
Storage Time and DNA Quality Determine BRCA1/2 Sequencing Success in Prostate Cancer: A Multicentre Analysis with Therapeutic Implications
 , , , , ,
, , , , ,  , ,
, ,  ,
,  , , ,
, , ,  , , ,
, , ,  , ,
, ,  , ,
, ,  and
and  add
Show full author list
add
Show full author list
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Tissue Samples
- •
- Short-term storage (<1 year; 223 biopsies [71.5%] and 89 surgical specimens [28.5%]);
- •
- Middle-term (1–2 years; 86 biopsies [61%] and 55 surgical specimens [39%]);
- •
- Long-term (>2 years; 250 biopsies [49.9%] and 251 surgical specimens [50.1%]).
2.2. Molecular Analysis
2.3. Statistical Analysis
3. Results
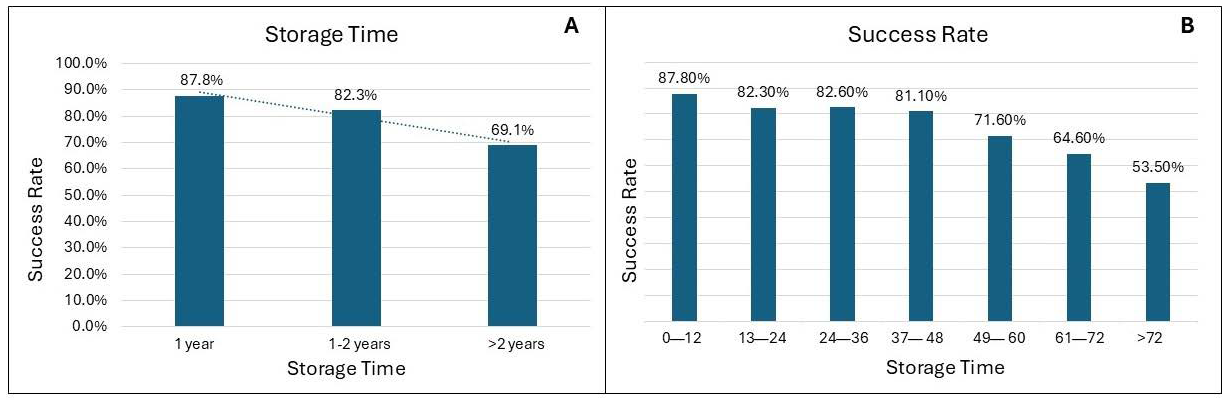
3.1. Success Rate and Storage Time
3.2. Success Rate and DNA Concentration and Fragmentation
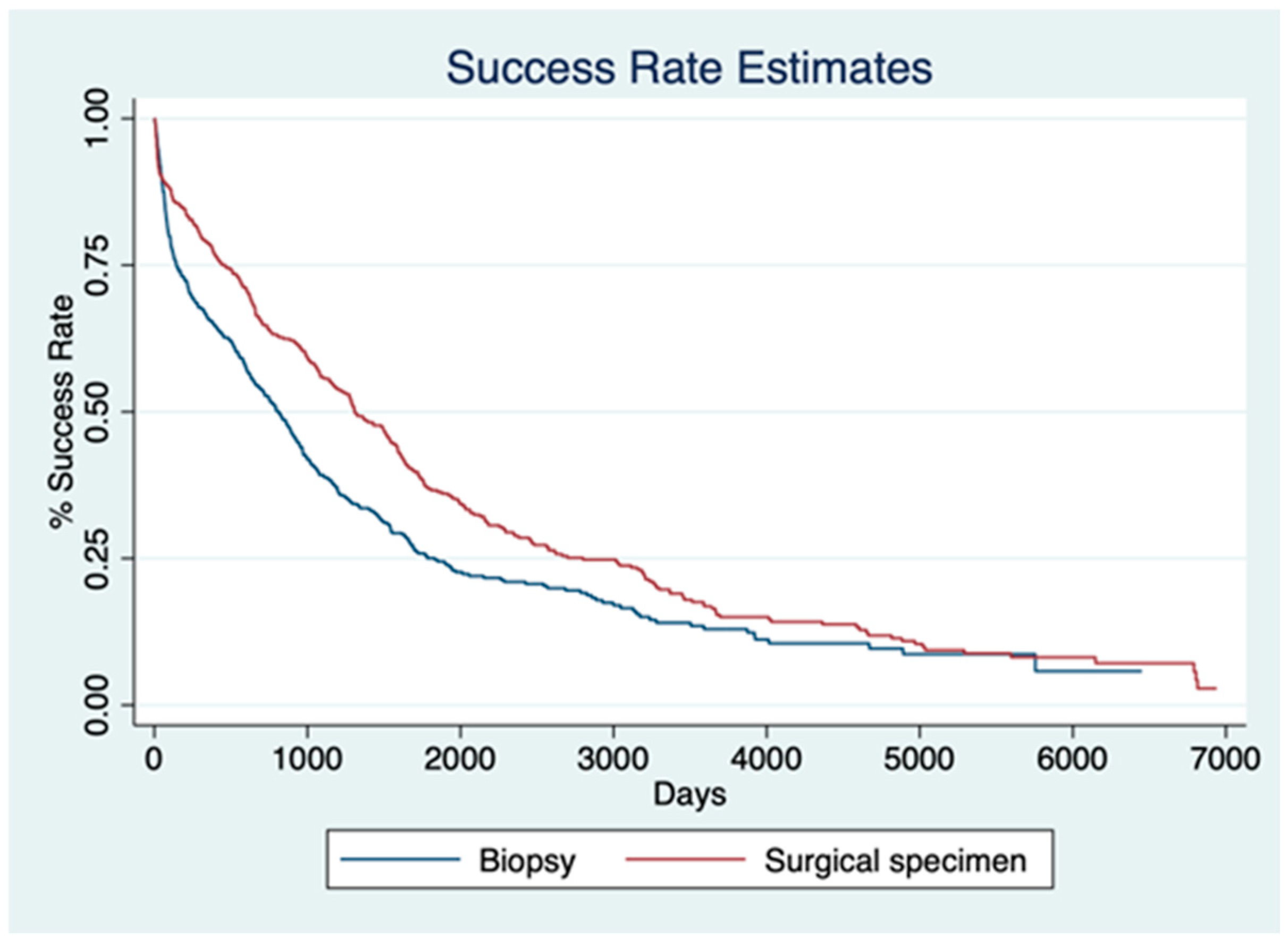
3.3. Success Rate and Type of Sample
3.4. Multivariate Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| NGS | Next-Generation Sequencing |
| PARP | Poly(ADP-ribose) Polymerase |
| BRCA | Breast Cancer Gene |
| FFPE | Formalin-Fixed Paraffin-Embedded |
References
- Wang, L.; Lu, B.; He, M.; Wang, Y.; Wang, Z.; Du, L. Prostate Cancer Incidence and Mortality: Global Status and Temporal Trends in 89 Countries From 2000 to 2019. Front. Public Health 2022, 10, 811044. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-Y.; Wang, P.-Y.; Liu, M.-Z.; Lyu, F.; Ma, M.-W.; Ren, X.-Y.; Gao, X.-S. Biomarkers for Prostate Cancer: From Diagnosis to Treatment. Diagnostics 2023, 13, 3350. [Google Scholar] [CrossRef]
- Tappero, S.; Piccinelli, M.L.; Incesu, R.-B.; Cano Garcia, C.; Barletta, F.; Morra, S.; Scheipner, L.; Baudo, A.; Tian, Z.; Parodi, S.; et al. Overall Survival of Metastatic Prostate Cancer Patients According to Location of Visceral Metastatic Sites. Clin. Genitourin. Cancer 2024, 22, 47–55.e2. [Google Scholar] [CrossRef] [PubMed]
- Akhoundova, D.; Francica, P.; Rottenberg, S.; Rubin, M.A. DNA Damage Response and Mismatch Repair Gene Defects in Advanced and Metastatic Prostate Cancer. Adv. Anat. Pathol. 2024, 31, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Rachmat, R.; Enyioma, S.; Ghose, A.; Revythis, A.; Boussios, S. BRCA Mutations in Prostate Cancer: Assessment, Implications and Treatment Considerations. Int. J. Mol. Sci. 2021, 22, 12628. [Google Scholar] [CrossRef]
- Paul, A.; Paul, S. The Breast Cancer Susceptibility Genes (BRCA) in Breast and Ovarian Cancers. Front. Biosci. Landmark Ed. 2014, 19, 605–618. [Google Scholar] [CrossRef]
- Giri, V.N.; Obeid, E.; Hegarty, S.E.; Gross, L.; Bealin, L.; Hyatt, C.; Fang, C.Y.; Leader, A. Understanding of Multigene Test Results among Males Undergoing Germline Testing for Inherited Prostate Cancer: Implications for Genetic Counseling. Prostate 2018, 78, 879–888. [Google Scholar] [CrossRef]
- Valsecchi, A.A.; Dionisio, R.; Panepinto, O.; Paparo, J.; Palicelli, A.; Vignani, F.; Di Maio, M. Frequency of Germline and Somatic BRCA1 and BRCA2 Mutations in Prostate Cancer: An Updated Systematic Review and Meta-Analysis. Cancers 2023, 15, 2435. [Google Scholar] [CrossRef]
- Zannini, G.; Facchini, G.; De Sio, M.; De Vita, F.; Ronchi, A.; Orditura, M.; Vietri, M.T.; Ciardiello, F.; Franco, R.; Accardo, M.; et al. Implementation of BRCA Mutations Testing in Formalin-Fixed Paraffin-Embedded (FFPE) Samples of Different Cancer Types. Pathol. Res. Pract. 2023, 243, 154336. [Google Scholar] [CrossRef]
- de Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2091–2102. [Google Scholar] [CrossRef]
- Mateo, J.; Carreira, S.; Sandhu, S.; Miranda, S.; Mossop, H.; Perez-Lopez, R.; Nava Rodrigues, D.; Robinson, D.; Omlin, A.; Tunariu, N.; et al. DNA-Repair Defects and Olaparib in Metastatic Prostate Cancer. N. Engl. J. Med. 2015, 373, 1697–1708. [Google Scholar] [CrossRef] [PubMed]
- McNevin, C.S.; Cadoo, K.; Baird, A.-M.; Finn, S.P.; McDermott, R. PARP Inhibitors in Advanced Prostate Cancer in Tumors with DNA Damage Signatures. Cancers 2022, 14, 4751. [Google Scholar] [CrossRef] [PubMed]
- Ferriero, M.; Prata, F.; Mastroianni, R.; De Nunzio, C.; Tema, G.; Tuderti, G.; Bove, A.M.; Anceschi, U.; Brassetti, A.; Misuraca, L.; et al. The Impact of Locoregional Treatments for Metastatic Castration Resistant Prostate Cancer on Disease Progression: Real Life Experience from a Multicenter Cohort. Prostate Cancer Prostatic Dis. 2024, 27, 89–94. [Google Scholar] [CrossRef]
- Tuffaha, H.; Edmunds, K.; Fairbairn, D.; Roberts, M.J.; Chambers, S.; Smith, D.P.; Horvath, L.; Arora, S.; Scuffham, P. Guidelines for Genetic Testing in Prostate Cancer: A Scoping Review. Prostate Cancer Prostatic Dis. 2024, 27, 594–603. [Google Scholar] [CrossRef] [PubMed]
- Pommier, Y.; O’Connor, M.J.; de Bono, J. Laying a Trap to Kill Cancer Cells: PARP Inhibitors and Their Mechanisms of Action. Sci. Transl. Med. 2016, 8, 362ps17. [Google Scholar] [CrossRef]
- Mafficini, A.; Simbolo, M.; Parisi, A.; Rusev, B.; Luchini, C.; Cataldo, I.; Piazzola, E.; Sperandio, N.; Turri, G.; Franchi, M.; et al. BRCA Somatic and Germline Mutation Detection in Paraffin Embedded Ovarian Cancers by Next-Generation Sequencing. Oncotarget 2016, 7, 1076. [Google Scholar] [CrossRef]
- Zannini, G.; Facchini, G.; De Sio, M.; De Vita, F.; Pagliuca, F.; Franco, R.; Zito Marino, F. BRCA1 and BRCA2 Mutations Testing in Prostate Cancer: Detection in Formalin Fixed Paraffin Embedded (FFPE) and Blood Samples. Pathol. Res. Pract. 2025, 266, 155803. [Google Scholar] [CrossRef]
- Hussain, M.; Corcoran, C.; Sibilla, C.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Mateo, J.; Olmos, D.; Mehra, N.; et al. Tumor Genomic Testing for >4000 Men with Metastatic Castration-Resistant Prostate Cancer in the Phase III Trial PROfound (Olaparib). Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2022, 28, 1518–1530. [Google Scholar] [CrossRef]
- Giannini, C.; Oelkers, M.M.; Edwards, W.D.; Aubry, M.C.; Muncil, M.M.; Mohamud, K.H.; Sandleback, S.G.; Nowak, J.M.; Bridgeman, A.; Brown, M.E.; et al. Maintaining Clinical Tissue Archives and Supporting Human Research: Challenges and Solutions. Arch. Pathol. Lab. Med. 2011, 135, 347–353. [Google Scholar] [CrossRef]
- Tommasi, S.; Coppola, C.A.; Caniglia, A.; Pilato, B.; Zito, F.A.; Carosi, M.; Melucci, E.; Casini, B.; Russo, A.; Gismondi, V.; et al. BRCA Testing in Metastatic Castration-Resistant Prostate Cancer: Successes and Troubles in a Real World Setting. An Italian Multicentric Study. Pathol.—J. Ital. Soc. Anat. Pathol. Diagn. Cytopathol. 2024, 116, 303–309. [Google Scholar] [CrossRef]
- Rehm, H.L.; Bale, S.J.; Bayrak-Toydemir, P.; Berg, J.S.; Brown, K.K.; Deignan, J.L.; Friez, M.J.; Funke, B.H.; Hegde, M.R.; Lyon, E. ACMG Clinical Laboratory Standards for Next-Generation Sequencing. Genet. Med. 2013, 15, 733–747. [Google Scholar] [CrossRef]
- Hiemenz, M.C.; Graf, R.P.; Schiavone, K.; Harries, L.; Oxnard, G.R.; Ross, J.S.; Huang, R.S.P. Real-World Comprehensive Genomic Profiling Success Rates in Tissue and Liquid Prostate Carcinoma Specimens. Oncologist 2022, 27, e970. [Google Scholar] [CrossRef]
- Eccher, A.; Seminati, D.; L’Imperio, V.; Casati, G.; Pilla, D.; Malapelle, U.; Piga, I.; Bindi, G.; Marando, A.; Bonoldi, E.; et al. Pathology Laboratory Archives: Conservation Quality of Nucleic Acids and Proteins for NSCLC Molecular Testing. J. Pers. Med. 2024, 14, 333. [Google Scholar] [CrossRef]
- Gonzalez, D.; Mateo, J.; Stenzinger, A.; Rojo, F.; Shiller, M.; Wyatt, A.W.; Penault-Llorca, F.; Gomella, L.G.; Eeles, R.; Bjartell, A. Practical Considerations for Optimising Homologous Recombination Repair Mutation Testing in Patients with Metastatic Prostate Cancer. J. Pathol. Clin. Res. 2021, 7, 311–325. [Google Scholar] [CrossRef]
- Wallace, A.J. New Challenges for BRCA Testing: A View from the Diagnostic Laboratory. Eur. J. Hum. Genet. 2016, 24, S10–S18. [Google Scholar] [CrossRef]
- Capoluongo, E.; Ellison, G.; López-Guerrero, J.A.; Penault-Llorca, F.; Ligtenberg, M.J.L.; Banerjee, S.; Singer, C.; Friedman, E.; Markiefka, B.; Schirmacher, P.; et al. Guidance Statement On BRCA1/2 Tumor Testing in Ovarian Cancer Patients. Semin. Oncol. 2017, 44, 187–197. [Google Scholar] [CrossRef]
- Castro, E.; Romero-Laorden, N.; Del Pozo, A.; Lozano, R.; Medina, A.; Puente, J.; Piulats, J.M.; Lorente, D.; Saez, M.I.; Morales-Barrera, R.; et al. PROREPAIR-B: A Prospective Cohort Study of the Impact of Germline DNA Repair Mutations on the Outcomes of Patients With Metastatic Castration-Resistant Prostate Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 490–503. [Google Scholar] [CrossRef]
- Leith, A.; Ribbands, A.; Kim, J.; Last, M.; Barlow, S.; Yang, L.; Ghate, S.R. Real-World Homologous Recombination Repair Mutation Testing in Metastatic Castration-Resistant Prostate Cancer in the USA, Europe and Japan. Future Oncol. Lond. Engl. 2022, 18, 937–951. [Google Scholar] [CrossRef]
- Fan, Y.; Liu, Z.; Chen, Y.; He, Z. Homologous Recombination Repair Gene Mutations in Prostate Cancer: Prevalence and Clinical Value. Adv. Ther. 2024, 41, 2196–2216. [Google Scholar] [CrossRef] [PubMed]
- Scott, R.J.; Mehta, A.; Macedo, G.S.; Borisov, P.S.; Kanesvaran, R.; Metnawy, W.E. Genetic Testing for Homologous Recombination Repair (HRR) in Metastatic Castration-Resistant Prostate Cancer (mCRPC): Challenges and Solutions. Oncotarget 2021, 12, 1600–1614. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome of Analysis | Biopsies | Surgical Specimens |
|---|---|---|
| Failed | 152/559 (27.2%) | 66/395 (16.7%) |
| Successful | 407/559 (72.8%) | 329/395 (83.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vescovo, M.; Raspollini, M.R.; Nibid, L.; Castiglione, F.; Nardi, E.; de Biase, D.; Massari, F.; Giunchi, F.; Pepe, F.; Troncone, G.; et al. Storage Time and DNA Quality Determine BRCA1/2 Sequencing Success in Prostate Cancer: A Multicentre Analysis with Therapeutic Implications. Cancers 2025, 17, 1705. https://doi.org/10.3390/cancers17101705
Vescovo M, Raspollini MR, Nibid L, Castiglione F, Nardi E, de Biase D, Massari F, Giunchi F, Pepe F, Troncone G, et al. Storage Time and DNA Quality Determine BRCA1/2 Sequencing Success in Prostate Cancer: A Multicentre Analysis with Therapeutic Implications. Cancers. 2025; 17(10):1705. https://doi.org/10.3390/cancers17101705
Chicago/Turabian StyleVescovo, Mariavittoria, Maria Rosaria Raspollini, Lorenzo Nibid, Francesca Castiglione, Eleonora Nardi, Dario de Biase, Francesco Massari, Francesca Giunchi, Francesco Pepe, Giancarlo Troncone, and et al. 2025. "Storage Time and DNA Quality Determine BRCA1/2 Sequencing Success in Prostate Cancer: A Multicentre Analysis with Therapeutic Implications" Cancers 17, no. 10: 1705. https://doi.org/10.3390/cancers17101705
APA StyleVescovo, M., Raspollini, M. R., Nibid, L., Castiglione, F., Nardi, E., de Biase, D., Massari, F., Giunchi, F., Pepe, F., Troncone, G., Malapelle, U., Carosi, M., Casini, B., Melucci, E., Fassan, M., Toffolatti, L., Guerini-Rocco, E., Conversano, F., Rappa, A., ... Perrone, G. (2025). Storage Time and DNA Quality Determine BRCA1/2 Sequencing Success in Prostate Cancer: A Multicentre Analysis with Therapeutic Implications. Cancers, 17(10), 1705. https://doi.org/10.3390/cancers17101705