
Unmasking Racial, Ethnic, and Socioeconomic Disparities in United States Chordoma Clinical Trials: Systematic Review

 ,
, 
 ,
,  ,
,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
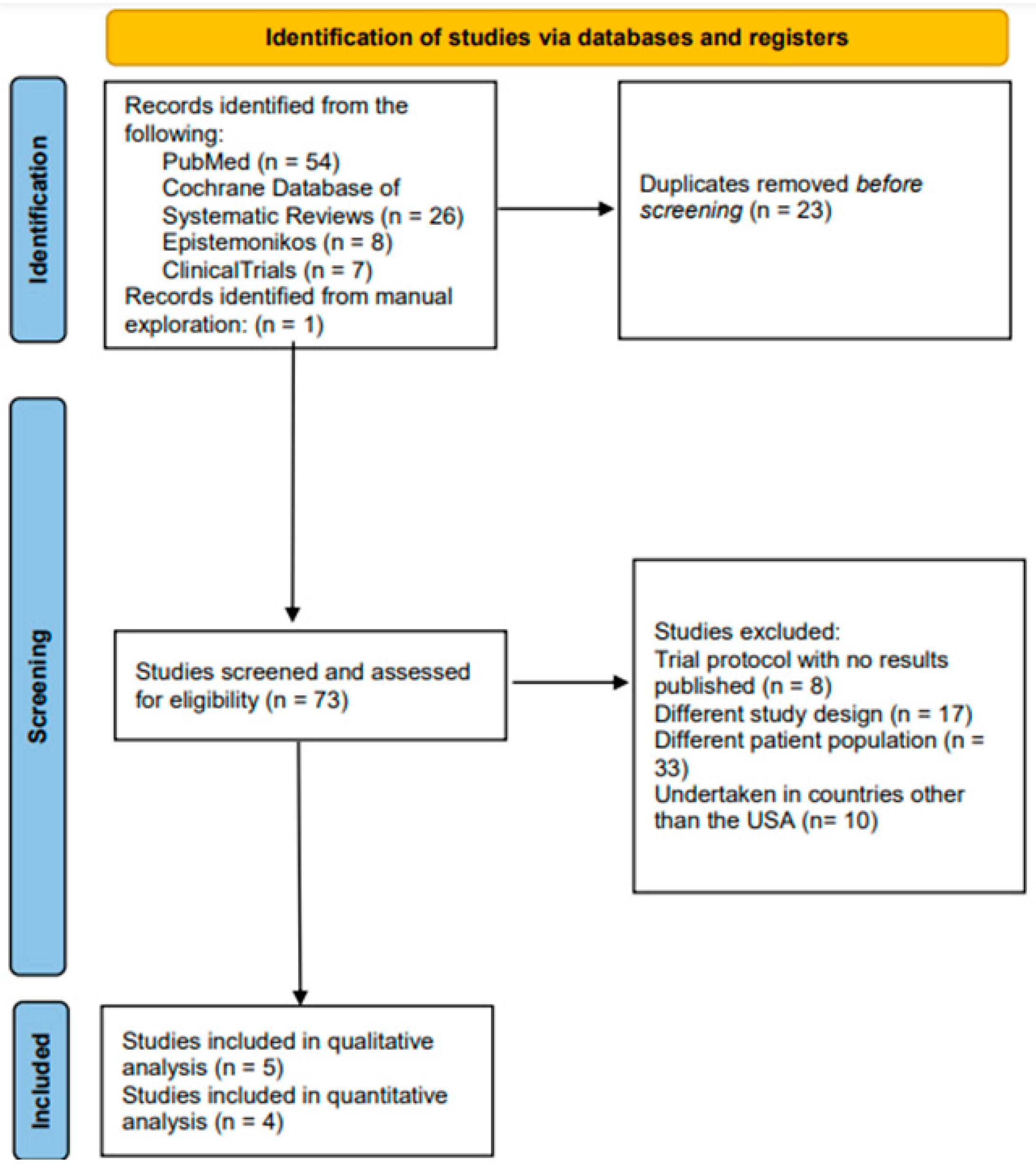
2.1. Search Strategy
2.2. Study Selection
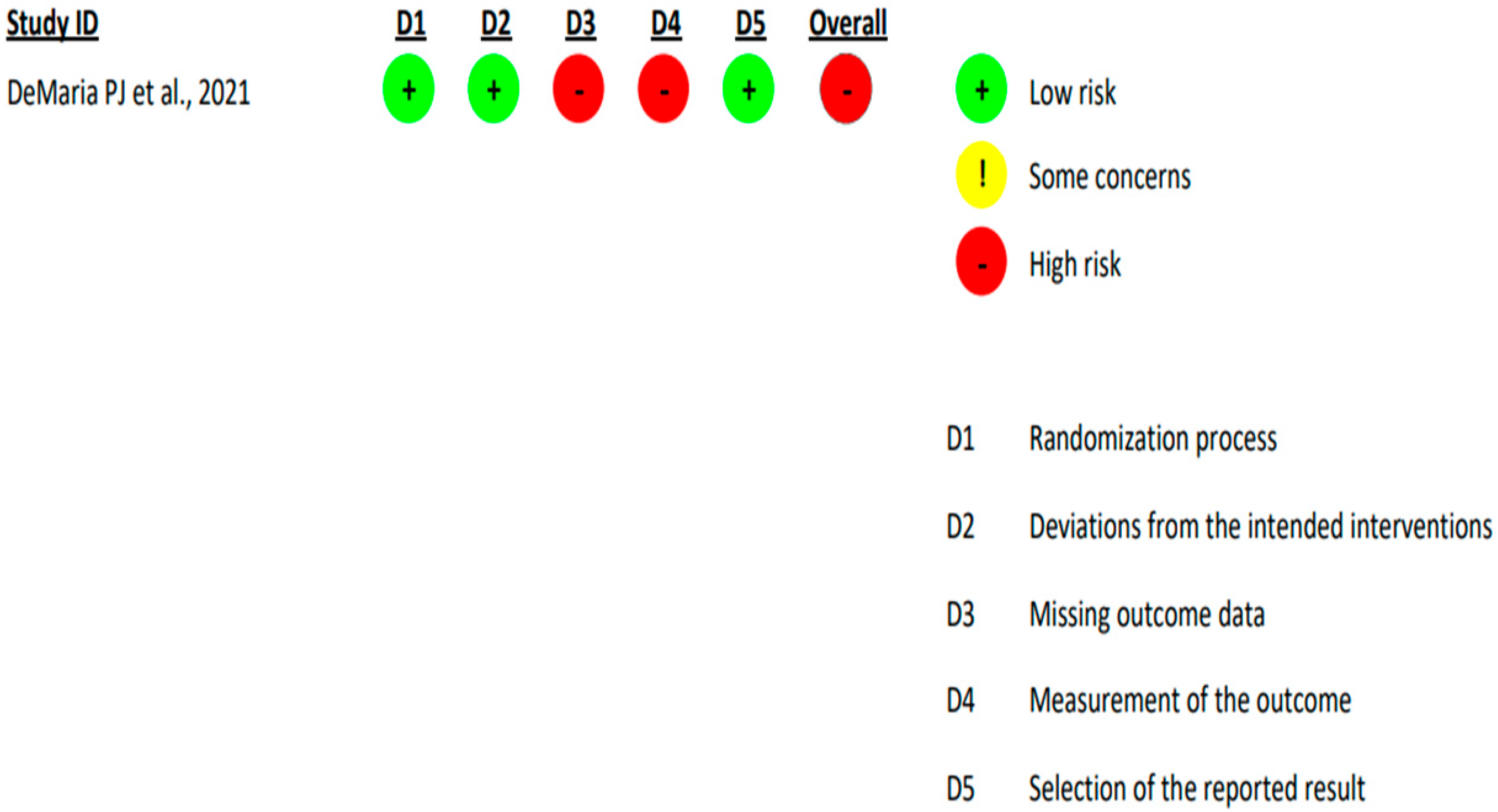
2.3. Quality Assessment and Risk of Bias
2.4. Statistical Analysis
3. Results
3.1. General Patient Demographics and Trial Characteristics
3.2. Quality Assessment and Risk of Bias
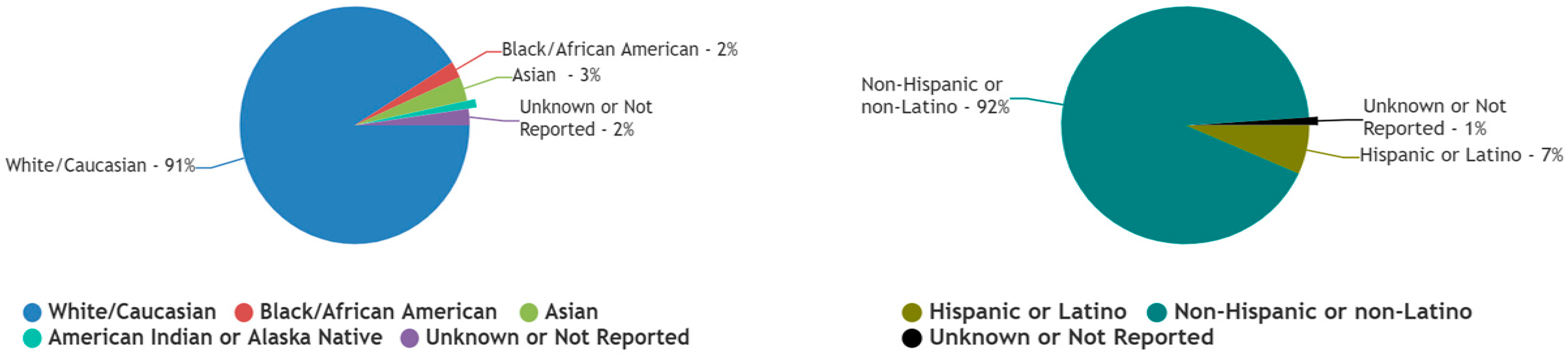
3.3. Race and Ethnicity
3.3.1. White/Caucasian Patients
3.3.2. Black/African American Patients
3.3.3. Asian Patients
3.3.4. American Indian or Alaska Native Patients
3.3.5. Native Hawaiian or Other Pacific Islander Patients
3.3.6. Unknown or Not Reported Racial Data
3.3.7. Hispanic or Latino Patients
3.3.8. Non-Hispanic or Latino Patients
3.3.9. Unknown or Not Reported Ethnicity Data
3.4. Measures of Socioeconomic Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Fiore, G.; Porto, E.; Bertani, G.A.; Marcus, H.J.; Saladino, A.; Pradilla, G.; DiMeco, F.; Locatelli, M. The Burden of Skull Base Chordomas: Insights from a Meta-Analysis of Observational Studies. Neurosurg. Focus 2024, 56, E13. [Google Scholar] [CrossRef]
- Karpathiou, G.; Dumollard, J.M.; Dridi, M.; Dal Col, P.; Barral, F.-G.; Boutonnat, J.; Peoc’h, M. Chordomas: A Review with Emphasis on Their Pathophysiology, Pathology, Molecular Biology, and Genetics. Pathol. Res. Pract. 2020, 216, 153089. [Google Scholar] [CrossRef]
- Barber, S.M.; Sadrameli, S.S.; Lee, J.J.; Fridley, J.S.; Teh, B.S.; Oyelese, A.A.; Telfeian, A.E.; Gokaslan, Z.L. Chordoma-Current Understanding and Modern Treatment Paradigms. J. Clin. Med. 2021, 10, 1054. [Google Scholar] [CrossRef]
- Campilan, B.; Schroeder, C.; Sagaityte, E.; Arditi, J.; Leary, O.P.; Gokaslan, Z.L.; Sullivan, P.L.Z.; Martinez-Moreno, M. Animal Model Considerations for Chordoma Research: Reproducing the Tumor Microenvironment in Vivo with Humanized Mice. Front. Oncol. 2024, 14, 1330254. [Google Scholar] [CrossRef] [PubMed]
- Agosti, E.; Antonietti, S.; Zeppieri, M.; Ius, T.; Fiorindi, A.; Tel, A.; Robiony, M.; Panciani, P.P.; Fontanella, M.M. Chordoma Genetic Aberrations and Targeted Therapies Panorama: A Systematic Literature Review. J. Clin. Med. 2024, 13, 2711. [Google Scholar] [CrossRef]
- Holtzman, A.L.; Bates, J.E.; Morris, C.G.; Rutenberg, M.S.; Indelicato, D.J.; Tavanaiepour, D.; Mendenhall, W.M. Impact of Type of Treatment Center and Access to Care on Mortality and Survival for Skull Base Chordoma and Chondrosarcoma. J. Neurol. Surg. Part B Skull Base 2022, 83, 328–338. [Google Scholar] [CrossRef]
- Ullah, A.; Kenol, G.S.; Lee, K.T.; Yasinzai, A.Q.K.; Waheed, A.; Asif, B.; Khan, I.; Sharif, H.; Khan, J.; Heneidi, S.; et al. Chordoma: Demographics and survival analysis with a focus on racial disparities and the role of surgery, a U.S. population-based study. Clin. Transl. Oncol. 2024, 26, 109–118. [Google Scholar] [CrossRef]
- Parry, D.M.; McMaster, M.L.; Liebsch, N.J.; Patronas, N.J.; Quezado, M.M.; Zametkin, D.; Yang, X.R.; Goldstein, A.M. Clinical Findings in Families with Chordoma with and without T Gene Duplications and in Patients with Sporadic Chordoma Reported to the Surveillance, Epidemiology, and End Results Program. J. Neurosurg. 2020, 134, 1399–1408. [Google Scholar] [CrossRef] [PubMed]
- Nieblas-Bedolla, E.; Christophers, B.; Williams, J.R.; Power-Hays, A.; Jimenez, N.; Rodriguez, A. Racial and Ethnic Disparities among Children with Primary Central Nervous System Tumors in the US. J. Neurooncol. 2021, 152, 451–466. [Google Scholar] [CrossRef] [PubMed]
- Mohan, S.V.; Freedman, J. A Review of the Evolving Landscape of Inclusive Research and Improved Clinical Trial Access. Clin. Pharmacol. Ther. 2023, 113, 518–527. [Google Scholar] [CrossRef]
- Donzo, M.W.; Nguyen, G.; Nemeth, J.K.; Owoc, M.S.; Mady, L.J.; Chen, A.Y.; Schmitt, N.C. Effects of Socioeconomic Status on Enrollment in Clinical Trials for Cancer: A Systematic Review. Cancer Med. 2024, 13, e6905. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological Index for Non-Randomized Studies (Minors): Development and Validation of a New Instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Hoelen, T.-C.A.; Willems, P.C.; Loenen, A.; Meisel, H.J.; Wang, J.C.; Jain, A.; Buser, Z.; Arts, J.J.; AO Spine Knowledge Forum Degenerative. The Evidence for the Use of Osteobiologics in Hybrid Constructs (Anterior Cervical Discectomy and Fusion and Total Disc Replacement) in Multilevel Cervical Degenerative Disc Disease: A Systematic Review. Glob. Spine J. 2024, 14, 120S–128S. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau.Gov|U.S. Census Bureau Homepage. Available online: https://www.census.gov/en.html (accessed on 21 September 2024).
- Kesari, S.; Wagle, N.; Carrillo, J.A.; Sharma, A.; Nguyen, M.; Truong, J.; Gill, J.M.; Nersesian, R.; Nomura, N.; Rahbarlayegh, E.; et al. Pilot Study of High-Dose Pemetrexed in Patients with Progressive Chordoma. Clin. Cancer Res. 2024, 30, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Bavarian Nordic A Phase 2 Trial of BN-Brachyury and Radiation Therapy in Patients with Advanced Chordoma; clinicaltrials.gov. 2023. Available online: https://clinicaltrials.gov/study/NCT03595228 (accessed on 11 January 2025).
- DeMaria, P.J.; Bilusic, M.; Park, D.M.; Heery, C.R.; Donahue, R.N.; Madan, R.A.; Bagheri, M.H.; Strauss, J.; Shen, V.; Marté, J.L.; et al. Randomized, Double-Blind, Placebo-Controlled Phase II Study of Yeast-Brachyury Vaccine (GI-6301) in Combination with Standard-of-Care Radiotherapy in Locally Advanced, Unresectable Chordoma. Oncologist 2021, 26, e847–e858. [Google Scholar] [CrossRef] [PubMed]
- Cote, G.M.; Barysauskas, C.M.; DeLaney, T.F.; Schwab, J.; Raskin, K.; Lozano-Calderon, S.; Bernstein, K.; Mullen, J.T.; Haynes, A.B.; Hornicek, F.; et al. A Phase 1 Study of Nilotinib Plus Radiation in High-Risk Chordoma. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1496–1504. [Google Scholar] [CrossRef] [PubMed]
- Fenerty, K.E.; Folio, L.R.; Patronas, N.J.; Marté, J.L.; Gulley, J.L.; Heery, C.R. Predicting Clinical Outcomes in Chordoma Patients Receiving Immunotherapy: A Comparison between Volumetric Segmentation and RECIST. BMC Cancer 2016, 16, 672. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau QuickFacts: United States. Available online: https://www.census.gov/quickfacts/fact/table/US/PST045222 (accessed on 21 September 2024).
- Das, P.; Soni, P.; Jones, J.; Habboub, G.; Barnholtz-Sloan, J.S.; Recinos, P.F.; Kshettry, V.R. Descriptive Epidemiology of Chordomas in the United States. J. Neurooncol. 2020, 148, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Lou, S.; Yao, T. Trends in Primary Malignant Bone Cancer Incidence and Mortality in the United States, 2000–2017: A Population-Based Study. J. Bone Oncol. 2024, 46, 100607. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Ulloa, R.; Soffer, J.; Alcazar-Felix, R.J.; Snyderman, C.H.; Gardner, P.A.; Patel, V.A.; Polster, S.P. Chordoma: A Comprehensive Systematic Review of Clinical Trials. Cancers 2023, 15, 5800. [Google Scholar] [CrossRef] [PubMed]
- Wani, A.K.; Prakash, A.; Sena, S.; Akhtar, N.; Singh, R.; Chopra, C.; Ariyanti, E.E.; Mudiana, D.; Yulia, N.D.; Rahayu, F. Unraveling Molecular Signatures in Rare Bone Tumors and Navigating the Cancer Pathway Landscapes for Targeted Therapeutics. Crit. Rev. Oncol. Hematol. 2024, 196, 104291. [Google Scholar] [CrossRef]
- Ganga, A.; Kim, E.J.; Lee, J.Y.; Leary, O.P.; Sastry, R.A.; Fridley, J.S.; Chang, K.-E.; Niu, T.; Sullivan, P.Z.; Somasundar, P.S.; et al. Disparities in Primary Spinal Osseous Malignant Bone Tumor Survival by Medicaid Status: A National Population-Based Risk Analysis. World Neurosurg. 2024, 181, e192–e202. [Google Scholar] [CrossRef] [PubMed]
- Taha, B.; Winston, G.; Tosi, U.; Hartley, B.; Hoffman, C.; Dahmane, N.; Mason, C.E.; Greenfield, J.P. Missing Diversity in Brain Tumor Trials. Neuro-Oncol. Adv. 2020, 2, vdaa059. [Google Scholar] [CrossRef] [PubMed]
- Elsamadicy, A.A.; Sayeed, S.; Sherman, J.J.Z.; Hengartner, A.C.; Pennington, Z.; Hersh, A.M.; Lo, S.-F.L.; Shin, J.H.; Mendel, E.; Sciubba, D.M. Racial Disparities in the Management and Outcomes of Primary Osseous Neoplasms of the Spine: A SEER Analysis. J. Neurooncol. 2024, 166, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Bhatia, N.N.; Hoang, B.H.; Ziogas, A.; Zell, J.A. Analysis of Prognostic Factors for Patients with Chordoma with Use of the California Cancer Registry. J. Bone Joint Surg. Am. 2012, 94, 356–363. [Google Scholar] [CrossRef]
- Battistin, U.; Nguyen, R.; Ghaith, A.K.; El-Hajj, V.G.; Soltan, F.; Ghaith, S.; Weinberg, J.H.; Elmi-Terander, A.; Grossbach, A.J.; Akinduro, O.O. The Impact of Socioeconomic Determinants on the Access to Care and Survival in Patients with Spinal Chordomas- a National Cancer Database Analysis. J. Neurooncol. 2024, 169, 359–368. [Google Scholar] [CrossRef]
- Baynam, G.; Baker, S.; Steward, C.; Summar, M.; Halley, M.; Pariser, A. Increasing Diversity, Equity, Inclusion, and Accessibility in Rare Disease Clinical Trials. Pharm. Med. 2024, 38, 261–276. [Google Scholar] [CrossRef] [PubMed]
- Vuong, I.; Wright, J.; Nolan, M.B.; Eggen, A.; Bailey, E.; Strickland, R.; Traynor, A.; Downs, T. Overcoming Barriers: Evidence-Based Strategies to Increase Enrollment of Underrepresented Populations in Cancer Therapeutic Clinical Trials-a Narrative Review. J. Cancer Educ. 2020, 35, 841–849. [Google Scholar] [CrossRef] [PubMed]
- Slade, A.L.; Retzer, A.; Ahmed, K.; Kyte, D.; Keeley, T.; Armes, J.; Brown, J.M.; Calman, L.; Gavin, A.; Glaser, A.W.; et al. Systematic Review of the Use of Translated Patient-Reported Outcome Measures in Cancer Trials. Trials 2021, 22, 306. [Google Scholar] [CrossRef] [PubMed]
- Niranjan, S.J.; Martin, M.Y.; Fouad, M.N.; Vickers, S.M.; Wenzel, J.A.; Cook, E.D.; Konety, B.R.; Durant, R.W. Bias and Stereotyping among Research and Clinical Professionals: Perspectives on Minority Recruitment for Oncology Clinical Trials. Cancer 2020, 126, 1958–1968. [Google Scholar] [CrossRef]
- Julian McFarlane, S.; Occa, A.; Peng, W.; Awonuga, O.; Morgan, S.E. Community-Based Participatory Research (CBPR) to Enhance Participation of Racial/Ethnic Minorities in Clinical Trials: A 10-Year Systematic Review. Health Commun. 2022, 37, 1075–1092. [Google Scholar] [CrossRef] [PubMed]
- Warren, R.C.; Shedlin, M.G.; Alema-Mensah, E.; Obasaju, C.; Hodge, D.A. Clinical Trials Participation Among African Americans and the Ethics of Trust: Leadership Perspectives. J. Healthc. Sci. Humanit. 2020, 10, 104–123. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, S.D.; Somers, F.; Boudes, M.; Nafria, B.; Robinson, P. Using Patient Perspectives to Inform Better Clinical Trial Design and Conduct: Current Trends and Future Directions. Pharm. Med. 2023, 37, 129–138. [Google Scholar] [CrossRef]
- Coyle, M.; Gillies, K. A Systematic Review of Risk Communication in Clinical Trials: How Does It Influence Decisions to Participate and What Are the Best Methods to Improve Understanding in a Trial Context? PLoS ONE 2020, 15, e0242239. [Google Scholar] [CrossRef]
- Levit, L.A.; Byatt, L.; Lyss, A.P.; Paskett, E.D.; Levit, K.; Kirkwood, K.; Schenkel, C.; Schilsky, R.L. Closing the Rural Cancer Care Gap: Three Institutional Approaches. JCO Oncol. Pract. 2020, 16, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Briel, M.; Elger, B.S.; McLennan, S.; Schandelmaier, S.; von Elm, E.; Satalkar, P. Exploring Reasons for Recruitment Failure in Clinical Trials: A Qualitative Study with Clinical Trial Stakeholders in Switzerland, Germany, and Canada. Trials 2021, 22, 844. [Google Scholar] [CrossRef] [PubMed]
- MacLennan, D.L.; Plahovinsak, J.L.; MacLennan, R.J.; Jones, C.T. Clinical Trial Site Perspectives and Practices on Study Participant Diversity and Inclusion. Clin. Pharmacol. Ther. 2023, 113, 670–679. [Google Scholar] [CrossRef]
- Wedekind, M.F.; Reilly, K.M.; Rivero, J.D.; Lockridge, R.; Allen, T.; Raygada, M.; Bernstein, D.; Thomas, B.J.; Vivelo, C.; Levine, J.; et al. NCI Intramural Program Approach to Rare Tumors: Natural History Study of Rare Solid Tumors in Children and Adults: A Longitudinal, Comprehensive Data and Biospecimen Collection Protocol. Pediatr. Blood Cancer 2023, 70, e30495. [Google Scholar] [CrossRef]
- Abdel-Rahman, S.M.; Wimes, M.P.; Curran, T. A Call to Action: Issuing a Diversity and Inclusion Challenge to Research Organizations. Clin. Transl. Sci. 2021, 14, 2095–2098. [Google Scholar] [CrossRef] [PubMed]
- Le-Rademacher, J.; Gunn, H.; Yao, X.; Schaid, D.J. Clinical Trials Overview: From Explanatory to Pragmatic Clinical Trials. Mayo Clin. Proc. 2023, 98, 1241–1253. [Google Scholar] [CrossRef] [PubMed]
- Robertson, D.S.; Choodari-Oskooei, B.; Dimairo, M.; Flight, L.; Pallmann, P.; Jaki, T. Point Estimation for Adaptive Trial Designs I: A Methodological Review. Stat. Med. 2023, 42, 122–145. [Google Scholar] [CrossRef]
- Petkovic, J.; Jull, J.; Yoganathan, M.; Dewidar, O.; Baird, S.; Grimshaw, J.M.; Johansson, K.A.; Kristjansson, E.; McGowan, J.; Moher, D.; et al. Reporting of Health Equity Considerations in Cluster and Individually Randomized Trials. Trials 2020, 21, 308. [Google Scholar] [CrossRef]
- Muehlemann, N.; Zhou, T.; Mukherjee, R.; Hossain, M.I.; Roychoudhury, S.; Russek-Cohen, E. A Tutorial on Modern Bayesian Methods in Clinical Trials. Ther. Innov. Regul. Sci. 2023, 57, 402–416. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Sridhar, S.; Hollingsworth, R.; Chit, A.; Kimball, T.; Murmello, K.; Greenberg, M.; Gurunathan, S.; Chen, J. Hybrid Clinical Trials to Generate Real-World Evidence: Design Considerations from a Sponsor’s Perspective. Contemp. Clin. Trials 2020, 94, 105856. [Google Scholar] [CrossRef] [PubMed]
- Hughson, J.-A.; Woodward-Kron, R.; Parker, A.; Hajek, J.; Bresin, A.; Knoch, U.; Phan, T.; Story, D. A Review of Approaches to Improve Participation of Culturally and Linguistically Diverse Populations in Clinical Trials. Trials 2016, 17, 263. [Google Scholar] [CrossRef]
- Bodicoat, D.H.; Routen, A.C.; Willis, A.; Ekezie, W.; Gillies, C.; Lawson, C.; Yates, T.; Zaccardi, F.; Davies, M.J.; Khunti, K. Promoting Inclusion in Clinical Trials-a Rapid Review of the Literature and Recommendations for Action. Trials 2021, 22, 880. [Google Scholar] [CrossRef] [PubMed]
- Hankivsky, O.; Springer, K.W.; Hunting, G. Beyond Sex and Gender Difference in Funding and Reporting of Health Research. Res. Integr. Peer Rev. 2018, 3, 6. [Google Scholar] [CrossRef] [PubMed]
- Pothuri, B.; Blank, S.V.; Myers, T.K.; Hines, J.F.; Randall, L.M.; O’Cearbhaill, R.E.; Slomovitz, B.M.; Eskander, R.N.; Alvarez Secord, A.; Coleman, R.L.; et al. Inclusion, Diversity, Equity, and Access (IDEA) in Gynecologic Cancer Clinical Trials: A Joint Statement from GOG Foundation and Society of Gynecologic Oncology (SGO). Gynecol. Oncol. 2023, 174, 278–287. [Google Scholar] [CrossRef]
- Acuña-Villaorduña, A.; Baranda, J.C.; Boehmer, J.; Fashoyin-Aje, L.; Gore, S.D. Equitable Access to Clinical Trials: How Do We Achieve It? Am. Soc. Clin. Oncol. Educ. Book 2023, 43, e389838. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Study and Year | Patients | Age | Race and Ethnicity of Patients | Intervention | Outcome |
|---|---|---|---|---|---|
| Kesari S et al., 2024 [17] | 15 | Median age: 61 years (Range: 30–80) | Race: 86.7% White (n = 13) and 13.3% Asian (n = 2) Ethnicity: 86.7% Not Hispanic or Latino (n = 13) and 3.2% Hispanic or Latino (n = 2) | Pemetrexed | Median Progression-free survival (PFS) = 10.5 months 6-month PFS = 67% Stable disease = 10/14 participants (71%) |
| Bavarian Nordic, 2023 [18] | 29 | Mean age: 65.9 (10.82) | Race: 89.7% White (n = 26), 3.4% Black or African American (n = 1), and 6.9% Unknown or Not Reported (n = 2) Ethnicity: 89.7% Not Hispanic or Latino (n = 26), 6.9% Hispanic or Latino (n = 2), and 3.4% Unknown or Not Reported (n = 1) | BN Brachyury + Standard-of-Care Radiotherapy | Objective Response Rate (ORR) = 7.7 (95% CI, 2.6 to 20.8) |
| DeMaria PJ et al., 2021 [19] | 24 | Median age: 61 years (Range: 30–76) | Race: 87.5% White (n = 21), 4.2% Black or African American (n = 1), 4.2% Asian (n = 1), and 4.2% American Indian or Alaska Native (n = 1) Ethnicity: 95.8% Not Hispanic or Latino (n = 23) and 4.2% Hispanic or Latino (n = 1) | Yeast–Brachyury Vaccine (GI-6301) + Standard-of-Care Radiotherapy | Overall Response Rate = vaccine arm 9% (1/11 patients) and placebo arm 8% (1/13 patients) PFS = vaccine arm median 20.6 months (95% CI, 5.7 to 37.5 months) and placebo arm median 25.9 months (95% CI, 9.2 to 30.8 months) OS = vaccine arm median 37.5 months (95% CI, 21.6 to 50.6 months) and placebo arm median not reached |
| Cote GM et al., 2018 [20] | 22 | Median age: 65 years (Range: 30–83) | Race: 100% White (n = 22) Ethnicity: 95.5% Not Hispanic or Latino (n = 21) and 4.5% Hispanic or Latino (n = 1) | Nilotinib + Standard-of-Care Radiotherapy | ORR: 6% (1/18 patients, 95% CI, and 0.1% to 27%) PFS: median 58.15 months (95% CI, 39.10 to N) OS: median 61.5 months (95% CI, 43.1 to N) and 2-year OS rate of 95% |
| Fenerty KE et al., 2016 [21] | 21 | Median age: 60 years (Range: 32–82) | Race: Not reported Ethnicity: Not reported | Yeast–Brachyury Vaccine (GI-6301), MVA–Brachyury–TRICOM Vaccine | Time to Progression (TTP) = good clinical outcome group with a longer TTP by volumetric assessment (p = 0.012, HR 0.21, and p = 0.02) and a poor clinical outcome group with a shorter TTP by volumetric assessment No significant difference in the TTP between groups when assessed by RECIST criteria (p = 0.37, HR 0.52, and p = 0.38) |
| Evaluation Parameters | Trials | |||
|---|---|---|---|---|
| Kesari S et al., 2024 [17] | Bavarian Nordic, 2023 [18] | Cote GM et al., 2018 [20] | Fenerty KE et al., 2016 [21] | |
| A clearly stated aim | 2 | 2 | 2 | 2 |
| Inclusion of consecutive patients | 1 | 1 | 2 | 1 |
| Prospective collection of data | 2 | 2 | 2 | 1 |
| Endpoints appropriate to the aim of the study | 2 | 2 | 2 | 2 |
| Unbiased assessment of the study endpoint | 1 | 1 | 2 | 1 |
| Follow-up period appropriate to the aim of the study | 2 | 1 | 2 | 2 |
| Loss to follow-up less than 5% | 1 | 0 | 2 | 1 |
| Prospective calculation of the study size | 1 | 2 | 1 | 0 |
| Scores | 12 | 10 | 15 | 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bangash, A.H.; Ryvlin, J.; Chakravarthy, V.; Akinduro, O.O.; Zadnik Sullivan, P.L.; Niu, T.; Galgano, M.A.; Shin, J.H.; Gokaslan, Z.L.; Fourman, M.S.; et al. Unmasking Racial, Ethnic, and Socioeconomic Disparities in United States Chordoma Clinical Trials: Systematic Review. Cancers 2025, 17, 225. https://doi.org/10.3390/cancers17020225
Bangash AH, Ryvlin J, Chakravarthy V, Akinduro OO, Zadnik Sullivan PL, Niu T, Galgano MA, Shin JH, Gokaslan ZL, Fourman MS, et al. Unmasking Racial, Ethnic, and Socioeconomic Disparities in United States Chordoma Clinical Trials: Systematic Review. Cancers. 2025; 17(2):225. https://doi.org/10.3390/cancers17020225
Chicago/Turabian StyleBangash, Ali Haider, Jessica Ryvlin, Vikram Chakravarthy, Oluwaseun O. Akinduro, Patricia L. Zadnik Sullivan, Tianyi Niu, Michael A. Galgano, John H. Shin, Ziya L. Gokaslan, Mitchell S. Fourman, and et al. 2025. "Unmasking Racial, Ethnic, and Socioeconomic Disparities in United States Chordoma Clinical Trials: Systematic Review" Cancers 17, no. 2: 225. https://doi.org/10.3390/cancers17020225
APA StyleBangash, A. H., Ryvlin, J., Chakravarthy, V., Akinduro, O. O., Zadnik Sullivan, P. L., Niu, T., Galgano, M. A., Shin, J. H., Gokaslan, Z. L., Fourman, M. S., Gelfand, Y., Murthy, S. G., Yassari, R., & De la Garza Ramos, R. (2025). Unmasking Racial, Ethnic, and Socioeconomic Disparities in United States Chordoma Clinical Trials: Systematic Review. Cancers, 17(2), 225. https://doi.org/10.3390/cancers17020225