
A Two-Stage Phase 2, Multicenter, Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Safety and Efficacy of Ec-18 in Altering the Severity and Course of Oral Mucositis Secondary to Chemoradiation Therapy for Squamous Cell Cancers of the Head and Neck

 , ,
, ,  , , , , and
, , , , and 
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
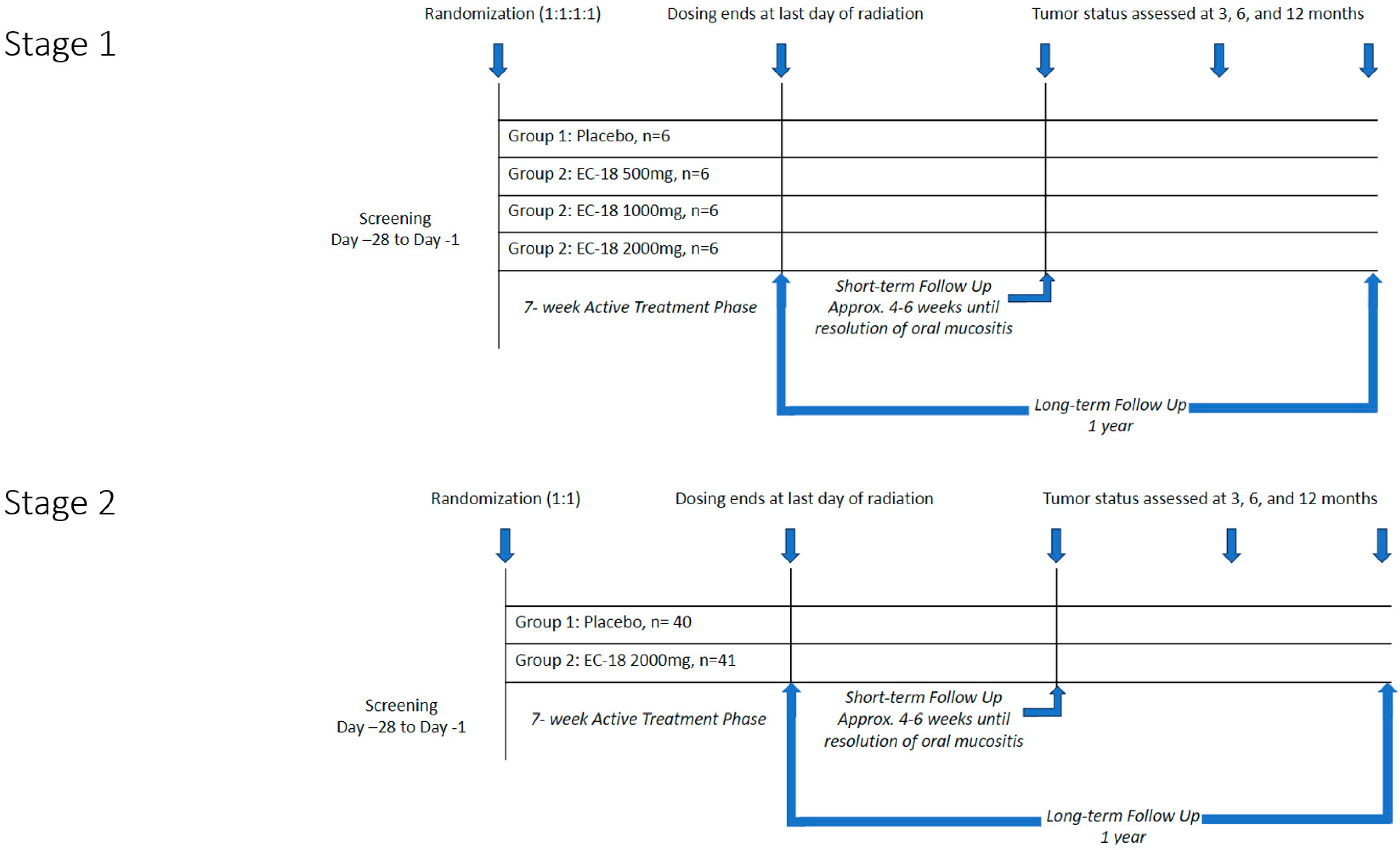
2.1. Study Design
2.2. Study Participants
2.3. Treatment and Assessments
2.4. Endpoints and Statistical Methods
3. Results
3.1. Patient Characteristics
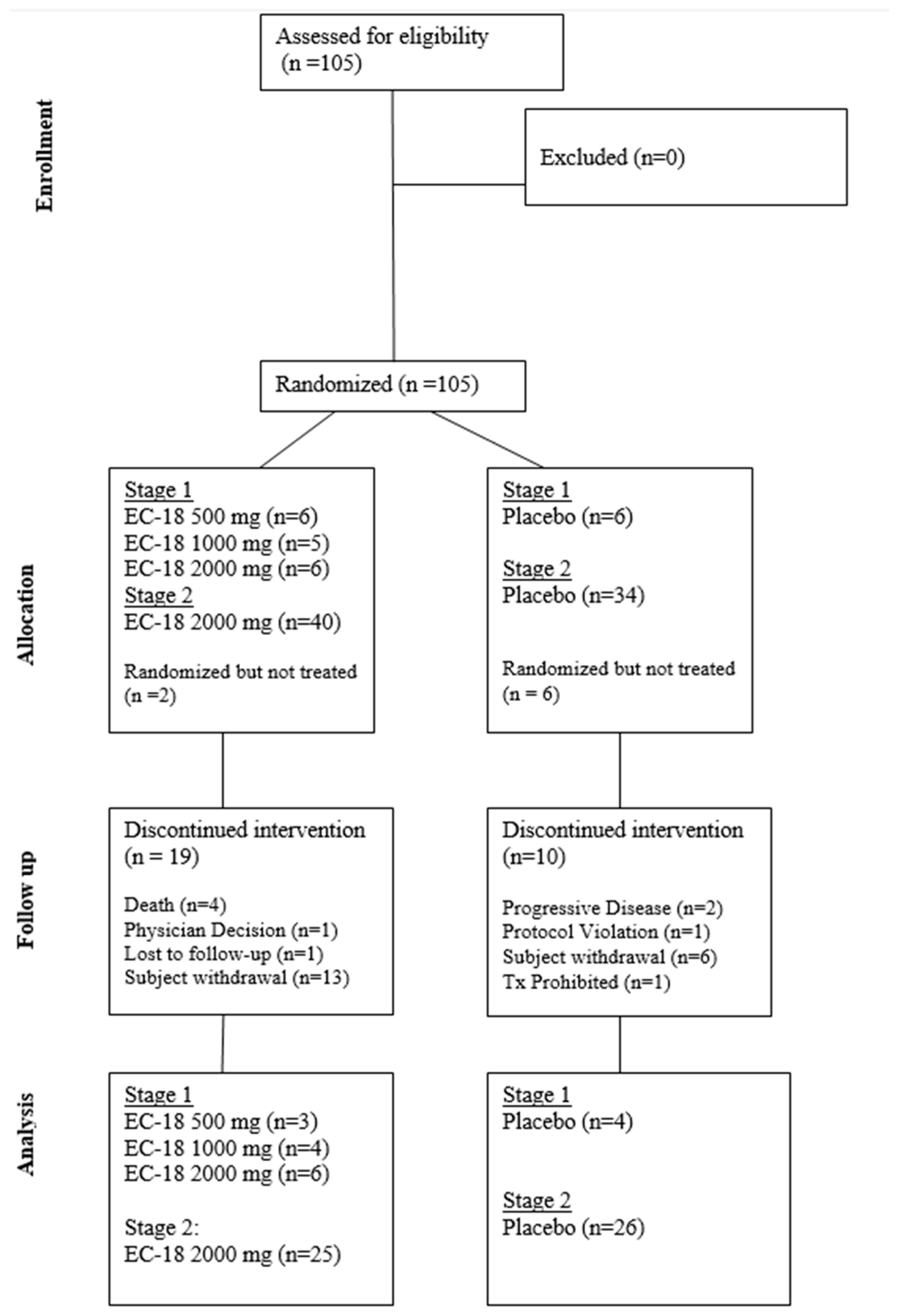
3.2. Compliance
3.3. Efficacy Analysis
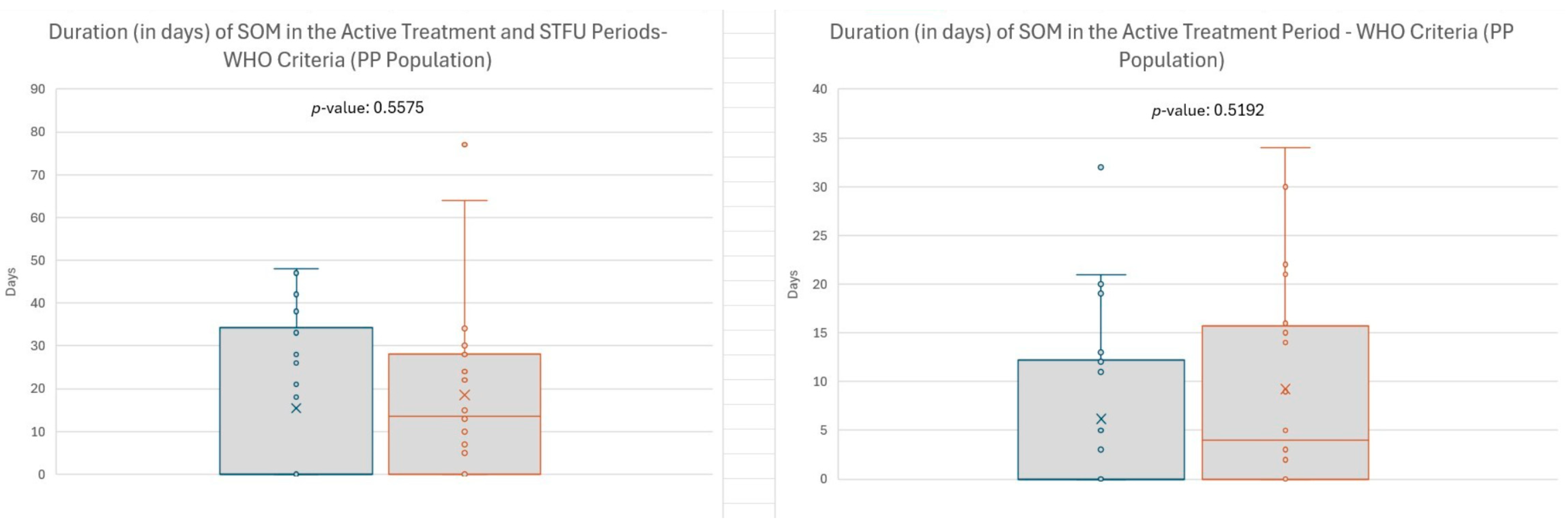
3.3.1. Duration of SOM Among All Patients in the per Protocol Cohort
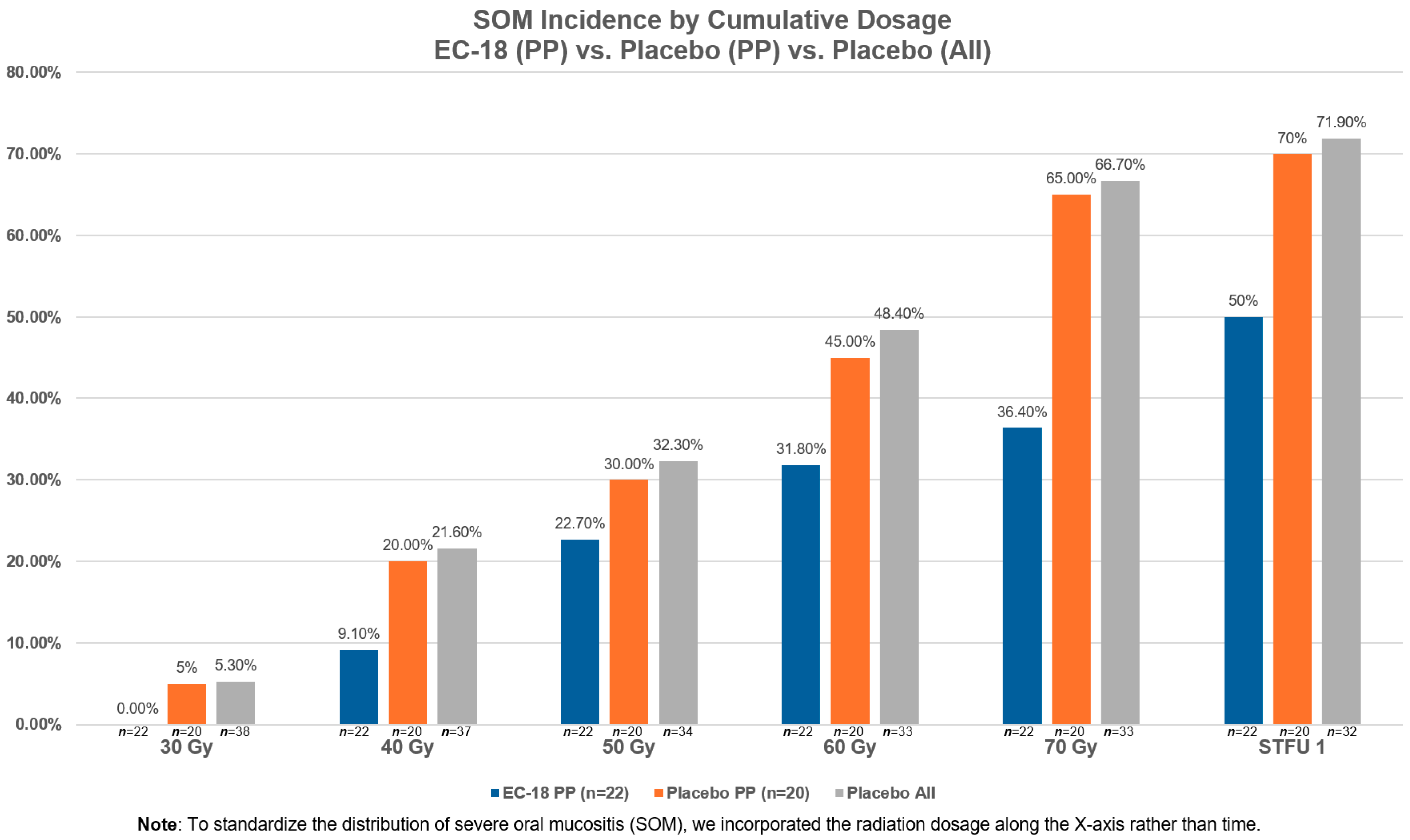
3.3.2. Incidence of SOM
3.3.3. Opioid Analgesic Use to Control Oral Pain
3.3.4. OMDQ and FACT-HN Assessments
3.4. Safety (Adverse Events)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AE | Adverse event |
| CMH | Cochran–Mantel–Haenszel |
| CRT | Chemoradiation therapy |
| FACT-HN | Functional Assessment of Cancer Therapy for Subjects with Head & Neck Cancer |
| HNC | Head and neck cancer |
| OM | Oral mucositis |
| OMDQ | Oral Mucositis Daily Questionnaire |
| LTFU | Long-term follow-up |
| NC | Non-compliant |
| PT | Preferred Term |
| RTQA | Radiation Therapy Quality Assurance |
| SAE | Severe adverse event |
| SOM | Severe oral mucositis |
| STFU | Short-term follow-up |
| TEAE | Treatment-emergent AEs |
| WHO | World Health Organization |
References
- Anderson, C.; Saunders, D. Oral Mucositis in Head and Neck Cancer Patients. Semin. Radiat. Oncol. 2025, 35, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, C.; Bohm, N.; Andersson, J.S.; Finizia, C.; Almståhl, A. Prospective study on health-related quality of life, oral mucositis and oral health on during treatment of head and neck cancer. BMC Oral Health 2024, 24, 697. [Google Scholar] [CrossRef]
- Elad, S.; Yarom, N.; Zadik, Y.; Kuten-Shorrer, M.; Sonis, S.T. The broadening scope of oral mucositis and oral ulcerative mucosal toxicities of anticancer therapies. CA Cancer J. Clin. 2022, 72, 57–77. [Google Scholar] [CrossRef] [PubMed]
- Elting, L.S.; Chang, Y.C. Costs of Oral Complications of Cancer Therapies: Estimates and a Blueprint fo Future Study. J. Natl. Cancer Inst. Monogr. 2019, 2019, lgz010. [Google Scholar] [CrossRef] [PubMed]
- Mohan, M.P.; Pili, R.; Epstein, J.B.; Rudin, L.; Eichhorn, S.; Satheeshkumar, P.S. Cancer treatment-induced ulcerative mucositis serves as a significant predictor of burden of illness including dysphagia, and associated disparities among hospitalized cancer patients. Support. Care Cancer 2024, 33, 22. [Google Scholar] [CrossRef] [PubMed]
- Iovoli, A.J.; Turecki, L.; Qiu, M.L.; Khan, M.; Smith, K.; Yu, H.; Ma, S.J.; Farrugia, M.K.; Singh, A.K. Severe Oral Mucositis After Intensity-Modulated Radiation Therapy for Head and Neck Cancer. JAMA Netw. Open 2023, 6, e2337265. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rosenthal, D.I. Consequences of mucositis-induced treatment breaks and dose reductions on head and neck cancer treatment outcomes. J. Support. Oncol. 2007, 5 (Suppl. 4), 23–31. [Google Scholar] [PubMed]
- Russo, G.; Haddad, R.; Posner, M.; Machtay, M. Radiation treatment breaks and ulcerative mucositis in head and neck cancer. Oncologist 2008, 13, 886–898. [Google Scholar] [CrossRef]
- Villa, A.; Sonis, S.T. Radiotherapy-induced severe oral mucositis: Pharmacotherapies in recent and current clinical trials. Expert. Opin. Investig. Drugs 2023, 32, 301–310. [Google Scholar] [CrossRef]
- Gobbo, M.; Joy, J.; Guedes, H.; Shazib, M.A.; Anderson, C.; Abdalla-Aslan, R.; Peechatanan, K.; Lajolo, C.; Nasir, K.S.; Gueiros, L.A.; et al. Emerging pharmacotherapy trends in preventing and managing oral mucositis induced by chemoradiotherapy and targeted agents. Expert Opin. Pharmacother. 2024, 25, 727–742. [Google Scholar] [CrossRef]
- Henson, C.; Clayburgh, D.; Lee, A.S.; Wong, D.J.; Kudrimoti, M.R.; Adkins, D.; Lee, S.P.; Kalman, N.; Oppelt, P.J.; Rao, K.A.; et al. Phase 2, randomized, double-blind trial of EC-18 versus placebo to mitigate the development and time course of oral mucositis from concomitant chemoradiation for head and neck cancer. J. Clin. Oncol. 2022, 40 (Suppl. 16), 12106. [Google Scholar] [CrossRef]
- Chen, C.; Zhang, Q.; Yu, W.; Chang, B.; Le, A.D. Oral Mucositis: An Update on Innate Immunity and New Interventional Targets. J. Dent. Res. 2020, 99, 1122–1130. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bowen, J.; Cross, C. The Role of the Innate Immune Response in Oral Mucositis Pathogenesis. Int. J. Mol. Sci. 2023, 24, 16314. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Choi, S.; Shin, S.H.; Lee, H.R.; Sohn, K.Y.; Yoon, S.Y.; Kim, J.W. 1-Palmitoyl-2-linoleoyl-3-acetyl-rac-glycerol ameliorates chemoradi-ation-induced oral mucositis. Oral. Dis. 2020, 26, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.R.; Shin, S.H.; Kim, J.H.; Sohn, K.Y.; Yoon, S.Y.; Kim, J.W. 1-Palmitoyl-2-Linoleoyl-3-Acetyl-rac-Glycerol (PLAG) Rapidly Re-solves LPS-Induced Acute Lung Injury Through the Effective Control of Neutrophil Recruitment. Front. Immunol. 2019, 10, 2177. [Google Scholar] [CrossRef]
- Study to Evaluate the Safety, Tolerability, and PK of EC-18 After Oral Administration in Healthy Volunteers. Available online: https://www.ngram.com/trials/NCT02532712#record-history (accessed on 27 January 2016).
- Villa, A.; Vollemans, M.; De Moraes, A.; Sonis, S. Concordance of the WHO, RTOG, and CTCAE v4.0 grading scales for the evaluation of oral mucositis associated with chemoradiation therapy for the treatment of oral and oropharyngeal cancers. Support. Care Cancer 2021, 29, 6061–6068. [Google Scholar] [CrossRef] [PubMed]
- Huynh-Dagher, S.; Duong, T.A.; Tournigand, C.; Kempf, E.; Lame, G. Concordance between patient-reported outcomes and CTCAE clinician-reported toxicities during outpatient chemotherapy courses: A retrospective cohort study in routine care. ESMO Real World Data Digit. Oncol. 2025, 8, 100127. [Google Scholar] [CrossRef]
- Stiff, P.J.; Erder, H.; Bensinger, W.I.; Emmanouilides, C.; Gentile, T.; Isitt, J.; Lu, Z.J.; Spielberger, R. Reliability and validity of a patient self-administered daily questionnaire to assess impact of oral mucositis (OM) on pain and daily functioning in patients undergoing autologous hematopoietic stem cell transplantation (HSCT). Bone Marrow Transpl. 2006, 37, 393–401. [Google Scholar] [CrossRef]
- List, M.A.; D’Antonio, L.L.; Cella, D.F.; Siston, A.; Mumby, P.; Haraf, D.; Vokes, E. The Performance Status Scale for Head and Neck Cancer Patients and the Functional Assessment of Cancer Therapy-Head and Neck Scale. A study of utility and validity. Cancer 1996, 77, 2294–2301. [Google Scholar] [CrossRef]
- Jin, Y.; Wang, J.; Wang, Y. Unraveling the complexity of radiotherapy- and chemotherapy-induced oral mucositis: Insights into pathogenesis and intervention strategies. Support. Care Cancer 2025, 33, 195. [Google Scholar] [CrossRef] [PubMed]
- Pang, H.; Li, S.; Fu, X.; Wen, S.; Chen, D.; Sun, X.; Chen, Y.; Yang, S. Effect of blood oxidative stress indicators on oral mucositis in patients undergoing radiotherapy for nasopharyngeal carcinoma. Eur. J. Med. Res. 2024, 29, 573. [Google Scholar] [CrossRef]
- Oronsky, B.; Takahashi, L.; Gordon, R.; Cabrales, P.; Caroen, S.; Reid, T. RRx-001: A chimeric triple action NLRP3 inhibitor, Nrf2 inducer, and nitric oxide superagonist. Front. Oncol. 2023, 13, 1204143. [Google Scholar] [CrossRef]
- Goel, G.; Alice, K.P.; Negi, P.; Aggarwal, N. Factors influencing radiation induced oral mucositis in head and neck cancer. J. Cancer Res. Ther. 2024, 20, 1564–1569. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.R.; Yoo, N.; Kim, J.H.; Sohn, K.Y.; Kim, H.J.; Kim, M.H.; Han, M.Y.; Yoon, S.Y.; Kim, J.W. The Therapeutic Effect of PLAG against Oral Mucositis in Hamster and Mouse Model. Front. Oncol. 2016, 6, 209. [Google Scholar] [CrossRef]
- Shin, I.S.; Ahn, K.S.; Shin, N.R.; Lee, H.J.; Ryu, H.W.; Kim, J.W.; Sohn, K.Y.; Kim, H.J.; Han, Y.H.; Oh, S.R. Protective effect of EC-18, a synthetic monoacetyldiglyceride on lung inflammation in a murine model induced by cigarette smoke and lipopolysaccharide. Int. Immunopharmacol. 2016, 30, 62–68. [Google Scholar] [CrossRef]
- Kim, Y.J.; Shin, J.M.; Shin, S.H.; Kim, J.H.; Sohn, K.Y.; Kim, H.J.; Kang, J.K.; Yoon, S.Y.; Kim, J.W. 1-palmitoyl-2-linoleoyl-3-acetyl-rac-glycerol ameliorates arthritic joints through reducing neutrophil infiltration mediated by IL-6/STAT3 and MIP-2 activation. Oncotarget 2017, 8, 96636–96648. [Google Scholar] [CrossRef]
- Kim, G.T.; Lee, D.Y.; Sohn, K.Y.; Yoon, S.Y.; Kim, J.W. PLAG enhances macrophage mobility for efferocytosis of active neutrophils via membrane redistribution of P2Y2. Cancer Res. 2019, 79 (Suppl. 13), 5016–5029. [Google Scholar]
- Sathian, B.; Asim, M.; Banerjee, I.; Pizarro, A.B.; Roy, B.; van Teijlingen, E.R.; do Nascimento, I.J.B.; Alhamad, H.K. Impact of COVID-19 on clinical trials and clinical research: A systematic review. Nepal. J. Epidemiol. 2020, 10, 878–887. [Google Scholar] [CrossRef]
- Singh, V.; Garg, S.; Klimek, M.; Sinha, R.R.; Dhanwal, D. COVID-19 and Clinical Trials: Current Challenges and Future Directions. Rev. Recent Clin. Trials 2021, 16, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Asaad, M.; Habibullah, N.K.; Butler, C.E. The Impact of COVID-19 on Clinical Trials. Ann. Surg. 2020, 272, e222–e223. [Google Scholar] [CrossRef]
- Ali, J.K.; Riches, J.C. The Impact of the COVID-19 Pandemic on Oncology Care and Clinical Trials. Cancers 2021, 13, 5924. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Kato, S.; Kurzrock, R. The Impact of COVID-19 on Cancer Clinical Trials Conducted by NCI-Designated Compre-hensive Cancer Centers. J. Immunother. Precis. Oncol. 2021, 4, 56–63. [Google Scholar] [CrossRef]
- Anderson, C.M.; Lee, C.M.; Saunders, D.P.; Curtis, A.; Dunlap, N.; Nangia, C.; Lee, A.S.; Gordon, S.M.; Kovoor, P.; Arevalo-Araujo, R.; et al. Phase IIb, Randomized, Double-Blind Trial of GC4419 Versus Placebo to Reduce Severe Oral Mucositis Due to Concurrent Radiotherapy and Cisplatin For Head and Neck Cancer. J. Clin. Oncol. 2019, 37, 3256–3265. [Google Scholar] [CrossRef] [PubMed]
- Jacinto, J.K.; Co, J.; Mejia, M.B.; Regala, E.E. The evidence on effectiveness of weekly vs triweekly cisplatin concurrent with radiotherapy in locally advanced head and neck squamous cell carcinoma (HNSCC): A systematic review and meta-analysis. Br. J. Radiol. 2017, 90, 20170442. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Szturz, P.; Wouters, K.; Kiyota, N.; Tahara, M.; Prabhash, K.; Noronha, V.; Castro, A.; Licitra, L.; Adelstein, D.; Vermorken, J.B. Weekly Low-Dose Versus Three-Weekly High-Dose Cisplatin for Concurrent Chemoradiation in Locoregionally Advanced Non-Nasopharyngeal Head and Neck Cancer: A Systematic Review and Meta-Analysis of Aggreg ate Data. Oncologist 2017, 22, 1056–1066. [Google Scholar] [CrossRef]
- Zoschke, I.N.; Bennis, S.L.; Tang, Y.; Wilkerson, J.M.; Stull, C.L.; Nyitray, A.G.; Khariwala, S.S.; Nichols, C.M.; Rosser, B.R.S.; Flash, C.A.; et al. The influence of tobacco use, hazardous drinking, and other risk factors on HPV-associated oropharyngeal cancer risk and screening perceptions among gay and bisexual men: A cross-sectional study. BMC Oral Health 2025, 25, 462. [Google Scholar] [CrossRef]
- Vani, N.V.; Rama, R.; Madhanagopal, R.; Vijayalakshmi, R.; Swaminathan, R. Human Papillomavirus-Attributable Head and Neck Cancers in India-A Systematic Review and Meta-Analysis. JCO Glob. Oncol. 2024, 10, e2300464. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Period | STFU | Active Treatment | ||||||
|---|---|---|---|---|---|---|---|---|
|
Incidence of SOM (Grades 3 and 4) [n (%)] |
EC-18 2000 mg (n = 22) |
Placebo (n= 20) |
Non-PP EC-18 (n = 14) | All Placebo (n = 32) |
EC-18 2000 mg (n = 22) |
Placebo (n = 20) |
Non-PP EC-18 (n = 14) | All Placebo (n = 32) |
| Incidence of SOM | 10 (45.5) | 14 (70.0) | 12 (85.7) | 22 (68.8) | 9 (40.9) | 13 (65.0) | 12 (85.7) | 21 (65.6) |
| 95% Confidence Interval a | (26.9, 65.3) | (48.1, 85.5) | (23.3, 61.3) | (43.3, 81.9) | ||||
| CMH Test p-value b | 0.1894 | 0.2953 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henson, C.; Clayburgh, D.; Lee, A.; Wong, D.; Kudrimoti, M.; Lee, S.; Kalman, N.; Rao, K.; Sohn, K.Y.; Crawford, J.; et al. A Two-Stage Phase 2, Multicenter, Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Safety and Efficacy of Ec-18 in Altering the Severity and Course of Oral Mucositis Secondary to Chemoradiation Therapy for Squamous Cell Cancers of the Head and Neck. Cancers 2025, 17, 1663. https://doi.org/10.3390/cancers17101663
Henson C, Clayburgh D, Lee A, Wong D, Kudrimoti M, Lee S, Kalman N, Rao K, Sohn KY, Crawford J, et al. A Two-Stage Phase 2, Multicenter, Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Safety and Efficacy of Ec-18 in Altering the Severity and Course of Oral Mucositis Secondary to Chemoradiation Therapy for Squamous Cell Cancers of the Head and Neck. Cancers. 2025; 17(10):1663. https://doi.org/10.3390/cancers17101663
Chicago/Turabian StyleHenson, Christina, Daniel Clayburgh, Arielle Lee, Deborah Wong, Mahesh Kudrimoti, Steve Lee, Noah Kalman, Krishna Rao, Ki Young Sohn, Jeffrey Crawford, and et al. 2025. "A Two-Stage Phase 2, Multicenter, Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Safety and Efficacy of Ec-18 in Altering the Severity and Course of Oral Mucositis Secondary to Chemoradiation Therapy for Squamous Cell Cancers of the Head and Neck" Cancers 17, no. 10: 1663. https://doi.org/10.3390/cancers17101663
APA StyleHenson, C., Clayburgh, D., Lee, A., Wong, D., Kudrimoti, M., Lee, S., Kalman, N., Rao, K., Sohn, K. Y., Crawford, J., Villa, A., & Sonis, S. (2025). A Two-Stage Phase 2, Multicenter, Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Safety and Efficacy of Ec-18 in Altering the Severity and Course of Oral Mucositis Secondary to Chemoradiation Therapy for Squamous Cell Cancers of the Head and Neck. Cancers, 17(10), 1663. https://doi.org/10.3390/cancers17101663