Simple Summary
RCC has traditionally been considered radioresistant, with surgery being the gold standard for primary localized RCC. However, not all patients are suitable for surgery and percutaneous, non-surgical options are invasive, with significant limitations. SABR is a non-invasive advanced RT technique that delivers high doses accurately. Growing evidence supports SABR as a definitive alternative therapy for medically inoperable patients, those who decline surgery, are unfit for invasive ablation, or are at high-risk of requiring postoperative dialysis. SABR has shifted the renal radioresistance paradigm, widening the therapeutic window. Additionally, SABR is increasingly used for locally recurrent, oligoprogressive, and oligometastatic disease. This review aims to support the use of SABR across various stages of RCC disease and explore future directions. The overall landscape of RCC is promising, and we are confident that our update will stimulate further research in this field and contribute to the advancement of patient care.
Abstract
Renal cell cancer (RCC) has traditionally been considered radioresistant. Because of this, conventional radiotherapy (RT) has been predominantly relegated to the palliation of symptomatic metastatic disease. The implementation of stereotactic ablative radiotherapy (SABR) has made it possible to deliver higher ablative doses safely, shifting the renal radioresistance paradigm. SABR has increasingly been adopted into the multidisciplinary framework for the treatment of locally recurrent, oligoprogressive, and oligometastatic disease. Furthermore, there is growing evidence of SABR as a non-invasive definitive therapy in patients with primary RCC who are medically inoperable or who decline surgery, unsuited to invasive ablation (surgery or percutaneous techniques), or at high-risk of requiring post-operative dialysis. Encouraging outcomes have even been reported in cases of solitary kidney or pre-existing chronic disease (poor eGFR), with a high likelihood of preserving renal function. A review of clinical evidence supporting the use of ablative radiotherapy (SABR) in primary, recurrent, and metastatic RCC has been conducted. Given the potential immunogenic effect of the high RT doses, we also explore emerging opportunities to combine SABR with systemic treatments. In addition, we explore future directions and ongoing clinical trials in the evolving landscape of this disease.
1. Introduction
Radiotherapy (RT) has not traditionally been considered a good treatment option for renal cell cancer (RCC), as it was thought to be intrinsically radioresistant. This view was formed in the 1970s [1,2,3] following studies that showed a lack of benefit from adjuvant and neo-adjuvant RT, delivered at doses that would currently be considered suboptimal. In addition, the kidney was considered to be at risk of radiation-induced long-term damage from relatively low doses of RT [4]. Because of this, RT was relegated to palliative use [5].
Until recently, therapy for primary RCC was limited to invasive local interventions, including surgery (open, robotic, or laparoscopic) or percutaneous interventions such as microwave ablation, radiofrequency ablation (RFA), or cryotherapy as the main options.
Surgical resection remains the standard of care (SOC) in localized disease, but this approach is not feasible in all patients due to disease factors, e.g., size, location, and/or patient factors, including co-morbidities and patient choice. Percutaneous techniques also have significant limitations.
Contrary to the historical notion of radioresistant disease, the current landscape has changed significantly with the advent of stereotactic ablative radiotherapy (SABR). Preclinical models have suggested ablative doses of RT may overcome the hypothetical radioresistance mechanism based on the activation of HIF1α (which is characteristic of clear cell cancers with von Hippel-Lindau [VHL] mutations), which stimulates endothelial cell survival, inducing cell death by alternative means to DNA damage and mitotic catastrophe [5].
SABR is a non-invasive advanced RT technique that delivers high doses accurately with a very steep dose gradient over a small number of treatment sessions, usually 5 sessions or less. This approach has recently shown promising local control (LC), an acceptable side-effect profile, and good preservation of renal function (nephron-sparing) in primary RCC for tumors up to 10 cm in diameter, even when these are encroaching on the central portion of the kidney or on the collecting system [6]. It has also been shown to be a safe approach in solitary kidney cases [7]. Given that, its use has become increasingly integrated into multidisciplinary management at different stages of the disease.
A review of clinical evidence supporting the use of ablative radiotherapy in primary, recurrent, and metastatic RCC has been conducted. Given the potential immunogenic effect of the high RT doses, we also explore emerging opportunities to combine systemic targeted agents or immunotherapies with ablative radiation (SABR) as a promising approach that might improve outcomes. In addition, we explore future directions and ongoing clinical trials in the evolving landscape of this disease.
2. Non-Surgical Approaches of Primary Renal Cell Cancer (RCC)
Surgery, either partial or total nephrectomy, remains the gold standard local intervention, where possible, in primary localized RCC. However, not all patients are suitable for a surgical approach. Non-surgical options include microwave ablation, RFA, or cryotherapy as the main options but they also present significant limitations and are invasive. They can typically only treat smaller tumors (<4 cm) which need to be distant from the collecting system and vascular structures due to the risk of heat sink effects, which can result in stricture and/or fistula [8].
Some studies have shown the feasibility of other ablative techniques, such as high-intensity, focused ultra-sound ablation and non-thermal, irreversible electroporation. However, these techniques are still considered experimental [9].
Given the limitations of surgery and non-surgical techniques, an ablative, non-invasive alternative was needed.
3. The Emerging Role of Stereotactic Ablative Radiotherapy (SABR) for Primary RCC
The technological evolution that RT has undergone has permitted more accurate treatments and consequently higher doses per fraction, while sparing critical surrounding organs at risk (OAR) delivered in ultra-hypofractionated treatment schedules. Kidney SABR has emerged as an ablative approach with curative intent in the primary RCC setting, particularly in the context of patients with primary RCC who are medically inoperable, refuse surgery, or are at high risk of surgical complications (larger renal masses > 4 cm or where the tumor is close to the renal pelvis), who have limited curative treatment options.
There is a growing body of evidence supporting the use of SABR for primary RCC management, including several retrospective studies, systematic reviews, and meta-analyses, as well as the promising results of the first large prospective trial, which has recently been published [7].
In contrast, in the SABR meta-analyses by Correa et al. [10], 26 studies were identified (11 prospective trials), including 383 tumors in 372 patients, most of whom were deemed inoperable. Median follow-up, median age, and mean tumor size were 28.0 (5.8–79.2) months, 70.4 (62–83) years, and 4.6 (2.3–9.5) cm, respectively. Dose fractionation varied, but 26 Gy in one fraction and 40 Gy in five fractions were the most common. The random-effect estimated for LC was 97.2%, grade 3–4 toxicity 1.5%, and post-SABR estimated glomerular filtration rate (eGFR) decrease of 7.7 mL/min. Six patients with pre-existing renal dysfunction (2.9%) required dialysis. Reported toxicity includes mild nausea, fatigue, dermatitis, pyelonephritis, gastric/duodenum ulcer. There was no treatment-related mortality.
In addition, the International Radiosurgery Oncology Consortium for Kidney (IROCK) [11] published a series of 223 patients with non-metastatic kidney cancer (around 50% with tumors > 4 cm diameter) treated with a single fraction of 25 Gy or multi-fractioned SABR to a median dose of 40 Gy. The five-year LC rate was 94.5%. Most patients had a reduction in eGFR (mean decrease of 5.5 mL/min), with a corresponding rise in creatinine after treatment (mean 28 μmol/L), with six patients requiring dialysis.
Even in cases where the patient only has a single kidney, SABR to the RCC is a potential treatment option [12], showing a 2-year LC of 98% and a change in eGFR ranging from a decrease of 5.8 mL/min to an improvement of 10.8 mL/min. No patients required dialysis.
Furthermore, the International Society of Stereotactic Radiosurgery (ISRS) conducted a systematic review [13] of 36 publications (822 eligible patients). The median LC rate was 94.1% (70.0–100), 5-year progression-free survival (PFS) was 80.5% (95% CI 72–92), and 5-year overall survival (OS) was 77.2% (95% CI 65–89).
Finally, the TransTasman Radiation Oncology Group (TROG) has recently reported encouraging outcomes of TROG 15.03 FASTRACK II [7,14,15]. This prospective phase II trial included 70 patients with biopsy-confirmed RCC. Patients with inoperable, high-risk, single-lesion kidney tumors or those who declined surgery were enrolled. Treated tumors were relatively large, measuring, on average, 4.7 cm. Patients with tumors < 4 cm (cT1a) received a single fraction of radiation (n = 23), and those with tumors > 4 cm (≥T1b) received three fractions (n = 47). None of the patients experienced local progression of their RCC during the FU (median 43 months), nor did any patients die from cancer. OS was 99% at 1 year after SABR and 82% at 3 years. One patient experienced a distant recurrence of their cancer. Cancer-specific survival (CSS) for longer than 3 years was 100%. Adverse effects (AEs) were relatively modest, with no grade 4 or 5 toxicities observed. Seven patients (10%) experienced grade 3 AEs, most commonly abdominal pain (n = 3). Fifty-one patients (73%) had grade 1 or 2 treatment-related AEs, and 11 patients (16%) experienced no AEs.
Renal function was assessed by measuring eGFR, with a key exclusion criterion being a pre-treatment eGFR < 30 mL/min per 1.73 m2. The cohort enrolled had significant pre-existing chronic disease (baseline mean eGFR of 61.1 mL/min per 1.73 m2). The average glomerular filtration rate declined by 10.8 mL/min at 1 year and 14.6 mL/min at 2 years after treatment, indicating mild-to-moderate kidney stress. Only one patient required dialysis following treatment. Overall, there was a modest drop in kidney function, which plateaued after 2 years. In fact, in the context of worse baseline renal function and larger tumors compared with surgical trials, the observed mean decline in eGFR in FASTRACK II [7] is similar to the expected decline with partial nephrectomy. The high efficacy rate and the ability to preserve kidney function was attributed to rigorous quality control, as well as the effectiveness of stereotactic radiation.
In line, IROCK recently demonstrated [16] a moderate decline in renal function with a low rate of dialysis at 5 years following SABR. Patients with a solitary kidney (n = 56) were compared with those with bilateral kidneys (n = 134). The eGFR decreased by −14.5 (SD 7.6) and −13.3 (SD 15.9) mL/min (p = 0.67), respectively, with similar rates of post-SABR dialysis (3.6% vs. 3.7%). A multivariable analysis demonstrated that increasing tumor size (OR per 1 cm: 1.57) and baseline eGFR (OR per 10 mL/min: 1.30) were associated with an eGFR decline of ≥ 15 mL/min at one year.
Table 1 is a summary of the most recent studies of SABR in primary localized RCC.

Table 1.
SABR Studies in primary localized RCC.
4. The Optimal Dose Schedule for SABR in Primary RCC
Currently, there is no single standard dose and fractionation. There are a range of options, which are still a matter of some debate and research (Table 1). However, there is a consensus on administering a biologically equivalent dose in 2 Gy per fraction (EQD2) equal or higher than 72 Gy [13], highlighting that this suggests a dose–effect relationship. Renal function reduces linearly with dose received by the healthy ipsilateral kidney up to 100 Gy BED3. In FASTRACK II [7], the local renal function loss was higher in the 3-fraction cohort than in the single-fraction at 12 and 24 months [23]. Given this, reducing the ipsilateral kidney volume receiving 50% of the dose at the planning stage is recommended to minimize loss of renal function post-SABR treatment. In addition, improving the plan quality overall by using advanced technologies such as better motion management is also recommended [18,22].
The ISRS [13] recommends that optimal dose regimens for SABR in patients with primary RCC include 26 Gy in one fraction if the tumor is ≤4–5 cm and 42–48 Gy in three fractions if the tumor is >4–5 cm, or even 40 Gy in five fractions if the dose constraints for OARs cannot be met for three fractions.
This is in line with the FASTRACK II trial [15], where differences in oncological outcomes between single-fraction and three-fraction SABR schedules were not observed; however, the fractionation schedules represented two different populations based on tumor size.
The Royal College of Radiologists in the United Kingdom have recently published a list of recommended dose/fractionations for a wide range of tumor types. The doses recommended are in line with the above, including 26 Gy in 1 fraction or multiple fraction regimens, such as 42 Gy in 3 fractions/40 Gy in 5 fractions [24].
Table 2 summarizes current recommendations on dosing schedules, and Figure 1 shows some representative cases of SABR for primary RCC.
Table 2.
Commonly used dose and prescription.
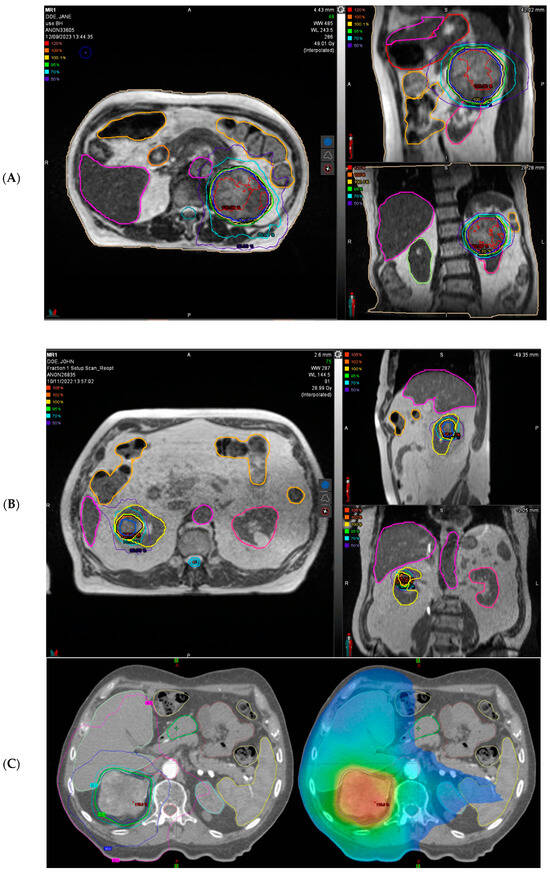
Figure 1.
Representative patients’ treatment plan of stereotactic ablative radiotherapy (SABR) for primary renal cell carcinoma (RCC). (A) A representative radiotherapy plan treating a large (8.5 cm) left-sided RCC with 40 Gy in five fractions is shown in 3 planes on MR-Linac (ViewRay®, Oakwood Village, OH, USA). Planning System MIM® 7.2.8 (Cleveland, OH, USA). (B) A representative radiotherapy plan treating a right-sided RCC with 26 Gy in one single fraction is shown in 3 planes on MR-Linac (ViewRay®). Planning System MIM® 7.2.8. (C) A representative radiotherapy plan treating a right-sided RCC with 42 Gy in 3 fraction (every other day) is shown in 3 planes on conventional linac (Varian® Clinac 2300 iX, Varian Medical Systems, Palo Alto, CA, USA).
5. Response Evaluation/Follow-Up
To date, LC after SABR is measured using the Response Evaluation Criteria in Solid Tumors (RECIST). This method is still considered the most robust tool for assessing progression following RT but has some limitations with SABR.
In contrast to percutaneous ablation, SABR does not immediately obliterate the tumor and vascular architecture but instead relies primarily upon DNA damage causing loss of proliferative capacity, with ongoing development of cell kill over a prolonged period of time [10]. The typical post-ablation changes, such as immediate histological changes, loss of contrast enhancement, or a complete response, are therefore not seen after SABR. In fact, persistent enhancement following RT is common and not correlated with a risk of subsequent progression in RCC [7]. Furthermore, RCC is a slow-growing tumor, and it can be expected to show a slow radiographic response to treatment.
“Pseudoprogression” is a commonly observed phenomenon in RCC, as the tumor may show an initial size increase that may be misinterpreted as disease progression but may actually be due to treatment-induced inflammation and edema. This eventually stabilizes or results in shrinkage over a prolonged period [25]. To avoid being misled by pseudoprogression, it is best to delay initial imaging after SABR until at least 3 months from completion of treatment [7].
SABR tends to cause a slow decrease in size over months to years, the rate of which does not appear to depend on the dose delivered to the tumor. In the evaluation of response after SABR, the definition of LC is that of stable disease. Ongoing enhancement, or even occasionally increased enhancement, in some cases, can be misinterpreted as persistent or recurrent disease, although no correlation with local failure has been observed [26]. Response assessment after SABR is challenging and demands close monitoring with frequent and long-term imaging follow-up.
Future research is focusing on multiparametric magnetic resonance imaging (MRI) and positron emission tomography (PET), which hold the promise of a better response assessment after SABR [27]. Novel modalities, including functional MRI sequences, showed promise in detecting early response to therapy. In fact, early changes in diffusion and perfusion following renal SABR appear to be a potential predictive imaging biomarker that correlates with subsequent CT–based tumor response.
Biopsy after SABR is not recommended in routine clinical practice and should be considered experimental, as the microscopic evaluation of viable cells can be misleading after exposure to radiation [28].
To conclude, no single follow-up plan is appropriate for all patients; therefore, it should be individualized based on the patient’s requirements [29]. Nevertheless, the general follow-up consensus includes regular cross-sectional imaging, which could be either CT or MRI scans, undertaken initially 3 months after completion of treatment, and then again at 6 and 12 months. After that, scans can be arranged every 6–12 months, as clinically indicated [13,29]. This is in line with what Siva et al proposed, as summarized in the Figure 2.
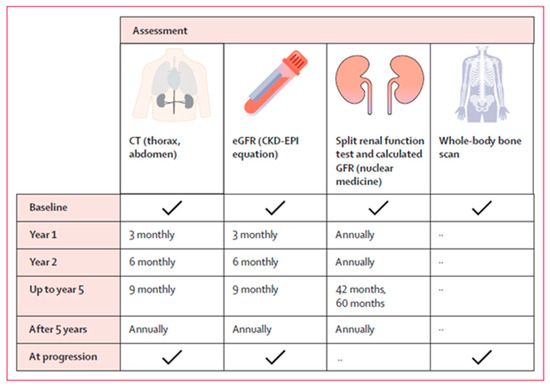
Figure 2.
The schedule of assessment proposed by Siva S et al., 2024 [7].
6. The Role of Stereotactic Ablative Radiotherapy (SABR) for Metastatic RCC (mRCC)
Approximately 20% of renal carcinoma patients present with metastatic disease (synchronous) and another 25–40% develop metastasis after radical treatment of the primary (metachronous) [24].
The SOC for metastatic RCC (mRCC) is systemic therapy (ST). Recent breakthroughs in ST, specifically, with immunotherapy (IO) and tyrosine kinase inhibitors (TKIs), have expanded lines of treatment and improved survival. Unfortunately, a cure for mRCC remains elusive, and complete responses are uncommon. Thus, it is important to develop new ST or new combination regimens, maximize the benefit of available therapies, and carefully delay initiation of ST whenever possible.
Metastatic-directed therapy (MDT) historically involved surgery [30] but has recently expanded to include SABR. SABR has emerged as an attractive therapeutic option in the setting of limited metastatic disease (between three and five metastases). Its effectiveness has been demonstrated in prospective clinical trials for selected patients with oligometastases and oligoprogression of different primary histology and lesion locations, both instead of and in combination with ST [31,32,33]. By leaving the tumor in situ, SABR may also induce immune remodeling, both intratumorally and within the systemic metastases, which may augment response to ST [34].
However, in the mRCC scenario, there are still limitations in the published literature, which are mainly retrospective in nature [35] and a lack of high-level evidence from randomized clinical trials. Therefore, the European Society of Therapeutic Radiation Oncology (ESTRO) has recently developed consensus recommendations to provide guidance on the application of SABR in oligometastatic RCC and to highlight the key areas of ongoing debate [36]. Panelists agreed not to apply age or primary RCC histology restrictions for SABR candidates. They established an upper threshold of three lesions to offer ablative treatment in the oligoprogressive setting and agreed on the concomitant administration of immune checkpoint inhibitors (ICI) (within 30 days from SABR). In addition, SABR was agreed upon as the modality of choice for RCC bone and adrenal oligometastases. Although no consensus was reached, there was a major agreement that SABR should be administered on an every-other-day scheme, and it could also represent a useful tool to postpone ST change in selected cases.
7. Overview of the Combination of Systemic Therapy (Chemo/IO/Targeted) with SABR for Metastatic RCC (mRCC)
The potential immunomodulatory effect of SABR has led to increased interest in its use in combination with immunotherapy (IO) via the abscopal effect and targeted agents. Preclinical data strongly support this synergy [37], as do emerging results from clinical trials such as RADVAX [38], which reported a 56% response rate of non-irradiated lesions in patients with high-volume mRCC.
In the neoadjuvant setting (neo-SABR), 3 patients with mRCC at diagnosis within a clinical trial (NCT02473536) also showed response in the unirradiated lesions without the concurrent use of ST; therefore, this response was attributable to the abscopal effect. In addition, neo-SABR resulted in decreased Ki-67 and increased PD-L1 expression [39].
In the oligometastatic setting, SABR and a short course of pembrolizumab were evaluated in the RAPPORT trial, which showed an acceptable toxicity profile (13% of G3 and 0% G4–5), with excellent LC (92% at 2 years) [40].
Furthermore, patients receiving ST often develop resistance because of intratumoral mutational heterogeneity and consequently, disease progression. Oligoprogression (OP) means that the progression occurs in a select number of metastases while other lesions remain responsive or stable to a given ST. For these patients, switching to another ST is the SOC. Unfortunately, subsequent lines of therapy are often less effective, and patients ultimately run out of options. In this scenario, administering high doses of RT (SABR) to the drug-resistant sites of progression may overcome this adaptive resistance [39], improving LC while extending the duration of the systemic agent administered. Cheung et al. [41] reported the first prospective trial testing SABR in 37 patients with mRCC receiving tyrosine kinase inhibitors (TKIs) with ≤5 progressing lesions and showed 93% LC and a time-to-change in ST of 12.6 months. Similarly, Hannan et al. [42] treated 37 lesions in 20 patients with oligoprogressive mRCC receiving TKIs, immune checkpoint inhibitors (ICIs), or mammalian target of rapamycin inhibitors (mTORs), with 100% LC, and a time-to-change in ST of 11.1 months.
In contrast, SABR as a monotherapy can be performed as a strategy for postponing the initiation of ST in a low-burden metastatic setting. One such study by Hannan et al. [43] reported a 91% rate of freedom from ST and 100% of LC in mRCC patients with ≤3 mets. Similarly, Tang et al. [44] showed excellent LC and OS rates (97% and 100%, respectively). However, the 1-year PFS was 64%, suggesting that most progressions occur outside the RT field.
With regard to anti-angiogenic TKIs, caution should be exercised when combining these with RT, particularly when the field encompasses a critical tissue such as brain, spinal cord, liver, or small bowel. Although there are no formal guidelines yet, drug interruption would be advisable when delivering higher palliative doses over critical structures [45].
A summary of important clinical trials’ results is listed in Table 3.
Table 3.
Studies of SABR in patients with metastatic renal cancer (mRCC).
Despite the increasing use in routine clinical practice, there is still little information on the safety of combining SABR with modern targeted therapy or IO, and a paucity of high-level evidence to guide clinical management. It is for this reason that consensus such as the OligoCare consortium [47] and further clinical trial results are much needed to guide our daily practice and allow for adequate patient selection.
8. SABR as Salvage Treatment for Locoregional Recurrent RCC
Locoregional recurrence after nephrectomy for localized RCC is rare (2–6%) due to improving surgical techniques and adjuvant therapies. However, 5-year survival decreases to 18–46% after recurrence, and the median CSS was 0.7–1 year if left untreated [48].
In this setting, systemic therapy remains the cornerstone approach, and although RT has been investigated for decades, the vast majority of studies have focused exclusively on the intraoperative RT (IORT) [49,50,51,52,53,54].
The selection criteria and efficacy of different treatments are unclear but local therapy could delay disease progression compared with ST alone. In this context, SABR might be effective, but there is a lack of data, which therefore means this is only a theoretical benefit that can be extrapolated from the outcomes of primary tumor SABR.
Only one [48] retrospective series is available, by Yang Liu et al. [48]. In this series, 106 patients with recurrent RCC without distant metastasis were analyzed, 31% of which received ST alone and 69% local therapy (34/73 surgery and SABR −30–40 Gy/5 fractions -in 39/73 patients). Patients receiving local therapy had significantly longer PFS than ST (19.7 vs. 7.5 months, p = 0.001). After matching, the PFS in the local therapy group remained higher (23.9 vs. 7.5 months, p = 0.001). The median PFS of patients undergoing surgery, SBRT, and ST alone was 15.4, 21.9, and 7.5 months, respectively (p = 0.003). The 2-year OS of the local therapy group and ST group was 91.6% and 71.8%, respectively (p = 0.084). Local therapy was associated with better PFS (HR 0.37; p = 0.0003) and OS (HR 0.23; p = 0.002) in multivariate analysis. Grade 2 or higher toxicities related to local therapy occurred in 9/73 patients. Patients undergoing locally directed therapy demonstrated a significantly decreased risk of progression by over 60% (HR 0.37; 95% CI 0.21–0.64; p = 0.0003) and risk of death by around 70% (HR 0.23; 95% CI 0.09–0.58; p = 0.002).
Therefore, SABR could play a role in the salvage of local recurrence cases with a low toxicity profile and good local control.
9. Review of Current Guidelines
Some of the main international clinical guidelines have already included SABR in primary RCC as an alternative therapy in medically inoperable patients [13,29,55]. Even though early results of SABR look encouraging, the latest 2024 European Association of Urology (EAU) update does not yet fully endorse this approach, suggesting that well-conducted prospective studies with longer follow-up are needed [9].
Table 4 shows the recommendations of current guidelines.
Table 4.
Review of current guidelines.
10. Future Directions/Ongoing Trials
SABR has become the standard treatment for primary RCC in patients unsuitable for other ablative techniques given the potentially high risk of toxicity (>4 cm or proximity to the renal pelvis). The promising outcomes of FASTRACK II [7,14] have shown the potential of this technique with curative intent in a primary setting to be not only an alternative to other local techniques but also a standard alternative to surgery if future studies corroborate its efficacy and toxicity profile. We look forward to seeing the design of randomized trials of SABR versus surgery for primary RCC.
Stereotactic magnetic resonance (MR)-guided adaptive radiotherapy (SMART) may result in more precise treatment delivery through its capabilities for improved image quality, daily adaptive planning, and respiratory motion during treatment with real-time tracking. Thus, a reduction of target volume margins can be applied, and therefore, a reduction in the impairment of kidney function could be achieved. Preliminary outcomes are encouraging [18,22], further results are awaited (MRI-MARK Trial-NCT04580836), and even potential predictive biomarkers of radiosensitivity are being investigated (the ISRAR Database).
In line with the rationale of cytoreductive surgery (CARMENA [57] and SURTIME [58] randomized trials), the cytoreductive role of SABR in mRCC is being investigated, with the advantage not just being a less invasive approach, but also of maintaining the pro-immunogenic and abscopal effect [39,59,60].
The role for SABR in deferring, enhancing, or delaying the switching of systemic therapy upon oligoprogression is another investigational field [60].
It is unclear which patients would derive the most benefit from a particular treatment approach. Thus, identifying, developing, and integrating multimodal biomarkers and driver mutations that predict therapeutic response and resistance is of critical importance to stratify and select suitable candidates. Emerging techniques such as spatial transcriptomics, single-cell analysis, and circulating tumor DNA show tremendous promise in both enhancing our understanding of RCC and uncovering new biomarkers. Advancements in this scenario could further transform the clinical management of RCC, moving toward more personalized and precise therapeutic interventions.
From the above, we can conclude that ongoing trials will help clarify the optimal patient selection, the impact of disease presentation, molecular subclassifications, the optimal combination of therapies, and SABR dosing, fractionations, and sequencing. In the meantime, there is work to be done to implement RCC SABR in our multidisciplinary decision-making framework across different stages of this disease.
Table 5 summarizes the most relevant ongoing trials in kidney SABR.
Table 5.
Main ongoing studies.
11. Conclusions
The management of RCC is evolving rapidly. SABR represents an attractive and safe option, and this has resulted in its implementation in the therapeutic algorithm in different stages of this disease, alone or in combination with systemic therapy. The promising outcomes of phase II prospective trials are reshaping the landscape of primary localized RCC. The design of randomized trials of SABR versus surgery in this scenario are awaited, but, to date, the available data encourage its implementation as a non-invasive ablative alternative for localized RCC. With metastatic RCC, SABR use has increased in routine clinical practice but there are still unsolved questions about the best candidates, treatment combinations, and schedules. Nevertheless, the overall landscape of RCC is promising, with several ongoing trials, the results of which will help to guide and optimize the diagnosis and treatment tools on a case-by-case basis.
Author Contributions
Conceptualization—P.C. and E.M.-O.; methodology—P.C. and E.M.-O.; writing—original draft preparation—A.S., P.D., N.D., D.F., C.P. and E.M.-O.; writing—review and editing—P.C. and E.M.-O.; supervision—P.C. and E.M.-O. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Finney, R. An evaluation of postoperative radiotherapy in hypernephroma treatment—A clinical trial. Cancer 1973, 32, 1332–1340. [Google Scholar] [CrossRef]
- Juusela, H.; Malmio, K.; Alfthan, O.; Oravisto, K.J. Preoperative irradiation in the treatment of renal adenocarcinoma. Scand. J. Urol. Nephrol. 1977, 11, 277–281. [Google Scholar] [CrossRef]
- van der Werf-Messing, B. Proceedings: Carcinoma of the kidney. Cancer 1973, 32, 1056–1061. [Google Scholar] [CrossRef]
- Dawson, L.A.; Kavanagh, B.D.; Paulino, A.C.; Das, S.K.; Miften, M.; Li, X.A.; Pan, C.; Haken, R.K.T.; Schultheiss, T.E. Radiation-associated kidney injury. Int. J. Radiat. Oncol. 2010, 76 (Suppl. S3), S108–S115. [Google Scholar] [CrossRef]
- Siva, S.; Kothari, G.; Muacevic, A.; Louie, A.V.; Slotman, B.J.; Teh, B.S.; Lo, S.S. Radiotherapy for renal cell carcinoma: Renaissance of an overlooked approach. Nat. Rev. Urol. 2017, 14, 549–563. [Google Scholar] [CrossRef]
- Ali, M.; Mooi, J.; Lawrentschuk, N.; McKay, R.R.; Hannan, R.; Lo, S.S.; Hall, W.A.; Siva, S. The Role of Stereotactic Ablative Body Radiotherapy in Renal Cell Carcinoma. Eur. Urol. 2022, 82, 613–622. [Google Scholar] [CrossRef]
- Siva, S.; Bressel, M.; Sidhom, M.; Sridharan, S.; Vanneste, B.G.; Davey, R.; Montgomery, R.; Ruben, J.; Foroudi, F.; Higgs, B.; et al. Stereotactic ablative body radiotherapy for primary kidney cancer (TROG 15.03 FASTRACK II): A non-randomised phase 2 trial. Lancet Oncol. 2024, 25, 308–316. [Google Scholar] [CrossRef]
- Zagoria, R.J.; Hawkins, A.D.; Clark, P.E.; Hall, M.C.; Matlaga, B.R.; Dyer, R.B.; Chen, M.Y. Percutaneous CT-Guided radiofrequency ablation of renal neoplasms: Factors influencing success. Am. J. Roentgenol. 2004, 183, 201–207. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bensalah, K.; Dabestani, S.; Fernández-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma; European Association of Urology: Arnhem, The Netherlands, 2024. [Google Scholar]
- Correa, R.J.; Louie, A.V.; Zaorsky, N.G.; Lehrer, E.J.; Ellis, R.; Ponsky, L.; Kaplan, I.; Mahadevan, A.; Chu, W.; Swaminath, A.; et al. The Emerging Role of Stereotactic Ablative Radiotherapy for Primary Renal Cell Carcinoma: A Systematic Review and Meta-Analysis. Eur. Urol. Focus 2019, 5, 958–969. [Google Scholar] [CrossRef]
- Siva, S.; Ali, M.; Correa, R.J.; Muacevic, A.; Ponsky, L.; Ellis, R.J.; Lo, S.S.; Onishi, H.; Swaminath, A.; McLaughlin, M.; et al. 5-year outcomes after stereotactic ablative body radiotherapy for primary renal cell carcinoma: An individual patient data meta-analysis from IROCK (the International Radiosurgery Consortium of the Kidney). Lancet Oncol. 2022, 23, 1508–1516. [Google Scholar] [CrossRef]
- Correa, R.J.M.; Louie, A.V.; Staehler, M.; Warner, A.; Gandhidasan, S.; Ponsky, L.; Ellis, R.; Kaplan, I.; Mahadevan, A.; Chu, W.; et al. Stereotactic Radiotherapy as a Treatment Option for Renal Tumors in the Solitary Kidney: A Multicenter Analysis from the IROCK. J. Urol. 2019, 201, 1097–1103. [Google Scholar] [CrossRef]
- Siva, S.; Louie, A.V.; Kotecha, R.; Barber, M.N.; Ali, M.; Zhang, Z.; Guckenberger, M.; Kim, M.S.; Scorsetti, M.; Tree, A.C.; et al. Stereotactic body radiotherapy for primary renal cell carcinoma: A systematic review and practice guideline from the International Society of Stereotactic Radiosurgery (ISRS). Lancet Oncol. 2024, 25, e18–e28. [Google Scholar] [CrossRef]
- Siva, S.; Bressel, M.; Sidhom, M.; Sridharan, S.; Vanneste, B.; Davey, R.; Ruben, J.; Foroudi, F.; Higgs, B.G.; Lin, C.; et al. TROG 15.03/ANZUP International Multicenter Phase II Trial of Focal Ablative STereotactic RAdiotherapy for Cancers of the Kidney (FASTRACK II). Int. J. Radiat. Oncol. Biol. Phys. 2023, 117, S3. [Google Scholar] [CrossRef]
- Siva, S.; Chesson, B.; Bressel, M.; Pryor, D.; Higgs, B.; Reynolds, H.M.; Hardcastle, N.; Montgomery, R.; Vanneste, B.; Khoo, V.; et al. TROG 15.03 phase II clinical trial of Focal Ablative STereotactic Radiosurgery for Cancers of the Kidney—FASTRACK II. BMC Cancer 2018, 18, 1030. [Google Scholar] [CrossRef]
- Tan, V.S.; Correa, R.J.; Warner, A.; Ali, M.; Muacevic, A.; Ponsky, L.; Ellis, R.J.; Lo, S.S.; Onishi, H.; Swaminath, A.; et al. Long-term Renal Function Outcomes after Stereotactic Ablative Body Radiotherapy for Primary Renal Cell Carcinoma Including Patients with a Solitary Kidney: A Report from the International Radiosurgery Oncology Consortium of the Kidney. Eur. Urol. Oncol. 2024. [Google Scholar] [CrossRef]
- Peddada, A.V.; Anderson, D.; Blasi, O.C.; McCollough, K.; Jennings, S.B.; Monroe, A.T. Nephron-Sparing Robotic Radiosurgical Therapy for Primary Renal Cell Carcinoma: Single-Institution Experience and Review of the Literature. Adv. Radiat. Oncol. 2020, 5, 204–211. [Google Scholar] [CrossRef]
- Tetar, S.U.; Bohoudi, O.; Senan, S.; Palacios, M.A.; Oei, S.S.; van der Wel, A.M.; Slotman, B.J.; van Moorselaar, R.J.A.; Lagerwaard, F.J.; Bruynzeel, A.M.E. The Role of daily adaptive stereotactic MR-guided radiotherapy for renal cell cancer. Cancers 2020, 12, 2763. [Google Scholar] [CrossRef]
- Staehler, M.; Schuler, T.; Spek, A.; Rodler, S.; Tamalunas, A.; Fürweger, C.; Muacevic, A. Propensity Score-Matched Analysis of Single Fraction Robotic Radiosurgery Versus Open Partial Nephrectomy in Renal Cell Carcinoma: Oncological Outcomes. Cureus 2022, 14, e21623. [Google Scholar] [CrossRef]
- Lapierre, A.; Badet, L.; Rouviere, O.; Crehange, G.; Berthiller, J.; Paparel, P.; Chapet, O. Safety and efficacy of stereotactic ablative radiation therapy for renal cell cancer: 24-month results of the RSR1 phase 1 dose escalation study. Pr. Radiat. Oncol. 2022, 13, e73–e79. [Google Scholar] [CrossRef]
- Hannan, R.; McLaughlin, M.F.; Pop, L.M.; Pedrosa, I.; Kapur, P.; Garant, A.; Ahn, C.; Christie, A.; Zhu, J.; Wang, T.; et al. Phase 2 Trial of Stereotactic Ablative Radiotherapy for Patients with Primary Renal Cancer. Eur. Urol. 2023, 84, 275–286. [Google Scholar] [CrossRef]
- Yim, K.; Hsu, S.-H.; Nolazco, J.I.; Cagney, D.; Mak, R.H.; D’Andrea, V.; Singer, L.; Williams, C.; Huynh, E.; Han, Z.; et al. Stereotactic Magnetic Resonance–guided Adaptive Radiation Therapy for Localized Kidney Cancer: Early Outcomes from a Prospective Phase 1 Trial and Supplemental Cohort. Eur. Urol. Oncol. 2024, 7, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Gaudreault, M.; Hardcastle, N.; Jackson, P.; McIntosh, L.; Higgs, B.; Pryor, D.; Sidhom, M.; Dykyj, R.; Moore, A.; Kron, T.; et al. Dose-effect Relationship of Kidney Function After Stereotactic Ablative Body Radiotherapy for Primary Renal Cell Carcinoma: Trog 15.03 Fastrack Ii. Int. J. Radiat. Oncol. Biol. Phys. 2024; in press. [Google Scholar] [CrossRef]
- The Royal College of Radiologist. Clinical Oncology Radiotherapy Dose Fractionation Fourth Edition. 2024. Available online: https://www.rcr.ac.uk/our-services/all-our-publications/clinical-oncology-publications/radiotherapy-dose-fractionation-fourth-edition/ (accessed on 4 March 2024).
- Funayama, S.; Onishi, H.; Kuriyama, K.; Komiyama, T.; Marino, K.; Araya, M.; Saito, R.; Aoki, S.; Maehata, Y.; Nonaka, H.; et al. Renal cancer is not radioresistant: Slowly but continuing shrinkage of the tumor after stereotactic body radiation therapy. Technol. Cancer Res. Treat. 2019, 18, 1533033818822329. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Alvarado, O.; Anderson, J.K. The role of radiologic imaging and biopsy in renal tumor ablation. World J. Urol. 2010, 28, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Siva, S.; Callahan, J.; Pryor, D.; Martin, J.; Lawrentschuk, N.; Hofman, M.S. Utility of 68Ga prostate specific membrane antigen—Positron emission tomography in diagnosis and response assessment of recurrent renal cell carcinoma. J. Med. Imaging Radiat. Oncol. 2017, 61, 372–378. [Google Scholar] [CrossRef]
- Siva, S.; Ellis, R.J.; Ponsky, L.; Teh, B.S.; Mahadevan, A.; Muacevic, A.; Staehler, M.; Onishi, H.; Wersall, P.; Nomiya, T.; et al. Consensus Statement from the International Radiosurgery Oncology Consortium for Kidney for Primary Renal Cell Carcinoma. Future Oncol. 2016, 12, 637–645. [Google Scholar] [CrossRef]
- Motzer, R.J.; Jonasch, E.; Agarwal, N.; Alva, A.; Bagshaw, H.; Baine, M.; Beckermann, K.; Carlo, M.I.; Choueiri, T.K.; Costello, B.A.; et al. NCCN Guidelines Version 2.2024 Kidney Cancer Continue NCCN Guidelines. J. Natl. Compr. Cancer Netw. 2024, 22, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Ferriero, M.; Cacciatore, L.; Ochoa, M.; Mastroianni, R.; Tuderti, G.; Costantini, M.; Anceschi, U.; Misuraca, L.; Brassetti, A.; Guaglianone, S.; et al. The Impact of Metastasectomy on Survival Outcomes of Renal Cell Carcinoma: A 10-Year Single Center Experience. Cancers 2023, 15, 3332. [Google Scholar] [CrossRef] [PubMed]
- Phillips, R.; Shi, W.Y.; Deek, M.; Radwan, N.; Lim, S.J.; Antonarakis, E.S.; Rowe, S.P.; Ross, A.E.; Gorin, M.A.; Deville, C.; et al. Outcomes of observation vs stereotactic ablative radiation for oligometastatic prostate cancer: The ORIOLE phase 2 randomized clinical trial. JAMA Oncol. 2020, 6, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic ablative radiotherapy for the comprehensive treatment of oligometastatic cancers: Long-Term Results of the SABR-COMET phase II randomized trial. J. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef]
- Le Guevelou, J.; Sargos, P.; Siva, S.; Ploussard, G.; Ost, P.; Gillessen, S.; Zilli, T. The Emerging Role of Extracranial Stereotactic Ablative Radiotherapy for Metastatic Renal Cell Carcinoma: A Systematic Review. Eur. Urol. Focus 2022, 9, 114–124. [Google Scholar] [CrossRef]
- Formenti, S.C.; Rudqvist, N.P.; Golden, E.; Cooper, B.; Wennerberg, E.; Lhuillier, C.; Vanpouille-Box, C.; Friedman, K.; Ferrari de Andrade, L.; Wucherpfennig, K.W.; et al. Radiotherapy induces responses of lung cancer to CTLA-4 blockade. Nat. Med. 2018, 24, 1845–1851. [Google Scholar] [CrossRef]
- Zaorsky, N.G.; Lehrer, E.J.; Kothari, G.; Louie, A.V.; Siva, S. Stereotactic ablative radiation therapy for oligometastatic renal cell carcinoma (SABR ORCA): A meta-analysis of 28 studies. Eur. Urol. Oncol. 2019, 2, 515–523. [Google Scholar] [CrossRef]
- Marvaso, G.; Jereczek-Fossa, B.A.; Zaffaroni, M.; Vincini, M.G.; Corrao, G.; Andratschke, N.; Balagamwala, E.H.; Bedke, J.; Blanck, O.; Capitanio, U.; et al. Policy Review Delphi consensus on stereotactic ablative radiotherapy for oligometastatic and oligoprogressive renal cell carcinoma-a European Society for Radiotherapy and Oncology study endorsed by the European Association of Urology. Lancet Oncol. 2024, 25, e193–e204. [Google Scholar] [CrossRef]
- Dovedi, S.J.; Adlard, A.L.; Lipowska-Bhalla, G.; McKenna, C.; Jones, S.; Cheadle, E.J.; Stratford, I.J.; Poon, E.; Morrow, M.; Stewart, R.; et al. Acquired resistance to fractionated radiotherapy can be overcome by concurrent PD-L1 blockade. Cancer Res. 2014, 74, 5458–5468. [Google Scholar] [CrossRef]
- Hammers, H.J.; Vonmerveldt, D.; Ahn, C.; Nadal, R.M.; Drake, C.G.; Folkert, M.R.; Laine, A.M.; Courtney, K.D.; Brugarolas, J.; Song, D.Y.; et al. Combination of dual immune checkpoint inhibition (ICI) with stereotactic radiation (SBRT) in metastatic renal cell carcinoma (mRCC) (RADVAX RCC). J. Clin. Oncol. 2020, 38, 614. [Google Scholar] [CrossRef]
- Margulis, V.; Freifeld, Y.; Pop, L.M.; Manna, S.; Kapur, P.; Pedrosa, I.; Christie, A.; Mohamad, O.; Mannala, S.; Singla, N.; et al. Neoadjuvant SABR for Renal Cell Carcinoma Inferior Vena Cava Tumor Thrombus—Safety Lead-in Results of a Phase 2 Trial. Int. J. Radiat. Oncol. 2021, 110, 1135–1142. [Google Scholar] [CrossRef]
- Siva, S.; Bressel, M.; Wood, S.T.; Shaw, M.G.; Loi, S.; Sandhu, S.K.; Tran, B.; Azad, A.A.; Lewin, J.H.; Cuff, K.E.; et al. Stereotactic Radiotherapy and Short-course Pembrolizumab for Oligometastatic Renal Cell Carcinoma—The RAPPORT Trial. Eur. Urol. 2021, 81, 364–372. [Google Scholar] [CrossRef]
- Cheung, P.; Patel, S.; North, S.A.; Sahgal, A.; Chu, W.; Soliman, H.; Ahmad, B.; Winquist, E.; Niazi, T.; Patenaude, F.; et al. Stereotactic radiotherapy for oligoprogression in metastatic renal cell cancer patients receiving tyrosine kinase inhibitor therapy: A phase 2 prospective multicenter study. Eur. Urol. 2021, 80, 693–700. [Google Scholar] [CrossRef]
- Hannan, R.; Christensen, M.; Hammers, H.; Christie, A.; Paulman, B.; Lin, D.; Garant, A.; Arafat, W.; Courtney, K.; Bowman, I.; et al. Phase II trial of stereotactic ablative radiation for oligoprogressive metastatic kidney cancer. Eur. Urol. Oncol. 2022, 5, 216–224. [Google Scholar] [CrossRef]
- Hannan, R.; Christensen, M.; Christie, A.; Garant, A.; Pedrosa, I.; Robles, L.; Mannala, S.; Wang, C.; Hammers, H.; Arafat, W.; et al. Stereotactic Ablative Radiation for Systemic Therapy–naïve Oligometastatic Kidney Cancer. Eur. Urol. Oncol. 2022, 5, 695–703. [Google Scholar] [CrossRef]
- Tang, C.; Msaouel, P.; Hara, K.; Choi, H.; Le, V.; Shah, A.Y.; Wang, J.; Jonasch, E.; Choi, S.; Nguyen, Q.-N.; et al. Definitive radiotherapy in lieu of systemic therapy for oligometastatic renal cell carcinoma: A single-arm, single-centre, feasibility, phase 2 trial. Lancet Oncol. 2021, 22, 1732–1739. [Google Scholar] [CrossRef]
- Fife, K.; Bang, A. Combined radiotherapy and new systemic therapies—Have we moved beyond palliation? Clin. Oncol. 2020, 32, 758–765. [Google Scholar] [CrossRef]
- Buti, S.; Bersanelli, M.; Viansone, A.; Leonetti, A.; Masini, C.; Ratta, R.; Procopio, G.; Maines, F.; Iacovelli, R.; Ciccarese, C.; et al. Treatment Outcome of metastatic lesions from renal cell carcinoma underGoing Extra-cranial stereotactic body radioTHERapy: The together retrospective study. Cancer Treat. Res. Commun. 2019, 22, 100161. [Google Scholar] [CrossRef]
- Kroeze, S.G.C.; Pavic, M.; Stellamans, K.; Lievens, Y.; Becherini, C.; Scorsetti, M.; Alongi, F.; Ricardi, U.; Jereczek-Fossa, B.A.; Westhoff, P.; et al. Metastases-directed stereotactic body radiotherapy in combination with targeted therapy or immunotherapy: Systematic review and consensus recommendations by the EORTC–ESTRO OligoCare consortium. Lancet Oncol. 2023, 24, e121–e132. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, X.; Ma, H.; Tian, L.; Mai, L.; Long, W.; Zhang, Z.; Han, H.; Zhou, F.; Dong, P.; et al. Locoregional recurrence after nephrectomy for localized renal cell carcinoma: Feasibility and outcomes of different treatment modalities. Cancer Med. 2022, 11, 4430–4439. [Google Scholar] [CrossRef]
- Du, Y.; Grüllich, C.; Hadaschik, B.; Hatiboglu, G.; Hohenfellner, M.; Pahernik, S. Local Recurrence After Curative Surgical Treatment of Renal Cell Cancer: A Study of 91 Patients. Clin. Genitourin. Cancer 2016, 14, e379–e385. [Google Scholar] [CrossRef]
- Master, V.A.; Gottschalk, A.R.; Kane, C.; Carroll, P.R. Management of Isolated Renal Fossa Recurrence Following Radical Nephrectomy. J. Urol. 2005, 174, 473–477. [Google Scholar] [CrossRef]
- Paly, J.J.; Hallemeier, C.L.; Biggs, P.J.; Niemierko, A.; Roeder, F.; Martínez-Monge, R.; Whitson, J.; Calvo, F.A.; Fastner, G.; Sedlmayer, F.; et al. Outcomes in a Multi-institutional Cohort of Patients Treated With Intraoperative Radiation Therapy for Advanced or Recurrent Renal Cell Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 618–623. [Google Scholar] [CrossRef]
- Habl, G.; Uhl, M.; Hensley, F.; Pahernik, S.; Debus, J.; Röder, F. Intraoperative electron radiation therapy (IOERT) in patients with locally recurrent renal cell carcinoma. Radiat. Oncol. 2013, 8, 282. [Google Scholar] [CrossRef][Green Version]
- Hallemeier, C.L.; Choo, R.; Davis, B.J.; Pisansky, T.M.; Gunderson, L.L.; Leibovich, B.C.; Haddock, M.G. Long-Term Outcomes After Maximal Surgical Resection and Intraoperative Electron Radiotherapy for Locoregionally Recurrent or Locoregionally Advanced Primary Renal Cell Carcinoma. Int. J. Radiat. Oncol. 2012, 82, 1938–1943. [Google Scholar] [CrossRef]
- Calvo, F.; Sole, C.; Martínez-Monge, R.; Azinovic, I.; Aristu, J.; Zudaire, J.; García-Sabrido, J.; Berián, J. Intraoperative EBRT and resection for renal cell carcinoma. Strahlenther. Und Onkol. 2012, 189, 129–136. [Google Scholar] [CrossRef]
- Escudier, B.; Porta, C.; Schmidinger, M.; Rioux-Leclercq, N.; Bex, A.; Khoo, V.; Grünwald, V.; Gillessen, S.; Horwich, A. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 706–720. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bedke, J.; Capitanio, U.; Dabestani, S.; Fernández-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. Eur. Urol. 2022, 82, 399–410. [Google Scholar] [CrossRef]
- Méjean, A.; Ravaud, A.; Thezenas, S.; Colas, S.; Beauval, J.-B.; Bensalah, K.; Geoffrois, L.; Thiery-Vuillemin, A.; Cormier, L.; Lang, H.; et al. Sunitinib Alone or after Nephrectomy in Metastatic Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 379, 417–427. [Google Scholar] [CrossRef]
- Bex, A.; Mulders, P.; Jewett, M.; Wagstaff, J.; Van Thienen, J.V.; Blank, C.U.; Van Velthoven, R.; Del Pilar Laguna, M.; Wood, L.; Van Melick, H.H.E.; et al. Comparison of Immediate vs Deferred Cytoreductive Nephrectomy in Patients With Synchronous Metastatic Renal Cell Carcinoma Receiving Sunitinib: The SURTIME Randomized Clinical Trial. JAMA Oncol. 2019, 5, 164–170. [Google Scholar] [CrossRef]
- Rudra, S.; Fischer-Valuck, B.; Pachynski, R.; Daly, M.; Green, O. Magnetic Resonance Image Guided Stereotactic Body Radiation Therapy to the Primary Renal Mass in Metastatic Renal Cell Carcinoma. Adv. Radiat. Oncol. 2019, 4, 566–570. [Google Scholar] [CrossRef]
- Singh, A.K.; Winslow, T.B.; Kermany, M.H.; Goritz, V.; Heit, L.; Miller, A.; Hoffend, N.C.; Stein, L.C.; Kumaraswamy, L.K.; Warren, G.W.; et al. A Pilot Study of Stereotactic Body Radiation Therapy Combined with Cytoreductive Nephrectomy for Metastatic Renal Cell Carcinoma. Clin. Cancer Res. 2017, 23, 5055–5065. [Google Scholar] [CrossRef]
- Hall, W.A.; Karrison, T.; McGregor, B.A.; Barata, P.C.; Nagar, H.; Tang, C.; Siva, S.; Morgan, T.M.; Lang, J.M.; Kamran, S.C.; et al. NRG-GU012: Randomized phase II stereotactic ablative radiation therapy (SABR) for patients with metastatic unresected renal cell carcinoma (RCC) receiving immunotherapy (SAMURAI). J. Clin. Oncol. 2023, 41, TPS4604. [Google Scholar] [CrossRef]
- Lalani, A.-K.A.; Swaminath, A.; Pond, G.R.; Kapoor, A.; Chu, W.; Bramson, J.L.; Surette, M.G.; Levine, M.N.; Hotte, S.J. Phase II trial of cytoreductive stereotactic hypofractionated radiotherapy with combination ipilimumab/nivolumab for metastatic kidney cancer (CYTOSHRINK). J. Clin. Oncol. 2020, 38, TPS761. [Google Scholar] [CrossRef]
- ECOG-ACRIN Cancer Research Group. Phase III Randomized Trial of Stereotactic Ablative Radiotherapy (SAbR) for Oligometastatic Advanced Renal Carcinoma (SOAR). J. Clin. Oncol. 2024, 42. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).