

Association Between Chemotherapy-Induced Peripheral Neuropathy and Low Anterior Resection Syndrome


 , , ,
, , ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
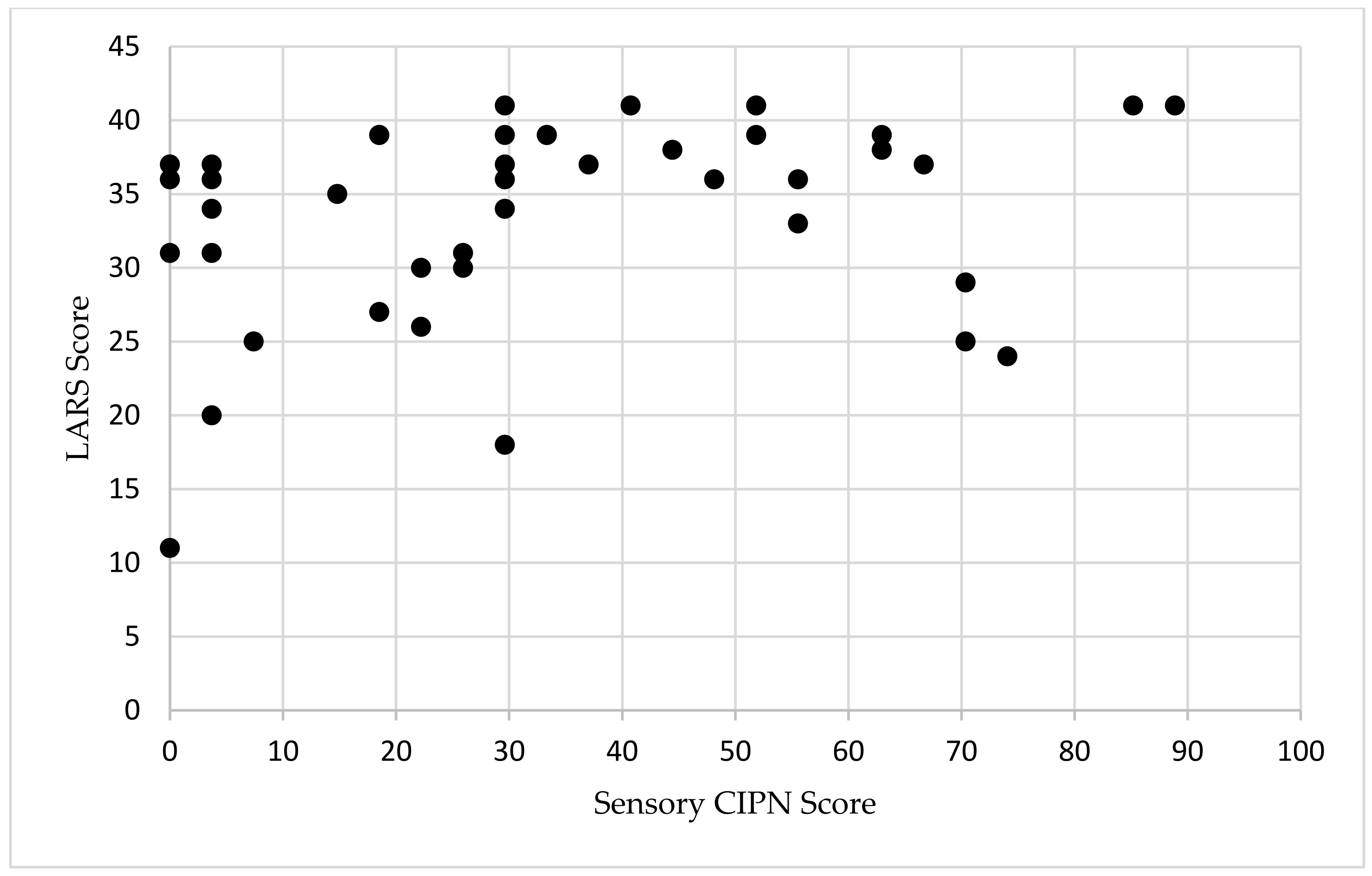
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kapiteijn, E.; Marijnen, C.A.; Nagtegaal, I.D.; Putter, H.; Steup, W.H.; Wiggers, T.; Rutten, H.J.; Pahlman, L.; Glimelius, B.; van Krieken, J.H.J.; et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N. Engl. J. Med. 2001, 345, 638–646. [Google Scholar] [CrossRef] [PubMed]
- van Gijn, W.; Marijnen, C.A.; Nagtegaal, I.D.; Kranenbarg, E.M.-K.; Putter, H.; Wiggers, T.; Rutten, H.J.; Påhlman, L.; Glimelius, B.; van de Velde, C.J.; et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 2011, 12, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Yeo, H.L.; Abelson, J.S.; Mao, J.; Cheerharan, M.; Milsom, J.; Sedrakyan, A. Minimally invasive surgery and sphincter preservation in rectal cancer. J. Surg. Res. 2016, 202, 299–307. [Google Scholar] [CrossRef]
- Croese, A.D.; Lonie, J.M.; Trollope, A.F.; Vangaveti, V.N.; Ho, Y.-H. A meta-analysis of the prevalence of low anterior resection syndrome and systematic review of risk factors. Int. J. Surg. 2018, 56, 234–241. [Google Scholar] [CrossRef]
- Bolton, W.S.; Chapman, S.J.; Corrigan, N.; Croft, J.; Collinson, F.; Brown, J.M.; Jayne, D.G. The Incidence of Low Anterior Resection Syndrome as Assessed in an International Randomized Controlled Trial (MRC/NIHR ROLARR). Ann. Surg. 2021, 274, e1223–e1229. [Google Scholar] [CrossRef]
- Emmertsen, K.J.; Laurberg, S. Low anterior resection syndrome score: Development and validation of a symptom-based scoring system for bowel dysfunction after low anterior resection for rectal cancer. Ann. Surg. 2012, 255, 922–928. [Google Scholar] [CrossRef]
- Keane, C.; Fearnhead, N.S.; Bordeianou, L.; Christensen, P.; Espin Basany, E.; Laurberg, S.; Mellgren, A.; Messick, C.; Orangio, G.R.; Verjee, A.; et al. International consensus definition of low anterior resection syndrome. Color. Dis. 2020, 22, 331–341. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision. Available online: https://icd.who.int/browse10/2016/en (accessed on 6 September 2024).
- McKenna, N.P.; Bews, K.A.; Yost, K.J.; Cima, R.R.; Habermann, E.B. Bowel Dysfunction after Low Anterior Resection for Colorectal Cancer: A Frequent Late Effect of Surgery Infrequently Treated. J. Am. Coll. Surg. 2022, 234, 529–537. [Google Scholar] [CrossRef]
- Battersby, N.J.; Juul, T.; Christensen, P.; Janjua, A.Z.; Branagan, G.; Emmertsen, K.J.; Norton, C.; Hughes, R.; Laurberg, S.; Moran, B.J.; et al. Predicting the Risk of Bowel-Related Quality-of-Life Impairment After Restorative Resection for Rectal Cancer: A Multicenter Cross-Sectional Study. Dis. Colon Rectum 2016, 59, 270–280. [Google Scholar] [CrossRef]
- Lee, W.Y.; Takahashi, T.; Pappas, T.; Mantyh, C.R.; Ludwig, K.A. Surgical autonomic denervation results in altered colonic motility: An explanation for low anterior resection syndrome? Surgery 2008, 143, 778–783. [Google Scholar] [CrossRef]
- Bryant, C.L.; Lunniss, P.J.; Knowles, C.H.; Thaha, M.A.; Chan, C.L. Anterior resection syndrome. Lancet Oncol. 2012, 13, e403–e408. [Google Scholar] [CrossRef] [PubMed]
- Ekkarat, P.; Boonpipattanapong, T.; Tantiphlachiva, K.; Sangkhathat, S. Factors determining low anterior resection syndrome after rectal cancer resection: A study in Thai patients. Asian J. Surg. 2016, 39, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Hughes, D.L.; Cornish, J.; Morris, C.; Group, L.T.M. Functional outcome following rectal surgery—Predisposing factors for low anterior resection syndrome. Int. J. Color. Dis. 2017, 32, 691–697. [Google Scholar] [CrossRef]
- Machado, M.; Nygren, J.; Goldman, S.; Ljungqvist, O. Similar outcome after colonic pouch and side-to-end anastomosis in low anterior resection for rectal cancer: A prospective randomized trial. Ann. Surg. 2003, 238, 214–220. [Google Scholar] [CrossRef]
- Parc, Y.; Ruppert, R.; Fuerst, A.; Golcher, H.; Zutshi, M.; Hull, T.; Tiret, E.; Hemminger, F.; Galandiuk, S.; Fender, S.; et al. Better function with a colonic J-pouch or a side-to-end anastomosis?: A randomized controlled trial to compare the complications, functional outcome, and quality of life in patients with low rectal cancer after a J-pouch or a side-to-end anastomosis. Ann. Surg. 2019, 269, 815–826. [Google Scholar] [CrossRef]
- Seretny, M.; Currie, G.L.; Sena, E.S.; Ramnarine, S.; Grant, R.; MacLeod, M.R.; Colvin, L.A.; Fallon, M. Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. PAIN® 2014, 155, 2461–2470. [Google Scholar] [CrossRef]
- Jordan, B.; Margulies, A.; Cardoso, F.; Cavaletti, G.; Haugnes, H.; Jahn, P.; Le Rhun, E.; Preusser, M.; Scotté, F.; Taphoorn, M.; et al. Systemic anticancer therapy-induced peripheral and central neurotoxicity: ESMO–EONS–EANO Clinical Practice Guidelines for diagnosis, prevention, treatment and follow-up. Ann. Oncol. 2020, 31, 1306–1319. [Google Scholar] [CrossRef]
- Loprinzi, C.L.; Lacchetti, C.; Bleeker, J.; Cavaletti, G.; Chauhan, C.; Hertz, D.L.; Kelley, M.R.; Lavino, A.; Lustberg, M.B.; Paice, J.A.; et al. Prevention and management of chemotherapy-induced peripheral neuropathy in survivors of adult cancers: ASCO guideline update. J. Clin. Oncol. 2020, 38, 3325–3348. [Google Scholar] [CrossRef]
- Postma, T.J.; Aaronson, N.; Heimans, J.; Muller, M.; Hildebrand, J.; Delattre, J.-Y.; Hoang-Xuan, K.; Lantéri-Minet, M.; Grant, R.; Huddart, R.; et al. The development of an EORTC quality of life questionnaire to assess chemotherapy-induced peripheral neuropathy: The QLQ-CIPN20. Eur. J. Cancer 2005, 41, 1135–1139. [Google Scholar] [CrossRef]
- Sturiale, A.; Martellucci, J.; Zurli, L.; Vaccaro, C.; Brusciano, L.; Limongelli, P.; Docimo, L.; Valeri, A. Long-term functional follow-up after anterior rectal resection for cancer. Int. J. Color. Dis. 2017, 32, 83–88. [Google Scholar] [CrossRef]
- O’Sullivan, N.J.; Temperley, H.C.; Nugent, T.S.; Low, E.Z.; Kavanagh, D.O.; Larkin, J.O.; Mehigan, B.J.; McCormick, P.H.; Kelly, M.E. Early vs. standard reversal ileostomy: A systematic review and meta-analysis. Tech. Coloproctol. 2022, 26, 851–862. [Google Scholar] [CrossRef]
- Cercek, A.; Roxburgh, C.S.; Strombom, P.; Smith, J.J.; Temple, L.K.; Nash, G.M.; Guillem, J.G.; Paty, P.B.; Yaeger, R.; Stadler, Z.K.; et al. Adoption of total neoadjuvant therapy for locally advanced rectal cancer. JAMA Oncol. 2018, 4, e180071. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, M.; Mège, D.; Maggiori, L.; Ferron, M.; Panis, Y. When is the best time for temporary stoma closure in laparoscopic sphincter-saving surgery for rectal cancer? A study of 259 consecutive patients. Tech. Coloproctol. 2015, 19, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Danielsen, A.K.; Park, J.; Jansen, J.E.; Bock, D.; Skullman, S.; Wedin, A.; Marinez, A.C.; Haglind, E.; Angenete, E.; Rosenberg, J. Early Closure of a Temporary Ileostomy in Patients With Rectal Cancer: A Multicenter Randomized Controlled Trial. Ann. Surg. 2017, 265, 284–290. [Google Scholar] [CrossRef] [PubMed]
- van Heinsbergen, M.; Van der Heijden, J.A.G.; Stassen, L.P.; Melenhorst, J.; de Witte, E.; Belgers, E.H.; Maaskant-Braat, A.J.G.; Bloemen, J.G.; Bouvy, N.D.; Janssen-Heijnen, M.L.; et al. The low anterior resection syndrome in a reference population: Prevalence and predictive factors in the Netherlands. Color. Dis. 2020, 22, 46–52. [Google Scholar] [CrossRef]
- Emmertsen, K.J.; Laurberg, S.; Jess, P.; Madsen, M.R.; Nielsen, H.J.; Ovesen, A.; Salomon, S.; Nielsen, K.T.; Vilandt, J. Impact of bowel dysfunction on quality of life after sphincter-preserving resection for rectal cancer. J. Br. Surg. 2013, 100, 1377–1387. [Google Scholar] [CrossRef]
- Ota, E.; Nagasaki, T.; Akiyoshi, T.; Mukai, T.; Hiyoshi, Y.; Yamaguchi, T.; Fukunaga, Y. Incidence and risk factors of bowel dysfunction after minimally invasive rectal cancer surgery and discrepancies between the Wexner score and the low anterior resection syndrome (LARS) score. Surg Today 2024, 54, 763–770. [Google Scholar] [CrossRef]
- Chen, T.Y.-T.; Wiltink, L.M.; Nout, R.A.; Kranenbarg, E.M.-K.; Laurberg, S.; Marijnen, C.A.; van de Velde, C.J. Bowel function 14 years after preoperative short-course radiotherapy and total mesorectal excision for rectal cancer: Report of a multicenter randomized trial. Clin. Color. Cancer 2015, 14, 106–114. [Google Scholar] [CrossRef]
- Zhang, R.; Luo, W.; Qiu, Y.; Chen, F.; Luo, D.; Yang, Y.; He, W.; Li, Q.; Li, X. Clinical Management of Low Anterior Resection Syndrome: Review of the Current Diagnosis and Treatment. Cancers 2023, 15, 5011. [Google Scholar] [CrossRef]
- Juul, T.; Elfeki, H.; Christensen, P.; Laurberg, S.; Emmertsen, K.J.; Bager, P. Normative data for the low anterior resection syndrome score (LARS score). Ann. Surg. 2019, 269, 1124–1128. [Google Scholar] [CrossRef]
- Popeskou, S.G.; Roesel, R.; Faes, S.; Vanoni, A.; Galafassi, J.; di Tor Vajana, A.F.; Piotet, L.M.; Christoforidis, D. Ondansetron for Low Anterior Resection Syndrome (LARS): A Double-Blind, Placebo-Controlled, Cross-Over, Randomized Study. Ann. Surg. 2024, 279, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Battersby, N.J.; Bouliotis, G.; Emmertsen, K.J.; Juul, T.; Glynne-Jones, R.; Branagan, G.; Christensen, P.; Laurberg, S.; Moran, B.J. Development and external validation of a nomogram and online tool to predict bowel dysfunction following restorative rectal cancer resection: The POLARS score. Gut 2018, 67, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Rethy, B.; Nordenvall, C.; Pieniowski, E.; Jansson-Palmer, G.; Johar, A.; Lagergren, P.; Abraham-Nordling, M. Validity assessment of the POLARS score tool in the prediction of post rectal cancer surgery LARS score in a population-based Swedish cohort. BMJ Open Gastroenterol. 2024, 11, e001274. [Google Scholar] [CrossRef] [PubMed]
- Molenaar, C.J.L.; Minnella, E.M.; Coca-Martinez, M.; Ten Cate, D.W.G.; Regis, M.; Awasthi, R.; Martínez-Palli, G.; López-Baamonde, M.; Sebio-Garcia, R.; Feo, C.V.; et al. Effect of multimodal prehabilitation on reducing postoperative complications and enhancing functional capacity following colorectal cancer surgery: The PREHAB randomized clinical trial. JAMA Surg. 2023, 158, 572–581. [Google Scholar] [CrossRef]
- Berkel, A.E.; Bongers, B.C.; Kotte, H.; Weltevreden, P.; De Jongh, F.H.; Eijsvogel, M.M.; Wymenga, M.; Bigirwamungu-Bargeman, M.; Van Der Palen, J.; van Det, M.J.; et al. Effects of community-based exercise prehabilitation for patients scheduled for colorectal surgery with high risk for postoperative complications: Results of a randomized clinical trial. Ann. Surg. 2022, 275, e299–e306. [Google Scholar] [CrossRef]
- Bosch, N.; Kalkdijk-Dijkstra, A.; van Westreenen, H.; Broens, P.; Pierie, J.; van der Heijden, J.; Klarenbeek, B.; FORCE trial group. Pelvic Floor Rehabilitation After Rectal Cancer Surgery One-year follow-up of a Multicenter Randomized Clinical Trial (FORCE trial). Ann. Surg. 2024. [Google Scholar] [CrossRef]
- Asnong, A.; D’Hoore, A.; Van Kampen, M.; Wolthuis, A.; Van Molhem, Y.; Van Geluwe, B.; Devoogdt, N.; De Groef, A.; Guler Caamano Fajardo, I.; Geraerts, I. The Role of Pelvic Floor Muscle Training on Low Anterior Resection Syndrome: A Multicenter Randomized Controlled Trial. Ann. Surg. 2022, 276, 761–768. [Google Scholar] [CrossRef]
- Coppersmith, N.A.; Schultz, K.S.; Esposito, A.C.; Reinhart, K.; Ray, E.; Leeds, I.L.; Pantel, H.J.; Reddy, V.B.; Longo, W.E.; Mongiu, A.K. Pelvic Floor Physical Therapy Prehabilitation (PrePFPT) for the prevention of low anterior resection syndrome. Surg. Oncol. Insight 2024, 1, 100097. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | Overall Cohort (n = 42) | Major LARS (n = 33) | No/Minor LARS (n = 9) | p-Value |
|---|---|---|---|---|
| Age, years, mean (SD) | 59.4 (10.9) | 59.6 (10.6) | 60 (26.8) | 0.914 |
| Sex, female, n (%) | 17 (41) | 12 (37) | 5 (56) | 0.446 |
| BMI, kg/m2, mean, (SD) | 26.8 (4.9) | 26.8 (4.6) | 26.8 (6.4) | 0.976 |
| Pathologic stage, n (%) | 0.438 | |||
| Complete pathologic response/in situ, n (%) | 12 (29) | 10 (30) | 2 (22) | |
| Stage 1 | 10 (24) | 9 (27) | 1 (11) | |
| Stage 2 | 6 (14) | 5 (16) | 1 (11) | |
| Stage 3 | 14 (33) | 9 (27) | 5 (56) | |
| Neoadjuvant chemoradiation, n (%) | 35 (83) | 29 (88) | 6 (67) | 0.155 |
| Neoadjuvant chemotherapy, n (%) | 7 (17) | 7 (21) | 0 (0) | 0.123 |
| Diverting ileostomy at time of LAR, n (%) | 38 (91) | 31 (97) | 6 (67) | 0.006 |
| Duration of diverting ileostomy, months, median (IQR) | 5.5 (3.5–7) | 5 (2–6) | 7 (5.8–8.5) | 0.032 |
| Distance from anal verge, cm, mean (SD) | 9.3 (4.6) | 9.4 (4.4) | 9 (5.5) | 0.809 |
| Time since most recent surgery, months, median (IQR) | 36.5 (15–50) | 37 (16.5–51) | 36 (12.5–50) | 0.526 |
| Sensory CIPN score, median (IQR) | 29.6 (13–53) | 29.6 (17–52) | 22 (5.6–70) | 0.833 |
| Variable | Standardized Coefficients (Beta) | Standard Error | T-Statistic | p-Value |
|---|---|---|---|---|
| Sensory CIPN score | 0.27 | 0.036 | 2.07 | 0.046 |
| Diverting loop ileostomy | 0.57 | 4.5 | 2.9 | 0.006 |
| Neoadjuvant chemoradiation | 0.02 | 3.5 | 0.08 | 0.94 |
| Distance from anal verge | 0.16 | 0.21 | 1.2 | 0.26 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Linhares, S.M.; Schultz, K.S.; Coppersmith, N.A.; Esposito, A.C.; Leeds, I.L.; Pantel, H.J.; Reddy, V.B.; Mongiu, A.K. Association Between Chemotherapy-Induced Peripheral Neuropathy and Low Anterior Resection Syndrome. Cancers 2024, 16, 3578. https://doi.org/10.3390/cancers16213578
Linhares SM, Schultz KS, Coppersmith NA, Esposito AC, Leeds IL, Pantel HJ, Reddy VB, Mongiu AK. Association Between Chemotherapy-Induced Peripheral Neuropathy and Low Anterior Resection Syndrome. Cancers. 2024; 16(21):3578. https://doi.org/10.3390/cancers16213578
Chicago/Turabian StyleLinhares, Samantha M., Kurt S. Schultz, Nathan A. Coppersmith, Andrew C. Esposito, Ira L. Leeds, Haddon J. Pantel, Vikram B. Reddy, and Anne K. Mongiu. 2024. "Association Between Chemotherapy-Induced Peripheral Neuropathy and Low Anterior Resection Syndrome" Cancers 16, no. 21: 3578. https://doi.org/10.3390/cancers16213578
APA StyleLinhares, S. M., Schultz, K. S., Coppersmith, N. A., Esposito, A. C., Leeds, I. L., Pantel, H. J., Reddy, V. B., & Mongiu, A. K. (2024). Association Between Chemotherapy-Induced Peripheral Neuropathy and Low Anterior Resection Syndrome. Cancers, 16(21), 3578. https://doi.org/10.3390/cancers16213578