
Clinical Outcome of Low-Grade Myofibroblastic Sarcoma in Japan: A Multicenter Study from the Japanese Musculoskeletal Oncology Group

 , ,
, ,  , , ,
, , ,  ,
, 
Abstract
Simple Summary
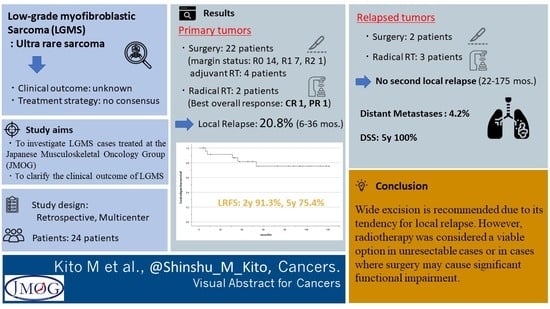
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Evaluation
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Pathological Features
3.3. Treatment and Outcome of Initial Tumor
3.4. Treatment and Outcome of Relapsed Tumor
3.5. Distant Metastases and Disease-Specific Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mentzel, T.; Dry, S.; Katenkamp, D.; Fletcher, C.D. Low-grade myofibroblastic sarcoma: Analysis of 18 cases in the spectrum of myofibroblastic tumors. Am. J. Surg. Pathol. 1998, 22, 1228–1238. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, C.D.M. World Health Organization; International Agency for Research on Cancer. In WHO Classification of Tumours of Soft Tissue and Bone, 4th ed.; IARC Press: Lyon, France, 2013. [Google Scholar]
- Montgomery, E.; Goldblum, J.R.; Fisher, C. Myofibrosarcoma: A clinicopathologic study. Am. J. Surg. Pathol. 2001, 25, 219–228. [Google Scholar] [CrossRef]
- Meng, G.Z.; Zhang, H.Y.; Bu, H.; Zhang, X.L.; Pang, Z.G.; Ke, Q.; Liu, X.; Yang, G. Myofibroblastic sarcomas: A clinicopathological study of 20 cases. Chin. Med. J. 2007, 120, 363–369. [Google Scholar] [CrossRef]
- Kim, J.H.; Choi, W.; Cho, H.S.; Lee, K.S.; Park, J.K.; Kim, B.K. Surgical treatment and long-term outcomes of low-grade myofibroblastic sarcoma: A single-center case series of 15 patients. World J. Surg. Oncol. 2021, 19, 339. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.Y.; Gooi, Z.; Wong, E.W.; Ng, S.K.; Tong, M.C.; Vlantis, A.C. Low-grade myofibroblastic sarcoma: A population-based study. Laryngoscope 2017, 127, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Xu, G.; Wang, X.; Mao, M.; Wu, H.; Baklaushev, V.P.; Chekhonin, V.P.; Peltzer, K.; Wang, G.; Zhang, C. Is there a role for chemotherapy and radiation in the treatment of patients with low-grade myofibroblastic sarcoma? Clin. Transl. Oncol. 2021, 23, 344–352. [Google Scholar] [CrossRef]
- Yonezawa, H.; Yamamoto, N.; Hayashi, K.; Takeuchi, A.; Miwa, S.; Igarashi, K.; Langit, M.B.; Kimura, H.; Shimozaki, S.; Kato, T.; et al. Low-grade myofibroblastic sarcoma of the levator scapulae muscle: A case report and literature review. BMC Musculoskelet. Disord. 2020, 21, 836. [Google Scholar] [CrossRef]
- Takácsi-Nagy, Z.; Muraközy, G.; Pogány, P.; Fodor, J.; Orosz, Z. Myofibroblastic sarcoma of the base of tongue. Case report and review of the literature. Strahlenther. Onkol. 2009, 185, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Tu, Y.; Li, Y.; Xiao, W. Low-grade myofibroblastic sarcoma of the pancreas: A case report and literature review. J. Cancer Res. Ther. 2018, 14 (Suppl. 3), S796–S799. [Google Scholar] [PubMed]
- Morii, T.; Mochizuki, K.; Sano, H.; Fujino, T.; Harasawa, A.; Satomi, K. Occult myofibroblastic sarcoma detected on FDG-PET performed for cancer screening. Ann. Nucl. Med. 2008, 22, 811–815. [Google Scholar] [CrossRef]
- Saito, T.; Mitomi, H.; Kurisaki, A.; Torigoe, T.; Takagi, T.; Suehara, Y.; Okubo, T.; Kaneko, K.; Yao, T. Low-grade myofibroblastic sarcoma of the distal femur. Int. J. Surg. Case Rep. 2013, 4, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Arora, R.; Gupta, R.; Sharma, A.; Dinda, A.K. A rare case of low-grade myofibroblastic sarcoma of the femur in a 38-year-old woman: A case report. J. Med. Case Rep. 2010, 4, 121. [Google Scholar] [CrossRef] [PubMed]
- Khosla, D.; Yadav, B.S.; Kumar, R.; Ghoshal, S.; Vaiphei, K.; Verma, R.; Sharma, S.C. Low-grade myofibroblastic sarcoma of the larynx: A rare entity with review of literature. J. Cancer Res. Ther. 2013, 9, 284–286. [Google Scholar] [PubMed]
- Murakami, Y.; Tsubamoto, H.; Hao, H.; Nishimoto, S.; Shibahara, H. Long-term disease-free survival after radical local excision of low-grade myofibroblastic sarcoma of the vulva. Gynecol. Oncol. Case Rep. 2013, 5, 34–36. [Google Scholar] [CrossRef]
- Humphries, W.E., 3rd; Satyan, K.B.; Relyea, K.; Kim, E.S.; Adesina, A.M.; Chintagumpala, M.; Jea, A. Low-grade myofibroblastic sarcoma of the sacrum. J. Neurosurg. Pediatr. 2010, 6, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Han, S.R.; Yee, G.T. Low Grade Myofibroblastic Sarcoma Occurred in the Scalp. J. Korean Neurosurg. Soc. 2015, 58, 385–388. [Google Scholar] [CrossRef]
- Qiu, J.Y.; Liu, P.; Shi, C.; Han, B. Low-grade myofibroblastic sarcomas of the maxilla. Oncol. Lett. 2015, 9, 619–625. [Google Scholar] [CrossRef]
- Miyazawa, M.; Naritaka, Y.; Miyaki, A.; Asaka, S.; Isohata, N.; Yamaguchi, K.; Murayama, M.; Shimakawa, T.; Katsube, T.; Ogawa, K.; et al. A low-grade myofibroblastic sarcoma in the abdominal cavity. Anticancer Res. 2011, 31, 2989–2994. [Google Scholar]
- Katalinic, D.; Santek, F. Giant low-grade primary myofibroblastic sarcoma of the posterior chest wall. World J. Surg. Oncol. 2017, 15, 96. [Google Scholar] [CrossRef]
- Yamada, T.; Yoshimura, T.; Kitamura, N.; Sasabe, E.; Ohno, S.; Yamamoto, T. Low-grade myofibroblastic sarcoma of the palate. Int. J. Oral Sci. 2012, 4, 170–173. [Google Scholar] [CrossRef]
- Kuo, Y.R.; Yang, C.K.; Chen, A.; Ramachandran, S.; Lin, S.D. Low-Grade Myofibroblastic Sarcoma Arising From Keloid Scar on the Chest Wall After Thoracic Surgery. Ann. Thorac. Surg. 2020, 110, e469–e471. [Google Scholar] [CrossRef]
- Wittekind, C.; Compton, C.C.; Greene, F.L.; Sobin, L.H. TNM residual tumor classification revisited. Cancer 2002, 94, 2511–2516. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Guillou, L.; Coindre, J.M.; Bonichon, F.; Nguyen, B.B.; Terrier, P.; Collin, F.; Vilain, M.O.; Mandard, A.M.; Le Doussal, V.; Leroux, A.; et al. Comparative study of the National Cancer Institute and French Federation of Cancer Centers Sarcoma Group grading systems in a population of 410 adult patients with soft tissue sarcoma. J. Clin. Oncol. 1997, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C. Myofibrosarcoma. Virchows Arch. 2004, 445, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Kusakabe, T.; Hoshi, N.; Saito, A.; Suzuki, T. h-Caldesmon in leiomyosarcoma and tumors with smooth muscle cell-like differentiation: Its specific expression in the smooth muscle cell tumor. Hum. Pathol. 1999, 30, 392–396. [Google Scholar] [CrossRef]
- Fujiwara, T.; Kaneuchi, Y.; Tsuda, Y.; Stevenson, J.; Parry, M.; Jeys, L. Low-grade soft-tissue sarcomas: What is an adequate margin for local disease control? Surg. Oncol. 2020, 35, 303–308. [Google Scholar] [CrossRef]
- Maki, R.G.; Moraco, N.; Antonescu, C.R.; Hameed, M.; Pinkhasik, A.; Singer, S.; Brennan, M.F. Toward better soft tissue sarcoma staging: Building on american joint committee on cancer staging systems versions 6 and 7. Ann. Surg. Oncol. 2013, 20, 3377–3383. [Google Scholar] [CrossRef]
- Yu, Y.; Xiao, J.; Wang, L.; Yang, G. Low-Grade Myofibroblastic Sarcoma in the Mandibular Canal: A Case Report. J. Oral Maxillofac. Surg. 2016, 74, e1501–e1505. [Google Scholar] [CrossRef]
- Yang, J.; Gao, J.; Qiu, X.; Hu, J.; Hu, W.; Wu, X.; Zhang, C.; Ji, T.; Kong, L.; Lu, J.J. Intensity-Modulated Proton and Carbon-Ion Radiation Therapy in the Management of Head and Neck Sarcomas. Cancer Med. 2019, 8, 4574–4586. [Google Scholar] [CrossRef]
- Allignet, B.; Sunyach, M.P.; Geets, X.; Waissi, W. Is there a place for definitive radiotherapy in the treatment of unresectable soft-tissue sarcoma? A systematic review. Acta Oncol. 2022, 61, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Jingu, K.; Tsujii, H.; Mizoe, J.E.; Hasegawa, A.; Bessho, H.; Takagi, R.; Morikawa, T.; Tonogi, M.; Tsuji, H.; Kamada, T.; et al. Carbon ion radiation therapy improves the prognosis of unresectable adult bone and soft-tissue sarcoma of the head and neck. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 2125–2131. [Google Scholar] [CrossRef] [PubMed]
- Musha, A.; Kubo, N.; Kawamura, H.; Okano, N.; Sato, H.; Okada, K.; Osu, N.; Yumisaki, H.; Adachi, A.; Takayasu, Y.; et al. Carbon-ion Radiotherapy for Inoperable Head and Neck Bone and Soft-tissue Sarcoma: Prospective Observational Study. Anticancer Res. 2022, 42, 1439–1446. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Age (y) | Sex | Initial Presentation | Primary Site | Localization | Maximum Diameter (cm) | F/U Periods (m) |
|---|---|---|---|---|---|---|---|
| 1 | 46 | F | Primary | Back | Deep | 2.5 | 113 |
| 2 | 58 | F | Primary | Neck | Deep | 3.5 | 101 |
| 3 | 48 | M | Primary | Abdominal wall | Superficial | 1 | 104 |
| 4 | 64 | M | Primary | Vocal cords | Deep | 1.4 | 34 |
| 5 | 30 | F | Primary | LE (ankle) | Superficial | 1.6 | 83 |
| 6 | 67 | M | Primary | Chest wall | Deep | 3 | 161 |
| 7 | 11 | M | Primary | UE (upper arm) | Superficial | 2.8 | 96 |
| 8 | 19 | F | Primary | LE (thigh) | Superficial | 3.7 | 94 |
| 9 | 12 | M | Primary | LE (foot) | Superficial | 2.8 | 118 |
| 10 | 36 | M | Primary | Back | Deep | 6.1 | 46 |
| 11 | 79 | F | Primary | UE (forearm) | Superficial | 4 | 50 |
| 12 | 27 | F | Relapse | UE (upper arm) | Superficial | 2.5 | 32 |
| 13 | 19 | F | Primary | Groin | Superficial | 3 | 55 |
| 14 | 68 | M | Primary | Buttock | Deep | 6.2 | 38 |
| 15 | 74 | F | Primary | LE (lower leg) | Deep | 9.5 | 54 |
| 16 | 33 | M | Primary | LE (thigh) | Deep | 2.8 | 73 |
| 17 | 26 | F | Primary | Axilla | Deep | 7 | 181 |
| 18 | 86 | F | Primary | LE (thigh) | Deep | 10 | 88 |
| 19 | 76 | F | Primary | Buttock | Superficial | 6.2 | 4 |
| 20 | 83 | F | Primary | Buttock | Superficial | 5.4 | 58 |
| 21 | 38 | F | Primary | Tongue | Superficial | 1.5 | 93 |
| 22 | 47 | M | Primary | Back | Deep | 4 | 11 |
| 23 | 28 | M | Primary | Neck | Deep | 14 | 121 |
| 24 | 22 | F | Primary | Neck | Deep | 7.2 | 75 |
| No. | Treatment | Margin Status | Local Relapse | Metastases | Outcome |
|---|---|---|---|---|---|
| 1 | Wide excision | R0 | - | - | CDF |
| 2 | Wide excision | R0 | - | - | CDF |
| 3 | Intralesional excision | R2 | - | - | AWD |
| 4 | Wide excision | R0 | - | - | CDF |
| 5 | Marginal excision | R1 | - | - | CDF |
| 6 | Wide excision | R0 | + | - | NED |
| 7 | Wide excision | R0 | - | - | CDF |
| 8 | Wide excision | R0 | - | - | CDF |
| 9 | Wide excision | R0 | - | - | CDF |
| 10 | Marginal excision + adjuvant RT (50 Gy) | R1 | - | - | CDF |
| 11 | Wide excision + adjuvant RT (48 Gy) | R1 | - | - | CDF |
| 12 | Wide excision | R1 | - | - | NED |
| 13 | Wide excision | R0 | - | - | CDF |
| 14 | Wide excision | R0 | - | - | CDF |
| 15 | Wide excision + adjuvant RT (60 Gy) | R0 | + | - | AWD |
| 16 | Wide excision | R0 | - | - | CDF |
| 17 | Marginal excision | R1 | + | - | NED |
| 18 | Wide excision + adjuvant RT (66 Gy) | R1 | - | - | CDF |
| 19 | Wide excision | R0 | - | - | CDF |
| 20 | Marginal excision | R1 | + | + | AWD |
| 21 | Wide excision | R0 | - | - | CDF |
| 22 | Wide excision | R0 | - | - | CDF |
| 23 | IMRT (60 Gy) | No surgery | - | - | CDF |
| 24 | IMRT (60 Gy) | No surgery | + | - | AWD |
| Variables | n | 5-Year Survival (%) | p-Value |
|---|---|---|---|
| Age (years) | |||
| 45> | 12 | 83.3 | 0.52 |
| 45≤ | 12 | 63.4 | |
| Sex | |||
| male | 10 | 83.3 | 0.25 |
| female | 14 | 68.4 | |
| Primary site | |||
| trunk | 10 | 57.1 | 0.68 |
| head and neck | 5 | 80 | |
| LE | 6 | 83.3 | |
| UE | 3 | 100 | |
| Localization | |||
| deep | 13 | 63.5 | 0.19 |
| superficial | 11 | 88.9 | |
| Maximum diameter (cm) | |||
| 5> | 15 | 90.9 | <0.01 |
| 5≤ | 9 | 50.0 | |
| Treatment | |||
| surgery | 18 | 79 | 0.58 |
| Surgery + adjuvant RT | 4 | 75 | |
| RT | 2 | 50 | |
| Surgical methods (only surgical cases) | |||
| wide excision | 17 | 84.4 | 0.16 |
| marginal + intra excision | 5 | 60.0 | |
| Margin status (only surgical cases) | |||
| R0 | 14 | 82.1 | 0.49 |
| R1 + R2 | 8 | 72.9 | |
| Ki-67 (%) | |||
| 10> | 12 | 71.4 | 0.78 |
| 10≤ | 12 | 79.5 |
| No. (Refer to Table 1) | Time to Local Relapse (m) | Treatment | Margin Status | Best Overall Response | Re-Local Relapse | F/U Periods after Treatment (m) |
|---|---|---|---|---|---|---|
| 6 | 53 | Surgery | R0 | N/A | - | 108 |
| 15 | 8 | RT (60 Gy) | No surgery | PR | - | 46 |
| 17 | 6 | Carbon ion RT (70.4 Gy) | No surgery | SD | - | 175 |
| 20 | 36 | Surgery | R0 | N/A | - | 22 |
| 24 | 31 | IMRT (60 Gy) | No surgery | PR | - | 43 |
| Authors, Year of Publication | n | Local Relapse | Distant Metastases | ||||
|---|---|---|---|---|---|---|---|
| Simple Excision | Wide Excision | Excision + RT | Excision + Chemotherapy | Radical RT | |||
| Mentzel et al., 1998 [1] | 11 | 28.6% (2/7) | 0% (0/1) | 0% (0/3) | N/A | N/A | 9.1% (1/11) |
| Montgomery et al., 2001 [3] | 13 | 66.7% (6/9) | 50% (1/2) | 0% (0/2) | N/A | N/A | 7.7% (1/13) |
| Meng et al., 2007 [4] | 14 | 12.5% (1/8) | 50% (1/2) | 75% (3/4) | N/A | 0% (0/14) | |
| Kim et al., 2021 [5] | 15 | 100% (2/2) | 0% (0/13) | N/A | N/A | N/A | 0% (0/15) |
| This study | 24 | 50% (2/4) | 7.1% (1/14) | 25% (1/4) | N/A | 50% (1/2) | 4.2% (1/24) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kito, M.; Ae, K.; Okamoto, M.; Endo, M.; Ikuta, K.; Takeuchi, A.; Yasuda, N.; Yasuda, T.; Imura, Y.; Morii, T.; et al. Clinical Outcome of Low-Grade Myofibroblastic Sarcoma in Japan: A Multicenter Study from the Japanese Musculoskeletal Oncology Group. Cancers 2023, 15, 2314. https://doi.org/10.3390/cancers15082314
Kito M, Ae K, Okamoto M, Endo M, Ikuta K, Takeuchi A, Yasuda N, Yasuda T, Imura Y, Morii T, et al. Clinical Outcome of Low-Grade Myofibroblastic Sarcoma in Japan: A Multicenter Study from the Japanese Musculoskeletal Oncology Group. Cancers. 2023; 15(8):2314. https://doi.org/10.3390/cancers15082314
Chicago/Turabian StyleKito, Munehisa, Keisuke Ae, Masanori Okamoto, Makoto Endo, Kunihiro Ikuta, Akihiko Takeuchi, Naohiro Yasuda, Taketoshi Yasuda, Yoshinori Imura, Takeshi Morii, and et al. 2023. "Clinical Outcome of Low-Grade Myofibroblastic Sarcoma in Japan: A Multicenter Study from the Japanese Musculoskeletal Oncology Group" Cancers 15, no. 8: 2314. https://doi.org/10.3390/cancers15082314
APA StyleKito, M., Ae, K., Okamoto, M., Endo, M., Ikuta, K., Takeuchi, A., Yasuda, N., Yasuda, T., Imura, Y., Morii, T., Kikuta, K., Kawamoto, T., Nezu, Y., Baba, I., Ohshika, S., Uehara, T., Ueda, T., Takahashi, J., & Kawano, H. (2023). Clinical Outcome of Low-Grade Myofibroblastic Sarcoma in Japan: A Multicenter Study from the Japanese Musculoskeletal Oncology Group. Cancers, 15(8), 2314. https://doi.org/10.3390/cancers15082314