

Systematic Review and Meta-Analysis of Laparoscopic versus Robotic-Assisted Surgery for Colon Cancer: Efficacy, Safety, and Outcomes—A Focus on Studies from 2020–2024


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
- Study types: peer-reviewed randomized controlled trials and cohort studies;
- Population: adult patients (aged 18 and older) diagnosed with colon cancer at any stage;
- Interventions: studies comparing laparoscopic and robotic surgical techniques used specifically for colon cancer resections;
- Outcomes: Studies must report at least one of the following outcomes: operative time, hospital stay, conversion rates, anastomotic leak rates, or harvested lymph nodes.
- Non-comparative studies;
- Cadaveric or animal studies;
- Irrelevant conditions (other types of cancer or non-oncological surgeries);
- Language restrictions;
- Incomplete data (missing outcome data relevant to the primary endpoints of this review).
2.1. Search Strategy
2.2. Study Selection
- Wrong publication type (review, meta-analysis);
- Focusing on other diseases (rectal cancer, hepatic pathology, urologic-gynecologic pathology, gastric cancer, NOSES—natural orifice specimen extraction site, endometriosis, etc.);
- Restricted access;
- Animal or cadaveric study;
- Foreign language;
- No relevant data;
- Missing data.
2.3. Data Extraction
2.4. Assessment
2.5. Statistical Analysis
3. Results
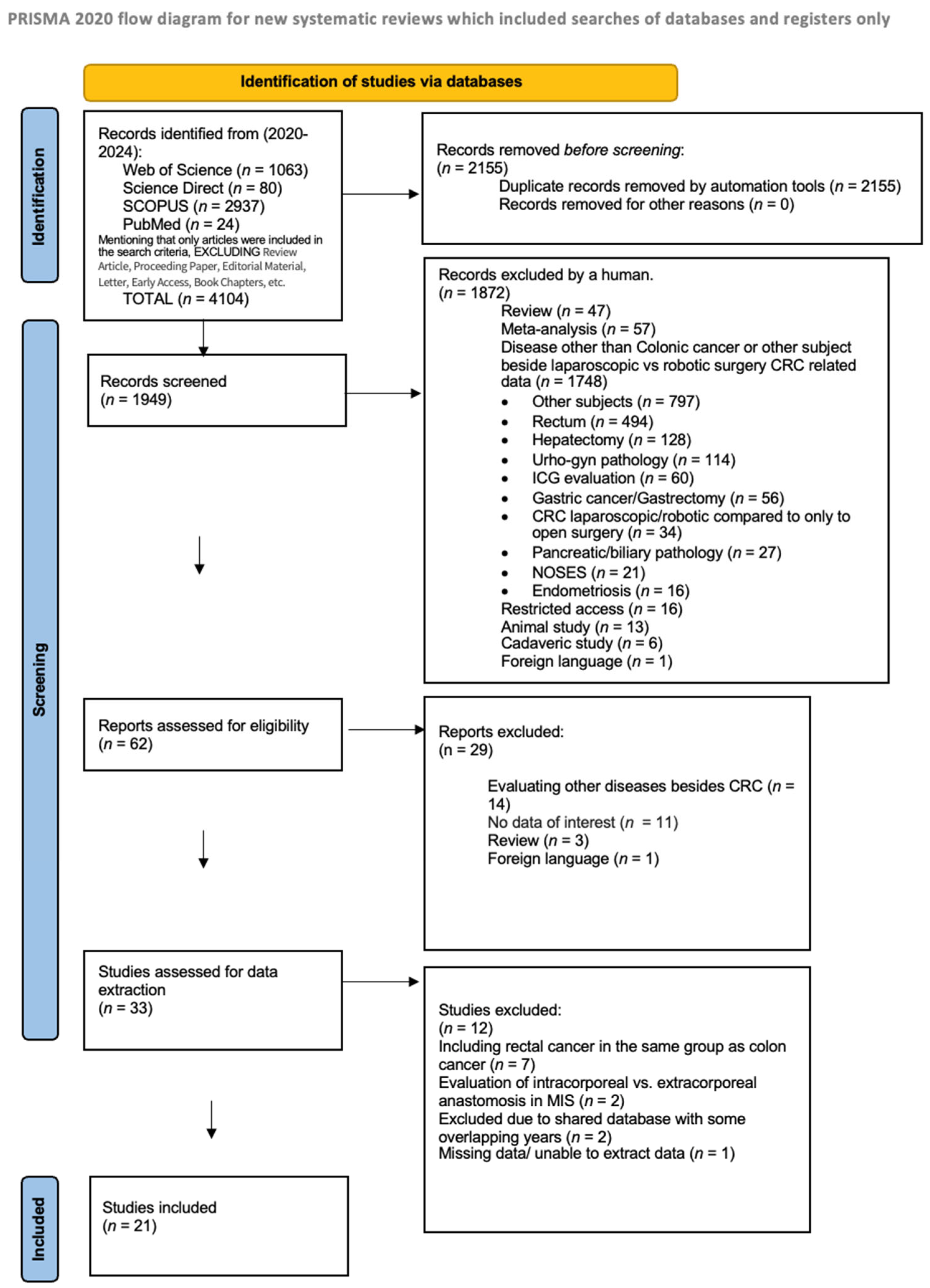
3.1. Study Selection
3.2. Risk of Bias
3.3. Studies Characteristics
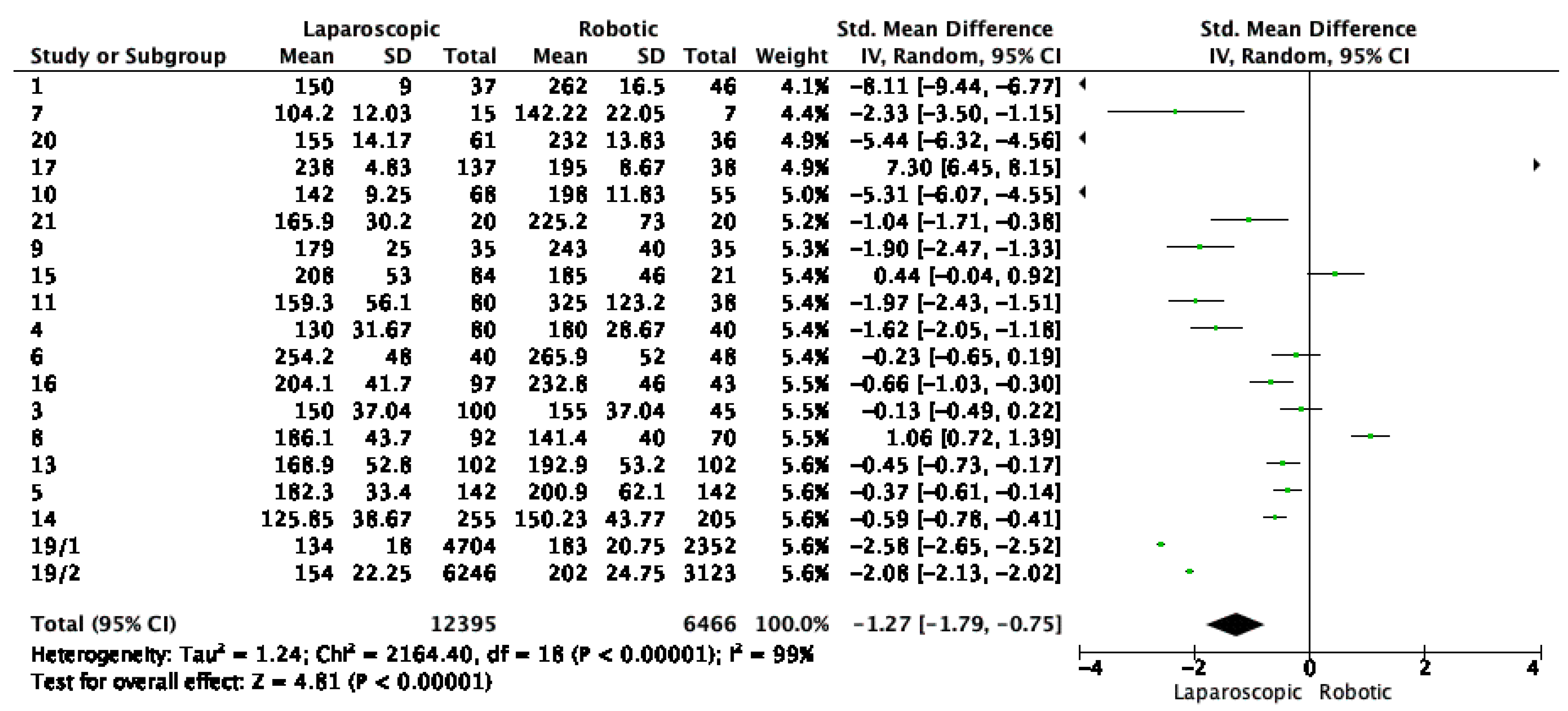
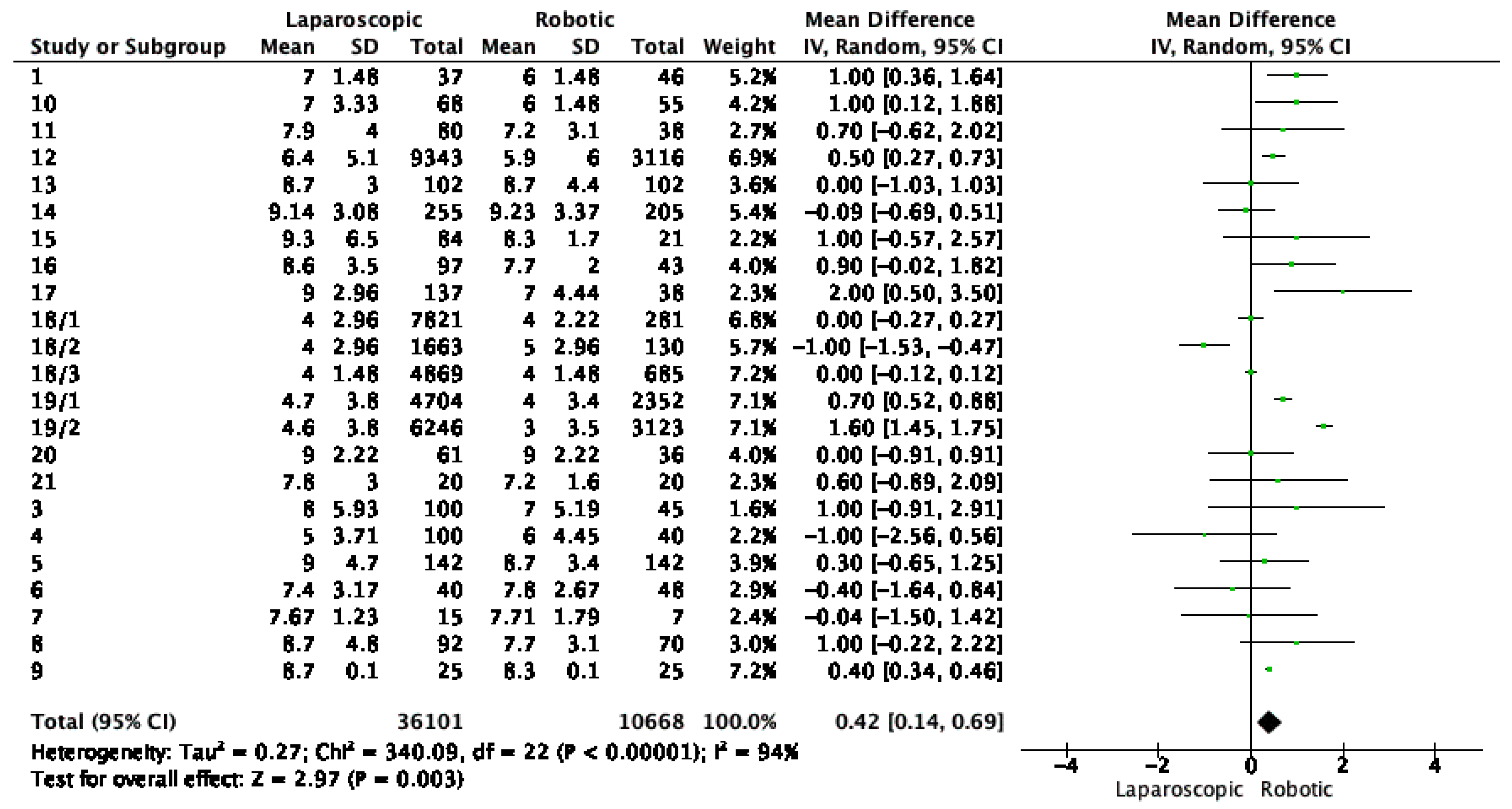
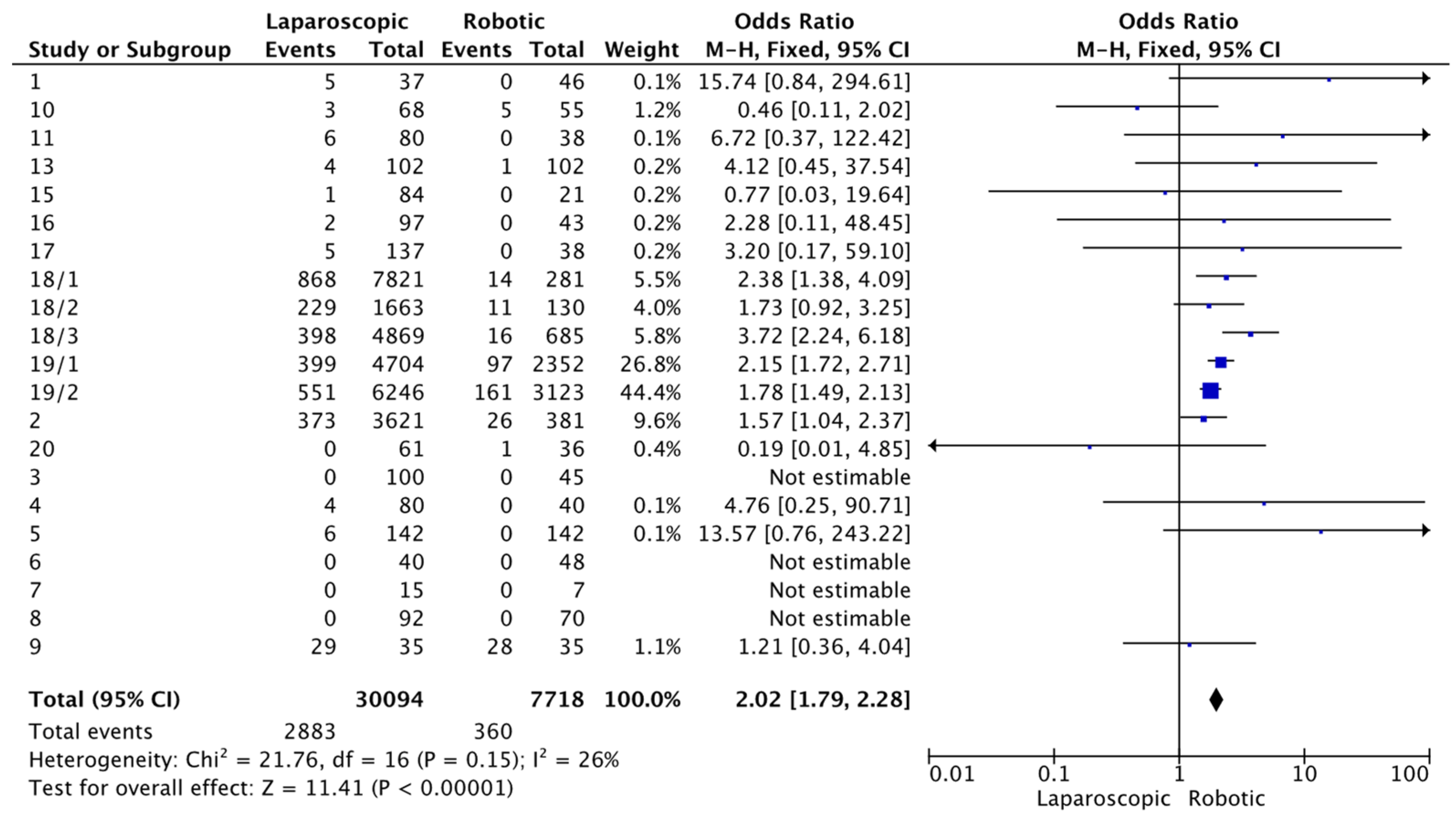
3.4. Meta-Analysis
Publication Bias
4. Discussion
- 1.
- Study design variability.
- 2.
- Confounding factors
- 3.
- Geographical representation.
- 4.
- Outcomes measured.
- 5.
- Publication bias.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Colorectal Cancer. WHO. Available online: https://www.who.int/news-room/fact-sheets/detail/colorectal-cancer (accessed on 10 February 2024).
- Reddy, K.; Gharde, P.; Tayade, H.; Patil, M.; Reddy, L.S.; Surya, D.; Srivani Reddy, L.; Surya, D., Jr. Advancements in Robotic Surgery: A Comprehensive Overview of Current Utilizations and Upcoming Frontiers. Cureus 2023, 15, e50415. [Google Scholar] [CrossRef] [PubMed]
- Sheetz, K.H.; Claflin, J.; Dimick, J.B. Trends in the adoption of robotic surgery for common surgical procedures. JAMA Netw. Open 2020, 3, e1918911. [Google Scholar] [CrossRef] [PubMed]
- Grimsley, E.A.; Barry, T.M.; Janjua, H.; Eguia, E.; DuCoin, C.; Kuo, P.C. Exploring the paradigm of robotic surgery and its contribution to the growth of surgical volume. Surg. Open Sci. 2022, 10, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, M.; Verdeja, J.C.; Goldstein, H.S. Minimally invasive colon resection (laparoscopic colectomy). Surg. Laparosc. Endosc. 1991, 1, 144–150. [Google Scholar] [PubMed]
- Monson, J.R.; Darzi, A.; Carey, P.D.; Guillou, P.J. Prospective evaluation of laparoscopic-assisted colectomy in an unselected group of patients. Lancet 1992, 340, 831–833. [Google Scholar] [CrossRef] [PubMed]
- Falk, P.M.; Beart, R.W., Jr.; Wexner, S.D.; Thorson, A.G.; Jagelman, D.G.; Lavery, I.C.; Johansen, O.B.; Fitzgibbons, R.J. Laparoscopic colectomy: A critical appraisal. Dis. Colon Rectum 1993, 36, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Simorov, A.; Shaligram, A.; Shostrom, V.; Boilesen, E.; Thompson, J.; Oleynikov, D. Laparoscopic colon resection trends in utilization and rate of conversion to open procedure: A national database review of academic medical centers. Ann. Surg. 2012, 256, 462–468. [Google Scholar] [CrossRef]
- Fox, J.; Gross, C.P.; Longo, W.; Reddy, V.M. Laparoscopic colectomy for the treatment of cancer has been widely adopted in the United States. Dis. Colon Rectum 2012, 55, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.P.; Albert, M.R. A current review of robotic colorectal surgery. Ann. Laparosc. Endosc. Surg. 2020, 5, 9. [Google Scholar] [CrossRef]
- Administration USFaD. 510(k) Premarket Notification. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm?ID=K990144 (accessed on 28 February 2024).
- Weber, P.A.; Merola, S.; Wasielewski, A.; Ballantyne, G.H. Telerobotic-assisted laparoscopic right and sigmoid colectomies for benign disease. Dis. Colon Rectum 2002, 45, 1689–1694; discussion 1695–1786. [Google Scholar] [CrossRef]
- Hashizume, M.; Shimada, M.; Tomikawa, M.; Ikeda, Y.; Takahashi, I.; Abe, R.; Koga, F.; Gotoh, N.; Konishi, K.; Maehara, S.; et al. Early experiences of endoscopic procedures in general surgery assisted by a computer-enhanced surgical system. Surg. Endosc. 2002, 16, 1187–1191. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- DeMars, M.M.; Perruso, C. MeSH and text-word search strategies: Precision, recall, and their implications for library instruction. J. Med. Libr. Assoc. 2022, 110, 23–33. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Peters, M.D.; Godfrey, C.M.; McInerney, P.; Soares, C.B.; Khalil, H.; Parker, D. The Joanna Briggs Institute Reviewers’ Manual 2015: Methodology for JBI Scoping Reviews; The Joanna Briggs Institute: Adelaide, Australia, 2015. [Google Scholar]
- Review Manager (RevMan) [Computer Program], version 5.4; The Cochrane Collaboration: London, UK, 2020.
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 6.4 (Updated August 2023); Cochrane: London, UK, 2023; Available online: www.training.cochrane.org/handbook (accessed on 28 February 2024).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Grosek, J.; Ales Kosir, J.; Sever, P.; Erculj, V.; Tomazic, A. Robotic versus laparoscopic surgery for colorectal cancer: A case-control study. Radiol. Oncol. 2021, 55, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Dohrn, N.; Klein, M.F.; Gögenur, I. Robotic versus laparoscopic right colectomy for colon cancer: A nationwide cohort study. Int. J. Colorectal. Dis. 2021, 36, 2147–2158. [Google Scholar] [CrossRef]
- Zhang, Y.; Feng, H.; Wang, S.; Gu, Y.; Shi, Y.; Song, Z.; Deng, Y.; Ji, X.; Cheng, X.; Zhang, T.; et al. Short- and long-term outcomes of robotic- versus laparoscopic-assisted right hemicolectomy: A propensity score-matched retrospective cohort study. Int. J. Surg. 2022, 105, 106855. [Google Scholar] [CrossRef]
- Khan, J.S.; Ahmad, A.; Odermatt, M.; Jayne, D.G.; Ahmad, N.Z.; Kandala, N.; West, N.P. Robotic complete mesocolic excision with central vascular ligation for right colonic tumours—A propensity score-matching study comparing with standard laparoscopy. BJS Open 2021, 5, zrab016. [Google Scholar] [CrossRef]
- Tian, Y.; Xiong, D.; Xu, M.; Fan, Q.; Zheng, H.; Shen, H.; Huang, B.; Wang, L.; Li, C.; Zhang, A.; et al. Robotic versus laparoscopic right hemicolectomy with complete mesocolic excision: A retrospective multicenter study with propensity score matching. Front. Oncol. 2023, 13, 1187476. [Google Scholar] [CrossRef]
- Sorgato, N.; Mammano, E.; Contardo, T.; Vittadello, F.; Sarzo, G.; Morpurgo, E. Right colectomy with intracorporeal anastomosis for cancer: A prospective comparison between robotics and laparoscopy. J. Robot. Surg. 2022, 16, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Di Lascia, A.; Tartaglia, N.; Petruzzelli, F.; Pacilli, M.; Maddalena, F.; Fersini, A.; Pavone, G.; Vovola, F.; Ambrosi, A. Right hemicolectomy: Laparoscopic versus robotic approach. Ann. Ital. Chir. 2020, 91, 478–485. [Google Scholar] [PubMed]
- Huang, Z.; Li, T.; Zhang, G.; Zhou, Z.; Shi, H.; Tang, C.; Yang, L.; Lei, X. Comparison of open, laparoscopic, and robotic left colectomy for radical treatment of colon cancer: A retrospective analysis in a consecutive series of 211 patients. World J. Surg. Oncol. 2022, 20, 345. [Google Scholar] [CrossRef] [PubMed]
- Ferri, V.; Quijano, Y.; Nuñez, J.; Caruso, R.; Duran, H.; Diaz, E.; Fabra, I.; Malave, L.; Isernia, R.; d’Ovidio, A.; et al. Robotic-assisted right colectomy versus laparoscopic approach: Case-matched study and cost-effectiveness analysis. J. Robot. Surg. 2021, 15, 115–123. [Google Scholar] [CrossRef]
- Tagliabue, F.; Burati, M.; Chiarelli, M.; Fumagalli, L.; Guttadauro, A.; Arborio, E.; De Simone, M.; Cioffi, U. Robotic vs. laparoscopic right colectomy—The burden of age and comorbidity in perioperative outcomes: An observational study. World J. Gastrointest. Surg. 2020, 12, 287–297. [Google Scholar] [CrossRef]
- Ozben, V.; de Muijnck, C.; Sengun, B.; Zenger, S.; Agcaoglu, O.; Balik, E.; Aytac, E.; Bilgin, I.A.; Baca, B.; Hamzaoglu, I.; et al. Robotic complete mesocolic excision for transverse colon cancer can be performed with a morbidity profile similar to that of conventional laparoscopic colectomy. Tech. Coloproctol. 2020, 24, 1035–1042. [Google Scholar] [CrossRef]
- Pacheco, F.; Harris-Gendron, S.; Luciano, E.; Zreik, J.; Kamel, M.K.; Solh, W.A. Robotic versus laparoscopic colectomy outcomes in colon adenocarcinoma in the elderly population: A propensity-score matched analysis of the National Cancer Database. Int. J. Colorectal. Dis. 2023, 38, 183, Erratum in Int. J. Colorectal. Dis. 2023, 39, 9. [Google Scholar] [CrossRef]
- Zheng, H.; Wang, Q.; Fu, T.; Wei, Z.; Ye, J.; Huang, B.; Li, C.; Liu, B.; Zhang, A.; Li, F.; et al. Robotic versus laparoscopic left colectomy with complete mesocolic excision for left-sided colon cancer: A multicentre study with propensity score matching analysis. Tech. Coloproctol. 2023, 27, 569–578. [Google Scholar] [CrossRef]
- Xu, M.; Zhao, Z.; Jia, B.; Liu, R.; Liu, H. Perioperative and long-term outcomes of robot-assisted versus laparoscopy-assisted hemicolectomy for left-sided colon cancers: A retrospective study. Updates Surg. 2021, 73, 1049–1056. [Google Scholar] [CrossRef]
- Chang, T.C.; Lin, E.K.; Lu, Y.J.; Huang, M.T.; Chen, C.H. Single-incision robotic colectomy versus single-incision laparoscopic colectomy: A matched case control study. Asian J. Surg. 2021, 44, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Oh, B.Y.; Chung, S.S.; Lee, R.A.; Noh, G.T. Short-term outcomes of single-incision robotic colectomy versus conventional multiport laparoscopic colectomy for colon cancer. J. Robot. Surg. 2023, 17, 2351–2359. [Google Scholar] [CrossRef]
- Maertens, V.; Stefan, S.; Rutgers, M.; Siddiqi, N.; Khan, J.S. Oncological outcomes of open, laparoscopic and robotic colectomy in patients with transverse colon cancer. Tech. Coloproctol. 2022, 26, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Sterk, M.F.M.; Crolla, R.M.P.H.; Verseveld, M.; Dekker, J.W.T.; van der Schelling, G.P.; Verhoef, C.; Olthof, P.B. Uptake of robot-assisted colon cancer surgery in the Netherlands. Surg. Endosc. 2023, 37, 8196–8203. [Google Scholar] [CrossRef]
- Farah, E.; Abreu, A.A.; Rail, B.; Salgado, J.; Karagkounis, G.; Zeh, H.J., 3rd; Polanco, P.M. Perioperative outcomes of robotic and laparoscopic surgery for colorectal cancer: A propensity score-matched analysis. World J. Surg. Oncol. 2023, 21, 272. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.U.; Jegon, W.K.; Baek, S.K. Single plus one-port robotic surgery using the da Vinci Single-Site Platform versus conventional multi-port laparoscopic surgery for left-sided colon cancer. Wideochir Inne Tech. Maloinwazyjne 2022, 17, 179–187. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Costa, G.; Ferraro, V.; De Rosa, M.; Rondelli, F.; Bugiantella, W. Robotic or three-dimensional (3D) laparoscopy for right colectomy with complete mesocolic excision (CME) and intracorporeal anastomosis? A propensity score-matching study comparison. Surg. Endosc. 2021, 35, 2039–2048. [Google Scholar] [CrossRef]
- JASP Team. JASP, version 0.18.3; Computer software; JASP Team: Amsterdam, The Netherlands, 2024. [Google Scholar]
- Köckerling, F. Robotic vs. Standard Laparoscopic Technique—What is Better? Front. Surg. 2014, 1, 15. [Google Scholar] [CrossRef]
- Liu, H.; Kinoshita, T.; Tonouchi, A.; Kaito, A.; Tokunaga, M. What are the reasons for a longer operation time in robotic gastrectomy than in laparoscopic gastrectomy for stomach cancer? Surg. Endosc. 2019, 33, 192–198. [Google Scholar] [CrossRef]
- Zheng, J.C.; Zhao, S.; Chen, W.; Wu, J.X. Robotic versus laparoscopic right colectomy for colon cancer: A systematic review and meta-analysis. Wideochir Inne Tech. Maloinwazyjne 2023, 18, 20–30. [Google Scholar] [CrossRef]
- Wei, P.-L.; Huang, Y.-J.; Wang, W.; Huang, Y.-M. Comparison of robotic reduced-port and laparoscopic approaches for left sided colorectal cancer surgery. Asian J. Surg. 2023, 46, 698–704. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | % YES | RISK | RISK |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Jan Grosek et al., Slovenia, 2021 [22] | Y | Y | Y | Y | Y | Y | Y | U | U | U | Y | 73% | ☺ | LOW |
| Niclas Dohrn et al. Denmark 2021 [23] | Y | Y | Y | Y | Y | Y | Y | U | U | U | Y | 73% | ☺ | LOW |
| Yaqi Zhang et al., China 2022 [24] | Y | Y | Y | Y | Y | Y | Y | Y | U | U | Y | 82% | ☺ | LOW |
| J. S. Khan et al., UK 2021 [25] | Y | Y | Y | Y | Y | Y | Y | Y | U | U | Y | 82% | ☺ | LOW |
| Yue Tian et al., China 2023 [26] | Y | U | U | Y | Y | Y | Y | Y | Y | U | Y | 73% | ☺ | LOW |
| Nadia Sorgato et al., Italy 2022 [27] | Y | U | U | Y | Y | Y | Y | Y | Y | U | Y | 73% | ☺ | LOW |
| Alessandra Di Lascia et al., Italy 2020 [28] | Y | Y | Y | U | U | Y | Y | U | U | U | Y | 55% | ☺ | MODERATE |
| Zhixiang Huang et al., China 2022 [29] | Y | Y | Y | Y | Y | Y | Y | Y | U | U | Y | 82% | ☺ | LOW |
| Valentina Ferri et al., Spain 2020 [30] | Y | U | U | Y | Y | Y | Y | Y | Y | U | Y | 73% | ☺ | LOW |
| Fulvio Tagliabue et al., Italy 2020 [31] | Y | U | U | Y | Y | Y | Y | Y | U | U | Y | 64% | ☺ | MODERATE |
| V. Ozben et al., Turkey 2020 [32] | Y | U | U | Y | Y | Y | Y | Y | Y | U | Y | 73% | ☺ | LOW |
| Filipe Pacheco et al., USA 2023 [33] | Y | U | U | Y | Y | Y | Y | Y | U | U | Y | 64% | ☺ | MODERATE |
| Huichao Zeng et al., China 2023 [34] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% | ☺ | LOW |
| Maolin Xu et al., China 2020 [35] | Y | Y | Y | Y | Y | Y | Y | Y | U | U | Y | 82% | ☺ | LOW |
| Tung-Cheng Chang et al., China 2021 [36] | Y | Y | Y | Y | Y | Y | Y | U | U | U | Y | 73% | ☺ | LOW |
| Ho Segun Kim et al., Korea 2021 [37] | Y | Y | Y | Y | Y | Y | Y | U | U | U | Y | 73% | ☺ | LOW |
| V. Maertens et al., UK 2022 [38] | Y | Y | Y | U | Y | Y | Y | Y | U | U | Y | 73% | ☺ | LOW |
| Marlou F. M. Sterk et al., Netherland 2023 [39] | Y | Y | Y | U | Y | Y | Y | U | U | U | Y | 64% | ☺ | MODERATE |
| Emile Farah et al., USA 2023 [40] | Y | Y | Y | Y | Y | Y | Y | Y | U | U | Y | 82% | ☺ | LOW |
| Sung Uk Bae et al., Korea 2022 [41] | Y | U | U | Y | Y | Y | Y | Y | U | U | Y | 64% | ☺ | MODERATE |
| Graziano Ceccarelli et al., Italy 2020 [42] | Y | Y | Y | Y | Y | Y | Y | U | U | U | Y | 55% | ☺ | MODERATE |
| Author, Country, Year of Publication, Ref. Nr. | Nr | Study Type, Period of Study | Cases Number Lap/Rob | Propensity Score Matching | Sex Male Lap/Rob | Age Lap/Rob | BMI Lap/Rob |
|---|---|---|---|---|---|---|---|
| Jan Grosek et al., Slovenia 2021 [22] | 1 | Retrospective single center 2019–2020 | 37 LAP | - | 23/26 | 67.5 ± 10.1/66.8 ± 11 | 27.2 (25.1–29.4)/27.5 (25.7–31.3) |
| 46 ROB | |||||||
| Niclas Dohrn et al., Denmark 2021 [23] | 2 | Retrospective National Cancer Database 2015–2018 | 3621 LAP | - | 1621/185 | 73 ± 8.89/73 ± 8.89 | 25.7 (22.9–29.04)/25.6 (23.2–28.8) |
| 381 ROB | |||||||
| Yaqi Zhang et al., China 2022 [24] | 3 | Retrospective | 100 LAP | 1:3 | 41/19 | - | - |
| single center 2016–2018 | 45 ROB | ||||||
| J. S. Khan et al., UK 2021 [25] | 4 | Prospective single center 2007–2017, 2014–2017 | 80 LAP | 2:1 | |||
| 40 ROB | 37/19 | 71 ± 33.3/69 ± 34.07 | 28 (19–47)/26 (20–37) | ||||
| Yue Tian et al., China 2023 [26] | 5 | Retrospective multicenter 2016–2021 | 142 LAP | 1:1 | 79/74 | 63.4 ± 11.3/63.2 ± 2.4 | 22.5 (3.24)/22.5 (3.2) |
| 142 ROB | |||||||
| Nadia Sorgato et al., Italy 2022 [27] | 6 | Prospective multicenter 2018–2019 | 40 LAP | - | 28/27 | 68 ± 10/71 ± 12.2 | 26.6 (17.9–36.3)/25.6 (17.5–47.3) |
| 48 ROB | |||||||
| Alessandra Di Lascia et al., Italy 2020 [28] | 7 | Retrospective single center 2014–2017 | 15 LAP 7 ROB | - | 8/4 | 75 ± 3/75.7 ± 2.56 | 25 (19–41)/26 (21–38) |
| Zhixiang Huang et al., China 2022 [29] | 8 | Retrospective single center 2012–2017 | 92 LAP 70 ROB | - | - | - | - |
| Valentina Ferri et al., Spain 2020 [30] | 9 | Prospective single center 2013–2017, 2014–2018 | 35 LAP 35 ROB | 1:1 | 20/23 | 68.2 ± 8.67/69.6 ± 7 | 25 (20–34)/23 (19–31) |
| Fulvio Tagliabue et al., Italy 2020 [31] | 10 | Retrospective single center 2014–2019 | 68 LAP 55 ROB | - | 40/32 | - | 24.81 (23.10–28.45)/24.31 (22.11–27.56) |
| V. Ozben et al., Turkey 2020 [32] | 11 | Retrospective multicenter 2011–2018 | 80 LAP 38 ROB | - | 47/27 | 64.1 ± 15.5/62.3 ± 15.7 | 26.7 (7.7)/25.3 (6.1) |
| Filipe Pacheco et al., USA 2023 [33] | 12 | Retrospective National Cancer Database 2010–2018 | 9343 LAP 3116ROB | 3:1 | 3957/1314 | - | - |
| Huichao Zeng et al., China 2023 [34] | 13 | Retrospective multicenter 2014–2022 | 102 LAP 102 ROB | 1:1 | 66/71 | 59 ± 12.5/61 ± 16.25 | 23.5 (4.86)/23.7 (4.46) |
| Maolin Xu et al., China 2020 [35] | 14 | Retrospective single center 2012–2018 | 255 LAP 205 ROB | - | 170/123 | 60.26 ± 11.04/60.36 ± 11.33 | 24.78 (4.27)/24.8 (4.51) |
| Tung-Cheng Chang et al., China 2021 [36] | 15 | Retrospective multicenter 2013–2019 | 84 LAP 21 ROB | 1:4 | 43/9 | 65.6 ± 13.6/62.1 ± 11.9 | 24.6 (4.19)/24.7 (5.27) |
| Ho Segun Kim et al., Korea 2021 [37] | 16 | Retrospective single center 2019–2022 | 97 LAP 43 ROB | - | 63/12 | 70.6 ± 7.7/58.8 ± 7.7 | 24.3 (10.4)/23.4 (4.05) |
| V. Maertens et al., UK 2022 [38] | 17 | Retrospective single center 2005–2021 | 137 LAP 38 ROB | - | 82/20 | 71 ± 9.17/65 ± 8.17 | 27 (18–40)/26.5 (20–33) |
| Marlou F. M. Sterk et al., Netherland 2023 [39] | 18/1; 18/2; 18/3 | Retrospective Dutch colorectal audit 2018–2020 | 14353 LAP 1096 ROB | - | Gr1:3557/136 Gr2:913/70 Gr3: 2886/405 | Gr1: 73 ± 9.63/73 ± 9.63 Gr2:70 ± 10.37/71 ± 11.11 Gr3:69 ± 12.59/69 ± 11.85 | Gr1:26.0 (23.4–29.1)/25.7 (23.4–28.9) Gr2: 26.2 (23.5–29.4)/26.7 (24.4–29.6) Gr3: 26.1 (23.6–29.1)/26.0 (23.7–28.7) |
| Emile Farah et al., USA 2023 [40] | 19/1; 19/2 | Retrospective ACS-NSQIP Database 2015–2020 | 10950 LAP 5475 ROB | 2:1 | Gr1:2187/1106 Gr2: 3266/1633 | - | - |
| Sung Uk Bae et al., Korea, 2022 [41] | 20 | Retrospective single center 2014–2016 | 61 LAP 36 ROB | - | 38/17 | 67 ± 10.37/62 ± 10.37 | 24.0 (21.0–27.0)/24.6 (21.0–27.0) |
| Graziano Ceccarelli et al., Italy, 2020 [42] | 1 | Retrospective single center 2014–2019 | 20 LAP 20 ROB | 1:1 | 13/14 | 74.6 ( ± 13.8)/70.6 ( ± 9.9) | 24.1 (22.14–26.06)/23 (21.38–24.62) |
| Outcome | Nr. of Studies | Lap | Rob | OR/MD (95%CI Interval) | I2 (%) | p-Value |
|---|---|---|---|---|---|---|
| Age mean(SD) | 18 | 69.065 ± 10.577 | 67.96 ± 12.697 | 0.98 [0.01–1.95] | 80% | 0.05 |
| Sex male | 20 | 19,085 (48.16%) | 5366 (48.81%) | 0.96 [0.85, 1.08] | 70% | 0.48 |
| ASA score > 3 | 18 | 12,863 (42.64%) | 4033 (51.75%) | 1.04 [0.98, 1.10] | 33% | 0.18 |
| UICC stage III–IV | 17 | 4737 (33.11%) | 1443 (32.44%) | 1.01 [0.94–1.09] | 0% | 0.80 |
| Laparoscopic vs. Robotic Surgery | Number of Studies | p-Value | I2 | OR/MD (95%CI) | Chi2 | Z |
|---|---|---|---|---|---|---|
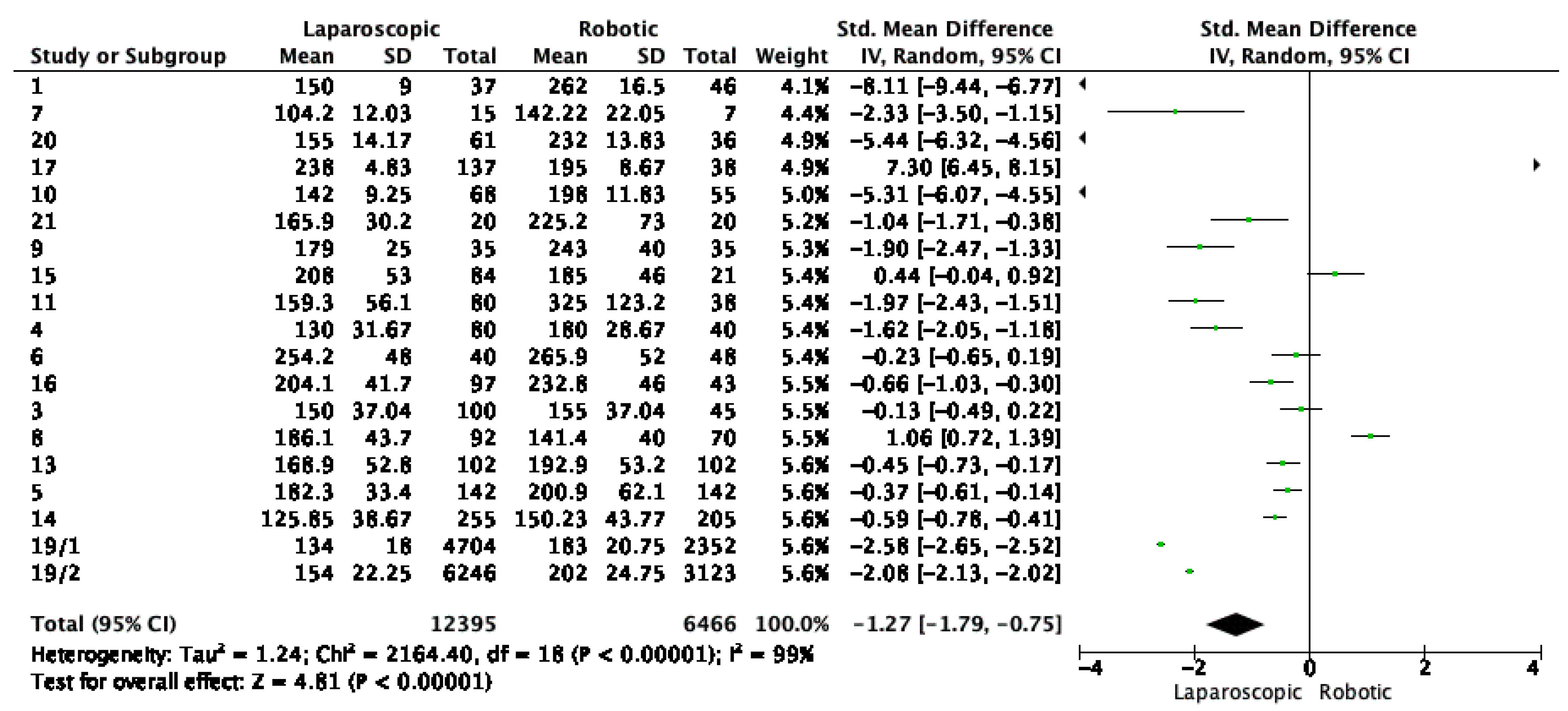
| Specimen size | 4 | 0.43 | 69% | −1.64 [−5.69, 2.42] | 12.72 | 0.79 |
| Positive resection margins | 12 | 0.81 | 0% | −0.00 [−0.02, 0.01] | 2.14 | 0.24 |
| Distance from tumor to distal margin | 4 | 0.79 | 0% | 0.15 [−0.96, 1.26] | 2.04 | 0.27 |
| Distance from tumor to proximal margin | 6 | 0.30 | 92% | 1.52 [−1.35, 4.38] | 66.61 | 1.04 |
| Complications | 18 | 0.44 | 0% | 1.03 [0.95, 1.12] | 17.01 | 0.78 |
| Major complications Clavien-Dindo III–IV | 17 | 0.98 | 0% | 1.00 [0.89, 1.13] | 7.18 | 0.03 |
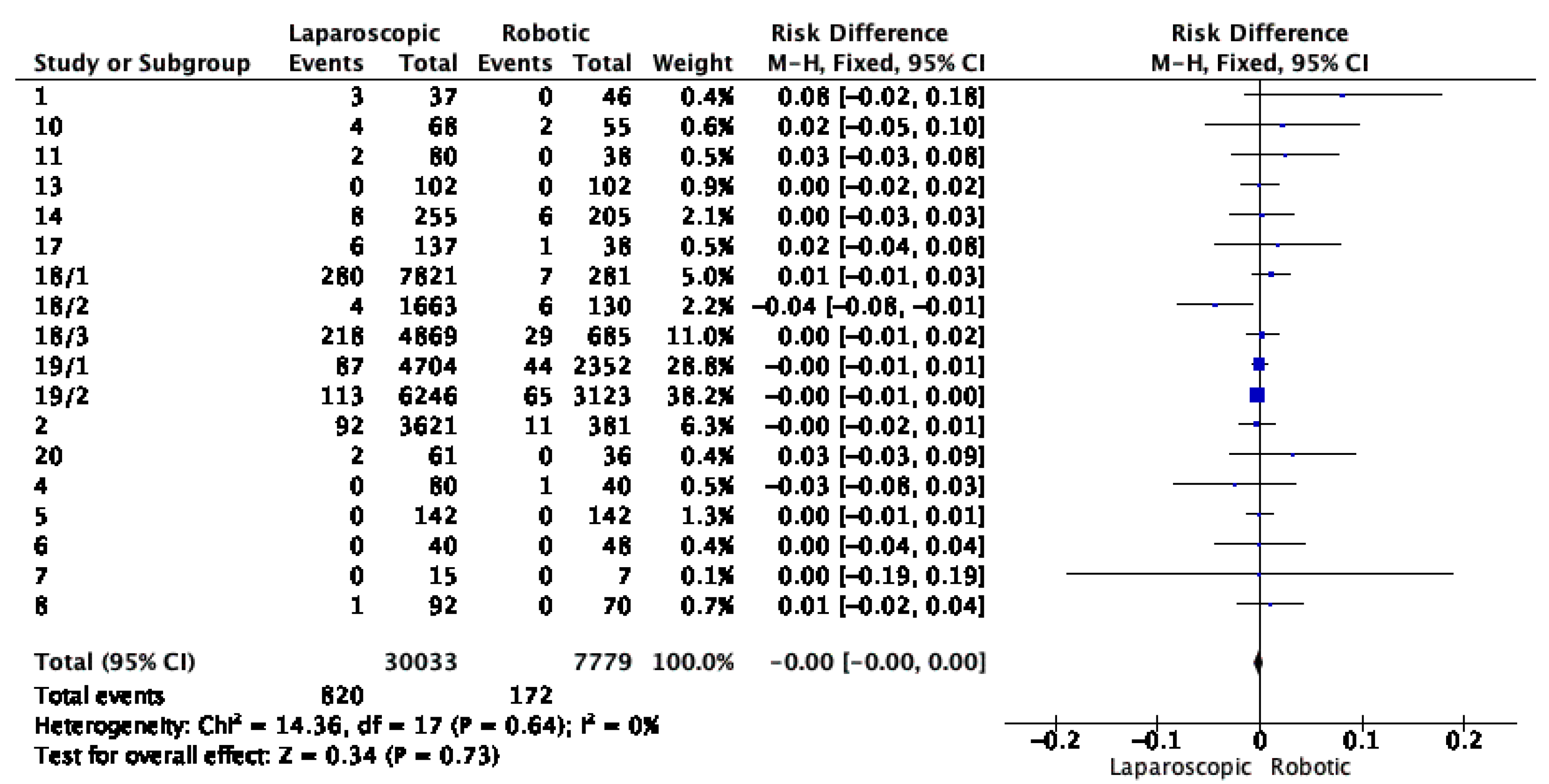
| 30-day mortality | 14 | 0.21 | 31% | 0.00 [−0.00, 0.01] | 20.38 | 1.26 |
| Regression Test for Funnel Plot Asymmetry (“Egger’s Test”) | ||
|---|---|---|
| Z | p | |
| sei | 2.733 | 0.006 |
| Mean Estimates (μ) | |||||||
|---|---|---|---|---|---|---|---|
| 95% Confidence Interval | |||||||
| Estimate | Standard Error | t | df | p | Lower | Upper | |
| PET | −0.076 | 0.061 | −1.242 | 19 | 0.229 | −0.196 | 0.044 |
| PEESE | 0.038 | 0.069 | 0.555 | 19 | 0.585 | −0.097 | 0.173 |
| Summary | ||||
|---|---|---|---|---|
| Models | P(M) | P(M|Data) | Inclusion BF | |
| Effect | 18/36 | 0.500 | 0.533 | 1.140 |
| Heterogeneity | 18/36 | 0.500 | 1.000 | 1.503 × 10+125 |
| Publication bias | 32/36 | 0.500 | 0.977 | 41.566 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Negrut, R.L.; Cote, A.; Caus, V.A.; Maghiar, A.M. Systematic Review and Meta-Analysis of Laparoscopic versus Robotic-Assisted Surgery for Colon Cancer: Efficacy, Safety, and Outcomes—A Focus on Studies from 2020–2024. Cancers 2024, 16, 1552. https://doi.org/10.3390/cancers16081552
Negrut RL, Cote A, Caus VA, Maghiar AM. Systematic Review and Meta-Analysis of Laparoscopic versus Robotic-Assisted Surgery for Colon Cancer: Efficacy, Safety, and Outcomes—A Focus on Studies from 2020–2024. Cancers. 2024; 16(8):1552. https://doi.org/10.3390/cancers16081552
Chicago/Turabian StyleNegrut, Roxana Loriana, Adrian Cote, Vasile Aurel Caus, and Adrian Marius Maghiar. 2024. "Systematic Review and Meta-Analysis of Laparoscopic versus Robotic-Assisted Surgery for Colon Cancer: Efficacy, Safety, and Outcomes—A Focus on Studies from 2020–2024" Cancers 16, no. 8: 1552. https://doi.org/10.3390/cancers16081552
APA StyleNegrut, R. L., Cote, A., Caus, V. A., & Maghiar, A. M. (2024). Systematic Review and Meta-Analysis of Laparoscopic versus Robotic-Assisted Surgery for Colon Cancer: Efficacy, Safety, and Outcomes—A Focus on Studies from 2020–2024. Cancers, 16(8), 1552. https://doi.org/10.3390/cancers16081552