
Prevalence and Distribution of MUTYH Pathogenic Variants, Is There a Relation with an Increased Risk of Breast Cancer?

 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of MUTYHmut Carriers
3.2. Genetic Findings of MUTYHmut Carriers
3.3. Breast Cancer in MUTYHmut Carriers
3.4. Prevalence of MUTYH Mutations and Association with Pathologies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F.; Bsc, M.F.B.; Me, J.F.; Soerjomataram, M.I.; et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Valle, L.; Vilar, E.; Tavtigian, S.V.; Stoffel, E.M. Genetic predisposition to colorectal cancer: Syndromes, genes, classification of genetic variants and implications for precision medicine. J. Pathol. 2018, 247, 574–588. [Google Scholar] [CrossRef]
- Al-Tassan, N.; Chmiel, N.H.; Maynard, J.; Fleming, N.; Livingston, A.L.; Williams, G.T.; Hodges, A.K.; Davies, D.R.; David, S.S.; Sampson, J.R.; et al. Inherited variants of MYH associated with somatic G:C→T:A mutations in colorectal tumors. Nat. Genet. 2002, 30, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; Emmerson, P.; Maynard, J.; Best, J.M.; Jordan, S.; Williams, G.T.; Sampson, J.R.; Cheadle, J.P. Biallelic germline mutations in MYH predispose to multiple colorectal adenoma and somatic G:C→T:A mutations. Hum. Mol. Genet. 2002, 11, 2961–2967. [Google Scholar] [CrossRef]
- Slupska, M.M.; Baikalov, C.; Luther, W.M.; Chiang, J.H.; Wei, Y.F.; Miller, J.H. Cloning and sequencing a human homolog (hMYH) of the Escherichia coli mutY gene whose function is required for the repair of oxidative DNA damage. J. Bacteriol. 1996, 178, 3885–3892. [Google Scholar] [CrossRef] [PubMed]
- Cheadle, J.P.; Sampson, J.R. Exposing the MYtH about base excision repair and human inherited disease. Hum. Mol. Genet. 2003, 12, R159–R165. [Google Scholar] [CrossRef]
- Russell, A.M.; Zhang, J.; Luz, J.; Hutter, P.; Chappuis, P.O.; Berthod, C.R.; Maillet, P.; Mueller, H.; Heinimann, K. Prevalence of MYH germline mutations in Swiss APC mutation-negative polyposis patients. Int. J. Cancer 2006, 118, 1937–1940. [Google Scholar] [CrossRef]
- VCV000005294.91-ClinVar-NCBI [Internet]. Available online: https://www.ncbi.nlm.nih.gov/clinvar/variation/5294/ (accessed on 22 May 2023).
- VCV000005293.82-ClinVar-NCBI [Internet]. Available online: https://www.ncbi.nlm.nih.gov/clinvar/variation/5293/ (accessed on 22 May 2023).
- Vogt, S.; Jones, N.; Christian, D.; Engel, C.; Nielsen, M.; Kaufmann, A.; Steinke, V.; Vasen, H.F.; Propping, P.; Sampson, J.R.; et al. Expanded Extracolonic Tumor Spectrum in MUTYH-Associated Polyposis. Gastroenterology 2009, 137, 1976–1985.e10. [Google Scholar] [CrossRef]
- Yoshida, R. Hereditary breast and ovarian cancer (HBOC): Review of its molecular characteristics, screening, treatment, and prognosis. Breast Cancer 2020, 28, 1167–1180. [Google Scholar] [CrossRef]
- Nielsen, M.; Franken, P.F.; Reinards, T.H.C.M.; Weiss, M.M.; Wagner, A.; van der Klift, H.; Kloosterman, S.; Houwing-Duistermaat, J.J.; Aalfs, C.M.; Ausems, M.G.E.M.; et al. Multiplicity in polyp count and extracolonic manifestations in 40 Dutch patients with MYH associated polyposis coli (MAP). J. Med. Genet. 2005, 42, e54. [Google Scholar] [CrossRef]
- Maxwell, K.N.; Wubbenhorst, B.; D’Andrea, K.; Garman, B.; Long, J.M.; Powers, J.; Rathbun, K.; Stopfer, J.E.; Zhu, J.; Bradbury, A.R.; et al. Prevalence of mutations in a panel of breast cancer susceptibility genes in BRCA1/2 negative patients with early onset breast cancer. Genet. Med. 2015, 17, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Le Page, F.; Randrianarison, V.; Marot, D.; Cabannes, J.; Perricaudet, M.; Feunteun, J.; Sarasin, A. BRCA1 and BRCA2 are necessary for the transcription-coupled repair of the oxidative 8-oxoguanine lesion in human cells. Cancer Res. 2000, 60, 5548–5552. [Google Scholar] [PubMed]
- Fulk, K.; LaDuca, H.; Black, M.H.; Qian, D.; Tian, Y.; Yussuf, A.; Espenschied, C.; Jasperson, K. Monoallelic MUTYH carrier status is not associated with increased breast cancer risk in a multigene panel cohort. Fam. Cancer 2019, 18, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Balaguer, F.; Leoz, M.; Carballal, S.; Moreira, L.; Ocaña, T. The genetic basis of familial adenomatous polyposis and its implications for clinical practice and risk management. Appl. Clin. Genet. 2015, 8, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Kurian, A.W.; Hare, E.E.; Mills, M.A.; Kingham, K.E.; McPherson, L.; Whittemore, A.S.; McGuire, V.; Ladabaum, U.; Kobayashi, Y.; Lincoln, S.E.; et al. Clinical Evaluation of a Multiple-Gene Sequencing Panel for Hereditary Cancer Risk Assessment. J. Clin. Oncol. 2014, 32, 2001–2009. [Google Scholar] [CrossRef] [PubMed]
- Ellingson, M.S.; Hart, S.N.; Kalari, K.R.; Suman, V.; Schahl, K.A.; Dockter, T.J.; Felten, S.J.; Sinnwell, J.P.; Thompson, K.J.; Tang, X.; et al. Exome sequencing reveals frequent deleterious germline variants in cancer susceptibility genes in women with invasive breast cancer undergoing neoadjuvant chemotherapy. Breast Cancer Res. Treat. 2015, 153, 435–443. [Google Scholar] [CrossRef]
- Lin, P.-H.; Kuo, W.-H.; Huang, A.-C.; Lu, Y.-S.; Lin, C.-H.; Kuo, S.-H.; Wang, M.-Y.; Liu, C.-Y.; Cheng, F.T.-F.; Yeh, M.-H.; et al. Multiple gene sequencing for risk assessment in patients with early-onset or familial breast cancer. Oncotarget 2016, 7, 8310–8320. [Google Scholar] [CrossRef] [PubMed]
- Rummel, S.K.; Lovejoy, L.; Shriver, C.D.; Ellsworth, R.E. Contribution of germline mutations in cancer predisposition genes to tumor etiology in young women diagnosed with invasive breast cancer. Breast Cancer Res. Treat. 2017, 164, 593–601. [Google Scholar] [CrossRef]
- Kaur, R.P.; Shafi, G.; Benipal, R.P.S.; Munshi, A. Frequency of pathogenic germline mutations in cancer susceptibility genes in breast cancer patients. Med. Oncol. 2018, 35, 1–9. [Google Scholar] [CrossRef]
- Meiss, A.E.; Thomas, M.; Modesitt, S.C.; Ring, K.L.; Atkins, K.A.; Mills, A.M. Clinicopathologic characterization of breast carcinomas in patients with non-BRCA germline mutations: Results from a single institution’s high-risk population. Hum. Pathol. 2018, 82, 20–31. [Google Scholar] [CrossRef]
- Oliver, J.; Quezada Urban, R.; Franco Cortés, C.A.; Díaz Velásquez, C.E.; Montealegre Paez, A.L.; Pacheco-Orozco, R.A.; Rojas, C.C.; Garcia-Robles, R.; Rivera, J.J.L.; Chaparro, S.G.; et al. Latin American Study of Hereditary Breast and Ovarian Cancer LACAM: A Genomic Epidemiology Approach. Front Oncol. 2019, 9, 1429. [Google Scholar] [CrossRef] [PubMed]
- Rizzolo, P.; Silvestri, V.; Bucalo, A.; Zelli, V.; Valentini, V.; Catucci, I.; Zanna, I.; Masala, G.; Bianchi, S.; Spinelli, A.M.; et al. Contribution of MUTYH Variants to Male Breast Cancer Risk: Results From a Multicenter Study in Italy. Front. Oncol. 2018, 8, 583. [Google Scholar] [CrossRef] [PubMed]
- Schneider, B.P.; Stout, L.A.; Philips, S.; Schroeder, C.; Scott, S.F.; Hunter, C.; Kassem, N.; Kiel, P.J.; Radovich, M. Implications of Incidental Germline Findings Identified In the Context of Clinical Whole Exome Sequencing for Guiding Cancer Therapy. JCO Precis. Oncol. 2020, 4, 1109–1121. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.; Lee, H.; Cho, E.H.; Yoon, K.; Kim, M.; Joo, J.; Lee, E.; Kang, H.; Lee, S.; Lee, D.O.; et al. Exon splicing analysis of intronic variants in multigene cancer panel testing for hereditary breast/ovarian cancer. Cancer Sci. 2020, 111, 3912–3925. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Zhang, G.; Li, X.; Ren, C.; Wang, Y.; Li, K.; Mok, H.; Cao, L.; Wen, L.; Jia, M.; et al. Comparison of BRCA versus non-BRCA germline mutations and associated somatic mutation profiles in patients with unselected breast cancer. Aging 2020, 12, 3140–3155. [Google Scholar] [CrossRef] [PubMed]
- Kurian, A.W.; Hughes, E.; Handorf, E.A.; Gutin, A.; Allen, B.; Hartman, A.-R.; Hall, M.J. Breast and Ovarian Cancer Penetrance Estimates Derived From Germline Multiple-Gene Sequencing Results in Women. JCO Precis. Oncol. 2017, 1, 1–12. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, J.M.; Zurro, N.B.; Coelho, A.V.C.; Caraciolo, M.P.; de Alexandre, R.B.; Cervato, M.C.; Minillo, R.M.; Neto, G.D.V.C.; Grivicich, I.; Oliveira, J.B. The genetics of hereditary cancer risk syndromes in Brazil: A comprehensive analysis of 1682 patients. Eur. J. Hum. Genet. 2022, 30, 818–823. [Google Scholar] [CrossRef]
- Tatineni, S.; Tarockoff, M.; Abdallah, N.; Purrington, K.S.; Assad, H.; Reagle, R.; Petrucelli, N.; Simon, M.S. Racial and ethnic variation in multigene panel testing in a cohort of BRCA1/2-negative individuals who had genetic testing in a large urban comprehensive cancer center. Cancer Med. 2022, 11, 1465–1473. [Google Scholar] [CrossRef]
- Rennert, G.; Lejbkowicz, F.; Cohen, I.; Pinchev, M.; Rennert, H.S.; Barnett-Griness, O. MutYH mutation carriers have increased breast cancer risk. Cancer 2012, 118, 1989–1993. [Google Scholar] [CrossRef]
- Beiner, M.E.; Zhang, W.W.; Zhang, S.; Gallinger, S.; Sun, P.; Narod, S.A. Mutations of the MYH gene do not substantially contribute to the risk of breast cancer. Breast Cancer Res. Treat. 2009, 114, 575–578. [Google Scholar] [CrossRef]
- Win, A.K.; Cleary, S.P.; Dowty, J.G.; Baron, J.A.; Young, J.P.; Buchanan, D.D.; Southey, M.C.; Burnett, T.; Parfrey, P.S.; Green, R.C.; et al. Cancer risks for monoallelic MUTYH mutation carriers with a family history of colorectal cancer. Int. J. Cancer 2011, 129, 2256–2262. [Google Scholar] [CrossRef]
- Out, A.A.; Wasielewski, M.; Huijts, P.E.A.; van Minderhout, I.J.H.M.; Houwing-Duistermaat, J.J.; Tops, C.M.J.; Nielsen, M.; Seynaeve, C.; Wijnen, J.T.; Breuning, M.H.; et al. MUTYH gene variants and breast cancer in a Dutch case–control study. Breast Cancer Res. Treat. 2012, 134, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Win, A.K.; Reece, J.C.; Dowty, J.G.; Buchanan, D.D.; Clendenning, M.; Rosty, C.; Southey, M.C.; Young, J.P.; Cleary, S.P.; Kim, H.; et al. Risk of extracolonic cancers for people with biallelic and monoallelic mutations in MUTYH. Int. J. Cancer 2016, 139, 1557–1563. [Google Scholar] [CrossRef] [PubMed]
- Jian, W.; Shao, K.; Qin, Q.; Wang, X.; Song, S.; Wang, X. Clinical and genetic characterization of hereditary breast cancer in a Chinese population. Hered. Cancer Clin. Pract. 2017, 15, 19. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.B.; Sutcliffe, E.G.; Arvai, K.; Roberts, M.E.; Susswein, L.R.; Marshall, M.L.; Torene, R.; Postula, K.J.V.; Hruska, K.S.; Bai, S. Monoallelic MUTYH pathogenic variants ascertained via multi-gene hereditary cancer panels are not associated with colorectal, endometrial, or breast cancer. Fam. Cancer 2022, 21, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Guindalini, R.S.C.; Viana, D.V.; Kitajima, J.P.F.W.; Rocha, V.M.; López, R.V.M.; Zheng, Y.; Freitas, É.; Monteiro, F.P.M.; Valim, A.; Schlesinger, D.; et al. Detection of germline variants in Brazilian breast cancer patients using multigene panel testing. Sci. Rep. 2022, 12, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Win, A.K.; Dowty, J.G.; Cleary, S.P.; Kim, H.; Buchanan, D.D.; Young, J.P.; Clendenning, M.; Rosty, C.; MacInnis, R.J.; Giles, G.G.; et al. Risk of Colorectal Cancer for Carriers of Mutations in MUTYH, With and Without a Family History of Cancer. Gastroenterology 2014, 146, 1208–1211.e5. [Google Scholar] [CrossRef]
- Lubbe, S.J.; Di Bernardo, M.C.; Chandler, I.P.; Houlston, R.S. Clinical Implications of the Colorectal Cancer Risk Associated With MUTYH Mutation. J. Clin. Oncol. 2009, 27, 3975–3980. [Google Scholar] [CrossRef]
- Croitoru, M.E.; Cleary, S.P.; Di Nicola, N.; Manno, M.; Selander, T.; Aronson, M.; Redston, M.; Cotterchio, M.; Knight, J.; Gryfe, R.; et al. Association Between Biallelic and Monoallelic Germline MYH Gene Mutations and Colorectal Cancer Risk. JNCI J. Natl. Cancer Inst. 2004, 96, 1631–1634. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | N = 56 |
|---|---|
| Age (years)—Median (range) | 60 (18–85) |
| Sex—n (%) -Male -Female | 12 (21.4%) 44 (78.6%) |
| Index case—n (%) -Yes -No | 36 (64.3%) 20 (35.7%) |
| Suspected hereditary syndrome—n (%) -HBOCS -Familial polyposis -HNPCC-Hereditary leukemia -Hereditary renal cancer | 27 (48.2%) 18 (32.1%) 7 (12.5%) 3 (5.4%) 1 (1.8%) |
| Pathology—n (%) -Non cancer/polyposis -Colonic polyposis -Breast cancer -Colorectal cancer -Ovarian cancer -Pancreatic cancer -Renal cancer -Prostate cancer -Hematological cancer -Melanoma -Endometrial cancer -Lung cancer | 15 (26.8%) 17 (30.4%) 14 (25%) 7 (12.5%) 5 (8.9%) 3 (5.4%) 3 (5.4%) 2 (3.6%) 2 (3.6%) 2 (3.6%) 1 (1.8%) 1 (1.8%) |
| Characteristics | N = 56 |
|---|---|
| MUTYH allele status—n (%) -Homozygous -Compound heterozygous -Heterozygous | 2 (3.6%) 4 (7.1%) 50 (89.2%) |
| MUTYH mutations—n (%) -p.G382D/Class 5 -p.Y179C/Class 5 -p.E410Gfs*43/Class 5 -p.R368Qfs*164/Class 4 -p.Q338*/Class 5 -p.R97Q/Class 3 -p.R109W/Class 4 -p.E453del/Class 5 -p.D147H/Class 3-p.Q324=/Class 1 -p.R426C/Class 3 -c.933+3A>C/Class 3 -c.934-2A>G/Class 4 -c.997+1G>T/Class 4 | 62 (100%) 39 (62.9%) 6 (9.7%) 3 (4.8%) 3 (4.8%) 2 (3.2%) 1 (1.6%) 1 (1.6%) 1 (1.6%) 1 (1.6%) 1 (1.6%) 1 (1.6%) 1 (1.6%) 1 (1.6%) 1 (1.6%) |
| Other mutations—n -BRCA2 -RAD50 -APC -ATM -NF1 -SDHB | 2 (3.6%) 2 (3.6%) 2 (3.6%) 1 (1.8%) 1 (1.8%) 1 (1.8%) |
| Nº | Sex/ Age | Suspected Syndrome | Index Case | Polyposis | Tumor | MUTYH Mutation | Other Mutation |
|---|---|---|---|---|---|---|---|
| 1 | F35 | HBOCS | Y | N | BC + RC | p.G382D (5) heterozygosis | |
| 2 | F33 | HBOCS | Y | N | BC + OC | p.G382D (5) heterozygosis | |
| 3 | F33 | HBOCS | Y | N | BC | p.G382D (5) heterozygosis | |
| 4 | F35 | HBOCS | Y | N | BC | p.G382D (5) + p.R97Q (3) compound heterozygosis | |
| 5 | F38 | HBOCS | Y | N | BC | p.G382D (5) heterozygosis | |
| 6 | F70 | HBOCS | Y | N | BC | p.G382D (5) heterozygosis | |
| 7 | F62 | HBOCS | Y | N | BC + PCC | p.G382D (5) heterozygosis | |
| 8 | F39 | HBOCS | Y | N | BC | p.Y179C (5) heterozygosis | ATM c.720T>C (3) |
| 9 | F60 | HBOCS | Y | N | BC + RC | p.Y179C (5) heterozygosis | |
| 10 | F43 | HBOCS | Y | N | BC | p.Q338* (5) heterozygosis | |
| 11 | F60 | HBOCS | Y | N | BC | p.Q338* (5) heterozygosis | |
| 12 | F60 | HBOCS | Y | N | BC | c.934-2A>G (4) heterozygosis | |
| 13 | F76 | HBOCS | Y | N | BC + LC | c.933+3A>C (3) heterozygosis | |
| 14 | F78 | HNPCC | Y | N | BC + CRC + OC | p.E410Gfs*43 (5) heterozygosis | BRCA2 p.E170A (3) |
| 15 | F64 | FAP | N | N | - | p.G382D (5) homozygosis | |
| 16 | F35 | FAP | Y | Y | - | p.G382D (5) homozygosis | |
| 17 | F57 | FAP | Y | Y | - | p.G382D (5) heterozygosis | APC p.N1739fs (5) |
| 18 | F56 | FAP | Y | Y | - | p.G382D (5) heterozygosis | |
| 19 | F60 | FAP | Y | Y | - | p.G382D (5) heterozygosis | APC p.D1711V (3) |
| 20 | M37 | FAP | N | Y | - | p.G382D (5) heterozygosis | |
| 21 | F62 | FAP | N | Y | - | p.G382D (5) heterozygosis | |
| 22 | M29 | FAP | N | Y | - | p.G382D (5) heterozygosis | |
| 23 | F61 | FAP | Y | Y | - | p.G382D (5) + p.R109W (4) compound heterozygosis | |
| 24 | F67 | FAP | N | Y | - | p.G382D (5) heterozygosis | |
| 25 | M60 | FAP | N | Y | - | p.G382D (5) heterozygosis | |
| 26 | F53 | FAP | Y | Y | EC | p.G382D (5) + p.E453del (5) compound heterozygosis | |
| 27 | F76 | FAP | N | N | - | p.Y179C (5) heterozygosis | |
| 28 | M85 | FAP | Y | Y | CRC | p.Y179C (5) heterozygosis | |
| 29 | F51 | FAP | Y | Y | - | p.Q324= (1) heterozygosis | |
| 30 | M76 | FAP | Y | Y | - | p.D147H (3) heterozygosis | |
| 31 | M62 | FAP | N | Y | - | p.R426C (3) heterozygosis | |
| 32 | M77 | FAP | Y | Y | - | p.E410Gfs*43 (5) heterozygosis | |
| 33 | F24 | HBOCS | N | N | - | p.G382D (5) heterozygosis | NF1 p.N2220Ifs*25 (5) |
| 34 | F59 | HBOCS | Y | N | CRC + OC | p.G382D (5) heterozygosis | |
| 35 | F66 | HBOCS | N | N | - | p.G382D (5) heterozygosis | |
| 36 | F69 | HBOCS | N | N | - | p.G382D (5) heterozygosis | |
| 37 | M67 | HBOCS | Y | N | M | p.G382D (5) heterozygosis | |
| 38 | F62 | HBOCS | N | N | - | p.G382D (5) heterozygosis | |
| 39 | F54 | HBOCS | N | N | - | p.G382D (5) heterozygosis | |
| 40 | F69 | HBOCS | Y | N | CRC + OC | p.G382D (5) heterozygosis | BRCA2 (3) |
| 41 | F67 | HBOCS | Y | Y | OC | p.G382D (5) heterozygosis | |
| 42 | M70 | HBOCS | Y | N | PC + L | p.G382D (5) heterozygosis | |
| 43 | F37 | HBOCS | N | N | - | p.G382D (5) heterozygosis | |
| 44 | F44 | HBOCS | N | N | - | p.G382D (5) heterozygosis | |
| 45 | M63 | HBOCS | Y | N | PC + PCC | p.Y179C (5) heterozygosis | |
| 46 | F69 | HBOCS | Y | N | PCC | c.997+1G>T (4) heterozygous | |
| 47 | F50 | HNPCC | Y | N | CRC | p.Y179C (5) + p.E410Gfs*43 (5) compound heterozygosis | RAD50 p.E723Gfs*5 (5) |
| 48 | F63 | HNPCC | Y | N | CRC | p.G382D (5) heterozygosis | RAD50 p.E723Gfs*5 (5) |
| 49 | F50 | HNPCC | N | N | - | p.G382D (5) heterozygosis | |
| 50 | F76 | HNPCC | N | N | - | p.R368Qfs*164 (4) heterozygosis | |
| 51 | F39 | HNPCC | N | N | - | p.R368Qfs*164 (4) heterozygosis | |
| 52 | F52 | HNPCC | N | N | - | p.R368Qfs*164 (4) heterozygosis | |
| 53 | F73 | HL | Y | N | L | p.G382D (5) heterozygosis | |
| 54 | F48 | HL | N | N | - | p.G382D (5) heterozygosis | |
| 55 | M18 | HL | N | N | - | p.G382D (5) heterozygosis | |
| 56 | M56 | HRC | Y | N | RC + CRC + M | p.G382D (5) heterozygosis | SDHB p.P56Yfs*5 (5) |
| Prevalence | OR | |
|---|---|---|
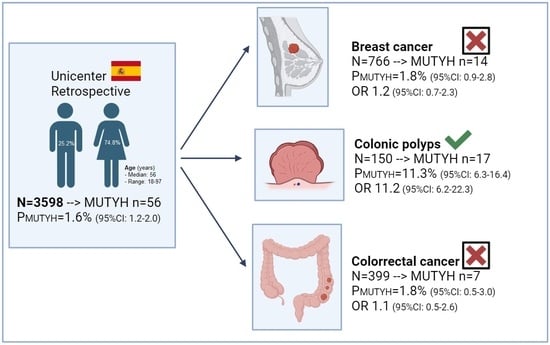
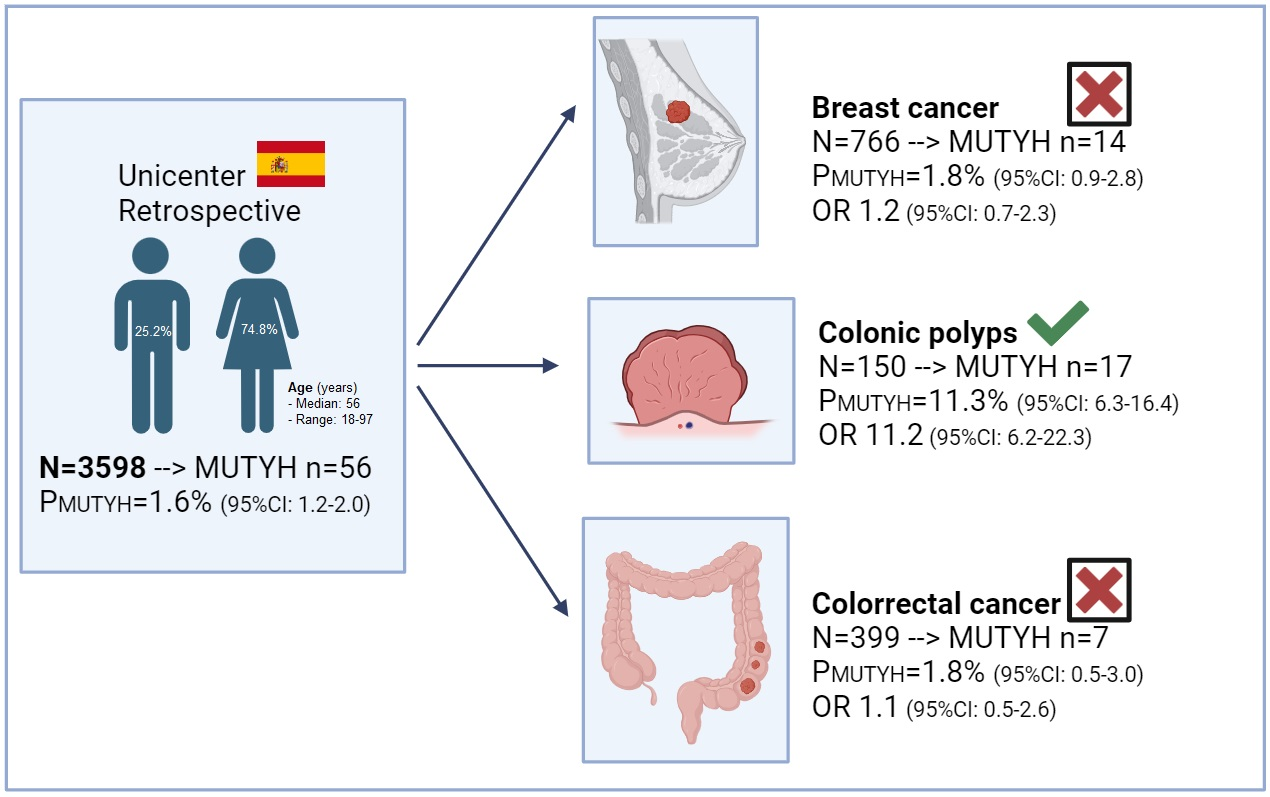
| Our setting | 1.6% (95%CI: 1.2–2.0) | - |
| Colonic polyposis | 11.3% (95%CI: 6.3–16.4) | 11.2 (95%CI: 6.2–22.3) |
| Ovarian cancer | 2.7% (95%CI: 0.4–5.0) | 1.8 (95%CI: 0.7–4.7) |
| Prostate cancer | 2.4% (95%CI 0.0–5.6) | 1.5 (95%CI: 0.4–6.4) |
| Breast cancer | 1.8% (95%CI: 0.9–2.8) | 1.2 (95%CI: 0.7–2.3) |
| Colorectal cancer | 1.8% (95%CI: 0.5–3.0) | 1.1 (95%CI: 0.5–2.6) |
| Pancreatic cancer | 1.7% (95%CI: 0.0–3.6) | 1.1 (95%CI: 0.3–3.6) |
| Article | Population | Sample Size | Prevalence |
|---|---|---|---|
| Kurian et al. 2014 [17] | Females with BC | 174 | 2.9% |
| Maxwell et al. 2015 [13] | Females with BC and BRCAx | 278 | 2.6% |
| Ellingson et al. 2015 [18] | Females with BC | 124 | 1.6% |
| Lin et al. 2016 [19] | Females with BC and HBOCS criteria | 133 | 0.8% |
| Rummel et al. 2017 [20] | Females with EOBC | 119 | 1.7% |
| Kaur et al. 2018 [21] | Females with BC | 296 | 5.6% |
| Meiss et al. 2018 [22] | Females with BC | 612 | 0.3% |
| Oliver et al. 2019 [23] | Latin Americans with HBOCS criteria | 222 | 1.4% |
| Rizzolo et al. 2018 [24] | Italian males with BC | 503 | 0.4% |
| Schneider et al. 2019 [25] | Patients with BC | 146 | 0.7% |
| Ryu et al. 2020 [26] | Patients with BC and HBOCS criteria | 507 | 0.6% |
| Chen et al. 2020 [27] | Chinese patients with BC | 524 | 0.8% |
| Kurian et al. 2021 [28] | Patients with BC | 15,256 | 1.4% |
| Oliveira et al. 2022 [29] | Patients with BC or OC | 971 | 2.7% |
| Tatineni et al. 2022 [30] | Patients with BC and HBOCS criteria | 922 | 1.4% |
| Our series | Patients with BC | 766 | 1.8% |
| Article | Population | Results |
|---|---|---|
| Rennert et al. 2012 [31] | Sephardi patients with BC (n = 389) vs. controls (n = 541) | Positive. Increase in BC in patients with heterozygous P/LP MUTYH G382D (6.7% vs. 3.7%, OR 1.86, 95%CI 1.02–3.39; p = 0.04). |
| Rizzolo et al. 2018 [24] | Males with BC and BRCAx (n = 503) vs. controls (n = 1540) | Positive. Heterozygous Y165C was associated with increased BC (OR 4.54, 95%CI 1.17–17.58, p = 0.028). |
| Beiner et al. 2008 [32] | Patients with BC (n = 691) vs. controls (n = 812) | Negative. No association in BC risk and heterozygous MUTYHmut. |
| Win et al. 2011 [33] | First and second-degree relatives (n = 2179) of 144 incident CCR cases who were mono/bi-allelic MUTYHmut carriers vs. expected number of cancers in general population | Negative. No association in BC and MUTYHmut (SIR 1.27, 95%CI 0.84–1.99, p = 0.28). |
| Out et al. 2012 [34] | Patients with incident BC (n = 1469) and patients with BC and BRCAx (n = 471) vs. controls (n = 1666) | Negative. No association in BC and monoallelic MUTYHmut. |
| Win et al. 2016 [35] | First and second-degree relatives (n = 5158) of 266 probands with MUTYHmut (42 biallelic and 225 monoallelic) vs. expected number of cancers in general population | Negative. No association in BC and monoallelic MUTYHmut (HR 1.4, 95%CI 1.0–2.0).Nevertheless, in the subgroup of female monoallelic mutation carriers, there is an estimated cumulative risk to age 70 years of BC of 11% (95%CI, 8%–16%) |
| Kurian et al. 2017 [28] | Patients with BC (n = 26,384) vs. controls (n = 64,649) | Negative. No association in BC and biallelic MUTYHmut (OR 0.55, 95%CI 0.22–1.38, p = 0.2) |
| Jian et al. 2017 [36] | Chinese patients with BC (n = 120) vs. Chinese women with high-risk for BC (n = 120) | Negative. No association in BC and MUTYHmut (1.7% vs. 5.8%, p = 0.17). |
| Fulk et al. 2019 [15] | Females with BC (n = 30,456) vs. controls (n = 12,289) | Negative. No association in BC and monoallelic MUTYHmut (OR 1.01, 95%CI 0.85–1.21, p = 0.89). |
| Thompson et al. 2022 [37] | Females with BC (n = 20,043) vs. controls (n = 22,150) | Negative. No association in BC and monoallelic P/LP MUTYHmut (1.9% vs. 1.7%, OR 1.1, 95%CI 0.96–1.3, p = 0.15). |
| Guindalini et al. 2022 [38] | Brazilian patients with BC (n = 1663) vs. controls (n = 18,919) | Negative. No association in BC and monoallelic MUTYHmut G382D (1.2% vs. 0.9%, OR 1.4, 95%CI: 0.8–2.4; p = 0.29) or Y165C (0.8% vs. 0.4%, OR 1.9. 95%CI 0.9–3.9, p = 0.09). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peña-López, J.; Jiménez-Bou, D.; Ruíz-Gutiérrez, I.; Martín-Montalvo, G.; Alameda-Guijarro, M.; Rueda-Lara, A.; Ruíz-Giménez, L.; Higuera-Gómez, O.; Gallego, A.; Pertejo-Fernández, A.; et al. Prevalence and Distribution of MUTYH Pathogenic Variants, Is There a Relation with an Increased Risk of Breast Cancer? Cancers 2024, 16, 315. https://doi.org/10.3390/cancers16020315
Peña-López J, Jiménez-Bou D, Ruíz-Gutiérrez I, Martín-Montalvo G, Alameda-Guijarro M, Rueda-Lara A, Ruíz-Giménez L, Higuera-Gómez O, Gallego A, Pertejo-Fernández A, et al. Prevalence and Distribution of MUTYH Pathogenic Variants, Is There a Relation with an Increased Risk of Breast Cancer? Cancers. 2024; 16(2):315. https://doi.org/10.3390/cancers16020315
Chicago/Turabian StylePeña-López, Jesús, Diego Jiménez-Bou, Icíar Ruíz-Gutiérrez, Gema Martín-Montalvo, María Alameda-Guijarro, Antonio Rueda-Lara, Leticia Ruíz-Giménez, Oliver Higuera-Gómez, Alejandro Gallego, Ana Pertejo-Fernández, and et al. 2024. "Prevalence and Distribution of MUTYH Pathogenic Variants, Is There a Relation with an Increased Risk of Breast Cancer?" Cancers 16, no. 2: 315. https://doi.org/10.3390/cancers16020315
APA StylePeña-López, J., Jiménez-Bou, D., Ruíz-Gutiérrez, I., Martín-Montalvo, G., Alameda-Guijarro, M., Rueda-Lara, A., Ruíz-Giménez, L., Higuera-Gómez, O., Gallego, A., Pertejo-Fernández, A., Sánchez-Cabrero, D., Feliu, J., & Rodríguez-Salas, N. (2024). Prevalence and Distribution of MUTYH Pathogenic Variants, Is There a Relation with an Increased Risk of Breast Cancer? Cancers, 16(2), 315. https://doi.org/10.3390/cancers16020315