

Atezolizumab and Bevacizumab Combination Therapy in the Treatment of Advanced Hepatocellular Cancer

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Search Methodology
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smith, R.A.; Andrews, K.S.; Brooks, D.; Fedewa, S.A.; Manassaram-Baptiste, D.; Saslow, D.; Wender, R.C. Cancer screening in the United States, 2019: A review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J. Clin. 2019, 69, 184–210. [Google Scholar] [CrossRef] [PubMed]
- Guevara, M.; Molinuevo, A.; Salmerón, D.; Marcos-Gragera, R.; Carulla, M.; Chirlaque, M.D.; Rodríguez Camblor, M.; Alemán, A.; Rojas, D.; Vizcaíno Batllés, A.; et al. Cancer survival in adults in Spain: A population-based study of the spanish network of cancer registries (REDECAN). Cancers 2022, 14, 2441. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, S.C.; Bernal, W.; Dasarathy, S.; Merli, M.; Plank, L.D.; Schütz, T.; Plauth, M.; Burgos Peláez, R.; Rivera Irigoin, R. Guía Práctica ESPEN: Nutrición clínica en las enfermedades del hígado [ESPEN Practical Guideline: Clinical nutrition in liver disease]. Nutr. Hosp. 2022, 39, 434–472. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Heckley, G.A.; Jarl, J.; Asamoah, B.O.; G-Gerdtham, U. How the risk of liver cancer changes after alcohol cessation: A review and meta-analysis of the current 59 literature. BMC Cancer 2011, 11, 446. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Ávila, M.A.; Ayuso, C.; Mínguez, B.; Varela, M.; Bilbao, I.; Bilba, J.I.; Burrel, M.; Bustamante, J.; et al. Diagnosis and treatment of hepatocellular carcinoma. Update of the consensus document of the AEEH, AEC, SEOM, SERAM, SERVEI, and SETH. Med. Clin. 2021, 156, 463.e1–463.e30, (In Spanish with English abstract). [Google Scholar] [CrossRef]
- Miyata, T.; Nagy, L.E. Programmed cell death in alcohol-associated liver disease. Clin. Mol. Hepatol. 2020, 26, 618–625. [Google Scholar] [CrossRef]
- Forner, A.; Vilana, R.; Bianchi, L.; Rodríguez-Lope, C.; Reig, M.; García-Criado, M.A.; Rimola, J.; Solé, M.; Ayuso, C.; Bru, C.; et al. Lack of arterial hypervascularity at contrast-enhanced ultrasound should not define the priority for diagnostic work-up of nodules. J. Hepatol. 2015, 62, 150–155. [Google Scholar] [CrossRef]
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef]
- Regimbeau, J.M.; Colombat, M.; Mognol, P.; Durand, F.; Abdalla, E.; Degott, C.; Degos, F.; Farges, O.; Belghiti, J. Obesity and diabetes as a risk factor for hepatocellular carcinoma. Liver Transpl. 2004, 10, S69–S70. [Google Scholar] [CrossRef]
- Bruix, J.; da Fonseca, L.G.; Reig, M. Insights into the success and failure of sys- temic therapy for hepatocellular carcinoma. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 617–630. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Saborowski, A. Current strategies for the treatment of intermediate and advanced hepatocelular carcinoma. Cancer Treat. Rev. 2020, 82, 101946. [Google Scholar] [CrossRef] [PubMed]
- Sangro, B.; Melero, I.; Wadhawan, S.; Finn, R.S.; Abou-Alfa, G.K.; Cheng, A.L.; Yau, T.; Furuse, J.; Won, P.J.; Boyd, Z.; et al. Association of inflammatory biomarkers with clinical outcomes in nivolumabtreated patients with advanced hepatocellular carcinoma. J. Hepatol. 2020, 73, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Gao, Y.; Shen, F. Identification of subtypes of hepatocellular carcinoma and screening of prognostic molecular diagnostic markers based on cell adhesion molecule related genes. Genet. Front. 2022, 13, 1042540. [Google Scholar] [CrossRef] [PubMed]
- Massagué, J. TGFβ signalling in contex. Nat. Rev. Mol. Cell Biol. 2012, 13, 616–630. [Google Scholar] [CrossRef]
- Tzavlaki, K.; Moustakas, A. TGF-β Signaling. Biomolecules 2020, 10, 487. [Google Scholar] [CrossRef]
- Batlle, E.; Massagué, J. Transforming growth factor-β signaling in immunity and cancer. Immunity 2019, 50, 924–940. [Google Scholar] [CrossRef]
- Metelli, A.; Salem, M.; Wallace, C.H.; Wu, B.X.; Li, A.; Li, X.; Li, Z. Immunoregulatory functions and the therapeutic implications of GARP-TGF-β in inflammation and cancer. J. Hematol. Oncol. 2018, 11, 24. [Google Scholar] [CrossRef]
- Dewidar, B.; Meyer, C.; Dooley, S.; Meindl-Beinker, A.N. TGF-β in hepatic stellate cell activation and liver fibrogenesis-updated 2019. Cells 2019, 8, 1419. [Google Scholar] [CrossRef]
- Yamazaki, K.; Masugi, Y.; Sakamoto, M. Molecular pathogenesis of hepatocellular carcinoma: Altering transforming growth factor-β signaling in hepatocarcinogenesis. Dig. Dis. 2011, 29, 284–288. [Google Scholar] [CrossRef]
- Zhang, L.; Ding, J.; Li, H.Y.; Wang, Z.H.; Wu, J. Immunotherapy for advanced hepatocellular carcinoma, where are we? Biochim. Biophys. Acta Rev. Cancer 2020, 1874, 188441. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Brandi, G. Biochemical predictors of response to immune checkpoint inhibitors in unresectable hepatocellular carcinoma. Cancer Treat. Res. Commun. 2021, 27, 100328. [Google Scholar] [CrossRef] [PubMed]
- Pinter, M.; Jain, R.K.; Duda, D.G. The current landscape of immune checkpoint blockade in hepatocellular carcinoma: A Review. JAMA Oncol. 2021, 7, 113–123. [Google Scholar] [CrossRef] [PubMed]
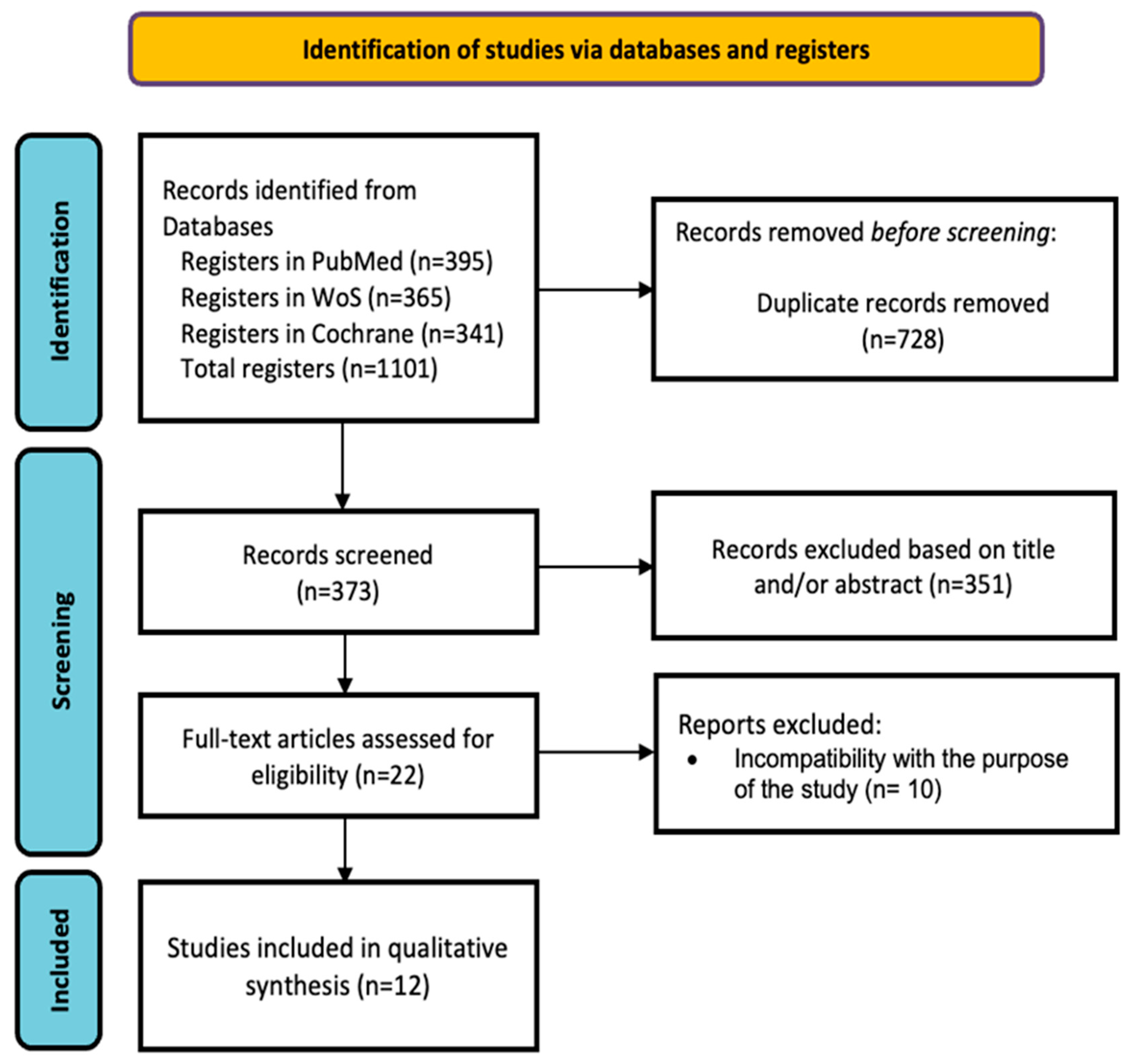
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Barker, T.H.; Stone, J.C.; Sears, K.; Klugar, M.; Tufanaru, C.; Leonardi-Bee, J.; Aromataris, E.; Munn, Z. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evid. Synth. 2023, 21, 494–506. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in unresectable hepatocellular carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Piñero, F.; Silva, M.; Iavarone, M. Sequencing of systemic treatment for hepatocellular carcinoma: Second line competitors. World J. Gastroenterol. 2020, 26, 1888–1900. [Google Scholar] [CrossRef]
- Lee, M.S.; Ryoo, B.Y.; Hsu, C.H.; Numata, K.; Stein, S.; Verret, W.; Hack, S.P.; Spahn, J.; Liu, B.; Abdullah, H.; et al. Atezolizumab with or without bevacizumab in unresectable hepatocellular carcinoma (GO30140): An open-label, multicentre, phase 1b study. Lancet Oncol. 2020, 21, 808–820. [Google Scholar] [CrossRef]
- Sonbol, M.B.; Riaz, I.B.; Naqvi, S.A.A.; Almquist, D.R.; Mina, S.; Almasri, J.; Shah, S.; Almader-Douglas, D.; Uson Junior, P.L.S.; Mahipal, A.; et al. Systemic therapy and sequencing options in advanced hepatocellular carcinoma: A Systematic Review and Network Meta-analysis. JAMA Oncol. 2020, 6, e204930. [Google Scholar] [CrossRef]
- Da Fonseca, L.G. Trial eligibility in advanced hepatocellular carcinoma: Does it support clinical practice in underrepresented subgroups? World J. Gastroenterol. 2021, 27, 3429–3439. [Google Scholar] [CrossRef]
- Han, Y.; Zhi, W.H.; Xu, F.; Zhang, C.B.; Huang, X.Q.; Luo, J.F. Selection of first-line systemic therapies for advanced hepatocellular carcinoma: A network meta-analysis of randomized controlled trials. World J. Gastroenterol. 2021, 27, 2415–2433. [Google Scholar] [CrossRef] [PubMed]
- Fulgenzi, C.A.M.; Talbot, T.; Murray, S.M.; Silletta, M.; Vincenzi, B.; Cortellini, A.; Pinato, D.J. Immunotherapy in hepatocellular carcinoma. Curr. Treat. Options Oncol. 2021, 22, 87. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 2022, 76, 862–873. [Google Scholar] [CrossRef] [PubMed]
- Pinter, M.; Scheiner, B.; Peck-Radosavljevic, M. Immunotherapy for advanced hepatocellular carcinoma: A focus on special subgroups. Gut 2021, 70, 204–214. [Google Scholar] [CrossRef]
- Fulgenzi, C.A.M.; Cheon, J.; D’Alessio, A.; Nishida, N.; Ang, C.; Marron, T.U.; Wu, L.; Saeed, A.; Wietharn, B.; Cammarota, A.; et al. Reproducible safety and efficacy of atezolizumab plus bevacizumab for HCC in clinical practice: Results of the AB-real study. Eur. J. Cancer 2022, 175, 204–213. [Google Scholar] [CrossRef]
- Rimini, M.; Rimassa, L.; Ueshima, K.; Burgio, V.; Shigeo, S.; Tada, T.; Suda, G.; Yoo, C.; Cheon, J.; Pinato, D.J.; et al. Atezolizumab plus bevacizumab versus lenvatinib or sorafenib in non-viral unresectable hepatocellular carcinoma: An international propensity score matching analysis. ESMO Open 2022, 7, 100591. [Google Scholar] [CrossRef]
- Rizzo, A.; Ricci, A.D.; Fanizzi, A.; Massafra, R.; De Luca, R.; Brandi, G. Immune-based combinations versus Sorafenib as first-line treatment for advanced hepatocellular carcinoma: A Meta-Analysis. Curr. Oncol. 2023, 30, 749–757. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Ref. | Year | n | Objective | Conclusions |
|---|---|---|---|---|
| [27] | 2020 | 165 | This article examines the efficacy of the combination of Atezolizumab and Bevacizumab in patients with unresectable HCC. The results suggest that this therapy could be promising, as it showed a positive response rate in patients with advanced HCC. However, associated serious adverse effects, such as gastrointestinal bleeding, arterial hypertension, and proteinuria, which require medical attention, were also highlighted. In addition, prognostic factors, such as TGF-β, AFP, and vascular invasion, were exploited as indicators of HCC progression. | The results showed that, at 12 months, the overall survival rate was 54.6% in the group treated with Sorafenib and 67.2% in the group treated with Atezolizumab and Bevacizumab, suggesting a superior benefit in the second group. However, serious side effects were reported in 38% of patients receiving combination therapy. This highlights the potential efficacy of Atezolizumab and Bevacizumab in the treatment of HCC but also underscores the need to manage the side effects associated with this therapy. |
| [28] | 2020 | 6125 | This article focuses on the sequencing of systemic treatment for HCC and discusses second-line treatment options for patients who have progressed after first-line therapy. Various second-line therapies, including second-line competitors, are discussed, and the importance of the appropriate selection of therapy according to individual patient needs is addressed. The article provides valuable information on the options available for the treatment of advanced stage HCC and highlights the need for personalized attention in therapeutic decision-making. | It is concluded that the combination of the drugs Atezolizumab and Bevacizumab represents an innovative and promising treatment, followed by Lenvatinib, which shows a median survival of 13.6 months in patients with advanced HCC. In addition, predictors of longer survival in patients treated with Sorafenib are identified, including the absence of extrahepatic pathology, the presence of hepatitis C, elevated AFP levels (>200 ng/mL), and the absence of vascular invasion at the macroscopic level. These findings provide useful information for patient stratification and therapeutic decision-making in advanced HCC. |
| [29] | 2020 | 223 | A multicenter phase 1b study evaluated the use of Atezolizumab, alone or in combination with Bevacizumab, in patients with unresectable HCC. The objective was to investigate the safety and efficacy of these therapies. The study was conducted in an open-label manner and revealed valuable information on the potential of these treatment options in patients with unresectable HCC. | Two groups of patients with unresectable HCC were evaluated. Group A (104 patients) received treatment with Atezolizumab and Bevacizumab, and Group F (119 patients) was treated with Atezolizumab alone. Group A had a mean follow-up of 12.4 months, and 36% of patients had a satisfactory response to treatment. In Group F, with a mean follow-up of 6.6 months, adverse effects such as hypertension were observed in 13% and proteinuria in 7% of the patients who received the combined therapy, compared to hypertension in 5% of the patients treated with Atezolizumab alone. These results highlight the efficacy and adverse effects associated with these therapies in patients with unresectable HCC. |
| [30] | 2020 | 8943 | This article discusses systemic therapy options and sequencing in the treatment of advanced HCC. It reviews the different therapies available for advanced HCC and discusses how to select the appropriate sequence of treatments. Effectiveness, tolerability, and clinical considerations in choosing between therapies are discussed, and the importance of personalized care for each patient with advanced HCC is highlighted. | It was shown that patients with unresectable HCC treated with the combination of Atezolizumab and Bevacizumab (a total of 6290 patients) had better outcomes compared to those treated with first-line drugs such as Sorafenib (a total of 2653 patients). The findings suggest that the combination of Atezolizumab and Bevacizumab may be a more effective treatment option for patients with unresectable HCC compared to conventional first-line therapies. |
| [31] | 2021 | 2198 | This study analyzes the eligibility of underrepresented subgroups in clinical trials for advanced hepatocellular carcinoma. They assess whether current clinical practice is adequate for these subgroups and whether clinical trials sufficiently include them. The objective is to determine whether disparities exist in the representation of these subgroups in clinical research and whether greater attention to the inclusion of these patients in trials is required to ensure that treatments are equitable and effective for all groups of patients with advanced hepatocellular carcinoma. | It is suggested that the combination of Atezolizumab and Bevacizumab may have a smaller benefit than Sorafenib in cases of HCC of nonviral etiology, with a HR of 0.91 and a 95% CI of 0.51–1.60. In contrast, for hepatitis B virus (HBV)-related cases, the HR was 0.51 (95% CI 0.32–0.81), and for hepatitis C virus (HCV)-related cases, the HR was 0.43 (95% CI 0.22–0.87). Furthermore, the study suggests that factors such as age, cirrhosis, hepatic decompensation, and portal hypertension may influence the prognosis of HCC treatment. These findings highlight the importance of considering the etiology of HCC and other clinical factors when selecting the appropriate therapy for these patients. |
| [32] | 2021 | 10,256 | This meta-analysis focused on the selection of first-line systemic therapies for advanced cancer. The investigators analyzed multiple clinical trials to determine which of the available therapies offer the best results in terms of efficacy and safety. This analysis allows for a comprehensive comparison between the different therapeutic options available and may provide valuable recommendations for the choice of first-line therapy in patients with advanced HCC. | Greater benefits in terms of overall survival were observed with the combination of Atezolizumab and Bevacizumab compared to Lenvatinib and Sorafenib. The group treated with Atezolizumab and Bevacizumab was found to have a significantly lower death rate compared to the other groups. However, the Atezolizumab- and Bevacizumab-treated group experienced a higher incidence of treatment discontinuations due to adverse effects, which included bleeding and other events. These findings suggest that the combination of Atezolizumab and Bevacizumab may offer benefits in terms of survival but with a higher risk of side effects compared to other therapies. |
| [33] | 2021 | 7881 | This article addresses the topic of immunotherapy in HCC. Immunotherapy is a therapeutic approach used to treat HCC, a type of liver cancer. Immunotherapy involves stimulating the patient’s immune system to fight cancer cells. The text provides information on the status of immunotherapy in the treatment of HCC, including different immunological approaches and therapies used. Recent advances in the understanding of how the immune system interacts with liver cancer cells and how more effective treatments can be developed are also discussed. | A clear superiority was found in terms of increased survival compared to Sorafenib. This analysis suggests that treatment alternatives, such as the drug Lenvatinib, may be more effective in this patient population. However, the study also highlighted the lack of existing predictive biomarkers to accurately target HCC therapy. This underscores the need for research and development of biomarkers that can help to personalize the treatment of this disease. |
| [34] | 2022 | 501 | This phase III study provides updated data on the efficacy and safety of the combination of Atezolizumab and Bevacizumab compared to Sorafenib for the treatment of unresectable hepatocellular carcinoma. The results indicate that this combination continues to show significant benefits in terms of efficacy compared to Sorafenib and remains a promising option for the treatment of this disease. In addition, it is noted that the safety of this therapy has also been supported by updated data from the IMBrave150 study. | The combination of Atezolizumab and Bevacizumab was confirmed to provide longer overall survival (19.2 months vs. 13.4 months) and longer progression-free survival (6.9 months vs. 4.3 months) compared to Sorafenib in patients with unresectable hepatocellular carcinoma. Sorafenib has been the standard treatment to date. Grade 3 adverse effects, such as gastrointestinal bleeding and gastric ulcer perforation, were observed in 43% of patients treated with Atezolizumab and Bevacizumab. However, these effects were considered manageable, and clinically significant survival benefits were obtained with an acceptable safety profile. In addition, a biomarker analysis was performed that revealed a high expression of VEGF receptor 2 was associated with an increased benefit of Atezolizumab and Bevacizumab therapy. These findings support the efficacy of this combination and the importance of identifying biomarkers for patient selection. |
| [35] | 2021 | 1657 | This article focuses on the use of immunotherapy as a treatment for advanced HCC, with a specific focus on special subgroups of patients. It explores how immunotherapy has emerged as a promising option in the treatment of HCC and highlights the importance of considering the specific characteristics of patient subgroups, such as those with viral infections or certain comorbidities. Advances and challenges in the use of immunotherapy in these special subgroups are discussed, and the need for personalized care in the management of advanced HCC is highlighted. | This study evaluated the combination therapy of Atezolizumab and Bevacizumab in patients with HCC and found a significant increase in the overall survival of these patients. However, adverse effects were also identified, such as upper gastrointestinal bleeding, arterial hypertension, and proteinuria, which led to the suggestion that this therapy should be contraindicated in patients with HCC who have previously received an organ transplant. In addition, it was noted that the presence of elevated VEGF levels could potentiate the first-line systemic treatment of HCC and was considered a relevant prognostic factor in the response to therapy. |
| [36] | 2022 | 296 | The AB- real study has provided strong evidence of reproducible safety and efficacy of the combination of Atezolizumab and Bevacizumab in the treatment of HCC in clinical practice. These results support the usefulness of this therapy in a real clinical setting, highlighting its safety profile and demonstrated efficacy in HCC patients. | The median duration of treatment was 7.3 months, while the median overall survival reached 15.7 months. It was reported that 74.6% of patients experienced therapy-related adverse effects, among which bleeding was reported in 8.4%, proteinuria in 30.4%, and hypertension in 28.3%. A significant finding of the study was that those patients who achieved a radiologically appreciable response experienced greater survival. These results suggest that the combination of Atezolizumab and Bevacizumab may be effective in patients with HCC of viral etiology, with improved survival in those who respond positively to treatment. |
| [37] | 2022 | 779 | This international study evaluated the efficacy of the combination of Atezolizumab and Bevacizumab compared to Lenvatinib or Sorafenib in the treatment of unresectable nonviral HCC. A propensity score-matched method was used to match groups of patients with similar characteristics. The results of this analysis suggest that Atezolizumab plus Bevacizumab therapy may be a promising option in the treatment of unresectable nonviral HCC, providing valuable information for clinical decision-making in patients with this disease. | The study found that patients treated with Lenvatinib showed a superior overall survival rate compared to those treated with Atezolizumab and Bevacizumab. However, no statistically significant differences were observed between the Atezolizumab- and Bevacizumab-treated group and the Sorafenib-treated group in terms of overall survival. These findings suggest that Lenvatinib may be more effective than the combination of Atezolizumab and Bevacizumab in the treatment of advanced HCC of nonviral etiology, while the efficacy of Atezolizumab and Bevacizumab is like that of Sorafenib in this context. |
| [38] | 2023 | 1334 | In this meta-analysis, immunological combinations were evaluated in comparison with Sorafenib as the first-line treatment for patients with advanced hepatocellular carcinoma. The results of the analysis suggest that immunologic combinations may be a promising option in terms of efficacy for the initial treatment of this disease. This study provides valuable information on the alternative therapies available for advanced hepatocellular carcinoma and may be relevant for clinical decision-making in this setting. | Alternative treatments (n = 1334) were found to reduce the risk of death by 27% (HR, 0.73; 95% CI, 0.65–0.83; p < 0.001), in addition to increasing both the overall survival and complete response rate compared to Sorafenib (HR, 0.64; 95% CI, 0.5–0.84; p < 0.001) and (12.4; 95% CI, 3.02–50.85; p < 0.001) respectively. These findings suggest that immune combinations may be more effective in terms of survival and complete response in patients with advanced hepatocellular carcinoma compared to Sorafenib. |
| Study | Was True Randomization Used for Assignment of Participants to Treatment Groups? | Was Allocation to Treatment Groups Concealed? | Were Treatment Groups Similar at the Baseline? | Were Participants Blind to Treatment Assignment? | Were Those Delivering Treatment Blind to Treatment Assignment? | Were Outcomes Assessors Blind to Treatment Assignment? | Were Treatment Groups Treated Identically Other Than the Intervention of Interest? | Was Follow-up Complete, and If Not, Were Differences between Groups in Terms of Their Follow-up Adequately Described and Analyzed? | Were Participants Analyzed in the Groups to Which They Were Randomized? | Were Outcomes Measured in the Same Way for Treatment Groups? | Were Outcomes Measured in a Reliable Way? | Was Appropriate Statistical Analysis Used? | Was the Trial Design Appropriate, and Any Deviations from the Standard RCT Design (Individual Randomization, Parallel Groups) Accounted for in the Conduct and Analysis of the Trial? | Score out of 13 (100%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Finn et al., 2020 [27] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Piñero et al., 2020 [28] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Lee et al., 2020 [29] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Sonbol et al., 2020 [30] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Da Fonseca et al., 2021 [31] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Han et al., 2021 [32] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Fulgenzi et al., 2021 [33] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Cheng et al., 2022 [34] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Pinter et al., 2021 [35] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Fulgenzi et al., 2022 [36] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Rimini et al., 2022 [37] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Rizzo et al., 2023 [38] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 100% |
| Studio | Monotherapy Group | Hazard Ratio for Overall Survival | p-Value |
|---|---|---|---|
| Finn et al., 2020 [27] | Sorafenib | 0.59; 95% CI, 0.47 to 0.76 | <0.001 |
| Piñero et al., 2020 [28] | Sorafenib | 0.58; 95% CI, 0.42 to 0.79 | <0.001 |
| Lee et al., 2020 [29] | Atezolizumab | 0.55; 80% CI, 0.40 to 0.74 | 0.011 |
| Sonbol et al., 2020 [30] |
Nivolimab Lenvatinib Sorafenib Linifanib Sunitinib | 0.68; 95% CI, 0.48 to 0.98 0.63; 95% CI, 0.44 to 0.89 0.58; 95% CI, 0.42 to 0.80 0.55; 95% CI, 0.39 to 0.78 0.45; 95% CI, 0.32 to 0.63 | NR |
| Han et al., 2021 [32] | Lenvatinib | 0.63; 95% CI, 0.44 to 0.89 | NR |
| Fulgenzi et al., 2021 [33] | Sorafenib | 0.59; 95% CI, 0.40 to 0.76 | <0.001 |
| Cheng et al., 2022 [34] | Sorafenib | 0.58; 95% CI, 0.42 to 0.79 | <0.001 |
| Pinter et al., 2021 [35] | Sorafenib | 0.95; 95% CI, 0.74 to 1.22 | <0.001 |
| Rimini et al., 2022 [37] | Lenvatinib | 0.65; 95% CI, 0.44 to 0.95 | 0.0268 |
| Rizzo et al., 2023 [38] | Sorafenib | 0.73; 95% CI, 0.65 to 0.83 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ventura, I.; Sanchiz, L.; Legidos-García, M.E.; Murillo-Llorente, M.T.; Pérez-Bermejo, M. Atezolizumab and Bevacizumab Combination Therapy in the Treatment of Advanced Hepatocellular Cancer. Cancers 2024, 16, 197. https://doi.org/10.3390/cancers16010197
Ventura I, Sanchiz L, Legidos-García ME, Murillo-Llorente MT, Pérez-Bermejo M. Atezolizumab and Bevacizumab Combination Therapy in the Treatment of Advanced Hepatocellular Cancer. Cancers. 2024; 16(1):197. https://doi.org/10.3390/cancers16010197
Chicago/Turabian StyleVentura, Ignacio, Lorena Sanchiz, María Ester Legidos-García, María Teresa Murillo-Llorente, and Marcelino Pérez-Bermejo. 2024. "Atezolizumab and Bevacizumab Combination Therapy in the Treatment of Advanced Hepatocellular Cancer" Cancers 16, no. 1: 197. https://doi.org/10.3390/cancers16010197
APA StyleVentura, I., Sanchiz, L., Legidos-García, M. E., Murillo-Llorente, M. T., & Pérez-Bermejo, M. (2024). Atezolizumab and Bevacizumab Combination Therapy in the Treatment of Advanced Hepatocellular Cancer. Cancers, 16(1), 197. https://doi.org/10.3390/cancers16010197