
A Risk Stratification System in Myeloma Patients with Autologous Stem Cell Transplantation

 ,
,  , ,
, ,  ,
,  , ,
, , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
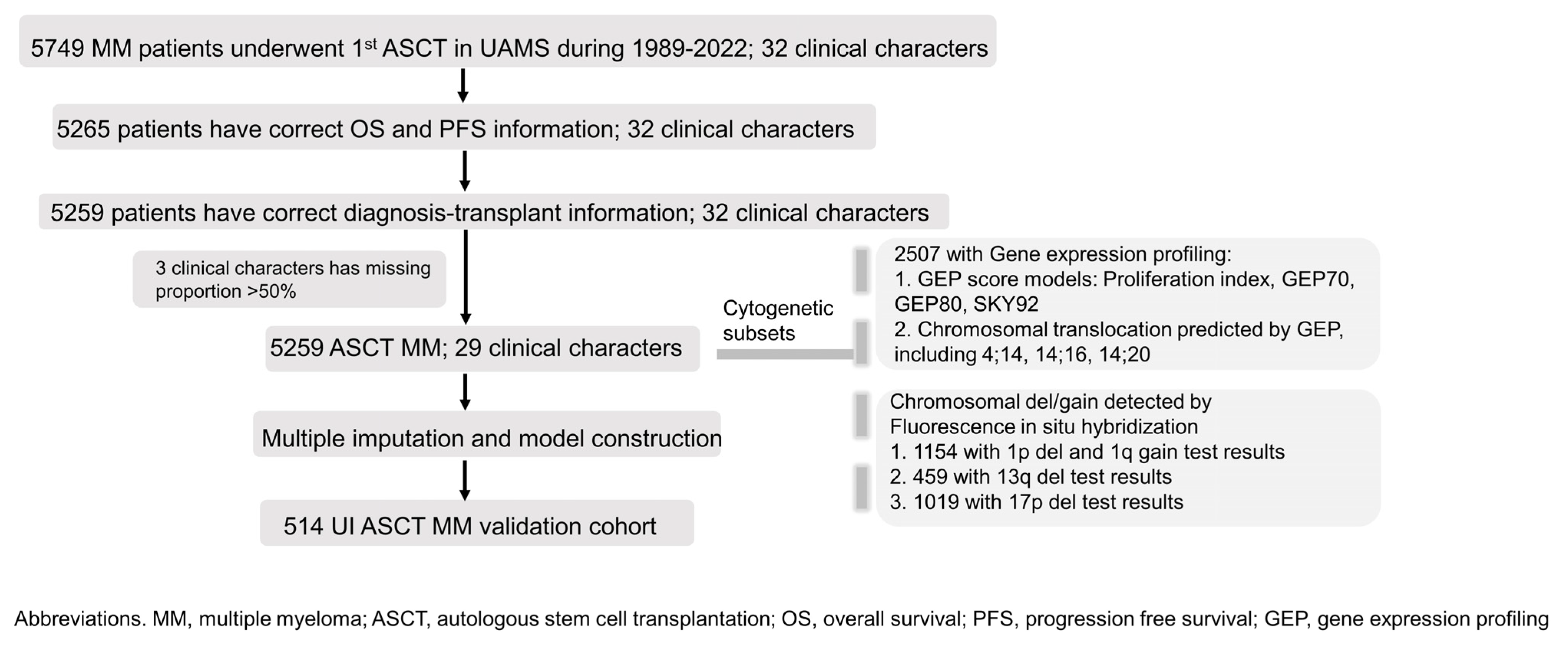
2.1. Study Design, Participants, and Clinical Variables
2.2. GEP Score Calculation and Chromosome Translocation Prediction by GEP
2.3. Fluorescence In Situ Hybridization
2.4. Statistical Analysis
2.5. Data-Sharing Statement
3. Results
3.1. Subsection
3.1.1. Patient Information
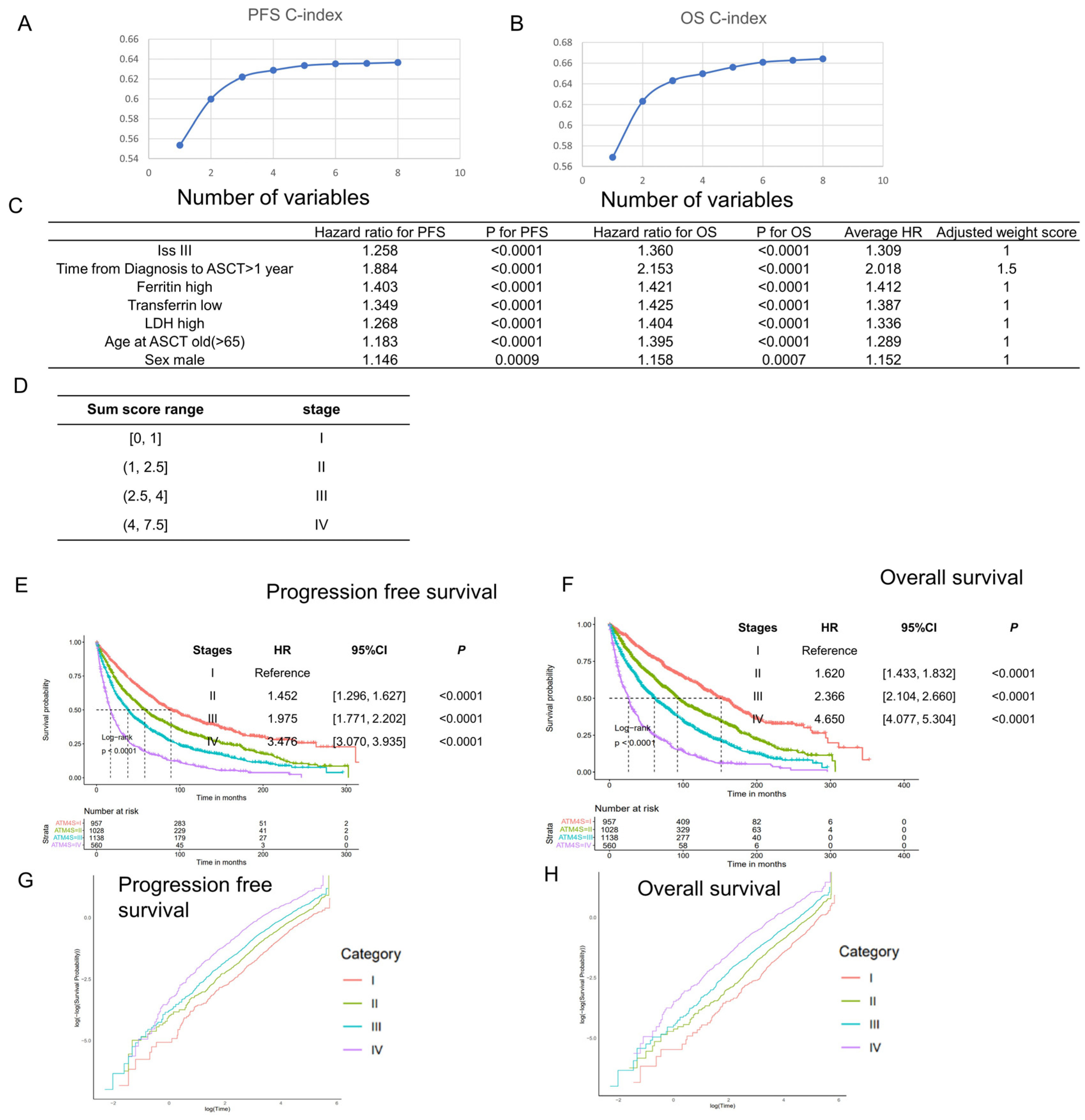
3.1.2. Stage System Development
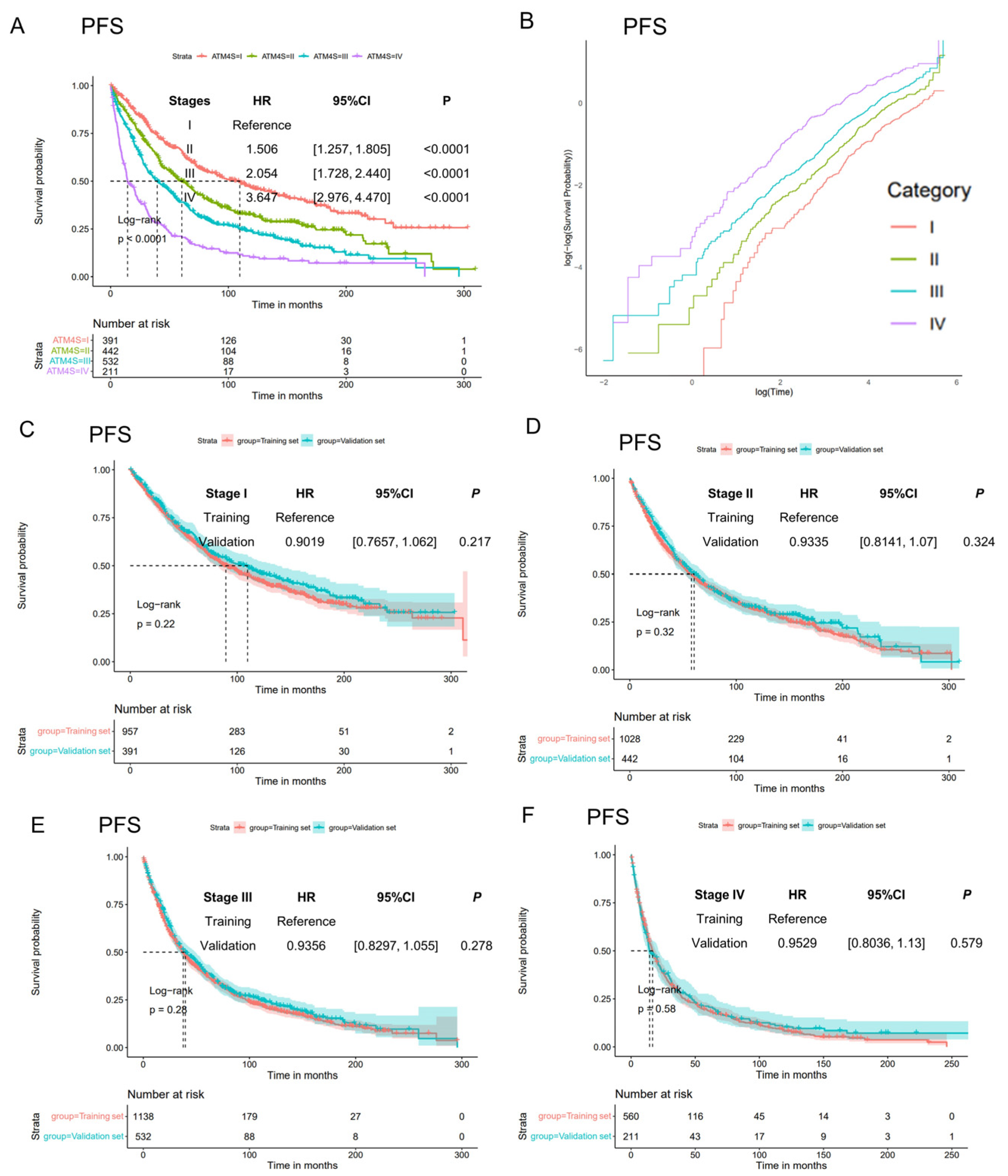
3.1.3. Model Generalization Performance in UAMS Validation Set
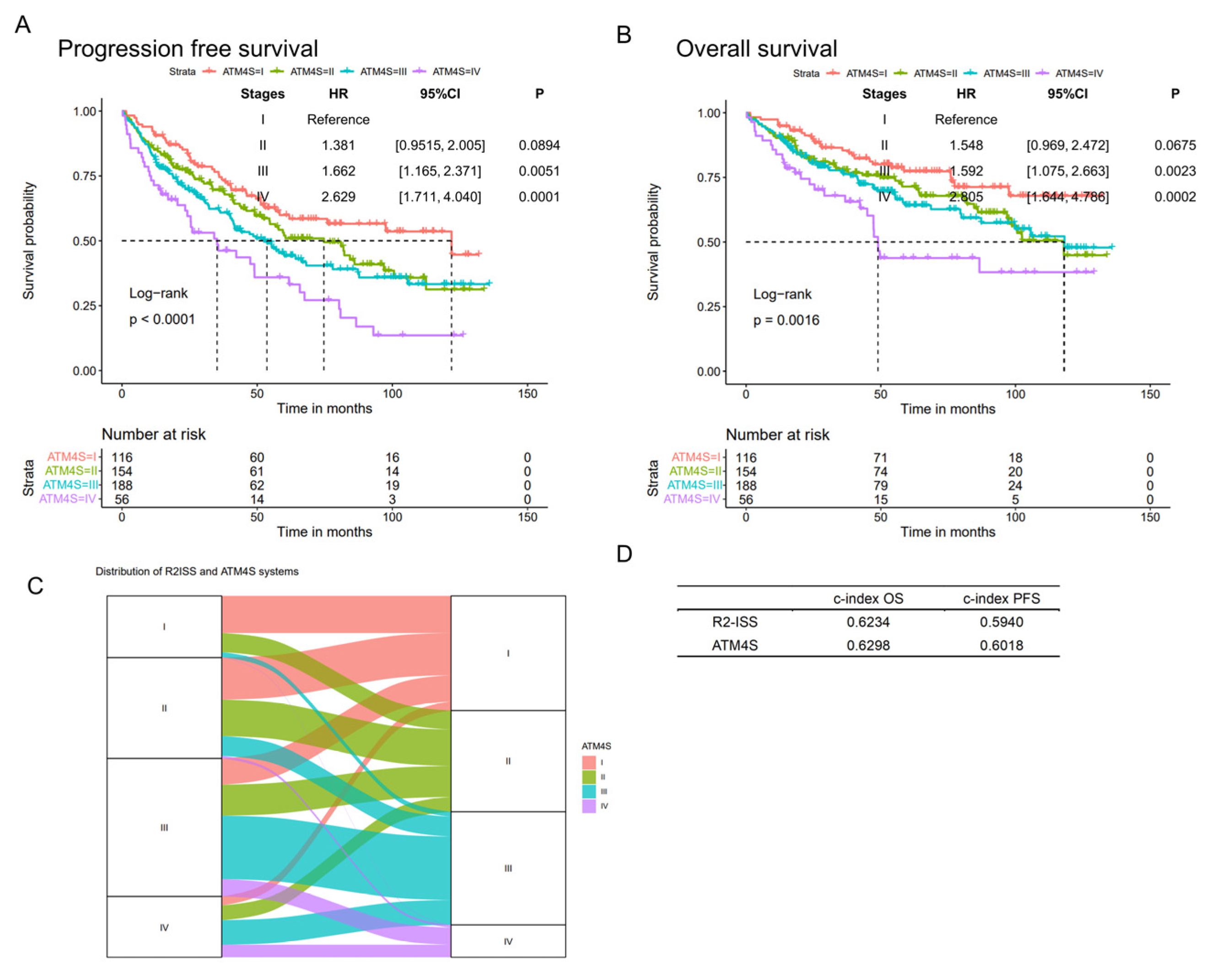
3.1.4. ATM4S Performance at Iowa Medical Center
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Voorhees, P.M.; Kaufman, J.L.; Laubach, J.; Sborov, D.W.; Reeves, B.; Rodriguez, C.; Chari, A.; Silbermann, R.; Costa, L.J.; Anderson, L.D., Jr.; et al. Daratumumab, lenalidomide, bortezomib, and dexamethasone for transplant-eligible newly diagnosed multiple myeloma: The GRIFFIN trial. Blood 2020, 136, 936–945. [Google Scholar] [CrossRef] [PubMed]
- Bazarbachi, A.H.; Al Hamed, R.; Malard, F.; Bazarbachi, A.; Harousseau, J.L.; Mohty, M. Induction therapy prior to autologous stem cell transplantation (ASCT) in newly diagnosed multiple myeloma: An update. Blood Cancer J. 2022, 12, 47. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S. Emerging options in multiple myeloma: Targeted, immune, and epigenetic therapies. Hematol. Am. Soc. Hematol. Educ. Program. 2017, 2017, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Landgren, O.; Rajkumar, S.V. New Developments in Diagnosis, Prognosis, and Assessment of Response in Multiple Myeloma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2016, 22, 5428–5433. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.; Chari, A.; Scott, E.; Mezzi, K.; Usmani, S.Z. B-cell maturation antigen (BCMA) in multiple myeloma: Rationale for targeting and current therapeutic approaches. Leukemia 2020, 34, 985–1005. [Google Scholar] [CrossRef] [PubMed]
- Saad, A.; Mahindra, A.; Zhang, M.J.; Zhong, X.; Costa, L.J.; Dispenzieri, A.; Drobyski, W.R.; Freytes, C.O.; Gale, R.P.; Gasparetto, C.J.; et al. Hematopoietic cell transplant comorbidity index is predictive of survival after autologous hematopoietic cell transplantation in multiple myeloma. Biol. Blood Marrow Transpl. 2014, 20, 402–408 e401. [Google Scholar] [CrossRef] [PubMed]
- Munshi, P.N.; Vesole, D.; Jurczyszyn, A.; Zaucha, J.M.; St Martin, A.; Davila, O.; Agrawal, V.; Badawy, S.M.; Battiwalla, M.; Chhabra, S.; et al. Age no bar: A CIBMTR analysis of elderly patients undergoing autologous hematopoietic cell transplantation for multiple myeloma. Cancer 2020, 126, 5077–5087. [Google Scholar] [CrossRef]
- Labonte, L.; Iqbal, T.; Zaidi, M.A.; McDiarmid, S.A.; Huebsch, L.B.; Tay, J.; Atkins, H.; Allan, D.S. Utility of comorbidity assessment in predicting transplantation-related toxicity following autologous hematopoietic stem cell transplantation for multiple myeloma. Biol. Blood Marrow Transpl. 2008, 14, 1039–1044. [Google Scholar] [CrossRef][Green Version]
- Belotti, A.; Ribolla, R.; Cancelli, V.; Crippa, C.; Bianchetti, N.; Ferrari, S.; Bottelli, C.; Cattaneo, C.; Tucci, A.; De La Fuente Barrigon, C.; et al. Transplant eligibility in elderly multiple myeloma patients: Prospective external validation of the international myeloma working group frailty score and comparison with clinical judgment and other comorbidity scores in unselected patients aged 65–75 years. Am. J. Hematol. 2020, 95, 759–765. [Google Scholar] [CrossRef]
- Gertz, M.A.; Dingli, D. How we manage autologous stem cell transplantation for patients with multiple myeloma. Blood 2014, 124, 882–890. [Google Scholar] [CrossRef]
- Martino, M.; Lemoli, R.M.; Girmenia, C.; Castagna, L.; Bruno, B.; Cavallo, F.; Offidani, M.; Scortechini, I.; Montanari, M.; Milone, G.; et al. Italian consensus conference for the outpatient autologous stem cell transplantation management in multiple myeloma. Bone Marrow Transpl. 2016, 51, 1032–1040. [Google Scholar] [CrossRef] [PubMed]
- Merlini, G.; Perfetti, V.; Gobbi, P.G.; Quaglini, S.; Franciotta, D.M.; Marinone, G.; Ascari, E. Acute phase proteins and prognosis in multiple myeloma. Br. J. Haematol. 1993, 83, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Bataille, R.; Grenier, J.; Sany, J. Beta-2-microglobulin in myeloma: Optimal use for staging, prognosis, and treatment—A prospective study of 160 patients. Blood 1984, 63, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Kiba, T.; Ito, T.; Nakashima, T.; Okikawa, Y.; Kido, M.; Kimura, A.; Kameda, K.; Miyamae, F.; Tanaka, S.; Atsumi, M.; et al. Bortezomib and dexamethasone for multiple myeloma: Higher AST and LDH levels associated with a worse prognosis on overall survival. BMC Cancer 2014, 14, 462. [Google Scholar] [CrossRef] [PubMed]
- Durie, B.G.; Salmon, S.E. A clinical staging system for multiple myeloma. Correlation of measured myeloma cell mass with presenting clinical features, response to treatment, and survival. Cancer 1975, 36, 842–854. [Google Scholar] [CrossRef]
- Shaughnessy, J.D., Jr.; Zhan, F.; Burington, B.E.; Huang, Y.; Colla, S.; Hanamura, I.; Stewart, J.P.; Kordsmeier, B.; Randolph, C.; Williams, D.R.; et al. A validated gene expression model of high-risk multiple myeloma is defined by deregulated expression of genes mapping to chromosome 1. Blood 2007, 109, 2276–2284. [Google Scholar] [CrossRef] [PubMed]
- Kuiper, R.; Broyl, A.; de Knegt, Y.; van Vliet, M.H.; van Beers, E.H.; van der Holt, B.; el Jarari, L.; Mulligan, G.; Gregory, W.; Morgan, G.; et al. A gene expression signature for high-risk multiple myeloma. Leukemia 2012, 26, 2406–2413. [Google Scholar] [CrossRef]
- Younes, M.; Hachfi, H.; Hammouda, F.; Younes, K.; Ben Hammouda, S.; Jguirim, M.; Zrour, S.; Bejia, I.; Touzi, M.; Bergaoui, N. [Survival prognosis factors in multiple myeloma]. Tunis. Med. 2014, 92, 399–405. [Google Scholar]
- Greipp, P.R.; San Miguel, J.; Durie, B.G.; Crowley, J.J.; Barlogie, B.; Blade, J.; Boccadoro, M.; Child, J.A.; Avet-Loiseau, H.; Kyle, R.A.; et al. International staging system for multiple myeloma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 3412–3420. [Google Scholar] [CrossRef]
- Palumbo, A.; Avet-Loiseau, H.; Oliva, S.; Lokhorst, H.M.; Goldschmidt, H.; Rosinol, L.; Richardson, P.; Caltagirone, S.; Lahuerta, J.J.; Facon, T.; et al. Revised International Staging System for Multiple Myeloma: A Report from International Myeloma Working Group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 2863–2869. [Google Scholar] [CrossRef]
- Tan, J.L.C.; Wellard, C.; Moore, E.M.; Mollee, P.; Rajagopal, R.; Quach, H.; Harrison, S.J.; McDonald, E.J.; Ho, P.J.; Prince, H.M.; et al. The second revision of the International Staging System (R2-ISS) stratifies progression-free and overall survival in multiple myeloma: Real world data results in an Australian and New Zealand Population. Br. J. Haematol. 2023, 200, e17–e21. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.D.; Bartlett, J.W.; Carpenter, J.; Nicholas, O.; Hemingway, H. Comparison of random forest and parametric imputation models for imputing missing data using MICE: A CALIBER study. Am. J. Epidemiol. 2014, 179, 764–774. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.J.; Eo, S.H.; Kim, S.C.; Park, K.M.; Lee, Y.J.; Lee, S.K.; Yu, E.; Cho, H.; Hong, S.M. Increased number of metastatic lymph nodes in adenocarcinoma of the ampulla of Vater as a prognostic factor: A proposal of new nodal classification. Surgery 2014, 155, 74–84. [Google Scholar] [CrossRef]
- Harrell, F.E.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Barlogie, B.; Anaissie, E.; van Rhee, F.; Haessler, J.; Hollmig, K.; Pineda-Roman, M.; Cottler-Fox, M.; Mohiuddin, A.; Alsayed, Y.; Tricot, G.; et al. Incorporating bortezomib into upfront treatment for multiple myeloma: Early results of total therapy 3. Br. J. Haematol. 2007, 138, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Usmani, S.Z.; Sawyer, J.; Rosenthal, A.; Cottler-Fox, M.; Epstein, J.; Yaccoby, S.; Sexton, R.; Hoering, A.; Singh, Z.; Heuck, C.J.; et al. Risk factors for MDS and acute leukemia following total therapy 2 and 3 for multiple myeloma. Blood 2013, 121, 4753–4757. [Google Scholar] [CrossRef] [PubMed]
- Barlogie, B.; Tricot, G.; Anaissie, E.; Shaughnessy, J.; Rasmussen, E.; van Rhee, F.; Fassas, A.; Zangari, M.; Hollmig, K.; Pineda-Roman, M.; et al. Thalidomide and hematopoietic-cell transplantation for multiple myeloma. N. Engl. J. Med. 2006, 354, 1021–1030. [Google Scholar] [CrossRef]
- Barlogie, B.; Jagannath, S.; Desikan, K.R.; Mattox, S.; Vesole, D.; Siegel, D.; Tricot, G.; Munshi, N.; Fassas, A.; Singhal, S.; et al. Total therapy with tandem transplants for newly diagnosed multiple myeloma. Blood 1999, 93, 55–65. [Google Scholar] [CrossRef]
- Usmani, S.Z.; Sexton, R.; Hoering, A.; Heuck, C.J.; Nair, B.; Waheed, S.; Al Sayed, Y.; Chauhan, N.; Ahmad, N.; Atrash, S.; et al. Second malignancies in total therapy 2 and 3 for newly diagnosed multiple myeloma: Influence of thalidomide and lenalidomide during maintenance. Blood 2012, 120, 1597–1600. [Google Scholar] [CrossRef]
- Salomon-Perzynski, A.; Bluszcz, A.; Krzywdzinska, A.; Spyra-Gorny, Z.; Jakacka, N.; Barankiewicz, J.; Borg, K.; Solarska, I.; Szpila, T.; Pula, B.; et al. The impact of cytogenetic evolution and acquisition of del(17p) on the prognosis of patients with multiple myeloma. Pol. Arch. Intern. Med. 2020, 130, 483–491. [Google Scholar] [CrossRef]
- Varma, A.; Sui, D.; Milton, D.R.; Tang, G.; Saini, N.; Hasan, O.; Mukherjee, A.; Joseph, J.J.; Bashir, Q.; Rondon, G.; et al. Outcome of Multiple Myeloma with Chromosome 1q Gain and 1p Deletion after Autologous Hematopoietic Stem Cell Transplantation: Propensity Score Matched Analysis. Biol. Blood Marrow Transpl. 2020, 26, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Paner, A.; Patel, P.; Dhakal, B. The evolving role of translocation t(11;14) in the biology, prognosis, and management of multiple myeloma. Blood Rev. 2020, 41, 100643. [Google Scholar] [CrossRef] [PubMed]
- Porrata, L.F.; Gertz, M.A.; Inwards, D.J.; Litzow, M.R.; Lacy, M.Q.; Tefferi, A.; Gastineau, D.A.; Dispenzieri, A.; Ansell, S.M.; Micallef, I.N.; et al. Early lymphocyte recovery predicts superior survival after autologous hematopoietic stem cell transplantation in multiple myeloma or non-Hodgkin lymphoma. Blood 2001, 98, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.; Li, J.; King, K.; Persaud, A.K.; Duah, E.; Vangundy, Z.; Hofmeister, C.C.; Lamba, J.K.; Tan, A.C.; Fridley, B.L.; et al. PARP1 and POLD2 as prognostic biomarkers for multiple myeloma in autologous stem cell transplant. Haematologica 2023, 108, 2155–2166. [Google Scholar] [CrossRef] [PubMed]
- Harousseau, J.L.; Avet-Loiseau, H.; Attal, M.; Charbonnel, C.; Garban, F.; Hulin, C.; Michallet, M.; Facon, T.; Garderet, L.; Marit, G.; et al. Achievement of at least very good partial response is a simple and robust prognostic factor in patients with multiple myeloma treated with high-dose therapy: Long-term analysis of the IFM 99-02 and 99-04 Trials. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 5720–5726. [Google Scholar] [CrossRef] [PubMed]
- Takamatsu, H.; Takezako, N.; Zheng, J.; Moorhead, M.; Carlton, V.E.H.; Kong, K.A.; Murata, R.; Ito, S.; Miyamoto, T.; Yokoyama, K.; et al. Prognostic value of sequencing-based minimal residual disease detection in patients with multiple myeloma who underwent autologous stem-cell transplantation. Ann. Oncol. 2017, 28, 2503–2510. [Google Scholar] [CrossRef] [PubMed]
- de Tute, R.M.; Pawlyn, C.; Cairns, D.A.; Davies, F.E.; Menzies, T.; Rawstron, A.; Jones, J.R.; Hockaday, A.; Henderson, R.; Cook, G.; et al. Minimal Residual Disease After Autologous Stem-Cell Transplant for Patients with Myeloma: Prognostic Significance and the Impact of Lenalidomide Maintenance and Molecular Risk. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2022, 40, 2889–2900. [Google Scholar] [CrossRef]
- Kaddoura, M.; Dingli, D.; Buadi, F.K.; Lacy, M.Q.; Gertz, M.A.; Dispenzieri, A.; Kapoor, P.; Hwa, L.; Fonder, A.; Hobbs, M.; et al. Prognostic impact of posttransplant FDG PET/CT scan in multiple myeloma. Blood Adv. 2021, 5, 2753–2759. [Google Scholar] [CrossRef]
- Cullis, J.O.; Fitzsimons, E.J.; Griffiths, W.J.; Tsochatzis, E.; Thomas, D.W.; British Society for Haematology. Investigation and management of a raised serum ferritin. Br. J. Haematol. 2018, 181, 331–340. [Google Scholar] [CrossRef]
- Franke, G.N.; Kubasch, A.S.; Cross, M.; Vucinic, V.; Platzbecker, U. Iron overload and its impact on outcome of patients with hematological diseases. Mol. Asp. Med. 2020, 75, 100868. [Google Scholar] [CrossRef]
- Plano, F.; Gigliotta, E.; Corsale, A.M.; Azgomi, M.S.; Santonocito, C.; Ingrasci, M.; Di Carlo, L.; Augello, A.E.; Speciale, M.; Vullo, C.; et al. Ferritin Metabolism Reflects Multiple Myeloma Microenvironment and Predicts Patient Outcome. Int. J. Mol. Sci. 2023, 24, 8852. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Jie, X.; Nian, L.; Wang, Y.; Wang, C.; Ma, J.; Jiang, J.; Wu, Q.; Qiao, J.; Chen, W.; et al. A combination of pre-infusion serum ferritin, CRP and IL-6 predicts outcome in relapsed/refractory multiple myeloma patients treated with CAR-T cells. Front. Immunol. 2023, 14, 1169071. [Google Scholar] [CrossRef] [PubMed]
- Zhan, F.; Hardin, J.; Kordsmeier, B.; Bumm, K.; Zheng, M.; Tian, E.; Sanderson, R.; Yang, Y.; Wilson, C.; Zangari, M.; et al. Global gene expression profiling of multiple myeloma, monoclonal gammopathy of undetermined significance, and normal bone marrow plasma cells. Blood 2002, 99, 1745–1757. [Google Scholar] [CrossRef] [PubMed]
- Zhan, F.; Huang, Y.; Colla, S.; Stewart, J.P.; Hanamura, I.; Gupta, S.; Epstein, J.; Yaccoby, S.; Sawyer, J.; Burington, B.; et al. The molecular classification of multiple myeloma. Blood 2006, 108, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Hanamura, I.; Stewart, J.P.; Huang, Y.; Zhan, F.; Santra, M.; Sawyer, J.R.; Hollmig, K.; Zangarri, M.; Pineda-Roman, M.; Van Rhee, F.; et al. Frequent gain of chromosome band 1q21 in plasma-cell dyscrasias detected by fluorescence in situ hybridization: Incidence increases from MGUS to relapsed myeloma and is related to prognosis and disease progression following tandem stem-cell transplantation. Blood 2006, 108, 1724–1732. [Google Scholar] [CrossRef] [PubMed]
- Shaughnessy, J.; Jacobson, J.; Sawyer, J.; McCoy, J.; Fassas, A.; Zhan, F.; Bumm, K.; Epstein, J.; Anaissie, E.; Jagannath, S.; et al. Continuous absence of metaphase-defined cytogenetic abnormalities, especially of chromosome 13 and hypodiploidy, ensures long-term survival in multiple myeloma treated with Total Therapy I: Interpretation in the context of global gene expression. Blood 2003, 101, 3849–3856. [Google Scholar] [CrossRef] [PubMed]
- Xiong, W.; Wu, X.; Starnes, S.; Johnson, S.K.; Haessler, J.; Wang, S.; Chen, L.; Barlogie, B.; Shaughnessy, J.D., Jr.; Zhan, F. An analysis of the clinical and biologic significance of TP53 loss and the identification of potential novel transcriptional targets of TP53 in multiple myeloma. Blood 2008, 112, 4235–4246. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.; Qi, C.; Yi, Q.L.; Reece, D.; Stewart, A.K. p53 gene deletion detected by fluorescence in situ hybridization is an adverse prognostic factor for patients with multiple myeloma following autologous stem cell transplantation. Blood 2005, 105, 358–360. [Google Scholar] [CrossRef]
- D’agostino, M.; Cairns, D.A.; Lahuerta, J.J.; Wester, R.; Bertsch, U.; Waage, A.; Zamagni, E.; Mateos, M.V.; Dall’Olio, D.; van de Donk, N.W.; et al. Second Revision of the International Staging System (R2-ISS) for Overall Survival in Multiple Myeloma: A European Myeloma Network (EMN) Report Within the HARMONY Project. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2022, 40, 3406–3418. [Google Scholar] [CrossRef]
- Durie, B.G.; Harousseau, J.; Miguel, J.S.; Blade, J.; Barlogie, B.; Anderson, K.; Gertz, M.; Dimopoulos, M.; Westin, J. International uniform response criteria for multiple myeloma. Leukemia 2006, 20, 1467–1473. [Google Scholar] [CrossRef] [PubMed]
- Shaughnessy, J.D., Jr.; Qu, P.; Usmani, S.; Heuck, C.J.; Zhang, Q.; Zhou, Y.; Tian, E.; Hanamura, I.; van Rhee, F.; Anaissie, E.; et al. Pharmacogenomics of bortezomib test-dosing identifies hyperexpression of proteasome genes, especially PSMD4, as novel high-risk feature in myeloma treated with Total Therapy 3. Blood 2011, 118, 3512–3524. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Gayle, A.A.; Wang, J.; Zhang, H.; Cardinal-Fernandez, P. Comparing baseline characteristics between groups: An introduction to the CBCgrps package. Ann. Transl. Med. 2017, 5, 484. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Training (n = 3683) | Validation (n = 1576) |
|---|---|---|
| Sex, n (%) | ||
| Female | 1448 (39) | 633 (40) |
| Male | 2235 (61) | 943 (60) |
| Age at transplant, Median (Q1, Q3), yr | 59.55 (51.66, 66.27) | 59 (51.67, 66.22) |
| Race, n (%) | ||
| Asian | 13 (0) | 10 (1) |
| African | 437 (12) | 185 (12) |
| Native American | 9 (0) | 11 (1) |
| Pacific islander | 2 (0) | 1 (0) |
| White/Caucasian | 3235 (88) | 1369 (87) |
| Isotype, n (%) | ||
| Biclonal disease | 6 (0) | 5 (0) |
| Free light chain | 671 (18) | 265 (17) |
| IgA | 723 (20) | 328 (21) |
| IgD | 51 (1) | 14 (1) |
| IgG | 2025 (55) | 880 (56) |
| IgM | 13 (0) | 7 (0) |
| Non-secretory | 194 (5) | 77 (5) |
| Light, n (%) | ||
| Kappa | 2246 (61) | 942 (60) |
| Kappa + Lambda | 4 (0) | 2 (0) |
| Lambda | 1256 (34) | 567 (36) |
| None | 177 (5) | 65 (4) |
| Transferrin, Median (Q1, Q3), g/L | 215 (177, 249) | 213.5 (179, 245.25) |
| Ferritin, Median (Q1, Q3), μg/L | 233.4 (100.4, 533.2) | 254.8 (100.97, 556) |
| Iron, Median (Q1, Q3), μg/dL | 73 (52, 98) | 71 (51, 96) |
| Plasma cell percentage (bone marrow aspiration), Median (Q1, Q3), % | 25 (7.5, 50) | 27 (7.5, 50) |
| Plasma cell percentage (bone marrow biopsy), Median (Q1, Q3), % | 30 (7.5, 60) | 30 (7.5, 60) |
| Albumin, Median (Q1, Q3), g/dL | 3.9 (3.5, 4.3) | 3.9 (3.4, 4.3) |
| B2M, Median (Q1, Q3), mg/L | 3.1 (2.1, 5.3) | 3.2 (2.2, 5.23) |
| LDH, Median (Q1, Q3), U/L | 158 (128, 200) | 155.5 (127, 194.25) |
| Creatinine, Median (Q1, Q3), mg/dL | 1 (0.8, 1.3) | 1 (0.8, 1.3) |
| CRP, Median (Q1, Q3), mg/dL | 2.42 (0.45, 5.5) | 2.9 (0.43, 5.4) |
| Hb, Median (Q1, Q3), g/dL | 11.4 (9.8, 12.8) | 11.3 (9.8, 12.72) |
| Platelets, Median (Q1, Q3), 103/μL | 223 (170, 278) | 219 (169, 278) |
| Monocytes, Median (Q1, Q3), % | 8.9 (6.85, 11.7) | 8.9 (6.88, 11.5) |
| Lymphocytes, Median (Q1, Q3), % | 26.4 (18.2, 35.15) | 26.3 (18.9, 35.2) |
| Serum M protein, Median (Q1, Q3), g/dL | 1.4 (0.09, 3.5) | 1.6 (0.2, 3.7) |
| Urine M protein, Median (Q1, Q3), g/L | 0 (0, 504) | 0 (0, 485.25) |
| Ca, Median (Q1, Q3), mg/dL | 9.2 (8.8, 9.7) | 9.2 (8.8, 9.7) |
| BMI, Median (Q1, Q3), kg/m2 | 27.94 (24.81, 31.62) | 27.94 (24.8, 31.48) |
| Glucose Serum, Median (Q1, Q3), mmol/L | 101 (90, 119) | 100 (89, 119) |
| Cholesterol, Median (Q1, Q3), mg/dL | 172 (138, 207) | 172 (138, 207) |
| Triglycerides, Median (Q1, Q3), mg/dL | 141 (93, 208) | 141 (94, 215) |
| HDL, Median (Q1, Q3), mg/dL | 42 (33, 53) | 41 (33, 52.25) |
| Time from MM diagnosis to ASCT, Median (Q1, Q3), mth | 6.53 (4.13, 11.97) | 6.47 (4.19, 12.08) |
| OS time, Median (Q1, Q3), mth | 56.1 (22.78, 112.52) | 59.2 (25.37, 112.55) |
| OS, n (%) | ||
| 0 | 1326 (36) | 594 (38) |
| 1 | 2357 (64) | 982 (62) |
| PFS time, Median (Q1, Q3), mth | 38.77 (14.77, 84.08) | 40.95 (16.72, 86.43) |
| PFS, n (%) | ||
| 0 | 1113 (30) | 517 (33) |
| 1 | 2570 (70) | 1059 (67) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, W.; Strouse, C.; Mery, D.; Siegel, E.R.; Munshi, M.N.; Ashby, T.C.; Cheng, Y.; Sun, F.; Wanchai, V.; Zhang, Z.; et al. A Risk Stratification System in Myeloma Patients with Autologous Stem Cell Transplantation. Cancers 2024, 16, 1116. https://doi.org/10.3390/cancers16061116
Guo W, Strouse C, Mery D, Siegel ER, Munshi MN, Ashby TC, Cheng Y, Sun F, Wanchai V, Zhang Z, et al. A Risk Stratification System in Myeloma Patients with Autologous Stem Cell Transplantation. Cancers. 2024; 16(6):1116. https://doi.org/10.3390/cancers16061116
Chicago/Turabian StyleGuo, Wancheng, Christopher Strouse, David Mery, Eric R. Siegel, Manit N. Munshi, Timothy Cody Ashby, Yan Cheng, Fumou Sun, Visanu Wanchai, Zijun Zhang, and et al. 2024. "A Risk Stratification System in Myeloma Patients with Autologous Stem Cell Transplantation" Cancers 16, no. 6: 1116. https://doi.org/10.3390/cancers16061116
APA StyleGuo, W., Strouse, C., Mery, D., Siegel, E. R., Munshi, M. N., Ashby, T. C., Cheng, Y., Sun, F., Wanchai, V., Zhang, Z., Bailey, C., Alapat, D. V., Peng, H., Al Hadidi, S., Thanendrarajan, S., Schinke, C., Zangari, M., van Rhee, F., Tricot, G., ... Zhan, F. (2024). A Risk Stratification System in Myeloma Patients with Autologous Stem Cell Transplantation. Cancers, 16(6), 1116. https://doi.org/10.3390/cancers16061116