Simple Summary
In the face of significant hurdles stemming from conflicts and resource constraints, Jordan has emerged as an exemplary paradigm, solidifying cancer care both locally and regionally. Despite the positive progress being made, a significant obstacle is emerging in the form of increasing rates of cancer, which is representative of a larger upsurge in non-communicable diseases. However, a thorough grasp of the various contributing factors is still lacking. Therefore, we aimed to carefully examine and discuss the current identified barriers that are hindering the achievement of optimal cancer care in Jordan.
Abstract
This narrative review explores the multifaceted barriers hindering access to quality cancer care in Jordan. A literature-based narrative review was undertaken to explore the current identified barriers to cancer care in Jordan. Four databases were searched using relevant keywords to identify key insights on barriers and proposed solutions. Key challenges and potential solutions were identified based on evidence from studies, reports, and initiatives. Medical services and infrastructure exhibit centralized disparities, impacting rural and underserved areas. Human resources shortages, geopolitical instability, and quality management issues pose significant challenges. Public awareness campaigns face hurdles in addressing the tobacco epidemic and late-stage diagnosis. Socioeconomic disparities, particularly in health insurance and urban–rural divides, further compound barriers. Refugees encounter distinct challenges, including late-stage diagnosis, financial barriers, and psychological distress. Despite multiple challenges, Jordan presents a model for regional development and health equity. This study not only contributes to improving cancer care in Jordan but also offers a roadmap for policymakers, healthcare practitioners, and researchers in similar contexts globally. Government initiatives, financial aspects, and proposed policy measures are examined as potential solutions. Recommendations include coordinated prevention strategies, enhanced screening uptake, training programs, the equitable distribution of facilities, and policy directives aligned with global commitments. The role of digital technologies, telemedicine, and community engagement models is emphasized.
1. Introduction
Jordan faces unique healthcare challenges as a low-middle-income country (LMIC) [1]. Located in the Eastern Mediterranean region with a land area of approximately 89,000 km, Jordan’s current population is estimated to be 10 million, with an annual population growth rate of 2.4% [2]. According to statistics from the Jordanian Cancer Registry, cancer is a leading cause of morbidity and mortality in Jordan, with breast and lung cancer being the most prevalent in women and men, respectively [3]. The cancer burden is compounded by high rates of major noncommunicable diseases (NCDs) like cardiovascular disease, diabetes, and hypertension. Demographic and economic pressures, such as poverty, urbanization, and the influx of refugees, strain Jordan’s healthcare system [1].
Healthcare comprises approximately 8% of gross domestic product (GDP) expenditure in Jordan [4]. Jordan’s healthcare is mainly provided through the public and private sectors. The public sector is composed of the Ministry of Health (MOH), the military’s Royal Medical Services, and university hospitals. The private sector accounts for approximately 33% of all hospital beds [5]. Specialized cancer care is centralized at the King Hussein Cancer Center (KHCC), which serves over 60% of cancer patients in Jordan [6]. Private insurance does not cover cancer treatment, and the government in Jordan assumes the costs of caring for Jordanian patients with cancer at public hospitals and the KHCC. However, barriers across the healthcare system, the economic landscape, and demographics impede equitable access to quality cancer care and put additional strain on patients with cancer seeking equitable and comprehensive cancer care.
This narrative review will establish the need to examine these barriers in the Jordanian context. It will preview key challenges within medical services, human resources, quality management, public awareness, and socioeconomics. The review will outline evidence-based solutions to overcome these barriers, guided by examples from the KHCC and global best practices, to ultimately enhance cancer prevention, early detection, and comprehensive treatment for the Jordanian population.
2. Materials and Methods
2.1. Data Sources and Validity
The data for this narrative review were gathered from a search of peer-reviewed academic literature, government reports, and international organization databases. Four public databases, namely PubMed, EMBASE, Scopus, and Web of Science, were searched using relevant keywords related to cancer care barriers in Jordan. Furthermore, the records of Google Scholar served as a supplementary resource to ensure a more comprehensive exploration of relevant studies. The search was manually conducted with the assistance of a medical librarian, and a detailed search strategy for databases can be found in the Supplementary File. Additionally, non-peer-reviewed reports from organizations such as the World Health Organization (WHO), the Jordanian Ministry of Health, the KHCC, and the Jordanian Cancer Registry were retrieved. All data sources used in this review were available in the public domain and were deemed valid based on peer-review processes, government oversight, and institutional credibility.
2.2. Review Conduct
Studies were reviewed to assess their eligibility based on their relevance to the topic of cancer care barriers in Jordan. The authors included the studies with relevant information on barriers to cancer care, including medical services and infrastructure, human resources, quality management, public awareness, socioeconomic disparities, and the specific challenges faced by vulnerable populations, with a focus on refugees. The data review included information on the nature of barriers, contributing factors, and proposed solutions. The review covered a period spanning from inception to 3 January 2023, providing a comprehensive analysis of the barriers to cancer care in Jordan over the past two decades.
2.3. Analysis Approach
Data analysis involved synthesizing information from diverse sources to identify common themes, patterns, and key insights related to barriers to cancer care in Jordan. Thematic analysis techniques were employed to categorize and organize findings according to thematic areas, including healthcare infrastructure, human resources, quality management, public awareness, socioeconomic disparities, and refugee healthcare. The review also examined proposed policy measures and initiatives aimed at overcoming identified barriers, highlighting successful strategies and areas requiring further attention.
3. Results
3.1. Medical Services and Infrastructure
The healthcare system in Jordan is divided between the private and public sectors, with 41 public and 65 private hospitals. However, the centralized and disconnected nature of cancer care services poses major barriers in Jordan. Both diagnostic and treatment facilities are concentrated in major cities, creating disparities for rural and underserved governorates [7]. Fragmented care across institutions and poor connectivity for sharing medical records hinder timely diagnosis and coordinated treatment [8]. Electronic medical records have been previously proposed as a solution to enable streamlined referrals and information exchange, but implementation challenges remain, mainly due to lack of funding and resources [7]. Structural and behavioral obstacles also lead to pronounced rural–urban disparities, including poorer health literacy on cancer symptoms and limited engagement with preventative services [9]. Initiatives to expand rural facilities and address provider absenteeism are needed [10], as suboptimal referral systems further delay cancer care as patients struggle to navigate between public, private, and non-governmental facilities [11].
3.2. Human Resources
Jordan faces shortages of specialized oncology professionals and trained oncology nurses, which strains existing staff and compromises patient care quality, and the associated rise in nurse–patient ratios impacts patients’ experiences and outcomes [12]. Due to this shortage, patients in rural areas may face challenges in accessing specialized cancer treatment due to the uneven distribution of healthcare professionals [10]. The shortage of oncologists and oncology nurses results in longer waiting times for cancer diagnosis and treatment, leading to delays in care and poorer outcomes [13]. Moreover, the emigration of oncologists and cancer specialists also cripples local capacity while draining global resources [7]. This brain drain is driven by limited career development and local incentives. Outdated training programs also contribute to suboptimal skills with newer technologies among healthcare workers. The KHCC faces staffing challenges due to the migration of highly qualified healthcare workers, mainly younger physicians seeking better opportunities abroad [14]. Despite efforts to retain talent, the allure of higher incomes and training opportunities in Western countries has led to a significant brain drain. This trend reflects global disparities in healthcare resources between LMICs like Jordan and high-income countries (HICs) [14].
3.3. Quality Management
Geopolitical instability in the region poses sustainability challenges for Jordan’s cancer care system. Political and economic fluctuations compromise consistent quality by disrupting supplies, healthcare funding, and service delivery [7]. Several barriers, including resource constraints, infrastructure deficiencies, regulatory gaps, and limited patient engagement, pose significant challenges to the implementation of quality management initiatives [12]. There are also disparities in care quality between private and public institutions, partly due to varying accreditation and standardization [15]. Centralized reporting and quality benchmarking are lacking in Jordan, which hinders the delivery of more uniform patient care. Robust primary care is also essential for effective cancer prevention and management but remains underdeveloped in Jordan [7]. Primary services that are equally distributed play a key preventive role in promoting healthy lifestyles and early detection [16]. Suboptimal reporting also impedes quality improvement efforts, as there are limitations in data accuracy and standardized quality metrics reported in Jordan [17].
3.4. Public Awareness
Public awareness of cancer is essential for promoting early detection, timely treatment, and better outcomes [18]. Misconceptions and misinformation about cancer may prevail, leading to delays in seeking medical attention and reluctance to engage in preventive behaviors [19]. The tobacco epidemic remains a major risk factor for cancer in Jordan, with over 60% of males smoking [20]. The high prevalence of smoking is associated with a high incidence of lung cancer, which is the leading cause of cancer death in Jordan. Besides lung cancer, tobacco use also increases the risk of cancers of the head and neck, colon, bladder, and acute leukemia; all are among the most common neoplasms in Jordan [21,22]. Despite public health efforts, smoking rates remain high and further expansion of smoke-free policies, advertising restrictions, and youth-focused interventions are needed [21]. Limited access to reliable sources of information, including healthcare providers, educational materials, and media campaigns, hinders efforts to raise awareness and promote early detection [23,24,25]. Late-stage diagnosis also impedes survival, driven by low rates of cancer screening, limited health literacy on symptoms, and healthcare access barriers (Figure 1) [7,22].
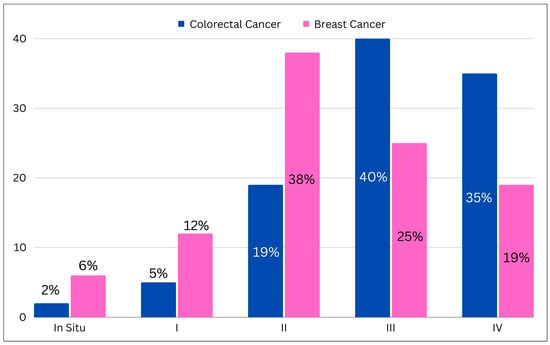
Figure 1.
Bar chart illustrating the initial stage of colorectal and breast cancer from the King Hussein Cancer Center registry (I: Stage 1; II: Stage 2; III: Stage 3; IV: Stage 4).
Support services for cancer survivors are also not well integrated, including home-based care, psychosocial support, and rehabilitation [7].
3.5. Socioeconomic Disparities
3.5.1. Health Insurance Disparities
There are significant gaps in health insurance coverage in Jordan driven by socioeconomic status. Only about 65% of Jordanians have some form of health insurance, with lower rates among unemployed, rural, and refugee populations [26]. Informal and agricultural workers lack access to government or private insurance schemes, resulting in high out-of-pocket health expenditures [27]. These disparities may lead to treatment delays, incomplete courses of therapy, or the abandonment of treatment altogether, compromising patient outcomes [26]. Uninsured patients face greater financial barriers to treatment, contributing to poorer survival rates compared to insured patients [28]. Government initiatives expanding insurance to schoolchildren and subsidizing premiums have reduced but not eliminated health insurance disparities, especially across geographic regions [29].
3.5.2. Urban–Rural Disparities
There are pronounced disparities in healthcare access between urban and rural areas in Jordan, with around 20% of the Jordanian population living in rural areas [16]. In Jordan, data from the World Bank showed a drop in the rural population from 49% in 1960 to 16% in 2015, constituting 8.8% of the total population in 2019 [30]. Rural populations face geographic barriers to reaching cancer diagnostic and treatment facilities that are concentrated in major cities [31]. Long distances and transport costs contribute to lower utilization of services and higher physician turnover [10]. Health literacy is also lower in rural communities, and illiteracy rates are higher than the national rate (6.7%) [2]. This is likely attributed to poor awareness of cancer symptoms and limited engagement in preventative behaviors [32,33]. High rates of provider absenteeism further exacerbate access challenges in rural regions [34]. Factors like poor work environments and lack of supervision contribute to absenteeism among rural health workers, which directly reduces service availability and quality [10]. These factors drive patients living in rural areas to seek services in the urban areas of Jordan; however, the lack of robust public transportation and the poor road network between the rural and urban areas of the county hinder the interaction between the rural and urban areas of Jordan [35].
3.6. Refugee Population and Cancer Care
Jordan has the largest population of refugees per capita in the world, with Syrians comprising the majority of the refugee population in Jordan [36]. Refugees face multiple challenges when it comes to cancer care in Jordan [37]. The Syrian refugee crisis has deeply affected the surrounding region since its onset in 2011, affecting more than five million Syrians that have sought refuge outside their homeland, predominantly in Turkey, Jordan, and Lebanon [38]. Studies from Jordan have shown that refugees often present at more advanced stages and receive suboptimal treatment [39,40]. Factors include disruptions in prior treatment, cost barriers, social marginalization, and discrimination [41]. Additionally, some refugees face structural barriers to receive care, such as not possessing the appropriate civil documentation for treatment [42]. Refugee care also relies heavily on humanitarian funding from United Nations agencies and international nongovernmental organizations, which remains below needs [43]. Despite government subsidies, refugees in Jordan have reported unaffordable out-of-pocket costs and long waiting times for care [44]. Refugees outside camps face particular disadvantages in accessing healthcare and navigating the system [45], and initiatives to expand insurance coverage, provide transport assistance, and strengthen primary care services for refugees are lacking in the region.
3.6.1. Late-Stage Diagnosis and Treatment Challenges
Cancer treatment in refugees involves a number of challenges, including financial stress, lack of health records, and frequent relocating and moving around [44]. Low awareness of cancer warning signs or symptoms, and stigma about cancer, persist in certain refugee populations in Jordan [19,46]. These issues make access to expensive oncological surgery, radiation, and chemotherapy difficult if not impossible for patients with long therapy plans, significantly complicating the provision of quality care [19]. In a study by Abdel-Razeq et al. on Syrian refugees seeking cancer treatment in Jordan, most patients with breast cancer had locally advanced or metastatic disease on presentation. More than one third of the patients had deviations from KHCC treatment guidelines and had worse outcomes than the general Jordanian population (Figure 2) [39].
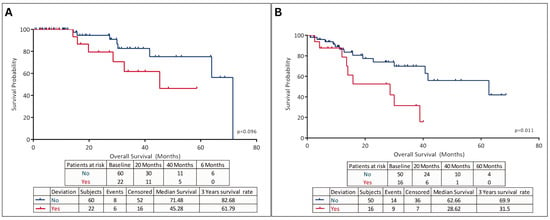
Figure 2.
Analysis of (A) overall survival, and (B) disease-free survival in Syrian refugees with breast cancer who sought treatment at KHCC (adapted from [39]).
3.6.2. Access to Timely and Optimal Treatment
It is of note that refugees also tend to have a higher incidence of delayed and suboptimal cancer treatment. One study found that the timing in receiving treatment varies from as low as 25% up to as high as 85%, with suboptimal timing of treatment in about 60% of patients [47]. These percentages illustrate only one aspect of this multidimensional problem; in addition to the aforementioned systemic barriers, refugees’ lack of capacity to navigate the system of a new country on their own makes expensive treatments like chemo-radio-surgery impossible without help or aid provided from outside sources [19]. Refugees also face challenges with timely access to treatment due to the grave cost of medical care and out-of-pocket medical costs stemming from clinical workups, multiple treatments, admission with complications, and indirect expenses such as accommodation and transportation [36]. A cost analysis in 2017 described the expenses linked to cancer treatment for Syrian refugees living in host nations using a per capita cost method, with an estimated total cost of 140.23 million euros in 2017 [48].
The medical services available within refugee camps managed by governmental bodies and non-governmental organizations are often relatively basic, lacking specialized providers and equipment to diagnose cancers or provide multimodal therapy, with suspected cases requiring referral to tertiary hospitals outside the camps after initial presentation and evaluation [49]. However, some recent global health initiatives have focused on facilitating direct oncology health services for refugees inside camps in Jordan through partnerships between humanitarian groups like Médecins sans Frontières (MSF) and national cancer treatment centers, to enable a more streamlined care.
3.6.3. Psychosocial and Survivorship Support
Refugees as a population report extremely high rates of adverse mental health conditions like major depression, post-traumatic stress disorder (PTSD), anxiety, and adjustment disorders that ultimately stem from prior violence exposure, traumatic loss of home/assets, family separation, uncertainty about the future, culture shock, and discrimination [50,51]. Most cancer care facilities in Jordan lack structured programs for psychosocial support [52]. This significant psychological distress and impaired quality of life amplifies the emotional burden typically associated with a concurrent cancer diagnosis. Additional culture-specific grief like losing one’s land also requires a nuanced understanding. Unfortunately, survivorship programs tailored specifically to promote rehabilitation and coping with cancer among refugee groups are markedly lacking, as seen from an assessment of the current global health literature, and are sorely needed to help address refugees’ unique psychosocial needs and facilitate community reintegration [53,54].
3.7. Government Initiatives and Financial Aspects
3.7.1. Government Subsidies and Investment
The Jordanian government has undertaken various initiatives to subsidize cancer treatment, recognizing the financial burden it imposes on patients [52]. Cancer treatment is offered at no cost to all Jordanian citizens through public hospitals including the MOH, Royal Medical Services, university hospitals, and the KHCC [52]. This approach is in line with global efforts to improve accessibility to lifesaving healthcare services. Notably, the government has been investing in increasing its health infrastructure, especially in cancer care and cancer screening. For example, one governmental initiative provided mobile mammography services to rural areas in Jordan that provided free-of-cost breast cancer screening to people who were eligible for breast cancer screening [55]. Such initiatives stand as an example of the commitment to a total service in cancer care, instead of a “quick fix” to direct cancer treatment. According to Marzouk et al. (2019), the uneven distribution of healthcare facilities is of paramount importance in equalizing access to health services [44]. However, the study concluded that it could be challenging to access underserved areas, and constant monitoring is important for the elimination of such disparities. A study carried out by Abdel-Razeq et al. highlighted the difficulties faced in the timely provision of cancer care among Syrian refugees, particularly by advocating for equal regional expansion drives [39]. Progress in this area has been made; however, more efforts have to be exerted so that these gaps can be closed and the whole population can benefit from better cancer care services.
3.7.2. Health Insurance Coverage
Health insurance coverage plays a crucial role in facilitating access to cancer care services. In Jordan, about 65% of Jordanians have some form of health insurance, with lower rates observed among unemployed individuals and rural populations [26]. There is coverage through the Health Insurance Fund, the Military Health Insurance Fund, and private medical insurance. Studies that explored the impact of health insurance status on cancer outcomes in Jordan revealed that uninsured cancer patients faced greater financial burdens, leading to delays in appropriate cancer screening or seeking treatment compared to insured patients [56,57]. Lack of health insurance coverage is associated with higher rates of advanced-stage cancer at diagnosis and increased mortality rates among cancer patients [39]. Prior studies in the literature have emphasized the importance of addressing gaps in health insurance coverage to improve cancer care delivery, as well as the need for policy interventions aimed at expanding health insurance coverage to vulnerable and underserved populations, such as rural communities and refugees, to ensure equitable access to cancer treatment services [58,59].
3.7.3. Financial Assistance Programs
Financial assistance programs play a crucial role in ensuring access to cancer care services for individuals in Jordan. However, disparities and limitations in these programs can hinder equitable access to treatment and support for cancer patients. Al-Qadi and Lozi examined the effectiveness of financial assistance programs for cancer patients in Jordan [60]. Their study highlighted challenges such as limited funding, eligibility criteria, and bureaucratic processes, which hinder access to financial support for many patients. Additionally, Hammad et. al. explored the impact of financial barriers on cancer care access in Jordan. The study identified gaps in existing financial assistance programs, particularly in terms of coverage for treatment costs, transportation, and supportive care services [17]. Another study investigated the outcomes of financial assistance programs provided by the Goodwill Cancer Care Fund in Jordan. Their findings indicated that while the fund has helped alleviate financial burdens for many cancer patients, there are still significant gaps in coverage and accessibility, particularly for marginalized populations [61].
3.8. Efforts to Overcome Barriers
In 2018, KHCC mobile clinics visited the remote and poor parts of Jordan to provide initial free detection services for the most common forms of cancer. Mobile clinics indeed have been highly effective, screening more than 5000 patients per year in communities plagued by poverty and with shortages of facilities for cancer care [26]. A study showed that over 75% of refugee patients came to the KHCC with a late-stage cancer diagnosis [40]. KHCC has strategically taken initiatives towards early confirmation through awareness of warning signals and free screening programs offered. It helps lower delays in diagnosis and initiates timely treatment, and this practice has been proven to be effective in enhancing outcomes of cancer prevention. Additionally, KHCC has been very proactive in launching campaigns in mass media across Jordan, which revolve around cancer awareness and promoting early detection. These campaigns, through television, radio, and social media or via community outreach programs, have targeted the whole population, not just the high-risk segments. Studies of awareness campaigns have indicated improved knowledge and attitudes related to cancer care [52]. Various specific educational programs focus on the stigmatization of cancer, which impedes patients from accessing proper care in a timely manner. KHCC has also linked up with religious leaders, teachers, and support groups to help reinforce the message that cancer can be treated if detected early. Since then, social awareness campaigns have done much in terms of de-stigmatizing cancer to encourage patients to receive screening services [62].
Since 1997, the Goodwill Fund set up by KHCC has been of help in distributing more than 150 million dollars’ worth of treatment costs to over 25,000 financially impoverished individuals [26]. By covering cancer treatment costs, it has helped eliminate financial barriers that can impact clinical outcomes. Despite the significant impact, the rising cancer burden in Jordan and the region has made it difficult for charitable organizations to adequately meet the increasing demand for financial assistance. Effective resource utilization and partnerships with government agencies can help expand coverage. A recent agreement signed between KHCC and Jordan’s Ministry of Health in 2022 has allowed the expansion of cancer care to disadvantaged regions through a new comprehensive cancer center to the east of Amman (Aqaba), operated by KHCC and starting in 2024. The new cancer facility will provide chemotherapy, palliative care, and pathology services to cancer patients in the eastern regions of Amman that lack specialized cancer care centers. This is a major milestone in addressing disparities by facilitating access to quality cancer care. Local non-governmental organizations like the Jordan Breast Cancer Program have played an instrumental role in tackling barriers through free early detection services, financing treatment costs, and implementing awareness campaigns targeted at low-income groups. Their field presence and ties to local communities have helped overcome disparities. Non-governmental organizations have advocated and developed partnerships with stakeholders, including KHCC and government agencies, to implement national policies focused on cancer prevention and early detection, especially among disadvantaged groups. Their collaborative efforts have been crucial for impacting cancer care on a larger scale in Jordan.
4. Discussion
This study holds significance as the first study in the region to provide a comprehensive understanding of barriers to cancer care across medical services, healthcare infrastructure, workforce, quality management systems, public awareness, and socioeconomic disparities (Table 1).

Table 1.
Summary of main barriers to cancer care in Jordan.
There is an urgent need for coordinated, integrated prevention strategies encompassing lifestyle changes, vaccination against oncogenic infections, and evidence-based preventive measures tailored to the local context.
As the first of its kind focused on Jordan, the findings of our review serve as a foundation for addressing gaps in cancer care within the country. Moreover, the study’s insights are highly applicable to LMICs facing similar healthcare challenges and can be extrapolated to the Middle East and North Africa (MENA) region. While each country may have its unique challenges, several common themes emerge across the region. In the MENA region, limited health insurance coverage poses a significant barrier to accessing cancer care. Studies in LMICs have shown that a lack of comprehensive health insurance schemes results in high out-of-pocket expenses for cancer treatment, leading to financial burdens that deter patients from seeking timely care [63,64,65]. This problem is exacerbated by the absence of government-funded healthcare programs tailored to cancer prevention, screening, diagnosis, and treatment. For example, in Egypt, where health insurance coverage is limited and out-of-pocket payments are common, access to essential cancer services remains a challenge for many individuals, particularly those from low-income backgrounds [66].
The inadequacy of healthcare infrastructure is another critical barrier to cancer care in LMICs. Limited access to oncology centers, diagnostic facilities, and essential medical equipment hinders early detection and timely treatment initiation [67,68,69]. In Iraq, the healthcare infrastructure has been severely affected by years of conflict and underinvestment, resulting in limited access to specialized cancer care services, particularly in rural areas [70]. The shortage of trained healthcare professionals, including oncologists, nurses, and allied healthcare workers, poses a significant challenge to cancer care provision in LMICs [67,71,72]. In countries like Syria and Yemen, ongoing conflicts and political instability have disrupted medical education and training programs, leading to a severe scarcity of qualified personnel capable of delivering comprehensive cancer care services [73]. Disparities in access to cancer care between urban and rural areas are pervasive in LMICs. In Saudi Arabia, there is a significant disparity in cancer care access between urban and rural areas, with rural populations facing challenges related to limited healthcare infrastructure and transportation barriers [74,75]. However, efforts to improve cancer care access in rural areas have been hampered by logistical challenges and disparities in healthcare resource allocation [76].
Governmental policies and regulatory frameworks play a crucial role in shaping cancer care delivery in LMICs. However, weak governance, corruption, and a lack of political will to prioritize cancer control initiatives hinder progress in this area [77,78]. Jordan has implemented national cancer control strategies and policies to improve cancer care delivery and outcomes, despite facing challenges related to limited resources and refugee healthcare [52]. The provision of cancer care to refugees presents unique challenges in LMICs hosting large refugee populations. In Turkey, which hosts millions of Syrian refugees, efforts to provide cancer care to refugees have been hindered by language barriers, legal restrictions, and limited access to healthcare services in refugee camps [79,80]. Similarly, in Lebanon, where a large refugee population resides, integrating refugee healthcare into national cancer control programs has been challenging due to resource constraints and legal barriers [81].
With these challenges to cancer care in LMICs comes the need for proposed solutions. Primary healthcare facilities can play a pivotal role through public education, promoting cancer screening, and early detection services. Concerted efforts are required to enhance cancer screening through cost subsidies, mobile clinics, and awareness campaigns [82]. Bridging public awareness gaps will involve coordinated action across policymakers, healthcare institutions, and grassroots organizations. Cancer prevention and control campaigns should encompass risk factor mitigation, early detection promotion, and holistic survivorship support.
Targeted outreach programs are vital to increasing screening rates among underprivileged communities where late-stage diagnosis remains high. Initiatives to improve rural postings through rotations, infrastructure upgrades, and incentive schemes could help address absenteeism. In addition, targeted enrollment campaigns, premium subsidies, and engagement of civil society groups could help extend coverage to disadvantaged communities [83,84]. Eliminating disparities will require ongoing monitoring and equitable resource allocation across all population groups. Tackling rural–urban cancer disparities requires improving geographic accessibility, community engagement, and health workforce capacity. Investments in outreach services, patient transport networks, telehealth solutions, and provider training and support are warranted. Partnerships between urban centers and rural facilities can also help transfer knowledge and resources to underserved areas. A balanced approach across all regions is key for equitable cancer outcomes.
Specialized training programs and incentives are crucial to address shortages of oncologists and cancer care professionals, especially in disadvantaged regions. Refining referral pathways through centralized coordination and enhanced communication between institutions could minimize treatment delays and improve outcomes [8]. Partnerships between academic institutions and healthcare facilities can help build localized capacity through structured residency and fellowship programs. Improved retention policies, including competitive compensation, research opportunities, and global collaborations, could help address this challenge [14]. There needs to be an equitable distribution of human resources between urban and rural locales enabled through needs-based healthcare planning and infrastructure expansion [85]. This can help eliminate disparities in access to quality cancer care based on geographic location. National policies need to align with global commitments toward equitable access to affordable, quality cancer services spanning prevention, treatment, palliation, and survivorship support. Policy directives can help eliminate financial and social barriers to cancer care. Policies must integrate evidence-based survivorship care models encompassing psychosocial support, management of late effects, screening for recurrence, and wellness education. This can help improve health outcomes and quality of life after cancer treatment.
Refugees face additional impediments to treatment and cancer care in LMICs, including late-stage diagnosis, increased costs, and suboptimal medical and mental support services. Proposed services should combine medical, mental health, complementary medicine, community/religious engagement, and refugee cancer patient peer support aspects to provide appropriately holistic support following primary treatment that cancer centers in high-income nations may take for granted. In addition, to address the barrier of lacking structured programs for psychosocial support in cancer care facilities, we propose the establishment of comprehensive psychosocial oncology programs that aim to provide emotional and spiritual support to both patients and their families, enhancing their quality of life and ensuring optimal treatment outcomes. Dedicated social workers, collaborating closely with healthcare management teams, can effectively address the emotional and social needs of patients and their families, thereby facilitating access to treatment and improving treatment compliance.
Digital technologies such as telemedicine, mHealth applications, and connected medical devices can help make access to quality cancer care services easier, especially for patients living in remote areas. Tele-oncology models might improve results by enabling remote consultations, online tumor boards, and remote monitoring in patients undergoing chemotherapy. Scaling such models, though, requires cross-sector coordination and the ability to develop digital infrastructure with an urgent need to design and implement national guidelines for screening common cancers that should be differentiated according to the local disease burden and resource context [86]. This can significantly enhance early detection. Access to free public education programs aimed at making the community aware of common cancer symptoms and benefits associated with early illness detection can also more significantly contribute because they will help enhance screening adoption rates in order to downstage cancer diagnosis. The vision should move from a short-term, disease-based care model to multidisciplinary patient-centered care throughout the cancer continuum that involves health promotion, prevention, end-of-life care, and survivorship based on individual needs [87]. Grassroots-based community engagement models are crucial as they enable local leaders or advocates for health to gain the capacities related to campaigning on reasons around cancer prevention and control and can accelerate progress in capacity building. Comprehensive monitoring and evaluation systems are also critical for identifying gaps in care quality management and outcomes. The adoption of unified performance indicators could better guide quality enhancement initiatives across Jordan’s cancer care system. We also propose to have simplified metrics for the objective evaluation of the quality of care so that the results can be shared to identify gaps and acquire best practices.
Advocating for broadening the scope of financial assistance is of paramount importance. Prior studies have highlighted that the problem of financial obstacles to various diseases has raised the need for comprehensive policies related to public healthcare needs [17,60]. A strategic recommendation would be to improve partnerships between government and non-governmental organizations such as the KHCC and the Jordanian Breast Cancer Program, which could help and support government programs. These partnerships can provide cancer patients with comprehensive financial support for cancer care [88]. It is also necessary to monitor and assess financial aid programs continuously in order to identify their effectiveness, and to improve financial assistance mechanisms to keep them updated with the evolving demands from the population and health system [89,90].
The comprehensive cancer care infrastructure in Jordan in the 1990s was almost non-existent, with services scattered throughout Amman, and there were no initiatives for prevention or early detection [52]. This resulted in late diagnosis and adverse outcomes. The year 1997 marked the creation of the KHCC, which encouraged radical changes in cancer care by setting up a full-fledged cancer facility that provided equitable and affordable access to quality diagnosis and treatment as well as palliative care corresponding with worldwide standards [62]. KHCC has been an innovative platform to elevate national principles of cancer treatment in Jordan as the standard-setting center. KHCC’s patient-centered approach, interdisciplinary model of care delivery, and comprehensiveness of services, along with its dedication to innovation, have provided care to thousands of patients over the last two decades. For instance, it led critical countrywide programs like the Jordan Breast Cancer Program in 2003 that substantially contributed towards breast cancer downstaging via diagnosis and improved results [91]. In 2006, KHCC received international accreditation by Joint Commission International (JCI) as a symbol of global safety and quality; in 2019 KHCC earned Magnet accreditation, which has been linked to superior clinical results; and in 2020 KHCC received AAHRPP accreditation for quality research and its protection of participants.
KHCC is on a continuous upgrade path, constantly adding the relevant tech to its arsenal, like intraoperative MRI neurosurgery rooms, numerous linear accelerators, and imaging equipment such as positron emission tomography/computed tomography (PET/CT) for a complete services package [92,93]. Stereotactic radiosurgery has been one of the most advanced techniques that emerged in the field of radiation oncology. KHCC has also been recognized as a training center for top-flight companies such as Elekta and Philips in new radiotherapy technologies. According to the latest Jordan Cancer Registry report, 10,000 new cancer cases were registered at KHCC in 2019, of which 75.9% were Jordanian citizens, representing substantial national reach [2]. Over 20% of cancer patients came from neighboring countries, reflecting KHCC’s emergence as a reputable tertiary care destination in the region despite local and regional challenges [94]. Managing an international population presents unique challenges but also allows experience-sharing with global centers.
Drawing upon lessons learned from Jordan, a sustainable cancer care system in LMICs can be designed to address key challenges while maximizing available opportunities (Table 2).
Table 2.
Proposed solutions to address barriers to cancer care in low-middle-income countries (LMICs).
A comprehensive healthcare delivery model would integrate primary care services with specialized cancer centers to ensure seamless patient management and coordinated multidisciplinary care [95]. Equitable access can be achieved by strategically allocating healthcare facilities and resources based on population needs, leveraging mobile clinics and telemedicine to bridge geographical gaps and improve access [49,94].
Capacity building involves investing in training and retaining a skilled healthcare workforce through collaborative partnerships with international institutions and tailored educational programs [9,12]. Some LMICs have established cancer registries at the federal level; however, the quality control mechanisms of these registries are extremely variable, and quite often data is either missing or lags behind current data entry mechanisms and long term outcomes, which leads to considerable delays in updating the data and would preclude accurate mortality or morbidity analysis. In addition, unless the burden of each cancer type and subtype is known, it is hard to allocate the appropriate resources for the prevention or treatment of the specific types of cancer. The need for accurate data of cancer cases in a country is imperative to develop cancer control programs and screening guidelines [96,97].
Financial support strategies include strengthening existing government initiatives and non-governmental partnerships to expand financial assistance programs, ensuring inclusivity in health insurance coverage and providing targeted support for vulnerable populations [26,44]. In addition, prioritizing prevention and early detection entails evidence-based public education campaigns and subsidized screening services [82,98]. Quality improvement initiatives would establish robust monitoring and benchmarking systems to track care quality across healthcare institutions, implementing standardized performance metrics and best practices informed by international standards and research evidence [11,17].
Medical training and research efforts would foster a culture of research infrastructure and collaborative partnerships between academia, healthcare institutions, and industry stakeholders [14,85]. Community engagement strategies would involve engaging local communities and grassroots organizations in cancer prevention and control efforts through culturally sensitive interventions and community-based participatory research approaches [45,46]. Additionally, ensuring comprehensive palliative care services integrated within the cancer care continuum is crucial. This includes addressing the physical, psychosocial, and spiritual needs of patients and their families, providing symptom management, pain relief, and end-of-life care [99,100]. By implementing evidence-based strategies within this framework, Jordan can overcome existing challenges and optimize its cancer care system to ensure equitable access to high-quality care for all residents, while acknowledging and addressing resource constraints and limitations.
This review possesses several strengths that enhance its significance and credibility, as it represents the first comprehensive review focused specifically on Jordan, providing a unique perspective on the country’s cancer care barriers. Moreover, its findings hold relevance beyond Jordan, serving as a valuable resource for other resource-limited LMICs confronting similar healthcare challenges, particularly in the MENA region. However, the study is not without its limitations. Potential publication bias may exist due to the reliance on the available literature, and the exclusion of non-English studies may limit the generalizability of the findings. The focus on barriers alone may overlook potential facilitators, while contextual differences between countries may restrict the direct applicability of lessons learned from Jordan to other countries. Additionally, the reliance on secondary data sources may constrain the depth of analysis and the ability to capture real-time changes in the healthcare landscape.
5. Conclusions
Key barriers to cancer care include shortages of specialists, maldistribution of facilities, financial constraints, low cancer awareness, and socioeconomic factors. To build equitable cancer care, strategies like investments, policy changes, and partnerships between the public and private sectors are needed. Research should focus on expanding specialized human resources and creating healthcare facilities. National cancer control plans should use technology to initiate awareness campaigns. Lessons learned from Jordan can inform strategies for improving cancer care access, quality, and outcomes in other thriving LMICs.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/cancers16061117/s1, Supplementary file summarizing adopted methodology for database search strategy.
Author Contributions
Conceptualization, R.M., M.A.-H., A.A.-I., A.A.-O., O.S., H.A.-R. and A.H.M.; methodology, R.M.; software, R.M. and A.A.-I.; validation, R.M., M.A.-H., A.A.-I. and H.A.-R.; formal analysis, R.M., A.A.-I. and H.A.-R.; writing—original draft preparation, R.M., A.A.-I. and A.H.M.; writing—review and editing, R.M., M.A.-H., A.A.-I., O.S., A.A.-O. and A.H.M.; visualization, H.A.-R.; supervision, A.H.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding authors. The data are not publicly available due to privacy.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Abuelhaija, Y.; Mustafa, A.; Al-Bataineh, H.A.; Alzaqh, M.; Mustafa, A.; Bawa’neh, F.; Alomari, M.; Alkhader, A. A systematic review on the healthcare system in Jordan: Strengths, weaknesses, and opportunities for improvement. World J. Adv. Res. Rev. 2023, 18, 1393–1396. [Google Scholar] [CrossRef]
- Department of Statistics: Jordan Annual Statistic Book—2017. 2017. Available online: https://dosweb.dos.gov.jo/product-category/statistical-yearbook/ (accessed on 7 February 2024).
- Jordan Cancer Registry: Cancer incidence in Jordan. 2018. Available online: https://moh.gov.jo/ebv4.0/root_storage/ar/eb_list_page/التقرير_السنوي_لاصابات_السرطان_المسجلة_في_الاردن_لعام_2018.pdf (accessed on 7 February 2024).
- World Health Organization: Global Health Observatory: Jordan Statistics Summary (2024). Available online: https://data.who.int/countries/400 (accessed on 7 February 2024).
- The National Strategy for Health Sector in Jordan, World Health Organization, 2015–2019. Available online: http://www.nationalplanningcycles.org/sites/default/files/planning_cycle_repository/jordan/jordan_national_health_sector_strategy_2015-2019_.pdf (accessed on 7 February 2024).
- Halasa, Y.A.; Zeng, W.; Chappy, E.; Shepard, D.S. Value and impact of international hospital accreditation: A case study from Jordan. East. Mediterr. Health J. 2015, 21, 90–99. [Google Scholar] [CrossRef]
- Kronfol, N.M. Access and barriers to health care delivery in Arab countries: A review. East. Mediterr. Health J. 2012, 18, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- Ajlouni, M.T.; Dawani, H.; Diab, S.M. Home Health Care (HHC) Managers Perceptions About Challenges and Obstacles that Hinder HHC Services in Jordan. Glob. J. Health Sci. 2015, 7, 121–129. [Google Scholar] [CrossRef]
- Lewando Hundt, G.; Alzaroo, S.; Hasna, F.; Alsmeiran, M. The provision of accessible, acceptable health care in rural remote areas and the right to health: Bedouin in the North East region of Jordan. Soc. Sci. Med. 2012, 74, 36–43. [Google Scholar] [CrossRef]
- Khatatbeh, M. Factors Associated with High Turnover of Jordanian Physicians in Rural Areas: A Sequential Exploratory Mixed Method Study. Ph.D. Thesis, Curtin University, Bentley, Australia, 2013. Available online: https://espace.curtin.edu.au/handle/20.500.11937/348 (accessed on 7 February 2024).
- Khoury, S.A.; Mawajdeh, S. Performance of health providers in primary health care services in Jordan. East. Mediterr. Health J. 2004, 10, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Obeidat, N.A.; Habashneh, M.A.; Shihab, R.A.; Hawari, F.I. Are Jordanian primary healthcare practitioners fulfilling their potential in cancer prevention and community health? Findings from a cross-sectional survey. BMJ Open 2017, 7, e015269. [Google Scholar] [CrossRef] [PubMed]
- Al Zoubi, A.M.; Saifan, A.R.; Alrimawi, I.; Aljabery, M.A. Challenges facing oncology nurses in Jordan: A qualitative study. Int. J. Health Plan. Manag. 2020, 35, 247–261. [Google Scholar] [CrossRef]
- Abdel-Razeq, H.; Barbar, M.; Shamieh, O.; Mansour, A. Oncology Medical Training and Practice: Managing Jordan’s Brain Drain Through Brain Train-The King Hussein Cancer Center Experience. JCO Glob. Oncol. 2020, 6, 1041–1045. [Google Scholar] [CrossRef]
- Abu-Kharmeh, S.S. Evaluating the Quality of Health Care Services in the Hashemite Kingdom of Jordan. Int. J. Bus. Manag. 2012, 7, 195. [Google Scholar]
- Ajlouni, M.T. Social determinants of health in selected slum areas in Jordan: Challenges and policy directions. Int. J. Health Plann. Manag. 2016, 31, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Hammad, E.A. The Use of Economic Evidence to Inform Drug Pricing Decisions in Jordan. Value Health 2016, 19, 233–238. [Google Scholar] [CrossRef]
- Saab, M.M.; FitzGerald, S.; Noonan, B.; Kilty, C.; Collins, A.; Lyng, Á.; Kennedy, U.; O’Brien, M.; Hegarty, J. Promoting lung cancer awareness, help-seeking and early detection: A systematic review of interventions. Health Promot. Int. 2021, 36, 1656–1671. [Google Scholar] [CrossRef] [PubMed]
- Al Qadire, M.; Aljezawi, M.; Al-Shdayfat, N. Cancer Awareness and Barriers to Seeking Medical Help Among Syrian Refugees in Jordan: A Baseline Study. J. Cancer Educ. 2019, 34, 19–25. [Google Scholar] [CrossRef]
- Nakkash, R.; Khader, Y.; Chalak, A.; Abla, R.; Abu-Rmeileh, N.M.E.; Mostafa, A.; Jawad, M.; Lee, J.H.; Salloum, R.G. Prevalence of cigarette and waterpipe tobacco smoking among adults in three Eastern Mediterranean countries: A cross-sectional household survey. BMJ Open 2022, 12, e055201. [Google Scholar] [CrossRef] [PubMed]
- Burki, T.K. Tobacco control in Jordan. Lancet Respir. Med. 2019, 7, 386. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Razeq, H.; Mansour, A.; Bater, R. Trends, Patterns, and Treatment Outcomes of Cancer Among Older Patients in Jordan: A Retrospective Analysis of National Cancer Registry and Institutional Outcome Data. JCO Glob. Oncol. 2020, 6, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Al-Mousa, D.S.; Alakhras, M.; Hossain, S.Z.; Al-Sa’di, A.G.; Al Hasan, M.; Al-Hayek, Y.; Brennan, P.C. Knowledge, Attitude and Practice Around Breast Cancer and Mammography Screening Among Jordanian Women. Breast Cancer Targets Ther. 2020, 12, 231–242. [Google Scholar] [CrossRef]
- Arafa, M.A.; Rabah, D.M.; Wahdan, I.H. Awareness of general public towards cancer prostate and screening practice in Arabic communities: A comparative multi-center study. Asian Pac. J. Cancer Prev. 2012, 13, 4321–4326. [Google Scholar] [CrossRef]
- Taha, H.; Jaghbeer, M.A.; Shteiwi, M.; AlKhaldi, S.; Berggren, V. Knowledge and Perceptions about Colorectal Cancer in Jordan. Asian Pac. J. Cancer Prev. 2015, 16, 8479–8486. [Google Scholar] [CrossRef][Green Version]
- Khader, Y.; Al Nsour, M.; Abu Khudair, S.; Saad, R.; Tarawneh, M.R.; Lami, F. Strengthening Primary Healthcare in Jordan for Achieving Universal Health Coverage: A Need for Family Health Team Approach. Healthcare 2023, 11, 2993. [Google Scholar] [CrossRef] [PubMed]
- Hagen-Zanker, J.; Ulrichs, M.; Holmes, R. What are the effects of cash transfers for refugees in the context of protracted displacement? Findings from Jordan. Int. Soc. Secur. Rev. 2018, 71, 57–77. [Google Scholar] [CrossRef]
- Krimphove, M.J.; Cole, A.P.; Fletcher, S.A.; Harmouch, S.S.; Berg, S.; Lipsitz, S.R.; Sun, M.; Nabi, J.; Nguyen, P.L.; Hu, J.C.; et al. Evaluation of the contribution of demographics, access to health care, treatment, and tumor characteristics to racial differences in survival of advanced prostate cancer. Prostate Cancer Prostatic Dis. 2019, 22, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Halsey, K.; Alarood, S.; Nawaiseh, M.; Mir, G. An exploration of politicized healthcare access for Syrian and Palestinian refugees in Jordan: A question of equity. Int. J. Migr. Health Soc. Care 2022, 18, 51–65. [Google Scholar] [CrossRef]
- World Bank Report. 2019. Available online: https://data.worldbank.org/indicator/SP.RUR.TOTL.ZS?locations=JO (accessed on 7 February 2024).
- Rehr, M.; Shoaib, M.; Ellithy, S.; Okour, S.; Ariti, C.; Ait-Bouziad, I.; van den Bosch, P.; Deprade, A.; Altarawneh, M.; Shafei, A.; et al. Prevalence of non-communicable diseases and access to care among non-camp Syrian refugees in northern Jordan. Confl. Health 2018, 12, 33. [Google Scholar] [CrossRef] [PubMed]
- Al Barmawi, M.; Al Hadid, L.A.; Al Kharabshah, M. Reasons for delay in seeking healthcare among women with acute coronary syndrome from rural and urban areas in Jordan. Health Care Women Int. 2022, 43, 293–308. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, P.; Odusina, E.K.; Ahinkorah, B.O.; Kota, K.; Yaya, S. Health insurance coverage and maternal healthcare services utilization in Jordan: Evidence from the 2017–18 Jordan demographic and health survey. Arch. Public Health 2021, 79, 81. [Google Scholar] [CrossRef]
- Belita, A.; Mbindyo, P.; English, M. Absenteeism amongst health workers—Developing a typology to support empiric work in low-income countries and characterizing reported associations. Hum. Resour. Health 2013, 11, 34. [Google Scholar] [CrossRef]
- Gharaibeh, A.A.; Alhamad, M.N.; Al-Hassan, D.A.; Abumustafa, N.I. The impact of the spatial configuration of socioeconomic services on rural-urban dependencies in Northern Jordan. GeoJournal 2022, 87, 4475–4490. [Google Scholar] [CrossRef]
- Heus, K.; Sartawi, T. The Realization of the Right to Health for Refugees in Jordan. In The Right to Health: A Multi-Country Study of Law, Policy and Practice; Toebes, B., Ferguson, R., Markovic, M.M., Nnamuchi, O., Eds.; T.M.C. Asser Press: The Hague, The Netherlands, 2014; pp. 193–229. [Google Scholar] [CrossRef]
- Al-Ibraheem, A.; Abdlkadir, A.S.; Mohamedkhair, A.; Mikhail-Lette, M.; Al-Qudah, M.; Paez, D.; Mansour, A.H. Cancer diagnosis in areas of conflict. Front. Oncol. 2022, 12, 1087476. [Google Scholar] [CrossRef]
- United Nations High Commissioner for Refugees: Syrian Refugee Response. Available online: https://data.unhcr.org/en/situations/syria/location/36 (accessed on 7 February 2024).
- Abdel-Razeq, H.; Tamimi, F.; Abdel-Razeq, N.; El-Atrash, M.; Sharaf, B.; Mustafa, R.; Mansour, R.; Bater, R. Late presentation and suboptimal treatment of breast cancer among Syrian refugees: A retrospective study. J. Int. Med. Res. 2021, 49, 3000605211018448. [Google Scholar] [CrossRef]
- Mansour, A.; Al-Omari, A.; Sultan, I. Burden of Cancer Among Syrian Refugees in Jordan. J. Glob. Oncol. 2018, 4, 1–6. [Google Scholar] [CrossRef]
- Guo, P.; Alajarmeh, S.; Alarjeh, G.; Alrjoub, W.; Al-Essa, A.; Abusalem, L.; Giusti, A.; Mansour, A.H.; Sullivan, R.; Shamieh, O.; et al. Providing person-centered palliative care in conflict-affected populations in the Middle East: What matters to patients with advanced cancer and families including refugees? Front. Oncol. 2023, 13, 1097471. [Google Scholar] [CrossRef] [PubMed]
- El Arab, R.; Sagbakken, M. Healthcare services for Syrian refugees in Jordan: A systematic review. Eur. J. Public Health 2018, 28, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, P.B.; Cheaib, J.G.; Aziz, S.A.; Abrahim, O.; Woodman, M.; Khalifa, A.; Jang, M.; Mateen, F.J. Cancer in Syrian refugees in Jordan and Lebanon between 2015 and 2017. Lancet Oncol. 2020, 21, e280–e291. [Google Scholar] [CrossRef] [PubMed]
- Marzouk, M.; Kelley, M.; Fadhil, I.; Slama, S.; Longuere, K.S.; Ariana, P.; Carson, G.; Marsh, V. “If I have a cancer, it is not my fault I am a refugee”: A qualitative study with expert stakeholders on cancer care management for Syrian refugees in Jordan. PLoS ONE 2019, 14, e0222496. [Google Scholar] [CrossRef] [PubMed]
- Ay, M.; Arcos González, P.; Castro Delgado, R. The Perceived Barriers of Access to Health Care Among a Group of Non-camp Syrian Refugees in Jordan. Int. J. Health Serv. 2016, 46, 566–589. [Google Scholar] [CrossRef]
- Alawa, J.; Alhalabi, F.; Khoshnood, K. Breast cancer management among refugees and forcibly displaced populations: A call to action. Curr. Breast Cancer Rep. 2019, 11, 129–135. [Google Scholar] [CrossRef]
- Thøgersen, H. Immigrants in Norway with Cancer: Stage at Diagnosis, Treatment and Surviva. Ph.D. Thesis, University of Oslo, Oslo, Norway, 2019. Available online: https://www.duo.uio.no/handle/10852/67678 (accessed on 27 February 2024).
- Abdul-Khalek, R.A.; Guo, P.; Sharp, F.; Gheorghe, A.; Shamieh, O.; Kutluk, T.; Fouad, F.; Coutts, A.; Aggarwal, A.; Mukherji, D.; et al. The economic burden of cancer care for Syrian refugees: A population-based modelling study. Lancet Oncol. 2020, 21, 637–644. [Google Scholar] [CrossRef]
- Lecadet, C. Refugee Politics: Self-Organized ‘Government’ and Protests in the Agamé Refugee Camp (2005–13). J. Refug. Stud. 2016, 29, fev021. [Google Scholar] [CrossRef]
- Eiset, A.H.; Aoun, M.P.; Stougaard, M.; Gottlieb, A.G.; Haddad, R.S.; Frydenberg, M.; Naja, W.J. The association between long-distance migration and PTSD prevalence in Syrian refugees. BMC Psychiatry 2022, 22, 363. [Google Scholar] [CrossRef]
- Steel, Z.; Silove, D.; Phan, T.; Bauman, A. Long-term effect of psychological trauma on the mental health of Vietnamese refugees resettled in Australia: A population-based study. Lancet 2002, 360, 1056–1062. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Razeq, H.; Attiga, F.; Mansour, A. Cancer care in Jordan. Hematol./Oncol. Stem Cell Ther. 2015, 8, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Böge, K.; Karnouk, C.; Hahn, E.; Demir, Z.; Bajbouj, M. On Perceived Stress and Social Support: Depressive, Anxiety and Trauma-Related Symptoms in Arabic-Speaking Refugees in Jordan and Germany. Front. Public Health 2020, 8, 239. [Google Scholar] [CrossRef] [PubMed]
- Wells, R.; Steel, Z.; Abo-Hilal, M.; Hassan, A.H.; Lawsin, C. Psychosocial concerns reported by Syrian refugees living in Jordan: Systematic review of unpublished needs assessments. Br. J. Psychiatry 2016, 209, 99–106. [Google Scholar] [CrossRef]
- Tahoun, L.A.; Khatib, Y.; Farfora, H.; Ghoul, S.; Abdallah, A.; Abdarrahman, R.; Jarrah, R.A.; Mansour, R.; Tamimi, Z.A.; Ammar, K.; et al. Mobile Mammography in Lower-Middle–Income Country, Jordan Experience. J. Glob. Oncol. 2018, 4 (Suppl. S2), 31s. [Google Scholar] [CrossRef]
- Rana, D.; Madi, J.; Mahmoud, S.; Amal, A.-O.; Nedal, A.-R. Unravelling the predictors of late cancer presentation and diagnosis in Jordan: A cross-sectional study of patients with lung and colorectal cancers. BMJ Open 2023, 13, e069529. [Google Scholar] [CrossRef]
- Hamadeh, T.; Moonesar, I.A. Financial Restrictions Limit Early Breast Cancer Screening: The Case of Jordan. J. Oncol. 2022, 2, 1037. [Google Scholar]
- Halasa-Rappel, Y.; Fardous, T.; Jrasat, M.; Al-Halaseh, I.; Abu-Shaer, M.; Hijazeen, R.; Shepard, D.S. Actuarial cost and fiscal impact of expanding the Jordan Civil Insurance Programme for health coverage to vulnerable citizens. East. Mediterr. Health J. 2020, 26, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Yabroff, K.R.; Reeder-Hayes, K.; Zhao, J.; Halpern, M.T.; Lopez, A.M.; Bernal-Mizrachi, L.; Collier, A.B.; Neuner, J.; Phillips, J.; Blackstock, W.; et al. Health Insurance Coverage Disruptions and Cancer Care and Outcomes: Systematic Review of Published Research. J. Natl. Cancer Inst. 2020, 112, 671–687. [Google Scholar] [CrossRef]
- Al-Qadi, N.; Lozi, B. The Impact of Middle East Conflict on the Jordanian Economy. Int. J. Acad. Res. Bus. Soc. Sci. 2017, 7, 331–341. [Google Scholar] [CrossRef]
- Rihani, R.; Jeha, S.; Nababteh, M.; Rodriguez-Galindo, C.; Mansour, A.; Sultan, I. The burden and scope of childhood cancer in displaced patients in Jordan: The King Hussein Cancer Center and Foundation Experience. Front. Oncol. 2023, 13, 1112788. [Google Scholar] [CrossRef]
- Moe, J.L.; Pappas, G.; Murray, A. Transformational leadership, transnational culture and political competence in globalizing health care services: A case study of Jordan’s King Hussein Cancer Center. Glob. Health 2007, 3, 11. [Google Scholar] [CrossRef]
- Hussien, M.; Azage, M. Barriers and Facilitators of Community-Based Health Insurance Policy Renewal in Low- and Middle-Income Countries: A Systematic Review. Clin. Outcomes Res. 2021, 13, 359–375. [Google Scholar] [CrossRef] [PubMed]
- Rahman, T.; Gasbarro, D.; Alam, K. Financial risk protection from out-of-pocket health spending in low- and middle-income countries: A scoping review of the literature. Health Res. Policy Syst. 2022, 20, 83. [Google Scholar] [CrossRef] [PubMed]
- Udayakumar, S.; Solomon, E.; Isaranuwatchai, W.; Rodin, D.L.; Ko, Y.J.; Chan, K.K.W.; Parmar, A. Cancer treatment-related financial toxicity experienced by patients in low- and middle-income countries: A scoping review. Support. Care Cancer 2022, 30, 6463–6471. [Google Scholar] [CrossRef]
- Omotoso, O.; Teibo, J.O.; Atiba, F.A.; Oladimeji, T.; Paimo, O.K.; Ataya, F.S.; Batiha, G.E.; Alexiou, A. Addressing cancer care inequities in sub-Saharan Africa: Current challenges and proposed solutions. Int. J. Equity Health 2023, 22, 189. [Google Scholar] [CrossRef] [PubMed]
- Olayemi, E.; Asare, E.V.; Benneh-Akwasi Kuma, A.A. Guidelines in lower-middle income countries. Br. J. Haematol. 2017, 177, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Andrews, J.; Kishore, S.; Panjabi, R.; Stuckler, D. Comparative performance of private and public healthcare systems in low-and middle-income countries: A systematic review. PLoS Med. 2012, 9, e1001244. [Google Scholar] [CrossRef] [PubMed]
- Datta, N.R.; Rogers, S.; Bodis, S. Challenges and Opportunities to Realize “The 2030 Agenda for Sustainable Development” by the United Nations: Implications for Radiation Therapy Infrastructure in Low- and Middle-Income Countries. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 918–933. [Google Scholar] [CrossRef]
- Al-Mosawi, A.J. Iraq healthcare system: An update. Lupine Online J. Med. Sci. 2020, 4, 404–411. [Google Scholar]
- Hoyler, M.; Finlayson, S.R.; McClain, C.D.; Meara, J.G.; Hagander, L. Shortage of doctors, shortage of data: A review of the global surgery, obstetrics, and anesthesia workforce literature. World J. Surg. 2014, 38, 269–280. [Google Scholar] [CrossRef]
- Adynski, G.I.; Morgan, L.L. A systematic review of the strategies to address health worker shortage in rural and remote areas of low-and middle-income countries. Online J. Rural. Nurs. Health Care 2021, 21, 167–207. [Google Scholar] [CrossRef]
- Fares, J.; Fares, M.Y.; Fares, Y. Medical schools in times of war: Integrating conflict medicine in medical education. Surg. Neurol. Int. 2020, 11, 5. [Google Scholar] [CrossRef]
- Alwadei, A.; Alnaami, I.; Alenazy, K.; Marei, A.; BaHammam, L.O.; Nasser, S.; Alswilem, A.M.; Maklad, A.; Shehata, S.F.; Alqahtani, M.S. Impact of rural vs. urban residence on survival rates of patients with glioblastoma: A tertiary care center experience. Brain Sci. 2022, 12, 1186. [Google Scholar] [CrossRef]
- Al-Ahmadi, K.; Al-Zahrani, A.; Al-Ahmadi, S. Spatial accessibility to cancer care facilities in Saudi Arabia. In Proceedings of the Esri Health GIS Conference, Cambridge, MA, USA, 14–16 October 2013. [Google Scholar]
- Gollapalli, M.; Al-Jaber, E.; Selham, J.; Al-awazem, W.; Al-Sayoud, Z.; Al-Qassab, S. Saudi rural breast cancer prevention framework. In Proceedings of the 2015 International Conference on Cloud Computing (ICCC), Riyadh, Saudi Arabia, 26–29 April 2015; pp. 1–8. [Google Scholar]
- Sahloul, E.; Salem, R.; Alrez, W.; Alkarim, T.; Sukari, A.; Maziak, W.; Atassi, M.B. Cancer care at times of crisis and war: The Syrian example. J. Glob. Oncol. 2017, 3, 338–345. [Google Scholar] [CrossRef]
- Skelton, M.; Alameddine, R.; Saifi, O.; Hammoud, M.; Zorkot, M.; Daher, M.; Charafeddine, M.; Temraz, S.; Shamseddine, A.; Mula-Hussain, L. High-cost cancer treatment across borders in conflict zones: Experience of Iraqi patients in Lebanon. JCO Glob. Oncol. 2020, 6, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Erenoğlu, R.; Yaman Sözbir, Ş. The effect of health education given to Syrian refugee women in their own language on awareness of breast and cervical cancer, in Turkey: A randomized controlled trial. J. Cancer Educ. 2020, 35, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Kutluk, T.; Koç, M.; Öner, İ.; Babalıoğlu, İ.; Kirazlı, M.; Aydın, S.; Ahmed, F.; Köksal, Y.; Tokgöz, H.; Duran, M. Cancer among syrian refugees living in Konya Province, Turkey. Confl. Health 2022, 16, 3. [Google Scholar] [CrossRef] [PubMed]
- Alawa, J.; Hamade, O.; Alayleh, A.; Fayad, L.; Khoshnood, K. Cancer awareness and barriers to medical treatment among Syrian refugees and Lebanese citizens in Lebanon. J. Cancer Educ. 2020, 35, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Miles, A.; Cockburn, J.; Smith, R.A.; Wardle, J. A perspective from countries using organized screening programs. Cancer 2004, 101, 1201–1213. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Lee, J.-Y.; Sridhar, S.; Mittal, V.; McCallister, K.; Singal, A.G. Improving cancer outreach effectiveness through targeting and economic assessments: Insights from a randomized field experiment. J. Mark. 2020, 84, 1–27. [Google Scholar] [CrossRef]
- Levano, W.; Miller, J.W.; Leonard, B.; Bellick, L.; Crane, B.E.; Kennedy, S.K.; Haslage, N.M.; Hammond, W.; Tharpe, F.S. Public education and targeted outreach to underserved women through the National Breast and Cervical Cancer Early Detection Program. Cancer 2014, 120, 2591–2596. [Google Scholar] [CrossRef] [PubMed]
- AlDossary, S.; Martin-Khan, M.G.; Bradford, N.K.; Armfield, N.R.; Smith, A.C. The Development of a Telemedicine Planning Framework Based on Needs Assessment. J. Med. Syst. 2017, 41, 74. [Google Scholar] [CrossRef]
- Hunter, N.; Dempsey, N.; Tbaishat, F.; Jahanzeb, M.; Al-Sukhun, S.; Gralow, J.R. Resource-Stratified Guideline-Based Cancer Care Should Be a Priority: Historical Context and Examples of Success. Am. Soc. Clin. Oncol. Educ. Book 2020, 40, 217–226. [Google Scholar] [CrossRef]
- Young, A.M.; Charalambous, A.; Owen, R.I.; Njodzeka, B.; Oldenmenger, W.H.; Alqudimat, M.R.; So, W.K.W. Essential oncology nursing care along the cancer continuum. Lancet Oncol. 2020, 21, e555–e563. [Google Scholar] [CrossRef]
- Tan, S.C.; Poh, W.T.; Yong, A.C.H.; Chua, E.W.; Ooi, J.; Mahmud, R.; Thiagarajan, M.; Stanslas, J. Challenges and Strategies for Improving Access to Cancer Drugs in Malaysia: Summary of Opinions Expressed at the 2nd MACR International Scientific Conference 2022. Cancer Manag. Res. 2023, 15, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Zafar, S.Y.; Peppercorn, J.M. Patient Financial Assistance Programs: A Path to Affordability or a Barrier to Accessible Cancer Care? J. Clin. Oncol. 2017, 35, 2113–2116. [Google Scholar] [CrossRef]
- Yezefski, T.; Schwemm, A.; Lentz, M.; Hone, K.; Shankaran, V. Patient assistance programs: A valuable, yet imperfect, way to ease the financial toxicity of cancer care. Semin. Hematol. 2018, 55, 185–188. [Google Scholar] [CrossRef]
- Abdel-Razeq, H.; Mansour, A.; Jaddan, D. Breast Cancer Care in Jordan. JCO Glob. Oncol. 2020, 6, 260–268. [Google Scholar] [CrossRef]
- Al-Ibraheem, A.; Mohamedkhair, A. Current status of theranostics in Jordan. Nucl. Med. Mol. Imaging 2019, 53, 7–10. [Google Scholar] [CrossRef]
- Al-Ibraheem, A.; Abdlkadir, A.; Albalooshi, B.; Muhsen, H.; Haidar, M.; Omar, Y.; Usmani, S.; al Kandari, F. Theranostics in the Arab world; achievements & challenges. Jordan Med. J. 2022, 56. [Google Scholar]
- Khatib, S.; Nimri, O. General Oncology Care in Jordan. In Cancer in the Arab World; Springer: Singapore, 2022; pp. 83–98. [Google Scholar] [CrossRef]
- Chubak, J.; Tuzzio, L.; Hsu, C.; Alfano, C.M.; Rabin, B.A.; Hornbrook, M.C.; Spegman, A.; Von Worley, A.; Williams, A.; Nekhlyudov, L. Providing care for cancer survivors in integrated health care delivery systems: Practices, challenges, and research opportunities. J. Oncol. Pract. 2012, 8, 184–189. [Google Scholar] [CrossRef]
- Curado, M.P.; Voti, L.; Sortino-Rachou, A.M. Cancer registration data and quality indicators in low and middle income countries: Their interpretation and potential use for the improvement of cancer care. Cancer Causes Control 2009, 20, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Znaor, A.; Cueva, P.; Korir, A.; Swaminathan, R.; Ullrich, A.; Wang, S.A.; Parkin, D.M. Planning and Developing Population-Based Cancer Registration in Low-or Middle-Income Settings. 2021. Available online: https://europepmc.org/article/med/33502836 (accessed on 27 February 2024).
- Abdulrahim, S.; Jawad, M. Socioeconomic differences in smoking in Jordan, Lebanon, Syria, and Palestine: A cross-sectional analysis of national surveys. PLoS ONE 2018, 13, e0189829. [Google Scholar] [CrossRef] [PubMed]
- Stjernswärd, J.; Ferris, F.D.; Khleif, S.N.; Jamous, W.; Treish, I.M.; Milhem, M.; Bushnaq, M.; Al Khateib, A.; Al Shtiat, M.N.; Wheeler, M.S. Jordan palliative care initiative: A WHO Demonstration Project. J. Pain Symptom Manag. 2007, 33, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Shamieh, O.; Kutluk, T.; Fouad, F.M.; Sullivan, R.; Mansour, A. Editorial: Cancer care in areas of conflict. Front. Oncol. 2023, 13, 1301552. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).