoracotomy | 45 | 5 (11.1%) | |
| Lymph node metastasis | Yes | 1 | 0 |
| No | 48 | 5 (10.4%) | |
| Age | mean | 65.2 | |
| SD | 11.8 | ||
| SEM | 1.68 | ||
| DFI in months (NA = 4) | Mean | 15.8 | |
| SD | 18.5 | ||
| SEM | 2.6 | ||
| Number of nodules per patient | Mean | 2.7 | |
| SD | 2.5 | ||
| SEM | 0.37 | ||
| Post-observation time in months | mean | 46.0 | |
| SD | 19.7 | ||
| SEM | 2.46 |
| Number (Percent) | Local Recurrence/Nodule (Percent) | ||
|---|---|---|---|
| Gender | Male | 92 (66.2%) | 6 (6.5%) |
| Female | 47 (33.8%) | 1 (2.1%) | |
| R status | R0 | 93 (66.9%) | 2 (2.1%) |
| Rx | 46 (33.1%) | 5 (10.9%) | |
| Size | <12 mm | 94 (67.6%) | 3 (3.2%) |
| ≥12 mm | 45 (32.4%) | 4 (8.9%) | |
| Number of nodules | Single | 14 (10.1%) | 2 (14.3%) |
| Multiple | 125 (89.9%) | 5 (4.0%) | |
| Laterality | Ipsilateral | 38 (27.3%) | 2 (5.3%) |
| Bilateral | 101(72.7%) | 5 (5.0%) | |
| Node location | LL | 68 (48.9%) | 2 (3.0%) |
| ML | 16 (11.5%) | 1 (6.2%) | |
| UL | 55 (39.6%) | 4 (7.3%) | |
| Total | 139 | 7 (5.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shalabi, A.; Shalabi, S.F.; Graeter, T.; Welter, S.; Ehab, A.; Kuon, J. Low Rates of Intrapulmonary Local Recurrence After Laser Metastasectomy: A Single-Center Retrospective Cohort Study of Colorectal Cancer Metastases. Cancers 2025, 17, 683. https://doi.org/10.3390/cancers17040683
Shalabi A, Shalabi SF, Graeter T, Welter S, Ehab A, Kuon J. Low Rates of Intrapulmonary Local Recurrence After Laser Metastasectomy: A Single-Center Retrospective Cohort Study of Colorectal Cancer Metastases. Cancers. 2025; 17(4):683. https://doi.org/10.3390/cancers17040683
Chicago/Turabian StyleShalabi, Ahmad, Sundus F. Shalabi, Thomas Graeter, Stefan Welter, Ahmed Ehab, and Jonas Kuon. 2025. "Low Rates of Intrapulmonary Local Recurrence After Laser Metastasectomy: A Single-Center Retrospective Cohort Study of Colorectal Cancer Metastases" Cancers 17, no. 4: 683. https://doi.org/10.3390/cancers17040683
APA StyleShalabi, A., Shalabi, S. F., Graeter, T., Welter, S., Ehab, A., & Kuon, J. (2025). Low Rates of Intrapulmonary Local Recurrence After Laser Metastasectomy: A Single-Center Retrospective Cohort Study of Colorectal Cancer Metastases. Cancers, 17(4), 683. https://doi.org/10.3390/cancers17040683