Simple Summary
Cancer immunotherapies, while revolutionary in boosting the immune system to fight cancer, can also trigger serious side effects, including inflammation of the brain. We review the existing literature on encephalitis with a special focus on cancer treatment-related encephalitis, including its etiopathogenesis, differential diagnosis, and identification of optimal diagnostic approaches and treatment strategies. This review aims to help clinicians from oncology and neurology improve the diagnosis and management of this condition, help reduce complications, improve patient outcomes, and inform future therapeutic approaches.
Abstract
Encephalitis associated with cancer therapies is a rare but serious complication that can significantly impact patients’ quality of life and it requires prompt identification and management. Over the past two decades, immunotherapy—particularly immune checkpoint inhibitors—has become a cornerstone of cancer treatment, with up to half of metastatic cancer patients in economically developed countries now receiving these therapies. The widespread adoption of immunotherapy has led to improved survival rates and long-term remissions, even in patients with advanced metastatic disease. However, as immune modulators, these therapies can trigger a range of immune-related adverse events, including a variety of novel neurological toxicities. Among these, encephalitis is of particular concern due to its potential severity, which can compromise treatment outcomes. This review aims to provide a comprehensive overview of the literature on this condition, highlighting optimal diagnostic strategies and management approaches to mitigate the risk of significant morbidity, while also comparing encephalitis induced by immunotherapy with that caused by traditional chemotherapies and targeted oncologic treatments.
Keywords:
cancer; adverse event; neurotoxicity; encephalitis; autoimmune; immunotherapy; checkpoint inhibitor; CAR-T; ICANS; BiTE 1. Introduction
1.1. Encephalitis
Encephalitis is an inflammation of the brain parenchyma, often involving the cortical or deep gray matter, with or without the involvement of white matter, meninges, or spinal cord. It generally results from a direct viral infection or an autoimmune process that may be postinfectious, paraneoplastic, or idiopathic. The typical clinical presentation is a combination of fever, headache, and altered mental status (behavior, personality, cognition, and consciousness). Focal neurological deficits, seizures, movement disorders, and/or autonomic instability are often associated. Unfortunately, symptoms remain largely nonspecific, and given the multiple etiologies, diagnosis of encephalitis remains challenging [1]. The typical diagnosis relies mostly on clinical symptoms and workup requires serum and cerebrospinal fluid (CSF) analysis, neuroimaging, and electroencephalography (EEG) [2]. Autoantibody testing should be considered in all cases, especially those with a recognizable autoimmune encephalitis phenotype [3].
Based on the International Encephalitis Consortium [4], encephalitis is defined as an altered mental status lasting 24 h or more, without alternative cause and at least two of the following:
- Fever above 38 °C within the last 72 h.
- New focal neurological signs.
- New epileptic seizure activity, unrelated to a pre-existing condition
- Signs of encephalitis on MRI.
- Abnormal EEG findings consistent with encephalitis.
- CSF pleocytosis.
However, most patients with encephalitis will not present a severely depressed Glasgow coma scale (GCS) score on admission and may even perform well on basic cognitive assessments such as mini-mental-status (MMS), or Montreal Cognitive Assessment (MoCA) tests, and might, especially in autoimmune or paraneoplastic forms, lack fever or CSF pleocytosis [1].
Encephalitis can be broadly classified as infectious or autoimmune [5,6]. Infectious encephalitis is beyond the scope of this review, is mostly viral in origin, and has been reviewed by Tyler et al. in the New England Journal of Medicine [2]. Autoimmune encephalitis (AE) is a group of non-infectious immune-mediated inflammatory diseases. In some (but not all) cases of AE, a specific autoantibody directed against a CNS antigen can be detected in the serum or cerebrospinal fluid [7]. The most common etiologies are associated with antibodies against leucine-rich glioma-inactivated 1 (LGI1) and contactin-associated protein-like 2 (CASPR2), and in patients under 50, autoantibodies against the N-methyl-D-aspartate receptor (NMDAR) are observed at similar frequencies [8]. In addition to these two autoantibodies, more than a dozen new types of autoantibodies have been identified in the last 15 years, and their incidence is increasing [7]. These antibodies are typically directed against extracellular domains of neuroglial proteins [9].
Autoimmune encephalitis is often observed as a paraneoplastic syndrome. One of the best and most comprehensively described models for this is the association of ovarian teratomas with anti-NMDAR AE [10], with up to 25% of patients with anti-NMDAR AE having an ovarian teratoma [11]. Paraneoplastic neurological disorders are usually subacute at onset, progressive due to accelerated neuronal death, have a poor prognosis, and are typically detected months to years before a tumor is diagnosed [12,13]. Brain imaging may show no abnormal findings. Testing for anti-NMDAR antibodies in the cerebrospinal fluid may be useful, but is not necessary to make a diagnosis of CNS toxicity related to an autoimmune process [14]. In contrast to classical autoimmune encephalitis, patients with paraneoplastic etiology show significantly less clinical improvement when treated with steroids and intravenous immunoglobulin [15]. In paraneoplastic encephalitis, a cancer elicits an immune-mediated response directed against CNS antigens, primarily by molecular mimicry. Specific autoantibodies associated with particular tumors (Table 1) are typically directed against intracellular targets [13]. For example, up to 50% of patients with gamma-aminobutyric acid B receptor [GABABR] [16] and α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor (AMPAR) [17] encephalitis have been shown to have cancer. Notably, the presence of onconeural antibodies such as anti-Hu and anti-Ma2 are almost always associated with an underlying cancer in adults [13]. Interestingly, the incidence of such paraneoplastic encephalitis increases with checkpoint inhibitors [18,19] and is discussed below.

Table 1.
High and intermediate risk tumor-associated autoantibody-mediated encephalitis.
In addition to the encephalitis described above, which is better defined as limbic encephalitis, paraneoplastic neurologic syndromes may include encephalomyelitis, sensory neuronopathy, opsoclonus-myoclonus, enteric neuropathy, rapidly progressive cerebellar syndrome, and Lambert–Eaton myasthenic syndrome. These conditions have been reviewed by Graus et al. [13]. The term encephalomyelitis (EM) only applies to patients presenting neurological dysfunction at multiple sites, affecting both central and peripheral nervous systems, including dorsal root ganglia, peripheral nerve, or nerve roots [13]. Rapidly progressive cerebellar syndrome (RPNS), as its name suggests, is a rapidly progressive, severe, and bilateral cerebellar syndrome limiting daily activities in less than 3 months and is characterized by the absence of substantial cerebellar atrophy on imaging [13]. RPNS has only been described in small patient series but appears to be associated with anti-Yo and Tr/delta/notch-like epidermal growth factor-related receptor (DNER) antibodies [13]. Opsoclonus-myoclonus syndrome (OMS) consists of involuntary, chaotic, multidirectional, high-frequency, saccadic movements of the head, trunk, and limbs. Signs of encephalopathy (ranging from confusion to coma) and cerebellar involvement (dysarthria or truncal ataxia) have also been reported. Paraneoplastic OMS in adults is most often associated with SCLC or breast cancer and is mostly associated with anti-Ri antibodies [13].
Finally, acute demyelinating encephalomyelitis (ADEM) also constitutes an important cause of non-infectious encephalitis. ADEM is defined as an autoimmune demyelinating disease caused by an autoimmune response. This immune response is thought to be post-infectious or following vaccination, although this has never been proven. It presents as an acute onset encephalopathy associated with polyfocal neurologic deficits preceded by fever, malaise, irritability, somnolence, headache, nausea, and vomiting. It is seen primarily in pediatric populations and is often associated with antibodies to myelin oligodendrocyte glycoprotein [20].
1.2. Immune Checkpoint Inhibitors
Over the past two decades, immune checkpoint inhibitors (ICIs) have become a mainstay of cancer therapy, with up to half of metastatic patients in economically developed countries now receiving ICIs [21]. ICIs enhance antitumor immunity by blocking immune checkpoint molecules expressed on the surface of T lymphocytes and tumor cells, such as cytotoxic T lymphocyte-associated antigen 4 (CTLA-4), programmed cell death protein 1 (PD-1), and its ligand (PD-L1) [22]. Today, more than 50 different malignancies can be treated with 10 approved ICIs either as monotherapy or in combination in the neoadjuvant, adjuvant, or palliative setting [23,24] (Table 2). The introduction of ICIs into routine oncology practice has led to increased survival and long-term remissions, even in patients with extensive metastatic cancer [21].
Table 2.
Approved immune checkpoint inhibitors and indications.
ICIs are surface receptors expressed by immune cells that regulate immune homeostasis. PD-1 and its primary ligand PD-L1 are expressed on T cells and tumor cells, respectively, resulting in T cell exhaustion upon interaction. This mechanism is exploited by tumor cells to avoid immune elimination [21]. Thus, PD-1/PD-L1 like LAG-3 inhibition acts directly at the tumor site, whereas CTLA-4 inhibition acts mainly during T cell priming when antigen-presenting cells (APC) and the T cells interact in lymph nodes.
2. Checkpoint Inhibitor-Induced Encephalitis
Although very beneficial, ICIs come at a cost: A major drawback is the development of immune-related adverse events (irAEs), including serious (grade 3 or higher) neurologic syndromes (1–3% of cases) [25,26,27,28]. Although neurologic adverse events from ICIs are less common than those from chemotherapy, they must be considered, as they account for 11% of all fatal adverse events linked to ICIs. [24]. These include the exacerbation of pre-existing and the de novo development of autoimmune neurological diseases of a central and/or peripheral nature.
Typically, ICIs have been associated with peripheral neuropathies, Guillain-Barré syndrome, myasthenia gravis, Tolosa–Hunt syndrome, and autoimmune encephalitis [25,27]. Checkpoint inhibitor-induced encephalitis (CIIE) is a rare (0.1–1%) but serious complication of checkpoint inhibitor immunotherapy, with increasing incidence with concurrent or sequential ICI treatment [29]. Interestingly, although the majority of autoimmune diseases are diagnosed in women, gender has not been found to be a specific risk factor for immune-related adverse events linked to checkpoint inhibitors [30]. With regard to encephalitis specifically, sufficient demographic data are lacking. Moreover, ICI is mostly used in lung, melanoma, and urinary tract tumors that typically predominantly affect men, the gender-specific analysis of adverse events is inherently biased. Removal of such a confounding factor will require large patient numbers that will only be obtained once very large data series of those rare side effects linked to ICIs are available.
The exact mechanism by which checkpoint inhibitors lead to CIIE is not fully understood. It is thought to involve an immune response to brain tissue, as seen in autoimmune and paraneoplastic encephalitis. Risk factors for developing CIIE include a history of autoimmune disease, prior radiation therapy, and concurrent infections.
As an illustrative case, a patient with pulmonary adenocarcinoma and type 1 diabetes developed GAD65 antibody-positive encephalitis while receiving nivolumab [31]. GAD65 is expressed on pancreatic islet cells and GABAergic neurons. In seropositive cases, autoantibodies against neuronal surface/synaptic antigens in the limbic system are usually found [32,33]. Mechanistically, antibody/antigen binding can lead to complement deposition, antigen internalization, and modulation of the function of the antigenic target. The origins and sources of these autoantibodies are generally unclear but may be secondary to previous infections, or paraneoplastic [34]. In contrast to classic PNS, which are known to precede the detection of cancer, ICI-induced neurological syndromes, by definition, develop when the cancer is already diagnosed, generally within weeks to months after the initiation of ICIs. Whether pre-existing autoreactivity is unleashed or, on the contrary, generated de novo remains unclear.
Recent data showed an increased incidence of anti-Ma2 autoimmune limbic encephalitis in patients receiving nivolumab, pembrolizumab, or a combination of ipilimumab and nivolumab [35]. A case of anti-NMDAR positive CSF in a melanoma patient treated with checkpoint inhibitors has been reported by Williams et al. [14]. We have published a case of anti-Hu positive limbic encephalitis in a patient with NSCLC who was treated with ipilimumab and nivolumab [36]. However, many cases remain seronegative despite thorough screening and antibody detection is not required to classify symptoms as irAEs. In a review of 47 cases of CIIE by Stuby et al., one or more autoantibodies (anti-CASPR2, anti-GAD65, anti-AGNA, anti-Hu, anti-NMDAR, anti-Ma2, anti-Ri, and anti-TPO/TG) were detected in 52% of patients treated with ipilimumab, nivolumab, pembrolizumab, or atezolizumab. Moreover, 29/47 cases (62%) were identified in anti-PD-1 ICI monotherapy patients and 5/47 cases (11%) in anti-CTLA-4 ICI monotherapy patients. The concurrent or sequential use of CTLA-4 and PD-1 inhibitors caused encephalitis in 9/47 cases (19%) [37]. In a more recent series by Farina et al., with 71 cases of CIIE mostly with single agent anti-PD1/PD-L1 ICI, anti-paraneoplastic autoantibodies (anti-Hu, Ma2, and Yo antibodies) were found in 84% of patients with focal encephalitis. In meningoencephalitis patients, however, 37% remain antibody-negative, 25% with non-specific brain reactive autoantibodies, and 33% with non-paraneoplastic autoantibodies (such as anti-GAD65) [38].
There is growing interest in the relationship between the gut–brain axis, neuroinflammation, and the role of ICIs. The microbiota–gut–brain axis is a complex and multi-faceted network that connects the brain and gut through a variety of immunological, hormonal, and neural signals. An imbalance in gut microbiota (dysbiosis) can affect and trigger neuroinflammation and microglial activation [39]. In murine models, alteration in the gut–brain axis has been shown to disrupt the blood–brain barrier and to be linked to CNS autoimmune diseases such as encephalomyelitis and multiple sclerosis [40]. Similarly, it is postulated that the gut microbiota may influence the effectiveness of ICIs by directly regulating immune cells and modulating the immune system through the gut–brain axis [41]. Whether the gut–brain axis and the microbiota play a role in CIIE remains largely unknown but represents an important emerging topic of research.
2.1. Diagnosis of CIIE
Diagnosis of CIIE can be challenging because symptoms can be subtle and indistinguishable from other causes of encephalitis, including viral infections. Any patient with altered mental status and fever without an obvious cause should be treated as having a central nervous system (CNS) infection until proven otherwise [42]. CIIE remains a diagnosis of exclusion (Table 3), but it is important for healthcare providers to consider CIIE in the differential diagnosis of patients receiving checkpoint inhibitors who present with a decreased level of consciousness, confusion, headache, fever, seizures, and/or focal neurologic deficits. The time interval between initiation of ICI therapy and the onset of symptoms is highly variable, ranging from less than a week to up to 2 years, with a median of 6 to 9 weeks [27,37]. In cases of uncertainty, neuronal damage biomarkers such as neurofilament light chain (NfL) and S100B can quickly signal neuroaxonal damage. These markers, though non-specific, help in flagging patients for further neurological evaluation, particularly when antibody tests are negative [43].
Table 3.
Differential diagnosis to exclude and recommended work-up.
Diagnosis is usually based on a combination of clinical presentation, imaging studies, and laboratory tests. CSF analysis must be performed to rule out infectious etiologies (bacterial, fungal, or viral meningoencephalitis) and leptomeningeal disease. Typical CSF findings in patients with CIIE are pleocytosis with predominantly lymphocytes and elevated protein concentrations. Glucose levels are unaffected. CSF polymerase chain reaction (PCR) for herpes simplex virus type 1 (HSV-1), herpes simplex virus type 2 (HSV-2), and varicella-zoster virus (VZV) should be ordered. Since we are dealing with cancer patients, a cytological examination of the cerebrospinal fluid is recommended.
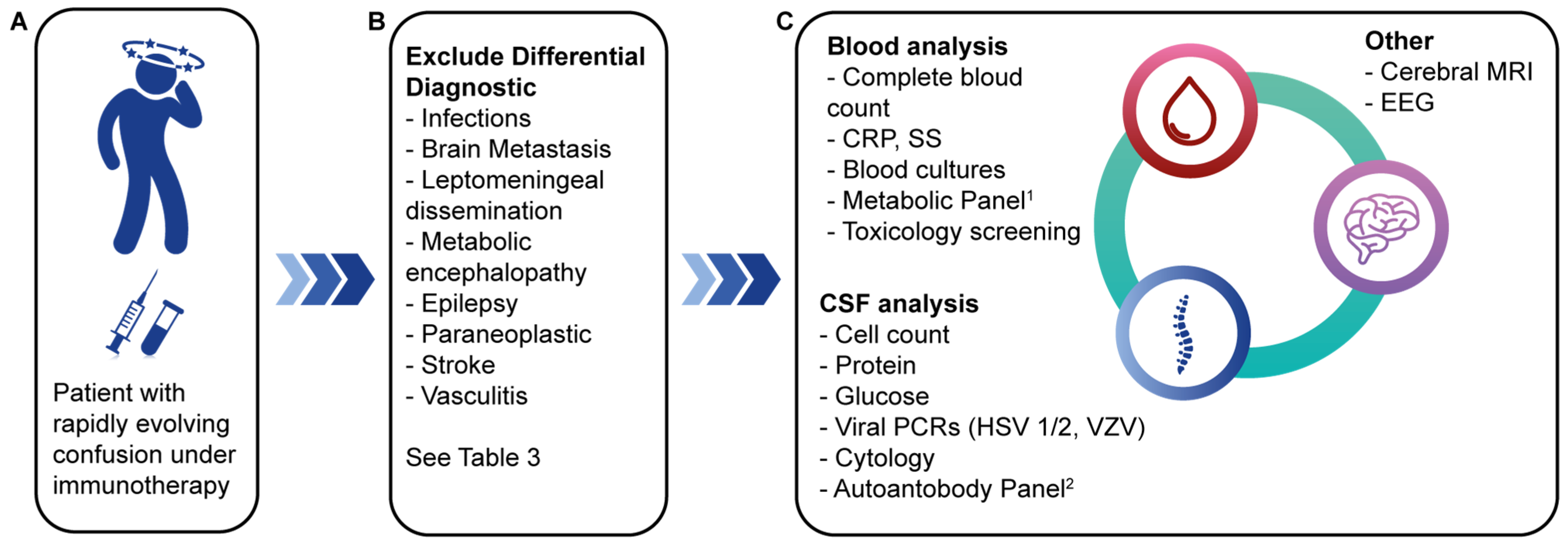
A cerebral MRI is part of the workup to rule out brain metastases, ischemia, and intracranial hemorrhage. An EEG can rule out nonconvulsive status epilepticus. A complete laboratory work-up is performed, including a complete blood count, a C-reactive protein (CRP) test, a comprehensive metabolic panel (including ammonia), blood concentrations of vitamins (B1, B12), an evaluation of the pituitary hormonal axes with thyroid-stimulating hormone (TSH) and cortisol. Blood and urine cultures should be obtained. Antineutrophil cytoplasmic antibody (ANCA) titers should be measured to rule out vasculitis. If intoxication is suspected, a toxicology screen should be performed [28,44]. There are no specific tests for CIIE; in the case series by Stuby et al., less than 50% of performed MRIs revealed findings consistent with encephalitis. No encephalitis-specific EEG pattern was found, although epileptiform spikes were seen in 30% of EEGs. CSF pleocytosis and elevated CSF protein levels were found in a majority of patients [37]. A summary of the diagnostic approach and workup is illustrated in Figure 1.
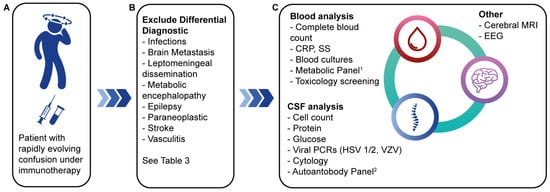
Figure 1.
Diagnosis of ICI-induced encephalitis. (A) Early symptoms, especially confusion, must raise suspicion of encephalitis. (B) Differential diagnosis to be evoked; (C) workup to be done. 1 Metabolic panel: electrolytes, glucose, creatinine, bilirubin, liver enzymes, ammonia, arterial blood gas analysis, vitamins B1 and B12, thyroid function tests, basal cortisol concentration, ANCA; 2 autoantibody panel: autoantibodies: AGNA (SOX1), AMPAR1/2, Amphiphysin, CRMP5 (CV2), DPPX, GABAR, GAD65, Hu (ANNA1), Ma1, Ma2, Ri (ANNA2), TG, TPO, TR, VGKC (anti-LGI1, anti-CASPR2), Yo (PCA1), ZIC44; Paraneoplastic antibodies: NMDAR, AMPAR1/2, VGKC (anti-LGI1, anti-CASPR2), Gly, GABAR. Abbreviations: ANCA = antineutrophil cytoplasmic antibody; CRP = C-reactive protein; CSF = cerebrospinal fluid, EEG = electroencephalogram > HSV-1 = herpes simplex virus type 1; HSV-2 = herpes simplex virus type 2, MRI = magnetic resonance imaging; PCR = polymerase chain reaction; SS = sedimentation speed; VZV = varicella-zoster virus. Adapted from [37].
2.2. Management of CIIE
Immune-mediated encephalitis is generally graded from 3 to 4 and requires permanent discontinuation of ICI. The standard of care is corticosteroids, which should be started as soon as possible after differential diagnoses have been ruled out. The search for autoimmune encephalitis or paraneoplastic antibodies should not delay the initiation of treatment, as they can be quantified even in the presence or after corticosteroids. Intravenous methylprednisolone at a dose of 1 to 2 mg/kg body weight/day is recommended initially [45,46]. In severe cases, the corticosteroid dose may be increased to ≥10 mg/kg daily. With such doses of corticosteroids, adverse events such as delirium, insomnia, hyperglycemia, or immunosuppression should be expected. As usual, in immunosuppressed patients, prophylaxis with trimethoprim/sulfamethoxazole (300 mg, three times a week) and acyclovir (500 mg daily) is indicated. In some cases, corticosteroid treatment becomes chronic, but ideally, treatment should be discontinued if possible. In this case, the steroids should be slowly tapered over a period of at least four weeks [45,46].
In steroid-refractory cases, treatment with intravenous immunoglobulins (IVIG), plasmapheresis, or rituximab should be considered [1,45,47]. We have successfully treated an NSCLC patient with anti-Hu-positive autoimmune limbic encephalitis on ipilimumab and nivolumab with natalizumab, an antibody that blocks the α4β1 integrin on blood–brain barrier endothelial cells, limiting lymphocyte recruitment into the CNS [36].
It is important for healthcare providers to be aware of the risk of CIIE and to closely monitor patients receiving checkpoint inhibitor immunotherapy for signs or symptoms of this complication. Early detection and treatment of CIIE can help improve patient outcomes. Early diagnosis and appropriate treatment improve patient outcomes, and symptom control is achieved in the majority of patients (82%). However, despite optimal management and supportive care, CIIE remains a serious complication with an in-hospital mortality of nearly 20%, depending on the series [37].
2.3. Monitoring of the Evolution of CIIE
Neural antibodies are well-recognized biomarkers of autoimmune and paraneoplastic encephalitis and treatment response and outcome largely depend on the targeted antigen. Antibodies against intracellular antigens (anti-Hu, Ma2, Yo) are associated with poor outcomes whereas antibodies against cell-surface antigens (anti-NMDAR, LGI1, CASPR2) are associated with more favorable outcomes [43]. Likewise, the prognostic value of neural antibodies has also been demonstrated in CIIE. Paraneoplastic antibodies were found associated with a lower probability of treatment response and higher risk of mortality as opposed to GFAP or neuron-surface antibodies [38].
3. Immunotherapy-Induced Acute Demyelinating Encephalomyelitis
Although atypical, Zafar et al. described a case of nivolumab-induced acute demyelinating encephalomyelitis (ADEM) [15]. Two weeks after starting palliative nivolumab immunotherapy, a patient with relapsed and metastatic laryngeal squamous cell carcinoma exhibited progressive weakness, altered mental status, and progressive dyspnea requiring intubation. A cMRI showed multiple hyperintense T2 flair white matter lesions without contrast enhancement or restricted diffusion, consistent with acute demyelinating encephalomyelitis. Similar to the encephalitis cases above, 5 days of intravenous methylprednisolone and immunoglobulin (IVIg) therapy allowed gradual improvement of motor symptoms.
4. Activated T Cell-Induced Encephalitis
4.1. Chimeric Antigen Receptor T-Cells
Chimeric antigen receptor T-cells (CAR-T cells) are a new approach in clinical cancer therapy and a form of tumor immunotherapy. The basic idea behind this approach is to harvest the patient’s T cells, provide them with receptors specific for tumor surface markers, and return them to the patient where they will eliminate tumor cells.
CAR-T cells are genetically engineered to express a chimeric transmembrane receptor that includes an extracellular single-chain variable fragment (scFv) targeting tumor antigens. This scFv fragment is linked via a hinge and transmembrane domain to intracellular T cell signaling domains. These signaling domains comprise the CD3 zeta chain (CD3ξ) of the T-cell receptor (TCR), which contains the immunoreceptor tyrosine-based activation motif (ITAM), as well as costimulatory domains from CD28 and 4-1BB. To date, all approved CAR-T cell therapies treat hematologic malignancies [48]. In total, six CAR-Ts have been approved, four of which are directed against CD19 in B-cell malignancies, primarily diffuse large B-cell lymphoma (DLBCL): axicabtagene ciloleucel (YESCARTA®) [49], tisagenlecleucel (KYMRIAH®) [50], brexucabtagene autoleucel (TECARTUS®) [51]. Lisocabtagene maraleucel (BREYANZI®) [52] and two directed against BCMA in multiple myeloma idecabtagene vicleucel (ABECMA®) [53] and ciltacabtagene autoleucel (CARVYKTI®) [54].
4.2. Chimeric Antigen Receptor T-Cell Related Encephalopathy
CAR-T-related encephalopathy (CRES) is a CAR-T-mediated CNS toxicity associated with significant morbidity and mortality that may hinder the expansion of CAR-T therapies. CRES has recently been renamed immune effector cell-associated neurotoxicity syndrome (ICANS) because similar neurotoxic symptoms have been reported with other immune effector cell-engaging therapies, such as bi-specific T-cell engagers (blinatumomab) [55].
ICANS is relatively common, affecting up to 45% of patients with severe, sometimes fatal, neurological symptoms [56,57,58,59]. This syndrome has been observed not only with CARs targeting CD19 but also with those targeting CD22 and BCMA. ICANS can occur with CARs containing either CD28 or 4-1BB costimulatory domains, although the incidence varies: up to 45% in patients with CD28-based CARs compared to only 13% with 4-1BB-based constructs [60,61,62]. The underlying mechanisms of these toxicities are not fully understood, but key features of ICANS include endothelial activation and disruption of the blood–brain barrier, leading to brain edema due to cytokine release by CAR-T cells [58,59,60,63,64,65]. Indeed, a report by Norelli et al. showed that proinflammatory cytokines and myeloid cells are involved in addition to activated T cells [66]. This leakage leads to cerebral edema, hemorrhage, infarction, and necrosis due to intravascular coagulation (DIC) [59]. The latter can be measured in the blood of patients with severe neurotoxicity, as they have significantly elevated DIC markers [60]. Elevated levels of the excitatory NMDA receptor agonists glutamate and quinolinic acid have also been shown in the cerebrospinal fluid of patients with neurotoxicity [67].
Although ICANS can develop without the presence of cytokine release syndrome (CRS), patients typically experience both conditions concurrently (91%). Clinically, CRS resembles septic shock and is characterized by high fever, tachycardia, hypotension, myalgia, respiratory failure, vascular leakage, coagulopathy (disseminated intravascular coagulation, or DIC), and oliguria, which can lead to multiple organ failure in severe cases [45,61,62]. It is a systemic phenomenon that has the potential to affect any organ, including the nervous system. The severity of ICANS is proportional to that of the CRS and is, therefore, closely related to in vivo T-cell expansion, with ICANS occurring when CAR-T levels are highest [59,60]. ICANS typically present 4–5 days after CAR T-cell administration, but delayed onset occurring 3–4 weeks after CAR T-cell treatment has been reported [57]. Clinically, ICANS follows a stereotypical progression, beginning with somnolence, confusion, attention deficit, disorientation, and mild aphasia. These symptoms can then worsen to include aphasia, hallucinations, delirium, myoclonus, and tremors. In severe cases, patients may experience generalized seizures and encephalopathy, leading to coma and potentially death [45,60,66]. EEG findings typically show nonspecific diffuse generalized slowing triphasic waves. Such patients risk developing posterior reversible encephalopathy syndrome (PRES) and acute necrotizing encephalopathy [59,64].
Unlike conventional CRS, for which tocilizumab is routinely used, ICANS does not respond well to IL-6R blockade. Intravenous methylprednisolone and antiepileptic drugs (levetiracetam) appear more effective in this situation [60,64]. Plasmapheresis has been proposed as it is used in thrombotic thrombocytopenic purpura, which shares similar endothelial cell activation mechanisms, but this approach has yet to be validated [68].
ICANS grading and management guidelines have been published by the American Society of Bone Marrow Transplantation (Table 4) [64].
Table 4.
Diagnosis and management of ICANS.
4.3. Bispecific T Cell Engager Immunotherapy (BiTEs)
Bi-specific T-cell engagers (BiTEs) can be considered at the interface between ICI and CAR-T, as they are an antibody-based, infused drug, but directly confer a novel T-cell specificity. To date, five BiTEs have been approved, blinatumomab (BLINCYTO®), a CD-19-targeting construct indicated as second-line treatment for Philadelphia chromosome-negative relapsed or refractory acute lymphoblastic leukemia [69], tebentafusp (KIMMTRAK®), a bispecific gp100 peptide-HLA-directed CD3 T-cell engager indicated for the treatment of HLA-A*02: 01-positive adult patients with unresectable or metastatic uveal melanoma [70], glofitamab, (COLUMVI®) a bispecific CD20-CD3 monoclonal antibody used for the treatment of diffuse large B-cell lymphoma [71], mosunetuzumab, (LUNSUMIO®), also a CD20-CD3 BiTE is used for the treatment of follicular lymphoma [72], and finally talquetamab, (TALVEY®), a humanized GPRC5D-CD3 BiTE is used in the treatment of multiple myeloma [73]. Many more are under development and will reach the market soon [74].
BiTEs induce systemic AEs similar to CAR T cell toxicity with the typical development of fever, headache, neutropenia, and cytokine release syndrome. However, this therapy is also known to induce neurologic adverse events in up to half of treated patients. These include tremors, seizures, confusion, febrile delirium, (leuko)encephalopathy, and cerebellar ataxia. Up to 30% of patients experience Grade 3 symptoms [75,76]. These nAEs typically occur early in treatment (median onset = 9 days) and are generally reversible and manageable with high-dose dexamethasone (3 × 8 mg/day for 4 days) and interruption of the BiTE infusion. Premedication with 20 mg of dexamethasone IV, administered 1 h prior to BiTE infusion, is recommended to minimize the risk of nAE development. Patients experiencing grade 4 symptoms or seizures should be permanently discontinued. Otherwise, treatment may be resumed once symptoms have resolved to grade 1 or have disappeared. Although not fully understood, BiTE nAEs are thought to result from transient neuroinflammation in the CNS due to endothelial adherence of BiTE-activated T cells [75].
5. Chemotherapy-Induced Encephalitis
Chemotherapy is known to induce chemotherapy-induced toxic (leuko)encephalopathy, or “chemobrain”, which is clinically characterized by progressive cognitive dysfunction. However, this chronic and progressive form of neurotoxicity is not the only one induced by chemotherapy regimens. In fact, several cytostatic drugs can damage the central nervous system after systemic (intravenous, oral) or topical (i.e., intrathecal, intraventricular, or intraarterial) administration. Cytotoxic drug-associated clinical syndromes are classified into 11 categories: acute encephalopathy, aseptic meningitis, cerebellar dysfunction, cerebral infarction, chronic encephalopathy, cortical blindness, multifocal leukoencephalopathy, posterior reversible (leuko)encephalopathy syndrome (PRES), thrombotic microangiopathy, seizure, and subacute encephalopathy [77]. For the scope of this review, we will only discuss systemic chemotherapy applications and acute complications.
The incidence of CNS toxicity depends on a number of factors, including the chemotherapeutic substance administered, its dosage (single and cumulative), the duration of treatment, the infusion speed, and additional risk factors including preexisting neurological conditions. The cytostatics most associated with CNS toxicity are cytarabine (Ara-C), ifosfamide, and methotrexate (MTX) [77]. These drugs are known to cause acute encephalopathy, which develops within hours to days after infusion. Patients display typical symptoms of somnolence, confusion, disorientation, agitation, and focal stroke-like symptoms such as hemiparesis, ataxia, dysarthria, and possibly even coma [78]. Myoclonic jerks, seizures, and hallucinatory symptoms may occur [79,80]. If untreated, acute encephalopathy may progress to chronic leukoencephalopathy with chronic sequelae.
As above, a broad differential diagnosis including infectious encephalitis, non-convulsive epileptic status, paraneoplastic syndrome, metabolic disorders, and brain metastasis is to be excluded [78]. Cytotoxics commonly associated with acute encephalopathy are 5-fluorouracil (5-FU), cytosine arabinoside (Ara-C), etoposide/VP16 (high dose), ifosfamide (10–15% of patients treated with doses > 1 g/m2), interferon-α, interleukin-2, methotrexate (MTX), nitrosoureas (high dose), paclitaxel, procarbazine, and tamoxifen (high dose) [78]. Table 5 provides a non-exhaustive summary of medications, associated symptoms, risk factors, and management.
Table 5.
Therapy/prophylaxis of chemotherapy-induced CNS toxicity. Adapted from [78].
Cases of acute encephalopathy and focal neurological deficits require urgent intervention to prevent the development of chronic leukoencephalopathy. Once established, there is no treatment available to reverse the chronic changes. Keeping in mind the absence of consensus on the best management of acute toxicity, several treatment approaches have been investigated with variable success rates. Treatment of MTX complications includes CSF drainage, ventriculo-lumbar perfusion with saline, and glucarpidase, a drug catabolizing an enzymatic cleavage degrading MTX into a non-toxic metabolite [81,82]. Unfortunately, leucovorin, routinely given to rescue patients from systemic MTX toxicities, cannot be given intrathecally. One fatal case has been reported [83].
Methylene blue, administered at a dose of 50 mg IV every 4 h, has been used successfully in the treatment of ifosfamide-induced encephalopathy, where it is thought to act as an alternative electron acceptor [84]. Ifosfamide and its metabolites are thought to interfere with thiamine functions. Thus, prophylaxis with 100 mg of thiamine IV every 4–6 h can be empirically administered to prevent ifosfamide-induced encephalopathy [85]. In all cases of acute encephalopathy, discontinuation of chemotherapy is often the only method to prevent further CNS toxicity [77,78,80]. However, none of these approaches have been evaluated prospectively or in a randomized manner.
Subacute encephalopathy is rare but may develop days to weeks after administration of certain cytostatic agents such as cisplatin or MTX, presenting as an abrupt onset of confusion, seizures, and focal signs such as hemiparesis or aphasia. It primarily affects children, but isolated cases have been reported in adults [86]. The mechanism of neurotoxicity is not well understood. Symptoms usually resolve spontaneously, but fatal outcomes have been observed [77].
Cerebellar and brain stem dysfunction with dysarthria, oculomotor disorders, and ataxia are typical complications of cytarabine, usually at cumulative doses over 36 g/m2 [77]. Autopsies have revealed widespread Purkinje cell loss. Fortunately, only isolated cases of complication have been reported at lower doses. Risk factors for the development of cerebellar dysfunction include advanced age, renal insufficiency, and elevated alkaline phosphatase. A similar cerebellar syndrome may be seen after treatment with high-dose 5-FU, which is reversible after interruption of therapy, but may recur with re-exposure to the drug [77].
Chemotherapy-induced autoimmune-mediated encephalitis is rare but has recently been described. A case of autoimmune encephalitis with oligoclonal bands in the cerebrospinal fluid has been reported in a 10-year-old patient treated for a pure germinoma in the suprasellar region. Her clinical status improved rapidly with steroids [87]. Similarly, a rare case of anti-Yo autoimmune encephalitis with confusion, behavioral changes, and seizures was reported in a 66-year-old patient receiving a capecitabine/oxaliplatin treatment [88]. Recently, chemotherapy for colorectal cancer has been shown to induce autoantibodies, although the pathophysiology is not yet understood [89].
Posterior reversible encephalopathy syndrome (PRES) typically presents itself with headache, paresis, blurred vision, nausea, seizures, and altered mental status. Risk factors include hypertension, eclampsia/preeclampsia, infection/sepsis, and cancer chemotherapy. Characteristic hyperintense parieto-occipital lesions involving gray and white matter are seen on T2-weighted MRI. These signal abnormalities are transient, and PRES is usually reversible upon withdrawal of the causative agent, but permanent disabilities have been reported. Despite a still largely unknown etiology, PRES is thought to be related to alterations in cerebrovascular autoregulatory control rather than direct drug cytotoxicity. It is hypothesized that exogenous toxins and chemicals may cause direct toxicity to the endothelium of the cerebral blood vessels, resulting in disruption of the blood–brain barrier. Chemotherapeutic drugs for which PRES has been reported include vincristine, oxaliplatin, gemcitabine, and doxorubicin [90,91,92]. No specific therapy has been shown to be effective in PRES; it is usually recommended to control possible hypertension and avoid the chemotherapeutic agent responsible in the future [78].
Targeted therapies may also cause encephalopathies. PRES has been described with several targeted therapies, including tyrosine kinase inhibitors such as sunitinib [93] and sorafenib [94]. Bevacizumab, a monoclonal antibody that inhibits angiogenesis by blocking vascular endothelial growth factor (VEGF), has also been implicated as a cause of PRES, particularly in patients with renal and colorectal cancer [95,96]. Rituximab, a monoclonal antibody targeting CD20 used to treat B-cell malignancies, is also capable of inducing PRES, although the pathophysiologic mechanism remains unknown [97].
Finally, radiation-induced CNS toxicity continues to be a significant cause of morbidity among cancer patients. Although there have been advances in creating more precise and safer radiation techniques, these improvements have been counterbalanced by the growing use of combined radio-chemotherapy regimens, the advent of radiosurgery, and the rising number of long-term survivors. However, these effects tend to develop over the long term and are due to general cerebral toxicity rather than encephalitis [98].
6. Conclusions
Although immunotherapy is revolutionizing cancer treatment and its use is rapidly expanding, it is associated with specific and often serious side effects that must be understood by treating physicians. Immunotoxicity and autoimmunity are common complications of checkpoint inhibitors and CAR T cells. Among the wide range of immune-related adverse events, neurological AEs, particularly encephalitis, are rare but represent an adverse outcome if not managed appropriately. The timing of symptom onset is highly variable, making patient monitoring and diagnosis difficult. Patients developing rapidly evolving confusion under ICI treatment should be suspected of having encephalitis. The diagnostic workup should include blood tests, CSF analysis, cerebral MRI, and an EEG. The treatment of choice relies on intravenous corticosteroids. Alternative treatment options include IVIG, rituximab, natalizumab, and plasma exchange therapy. However, current consensus guidelines are based on empirical data. Prospective clinical trials remain an important priority. Targeted therapies and chemotherapy can also induce encephalopathies to a lesser extent, some specific treatments have been discussed, but the main intervention remains treatment discontinuation.
Author Contributions
Writing—original draft preparation, N.P.D.; writing—review and editing, A.F.H.; funding acquisition, A.F.H. All authors have read and agreed to the published version of the manuscript.
Funding
Lundin Family Brain Tumor Research Centre covered the costs of publication of this review.
Acknowledgments
The authors thank Stéphanie Viguet-Carrin and Frédérique Landuyt for their administrative and editorial support.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Alam, A.M.; Easton, A.; Nicholson, T.R.; Irani, S.R.; Davies, N.W.; Solomon, T.; Michael, B.D. Encephalitis: Diagnosis, Management and Recent Advances in the Field of Encephalitides. Postgrad. Med. J. 2022, 99, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Tyler, K.L. Acute Viral Encephalitis. N. Engl. J. Med. 2018, 379, 557–566. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.; Zhang, J.; Greene, M.; Crivaro, A.; Gonzalez, J.; Kamoun, M.; Lancaster, E. Improving the Antibody-Based Evaluation of Autoimmune Encephalitis. Neurol. Neuroimmunol. Neuroinflammation 2017, 4, e404. [Google Scholar] [CrossRef] [PubMed]
- Venkatesan, A.; Tunkel, A.R.; Bloch, K.C.; Lauring, A.S.; Sejvar, J.; Bitnun, A.; Stahl, J.-P.; Mailles, A.; Drebot, M.; Rupprecht, C.E.; et al. Case Definitions, Diagnostic Algorithms, and Priorities in Encephalitis: Consensus Statement of the International Encephalitis Consortium. Clin. Infect. Dis. 2013, 57, 1114–1128. [Google Scholar] [CrossRef] [PubMed]
- Granerod, J.; Ambrose, H.E.; Davies, N.W.; Clewley, J.P.; Walsh, A.L.; Morgan, D.; Cunningham, R.; Zuckerman, M.; Mutton, K.J.; Solomon, T.; et al. Causes of Encephalitis and Differences in Their Clinical Presentations in England: A Multicentre, Population-Based Prospective Study. Lancet Infect. Dis. 2010, 10, 835–844. [Google Scholar] [CrossRef]
- Huang, C.-N.; Tian, X.-B.; Jiang, S.-M.; Chang, S.-H.; Wang, N.; Liu, M.-Q.; Zhang, Q.-X.; Li, T.; Zhang, L.-J.; Yang, L. Comparisons Between Infectious and Autoimmune Encephalitis: Clinical Signs, Biochemistry, Blood Counts, and Imaging Findings. Neuropsychiatr. Dis. Treat. 2020, 16, 2649–2660. [Google Scholar] [CrossRef]
- Graus, F.; Titulaer, M.J.; Balu, R.; Benseler, S.; Bien, C.G.; Cellucci, T.; Cortese, I.; Dale, R.C.; Gelfand, J.M.; Geschwind, M.; et al. A Clinical Approach to Diagnosis of Autoimmune Encephalitis. Lancet Neurol. 2016, 15, 391–404. [Google Scholar] [CrossRef]
- Zuliani, L.; Marangoni, S.; Gaspari, P.D.; Rosellini, I.; Nosadini, M.; Fleming, J.M.; Riva, V.D.; Galloni, E.; Perini, F.; Frigo, A.C.; et al. Epidemiology of Neuronal Surface Antibody-Mediated Autoimmune Encephalitis and Antibody-Based Diagnostics. J. Neuroimmunol. 2021, 357, 577598. [Google Scholar] [CrossRef]
- Lang, B.; Makuch, M.; Moloney, T.; Dettmann, I.; Mindorf, S.; Probst, C.; Stoecker, W.; Buckley, C.; Newton, C.R.; Leite, M.I.; et al. Intracellular and Non-Neuronal Targets of Voltage-Gated Potassium Channel Complex Antibodies. J. Neurol. Neurosurg. Psychiatry 2017, 88, 353. [Google Scholar] [CrossRef]
- Dalmau, J.; Tüzün, E.; Wu, H.; Masjuan, J.; Rossi, J.E.; Voloschin, A.; Baehring, J.M.; Shimazaki, H.; Koide, R.; King, D.; et al. Paraneoplastic Anti–N-methyl-D-aspartate Receptor Encephalitis Associated with Ovarian Teratoma. Ann. Neurol. 2007, 61, 25–36. [Google Scholar] [CrossRef]
- Irani, S.R.; Bera, K.; Waters, P.; Zuliani, L.; Maxwell, S.; Zandi, M.S.; Friese, M.A.; Galea, I.; Kullmann, D.M.; Beeson, D.; et al. N-Methyl-d-Aspartate Antibody Encephalitis: Temporal Progression of Clinical and Paraclinical Observations in a Predominantly Non-Paraneoplastic Disorder of Both Sexes. Brain 2010, 133, 1655–1667. [Google Scholar] [CrossRef]
- Darnell, R.B.; Posner, J.B. Paraneoplastic Syndromes Involving the Nervous System. N. Engl. J. Med. 2003, 349, 1543–1554. [Google Scholar] [CrossRef] [PubMed]
- Graus, F.; Vogrig, A.; Muñiz-Castrillo, S.; Antoine, J.-C.G.; Desestret, V.; Dubey, D.; Giometto, B.; Irani, S.R.; Joubert, B.; Leypoldt, F.; et al. Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes. Neurol. Neuroimmunol. Neuroinflammation 2021, 8, e1014. [Google Scholar] [CrossRef]
- Williams, T.J.; Benavides, D.R.; Patrice, K.-A.; Dalmau, J.O.; de Ávila, A.L.R.; Le, D.T.; Lipson, E.J.; Probasco, J.C.; Mowry, E.M. Association of Autoimmune Encephalitis with Combined Immune Checkpoint Inhibitor Treatment for Metastatic Cancer. JAMA Neurol. 2016, 73, 928. [Google Scholar] [CrossRef] [PubMed]
- Zafar, Z.; Vogler, C.; Hudali, T.; Bhattarai, M. Nivolumab-Associated Acute Demyelinating Encephalitis: A Case Report and Literature Review. Clin. Med. Res. 2019, 17, 29–33. [Google Scholar] [CrossRef]
- Jeffery, O.J.; Lennon, V.A.; Pittock, S.J.; Gregory, J.K.; Britton, J.W.; McKeon, A. GABAB Receptor Autoantibody Frequency in Service Serologic Evaluation. Neurology 2013, 81, 882–887. [Google Scholar] [CrossRef] [PubMed]
- Joubert, B.; Kerschen, P.; Zekeridou, A.; Desestret, V.; Rogemond, V.; Chaffois, M.-O.; Ducray, F.; Larrue, V.; Daubail, B.; Idbaih, A.; et al. Clinical Spectrum of Encephalitis Associated With Antibodies Against the α-Amino-3-Hydroxy-5-Methyl-4-Isoxazolepropionic Acid Receptor: Case Series and Review of the Literature. JAMA Neurol. 2015, 72, 1163–1169. [Google Scholar] [CrossRef] [PubMed]
- Graus, F.; Dalmau, J. Paraneoplastic Neurological Syndromes in the Era of Immune-Checkpoint Inhibitors. Nat. Rev. Clin. Oncol. 2019, 16, 535–548. [Google Scholar] [CrossRef]
- Duong, S.L.; Prüss, H. Paraneoplastic Autoimmune Neurological Syndromes and the Role of Immune Checkpoint Inhibitors. Neurotherapeutics 2022, 19, 848–863. [Google Scholar] [CrossRef]
- Pohl, D.; Alper, G.; Haren, K.V.; Kornberg, A.J.; Lucchinetti, C.F.; Tenembaum, S.; Belman, A.L. Acute Disseminated Encephalomyelitis: Updates on an Inflammatory CNS Syndrome. Neurology 2016, 87, S38–S45. [Google Scholar] [CrossRef]
- Johnson, D.B.; Nebhan, C.A.; Moslehi, J.J.; Balko, J.M. Immune-Checkpoint Inhibitors: Long-Term Implications of Toxicity. Nat. Rev. Clin. Oncol. 2022, 19, 254–267. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.C.; Duffy, C.R.; Allison, J.P. Fundamental Mechanisms of Immune Checkpoint Blockade Therapy. Cancer Discov. 2018, 8, 1069–1086. [Google Scholar] [CrossRef] [PubMed]
- Haslam, A.; Prasad, V. Estimation of the Percentage of US Patients With Cancer Who Are Eligible for and Respond to Checkpoint Inhibitor Immunotherapy Drugs. JAMA Netw. Open 2019, 2, e192535. [Google Scholar] [CrossRef] [PubMed]
- Farooq, M.Z.; Aqeel, S.B.; Lingamaneni, P.; Pichardo, R.C.; Jawed, A.; Khalid, S.; Banskota, S.U.; Fu, P.; Mangla, A. Association of Immune Checkpoint Inhibitors With Neurologic Adverse Events: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2022, 5, e227722. [Google Scholar] [CrossRef] [PubMed]
- Perrinjaquet, C.; Desbaillets, N.; Hottinger, A.F. Neurotoxicity Associated with Cancer Immunotherapy: Immune Checkpoint Inhibitors and Chimeric Antigen Receptor T-Cell Therapy. Curr. Opin. Neurol. 2019, 32, 500–510. [Google Scholar] [CrossRef]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef]
- Cuzzubbo, S.; Javeri, F.; Tissier, M.; Roumi, A.; Barlog, C.; Doridam, J.; Lebbe, C.; Belin, C.; Ursu, R.; Carpentier, A.F. Neurological Adverse Events Associated with Immune Checkpoint Inhibitors: Review of the Literature. Eur. J. Cancer 2017, 73, 1–8. [Google Scholar] [CrossRef]
- Astaras, C.; de Micheli, R.; Moura, B.; Hundsberger, T.; Hottinger, A.F. Neurological Adverse Events Associated with Immune Checkpoint Inhibitors: Diagnosis and Management. Curr. Neurol. Neurosci. Rep. 2018, 18, 3. [Google Scholar] [CrossRef]
- Schneider, S.; Potthast, S.; Komminoth, P.; Schwegler, G.; Böhm, S. PD-1 Checkpoint Inhibitor Associated Autoimmune Encephalitis. Case Rep. Oncol. 2017, 10, 473–478. [Google Scholar] [CrossRef]
- Shah, K.P.; Song, H.; Ye, F.; Moslehi, J.J.; Balko, J.M.; Salem, J.-E.; Johnson, D.B. Demographic Factors Associated with Toxicity in Patients Treated with Anti–Programmed Cell Death-1 Therapy. Cancer Immunol. Res. 2020, 8, 851–855. [Google Scholar] [CrossRef]
- Shah, S.; Dunn-Pirio, A.; Luedke, M.; Morgenlander, J.; Skeen, M.; Eckstein, C. Nivolumab-Induced Autoimmune Encephalitis in Two Patients with Lung Adenocarcinoma. Case Rep. Neurol. Med. 2018, 2018, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Geis, C.; Planagumà, J.; Carreño, M.; Graus, F.; Dalmau, J. Autoimmune Seizures and Epilepsy. J. Clin. Investig. 2019, 129, 926–940. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Ramberger, M.; O’Connor, K.C.; Bashford-Rogers, R.J.M.; Irani, S.R. The B Cell Immunobiology That Underlies CNS Autoantibody-Mediated Diseases. Nat. Rev. Neurol. 2020, 16, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Dalmau, J.; Graus, F. Antibody-Mediated Encephalitis. N. Engl. J. Med. 2018, 378, 840–851. [Google Scholar] [CrossRef] [PubMed]
- Vogrig, A.; Fouret, M.; Joubert, B.; Picard, G.; Rogemond, V.; Pinto, A.-L.; Muñiz-Castrillo, S.; Roger, M.; Raimbourg, J.; Dayen, C.; et al. Increased Frequency of Anti-Ma2 Encephalitis Associated with Immune Checkpoint Inhibitors. Neurol.-Neuroimmunol. Neuroinflammation 2019, 6, e604. [Google Scholar] [CrossRef]
- Hottinger, A.F.; de Micheli, R.; Guido, V.; Karampera, A.; Hagmann, P.; Pasquier, R.D. Natalizumab May Control Immune Checkpoint Inhibitor–Induced Limbic Encephalitis. Neurol. Neuroimmunol. Neuroinflammation 2018, 5, e439. [Google Scholar] [CrossRef]
- Stuby, J.; Herren, T.; Naumburger, G.S.; Papet, C.; Rudiger, A. Immune Checkpoint Inhibitor Therapy-Associated Encephalitis: A Case Series and Review of the Literature. Swiss Med. Wkly. 2020, 150, w20377. [Google Scholar] [CrossRef]
- Farina, A.; Villagrán-García, M.; Fourier, A.; Pinto, A.-L.; Chorfa, F.; Timestit, N.; Alberto, T.; Aupy, J.; Benaiteau, M.; Birzu, C.; et al. Diagnostic and Prognostic Biomarkers in Immune Checkpoint Inhibitor-Related Encephalitis: A Retrospective Cohort Study. Lancet Reg. Health-Eur. 2024, 44, 101011. [Google Scholar] [CrossRef]
- Ashique, S.; Mohanto, S.; Ahmed, M.G.; Mishra, N.; Garg, A.; Chellappan, D.K.; Omara, T.; Iqbal, S.; Kahwa, I. Gut-Brain Axis: A Cutting-Edge Approach to Target Neurological Disorders and Potential Synbiotic Application. Heliyon 2024, 10, e34092. [Google Scholar] [CrossRef]
- Khawar, M.M.; Ijaz, S.; Goyal, P.; Kandambige, D.; Sharifa, M.; Maslamani, A.N.J.; Kutabi, S.A.; Saleh, I.; Albshir, M.M.; Almadhoun, M.K.I.K.; et al. The Gut-Brain Axis in Autoimmune Diseases: Emerging Insights and Therapeutic Implications. Cureus 2023, 15, e48655. [Google Scholar] [CrossRef]
- Andrews, M.C.; Vasanthakumar, A. Gut Microbiota—A Double-Edged Sword in Cancer Immunotherapy. Trends Cancer 2023, 9, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Solomon, T.; Michael, B.D.; Smith, P.E.; Sanderson, F.; Davies, N.W.S.; Hart, I.J.; Holland, M.; Easton, A.; Buckley, C.; Kneen, R.; et al. Management of Suspected Viral Encephalitis in Adults–Association of British Neurologists and British Infection Association National Guidelines. J. Infect. 2012, 64, 347–373. [Google Scholar] [CrossRef] [PubMed]
- Farina, A.; Villagrán-García, M.; Joubert, B. Soluble Biomarkers for Immune Checkpoint Inhibitor-Related Encephalitis: A Mini-Review. Rev. Neurol. 2024; in press. [Google Scholar] [CrossRef]
- Larkin, J.; Chmielowski, B.; Lao, C.D.; Hodi, F.S.; Sharfman, W.; Weber, J.; Suijkerbuijk, K.P.M.; Azevedo, S.; Li, H.; Reshef, D.; et al. Neurologic Serious Adverse Events Associated with Nivolumab Plus Ipilimumab or Nivolumab Alone in Advanced Melanoma, Including a Case Series of Encephalitis. Oncologist 2017, 22, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.A.; Schneider, B.J.; Brahmer, J.; Achufusi, A.; Armand, P.; Berkenstock, M.K.; Bhatia, S.; Budde, L.E.; Chokshi, S.; Davies, M.; et al. Management of Immunotherapy-Related Toxicities, Version 1.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 387–405. [Google Scholar] [CrossRef] [PubMed]
- Gresa-Arribas, N.; Titulaer, M.J.; Torrents, A.; Aguilar, E.; McCracken, L.; Leypoldt, F.; Gleichman, A.J.; Balice-Gordon, R.; Rosenfeld, M.R.; Lynch, D.; et al. Antibody Titres at Diagnosis and during Follow-up of Anti-NMDA Receptor Encephalitis: A Retrospective Study. Lancet Neurol. 2014, 13, 167–177. [Google Scholar] [CrossRef]
- Haanen, J.B.A.G.; Carbonnel, F.; Robert, C.; Kerr, K.M.; Peters, S.; Larkin, J.; Jordan, K. Management of Toxicities from Immunotherapy: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2017, 28, iv119–iv142. [Google Scholar] [CrossRef]
- Charrot, S.; Hallam, S. CAR-T Cells: Future Perspectives. Hemasphere 2019, 3, e188. [Google Scholar] [CrossRef]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; Lin, Y.; et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N. Engl. J. Med. 2017, 377, 2531–2544. [Google Scholar] [CrossRef]
- Schuster, S.J.; Bishop, M.R.; Tam, C.S.; Waller, E.K.; Borchmann, P.; McGuirk, J.P.; Jäger, U.; Jaglowski, S.; Andreadis, C.; Westin, J.R.; et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2019, 380, 45–56. [Google Scholar] [CrossRef]
- Shah, B.D.; Ghobadi, A.; Oluwole, O.O.; Logan, A.C.; Boissel, N.; Cassaday, R.D.; Leguay, T.; Bishop, M.R.; Topp, M.S.; Tzachanis, D.; et al. KTE-X19 for Relapsed or Refractory Adult B-Cell Acute Lymphoblastic Leukaemia: Phase 2 Results of the Single-Arm, Open-Label, Multicentre ZUMA-3 Study. Lancet 2021, 398, 491–502. [Google Scholar] [CrossRef]
- Abramson, J.S.; Palomba, M.L.; Gordon, L.I.; Lunning, M.A.; Wang, M.; Arnason, J.; Mehta, A.; Purev, E.; Maloney, D.G.; Andreadis, C.; et al. Lisocabtagene Maraleucel for Patients with Relapsed or Refractory Large B-Cell Lymphomas (TRANSCEND NHL 001): A Multicentre Seamless Design Study. Lancet 2020, 396, 839–852. [Google Scholar] [CrossRef]
- Munshi, N.C.; Anderson, L.D., Jr.; Shah, N.; Madduri, D.; Berdeja, J.; Lonial, S.; Raje, N.; Lin, Y.; Siegel, D.; Oriol, A.; et al. Idecabtagene Vicleucel in Relapsed and Refractory Multiple Myeloma. N. Engl. J. Med. 2021, 384, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Berdeja, J.G.; Madduri, D.; Usmani, S.Z.; Jakubowiak, A.; Agha, M.; Cohen, A.D.; Stewart, A.K.; Hari, P.; Htut, M.; Lesokhin, A.; et al. Ciltacabtagene Autoleucel, a B-Cell Maturation Antigen-Directed Chimeric Antigen Receptor T-Cell Therapy in Patients with Relapsed or Refractory Multiple Myeloma (CARTITUDE-1): A Phase 1b/2 Open-Label Study. Lancet 2021, 398, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Topp, M.S.; Gökbuget, N.; Stein, A.S.; Zugmaier, G.; O’Brien, S.; Bargou, R.C.; Dombret, H.; Fielding, A.K.; Heffner, L.; Larson, R.A.; et al. Safety and Activity of Blinatumomab for Adult Patients with Relapsed or Refractory B-Precursor Acute Lymphoblastic Leukaemia: A Multicentre, Single-Arm, Phase 2 Study. Lancet Oncol. 2015, 16, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Weber, J.S.; Yang, J.C.; Atkins, M.B.; Disis, M.L. Toxicities of Immunotherapy for the Practitioner. J. Clin. Oncol. 2015, 33, 2092–2099. [Google Scholar] [CrossRef] [PubMed]
- Neelapu, S.S.; Tummala, S.; Kebriaei, P.; Wierda, W.; Gutierrez, C.; Locke, F.L.; Komanduri, K.V.; Lin, Y.; Jain, N.; Daver, N.; et al. Chimeric Antigen Receptor T-Cell Therapy - Assessment and Management of Toxicities. Nat. Rev. Clin. Oncol. 2018, 15, 47–62. [Google Scholar] [CrossRef]
- Torre, M.; Solomon, I.H.; Sutherland, C.L.; Nikiforow, S.; DeAngelo, D.J.; Stone, R.M.; Vaitkevicius, H.; Galinsky, I.A.; Padera, R.F.; Trede, N.; et al. Neuropathology of a Case With Fatal CAR T-Cell-Associated Cerebral Edema. J. Neuropathol. Exp. Neurol. 2018, 77, 877–882. [Google Scholar] [CrossRef]
- Gust, J.; Hay, K.A.; Hanafi, L.-A.; Li, D.; Myerson, D.; Gonzalez-Cuyar, L.F.; Yeung, C.; Liles, W.C.; Wurfel, M.; Lopez, J.A.; et al. Endothelial Activation and Blood–Brain Barrier Disruption in Neurotoxicity after Adoptive Immunotherapy with CD19 CAR-T Cells. Cancer Discov. 2017, 7, 1404–1419. [Google Scholar] [CrossRef]
- Santomasso, B.D.; Park, J.H.; Salloum, D.; Riviere, I.; Flynn, J.; Mead, E.; Halton, E.; Wang, X.; Senechal, B.; Purdon, T.; et al. Clinical and Biological Correlates of Neurotoxicity Associated with CAR T-Cell Therapy in Patients with B-Cell Acute Lymphoblastic Leukemia. Cancer Discov. 2018, 8, 958–971. [Google Scholar] [CrossRef]
- Zhou, X.; Rasche, L.; Kortüm, K.M.; Danhof, S.; Hudecek, M.; Einsele, H. Toxicities of Chimeric Antigen Receptor T Cell Therapy in Multiple Myeloma: An Overview of Experience From Clinical Trials, Pathophysiology, and Management Strategies. Front. Immunol. 2020, 11, 620312. [Google Scholar] [CrossRef]
- Schubert, M.-L.; Schmitt, M.; Wang, L.; Ramos, C.A.; Jordan, K.; Müller-Tidow, C.; Dreger, P. Side-Effect Management of Chimeric Antigen Receptor (CAR) T-Cell Therapy. Ann. Oncol. 2021, 32, 34–48. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Huang, S.; Chen, S.; Wang, Y.; Sun, Q.; Xu, X.; Li, Y. Mechanisms of Cytokine Release Syndrome and Neurotoxicity of CAR T-Cell Therapy and Associated Prevention and Management Strategies. J. Exp. Clin. Cancer Res. 2021, 40, 367. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Santomasso, B.D.; Locke, F.L.; Ghobadi, A.; Turtle, C.J.; Brudno, J.N.; Maus, M.V.; Park, J.H.; Mead, E.; Pavletic, S.; et al. ASTCT Consensus Grading for Cytokine Release Syndrome and Neurologic Toxicity Associated with Immune Effector Cells. Biol. Blood Marrow Transplant. 2019, 25, 625–638. [Google Scholar] [CrossRef] [PubMed]
- Neelapu, S.S.; Tummala, S.; Kebriaei, P.; Wierda, W.; Locke, F.L.; Lin, Y.; Jain, N.; Daver, N.; Gulbis, A.M.; Adkins, S.; et al. Toxicity Management after Chimeric Antigen Receptor T Cell Therapy: One Size Does Not Fit “ALL”. Nat. Rev. Clin. Oncol. 2018, 15, 218. [Google Scholar] [CrossRef] [PubMed]
- Norelli, M.; Camisa, B.; Barbiera, G.; Falcone, L.; Purevdorj, A.; Genua, M.; Sanvito, F.; Ponzoni, M.; Doglioni, C.; Cristofori, P.; et al. Monocyte-Derived IL-1 and IL-6 Are Differentially Required for Cytokine-Release Syndrome and Neurotoxicity Due to CAR T Cells. Nat. Med. 2018, 24, 739–748. [Google Scholar] [CrossRef]
- Nellan, A.; McCully, C.M.L.; Garcia, R.C.; Jayaprakash, N.; Widemann, B.C.; Lee, D.W.; Warren, K.E. Improved CNS Exposure to Tocilizumab after Cerebrospinal Fluid Compared to Intravenous Administration in Rhesus Macaques. Blood 2018, 132, 662–666. [Google Scholar] [CrossRef]
- Mackall, C.L.; Miklos, D.B. CNS Endothelial Cell Activation Emerges as a Driver of CAR T Cell–Associated Neurotoxicity. Cancer Discov. 2017, 7, 1371–1373. [Google Scholar] [CrossRef]
- Hagop, K.; Anthony, S.; Nicola, G.; Fielding, A.K.; Schuh, A.C.; Josep-Maria, R.; Andrew, W.; Hervé, D.; Robin, F.; Renato, B.; et al. Blinatumomab versus Chemotherapy for Advanced Acute Lymphoblastic Leukemia. N. Engl. J. Med. 2017, 376, 836–847. [Google Scholar] [CrossRef]
- Nathan, P.; Hassel, J.C.; Rutkowski, P.; Baurain, J.-F.; Butler, M.O.; Schlaak, M.; Sullivan, R.J.; Ochsenreither, S.; Dummer, R.; Kirkwood, J.M.; et al. Overall Survival Benefit with Tebentafusp in Metastatic Uveal Melanoma. N. Engl. J. Med. 2021, 385, 1196–1206. [Google Scholar] [CrossRef]
- Hutchings, M.; Morschhauser, F.; Iacoboni, G.; Carlo-Stella, C.; Offner, F.C.; Sureda, A.; Salles, G.; Martínez-Lopez, J.; Crump, M.; Thomas, D.N.; et al. Glofitamab, a Novel, Bivalent CD20-Targeting T-Cell–Engaging Bispecific Antibody, Induces Durable Complete Remissions in Relapsed or Refractory B-Cell Lymphoma: A Phase I Trial. J. Clin. Oncol. 2021, 39, 1959–1970. [Google Scholar] [CrossRef]
- Budde, L.E.; Sehn, L.H.; Matasar, M.; Schuster, S.J.; Assouline, S.; Giri, P.; Kuruvilla, J.; Canales, M.; Dietrich, S.; Fay, K.; et al. Safety and Efficacy of Mosunetuzumab, a Bispecific Antibody, in Patients with Relapsed or Refractory Follicular Lymphoma: A Single-Arm, Multicentre, Phase 2 Study. Lancet Oncol. 2022, 23, 1055–1065. [Google Scholar] [CrossRef] [PubMed]
- Chari, A.; Minnema, M.C.; Berdeja, J.G.; Oriol, A.; van de Donk, N.W.C.J.; Rodríguez-Otero, P.; Askari, E.; Mateos, M.-V.; Costa, L.J.; Caers, J.; et al. Talquetamab, a T-Cell–Redirecting GPRC5D Bispecific Antibody for Multiple Myeloma. N. Engl. J. Med. 2022, 387, 2232–2244. [Google Scholar] [CrossRef] [PubMed]
- Shanshal, M.; Caimi, P.F.; Adjei, A.A.; Ma, W.W. T-Cell Engagers in Solid Cancers—Current Landscape and Future Directions. Cancers 2023, 15, 2824. [Google Scholar] [CrossRef] [PubMed]
- Goebeler, M.-E.; Bargou, R. Blinatumomab: A CD19/CD3 Bispecific T Cell Engager (BiTE) with Unique Anti-Tumor Efficacy. Leuk. Lymphoma 2016, 57, 1021–1032. [Google Scholar] [CrossRef] [PubMed]
- Stein, A.S.; Schiller, G.; Benjamin, R.; Jia, C.; Zhang, A.; Zhu, M.; Zimmerman, Z.; Topp, M.S. Neurologic Adverse Events in Patients with Relapsed/Refractory Acute Lymphoblastic Leukemia Treated with Blinatumomab: Management and Mitigating Factors. Ann. Hematol. 2018, 98, 159–167. [Google Scholar] [CrossRef]
- Schlegel, U. Central Nervous System Toxicity of Chemotherapy. Eur. Assoc. Neurooncology Mag. 2011, 1, 25–29. [Google Scholar]
- Peddi, P.F.; Peddi, S.; Santos, E.S.; Morgensztern, D. Central Nervous System Toxicities of Chemotherapeutic Agents. Expert. Rev. Anticancer 2014, 14, 857–863. [Google Scholar] [CrossRef]
- Ziske, C.G.; Schöttker, B.; Gorschlüter, M.; Mey, U.; Kleinschmidt, R.; Schlegel, U.; Sauerbruch, T.; Schmidt-Wolf, I.G.H. Acute Transient Encephalopathy after Paclitaxel Infusion: Report of Three Cases. Ann. Oncol. 2002, 13, 629–631. [Google Scholar] [CrossRef]
- Verstappen, C.C.P.; Heimans, J.J.; Hoekman, K.; Postma, T.J. Neurotoxic Complications of Chemotherapy in Patients with Cancer. Drugs 2003, 63, 1549–1563. [Google Scholar] [CrossRef]
- Widemann, B.C.; Balis, F.M.; Shalabi, A.; Boron, M.; O’Brien, M.; Cole, D.E.; Jayaprakash, N.; Ivy, P.; Castle, V.; Muraszko, K.; et al. Treatment of Accidental Intrathecal Methotrexate Overdose With Intrathecal Carboxypeptidase G2. JNCI J. Natl. Cancer Inst. 2004, 96, 1557–1559. [Google Scholar] [CrossRef]
- Widemann, B.C.; Sung, E.; Anderson, L.; Salzer, W.L.; Balis, F.M.; Monitjo, K.S.; McCully, C.; Hawkins, M.; Adamson, P.C. Pharmacokinetics and Metabolism of the Methotrexate Metabolite 2, 4-Diamino-N(10)-Methylpteroic Acid. J. Pharmacol. Exp. Ther. 2000, 294, 894–901. [Google Scholar] [PubMed]
- Green, J.M. Glucarpidase to Combat Toxic Levels of Methotrexate in Patients. Ther. Clin. Risk Manag. 2012, 8, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Pelgrims, J.; Vos, F.D.; den Brande, J.V.; Schrijvers, D.; Prové, A.; Vermorken, J.B. Methylene Blue in the Treatment and Prevention of Ifosfamide-Induced Encephalopathy: Report of 12 Cases and a Review of the Literature. Br. J. Cancer 2000, 82, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Hamadani, M.; Awan, F. Role of Thiamine in Managing Ifosfamide-Induced Encephalopathy. J. Oncol. Pharm. Pr. 2006, 12, 237–239. [Google Scholar] [CrossRef] [PubMed]
- Eichler, A.F.; Batchelor, T.T.; Henson, J.W. Diffusion and Perfusion Imaging in Subacute Neurotoxicity Following High-Dose Intravenous Methotrexate. Neuro-Oncol. 2007, 9, 373–377. [Google Scholar] [CrossRef]
- Yamada, N.; Yamasaki, K.; Yamamoto, N.; Kuki, I.; Sakuma, H.; Hara, J. Chemotherapy-Induced Autoimmune-Mediated Encephalitis during Germinoma Treatment. Brain Dev. 2021, 43, 967–971. [Google Scholar] [CrossRef]
- Jung, N.-Y.; Woo, K.-N.; Cho, J.W.; Kim, H.-W. Anti-Yo-Associated Autoimmune Encephalitis after Colon Cancer Treatment. J. Neurocritical Care 2020, 13, 104–107. [Google Scholar] [CrossRef]
- Broecker, F.; Shanin, E.; Lysov, N.; Shanin, V. Chemotherapy-Induced, Broadly Reactive Autoantibodies in a Colon Cancer Patient. Cureus 2022, 14, e31954. [Google Scholar] [CrossRef]
- Janjua, T.K.; Hassan, M.; Afridi, H.K.; Zahid, N.A. Oxaliplatin-Induced Posterior Reversible Encephalopathy Syndrome (PRES). BMJ Case Rep. 2017, 2017, bcr-2017-221571. [Google Scholar] [CrossRef]
- Floeter, A.E.; Patel, A.; Tran, M.; Chamberlain, M.C.; Hendrie, P.C.; Gopal, A.K.; Cassaday, R.D. Posterior Reversible Encephalopathy Syndrome Associated With Dose-Adjusted EPOCH (Etoposide, Prednisone, Vincristine, Cyclophosphamide, Doxorubicin) Chemotherapy. Clin. Lymphoma Myeloma Leuk. 2016, 17, 225–230. [Google Scholar] [CrossRef]
- Kabre, R.S.; Kamble, K.M. Gemcitabine and Cisplatin Induced Posterior Reversible Encephalopathy Syndrome: A Case Report with Review of Literature. J. Res. Pharm. Pr. 2016, 5, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Martín, G.; Bellido, L.; Cruz, J.J. Reversible Posterior Leukoencephalopathy Syndrome Induced by Sunitinib. J. Clin. Oncol. 2007, 25, 3559. [Google Scholar] [CrossRef] [PubMed]
- Govindarajan, R.; Adusumilli, J.; Baxter, D.L.; El-Khoueiry, A.; Harik, S.I. Reversible Posterior Leukoencephalopathy Syndrome Induced by RAF Kinase Inhibitor BAY 43-9006. J. Clin. Oncol. 2006, 24, e48. [Google Scholar] [CrossRef] [PubMed]
- Glusker, P.; Recht, L.; Lane, B. Reversible Posterior Leukoencephalopathy Syndrome and Bevacizumab. N. Engl. J. Med. 2006, 354, 980–982. [Google Scholar] [CrossRef]
- Hamid, M.; Ghani, A.; Micaily, I.; Sarwar, U.; Lashari, B.; Malik, F. Posterior Reversible Encephalopathy Syndrome (PRES) after Bevacizumab Therapy for Metastatic Colorectal Cancer. J. Community Hosp. Intern. Med. Perspect. 2018, 8, 130–133. [Google Scholar] [CrossRef]
- Mavragani, C.P.; Vlachoyiannopoulos, P.G.; Kosmas, N.; Boletis, I.; Tzioufas, A.G.; Voulgarelis, M. A Case of Reversible Posterior Leucoencephalopathy Syndrome after Rituximab Infusion. Rheumatology 2004, 43, 1450–1451. [Google Scholar] [CrossRef]
- Ricard, D.; Durand, T.; Tauziède-Espariat, A.; Leclercq, D.; Psimaras, D. Cancer Neurology in Clinical Practice, Neurological Complications of Cancer and Its Treatment; Springer: Cham, Switzerland, 2017; pp. 241–273. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).