
Impact of Hormone Replacement Therapy on Risk of Ovarian Cancer in Postmenopausal Women with De Novo Endometriosis or a History of Endometriosis

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
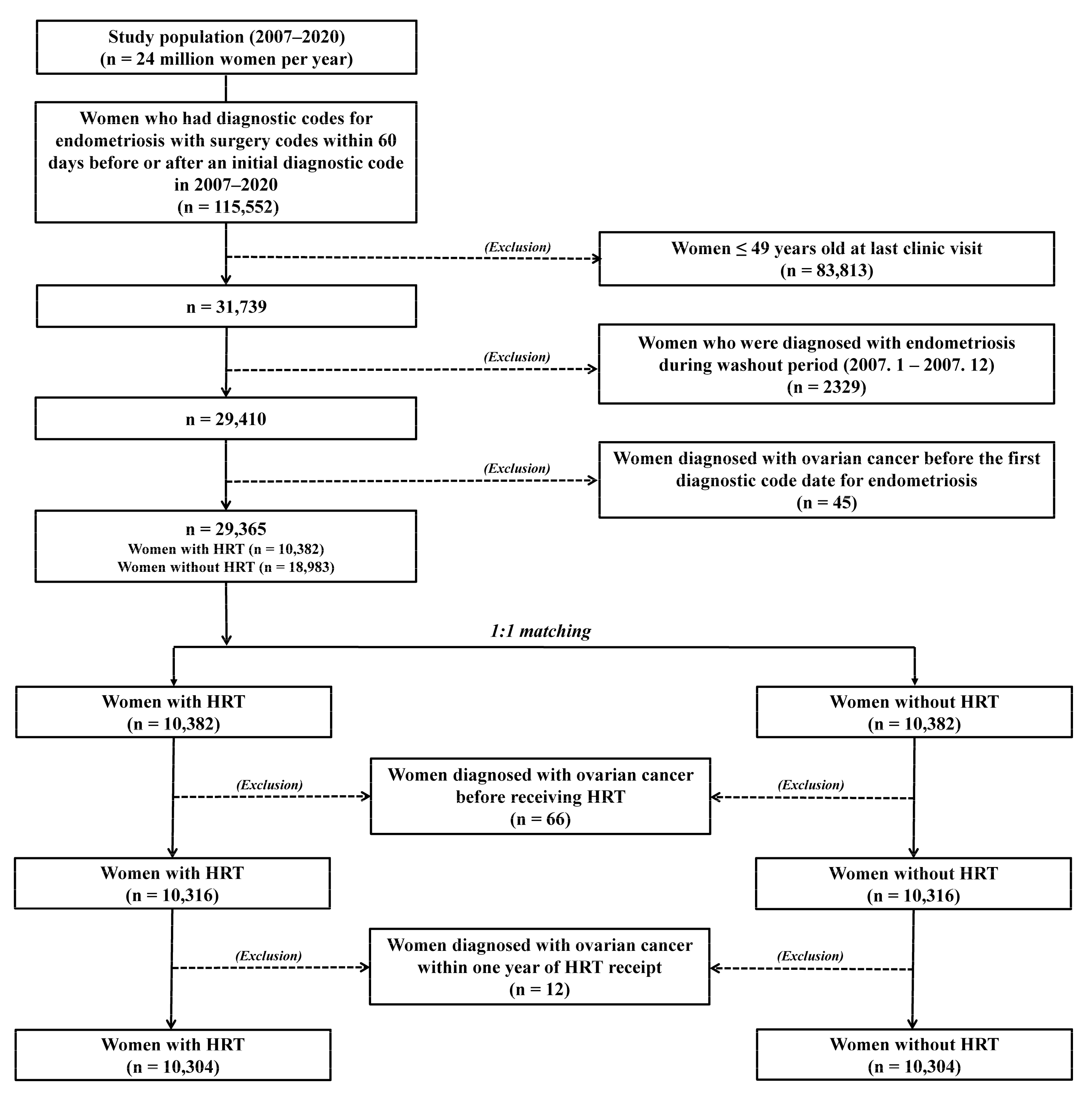
2. Materials and Methods
Statistical Analyses
3. Results
3.1. Characteristics of Women with Endometriosis According to Receipt of HRT
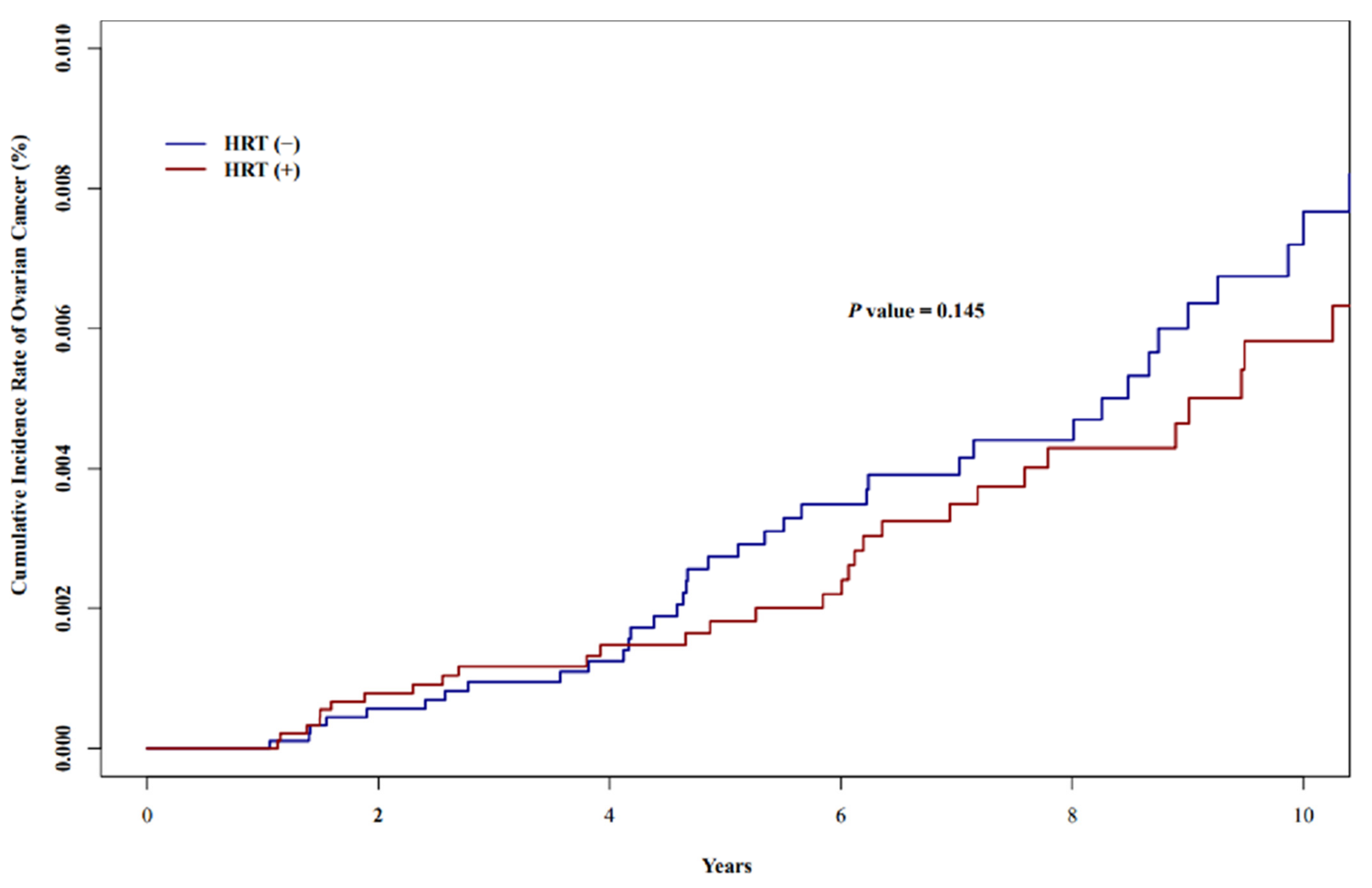
3.2. Incidences and Characteristics of Ovarian Cancer According to Receipt of HRT in Women with Endometriosis
3.3. Risk Factors of Ovarian Cancer According to Receipt of HRT in Women with Endometriosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Gemmell, L.C.; Webster, K.E.; Kirtley, S.; Vincent, K.; Zondervan, K.T.; Becker, C.M. The management of menopause in women with a history of endometriosis: A systematic review. Hum. Reprod. Update 2017, 23, 481–500. [Google Scholar] [CrossRef]
- Giannella, L.; Marconi, C.; Di Giuseppe, J.; Delli Carpini, G.; Fichera, M.; Grelloni, C.; Giuliani, L.; Montanari, M.; Insinga, S.; Ciavattini, A. Malignant Transformation of Postmenopausal Endometriosis: A Systematic Review of the Literature. Cancers 2021, 13, 4026. [Google Scholar] [CrossRef]
- Gadducci, A.; Lanfredini, N.; Tana, R. Novel insights on the malignant transformation of endometriosis into ovarian carcinoma. Gynecol. Endocrinol. 2014, 30, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.T.; Wang, D.B.; Liu, K.R.; Li, Y.; Sun, C.X.; Guo, C.S.; Ren, F. Inducing malignant transformation of endometriosis in rats by long-term sustaining hyperestrogenemia and type II diabetes. Cancer Sci. 2015, 106, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Hickman, T.N.; Namnoum, A.B.; Hinton, E.L.; Zacur, H.A.; Rock, J.A. Timing of estrogen replacement therapy following hysterectomy with oophorectomy for endometriosis. Obstet. Gynecol. 1998, 91, 673–677. [Google Scholar] [CrossRef] [PubMed]
- Morotti, M.; Remorgida, V.; Venturini, P.L.; Ferrero, S. Endometriosis in menopause: A single institution experience. Arch. Gynecol. Obstet. 2012, 286, 1571–1575. [Google Scholar] [CrossRef]
- Pearce, C.L.; Templeman, C.; Rossing, M.A.; Lee, A.; Near, A.M.; Webb, P.M.; Nagle, C.M.; Doherty, J.A.; Cushing-Haugen, K.L.; Wicklund, K.G.; et al. Association between endometriosis and risk of histological subtypes of ovarian cancer: A pooled analysis of case-control studies. Lancet Oncol. 2012, 13, 385–394. [Google Scholar] [CrossRef]
- Mogensen, J.B.; Kjær, S.K.; Mellemkjær, L.; Jensen, A. Endometriosis and risks for ovarian, endometrial and breast cancers: A nationwide cohort study. Gynecol Oncol. 2016, 143, 87–92. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Ji, E.; Kim, K.; Lee, B.; Hwang, S.O.; Lee, H.J.; Lee, K.; Lee, M.; Kim, Y.B. Postoperative Hormone Replacement Therapy and Survival in Women with Ovarian Cancer. Cancers 2022, 14, 3090. [Google Scholar] [CrossRef]
- Beral, V.; Gaitskell, K.; Hermon, C.; Moser, K.; Reeves, G.; Peto, R. Menopausal hormone use and ovarian cancer risk: Individual participant meta-analysis of 52 epidemiological studies. Lancet 2015, 385, 1835–1842. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.W.; Ness, R.B.; Roman, L.D.; Terry, K.L.; Schildkraut, J.M.; Chang-Claude, J.; Doherty, J.A.; Menon, U.; Cramer, D.W.; Gayther, S.A.; et al. Association Between Menopausal Estrogen-Only Therapy and Ovarian Carcinoma Risk. Obstet. Gynecol. 2016, 127, 828–836. [Google Scholar] [CrossRef]
- Zanello, M.; Borghese, G.; Manzara, F.; Degli Esposti, E.; Moro, E.; Raimondo, D.; Abdullahi, L.O.; Arena, A.; Terzano, P.; Meriggiola, M.C.; et al. Hormonal Replacement Therapy in Menopausal Women with History of Endometriosis: A Review of Literature. Medicina 2019, 55, 477. [Google Scholar] [CrossRef] [PubMed]
- Petersen, V.C.; Underwood, J.C.; Wells, M.; Shepherd, N.A. Primary endometrioid adenocarcinoma of the large intestine arising in colorectal endometriosis. Histopathology 2002, 40, 171–176. [Google Scholar] [CrossRef]
- Leiserowitz, G.S.; Gumbs, J.L.; Oi, R.; Dalrymple, J.L.; Smith, L.H.; Ryu, J.; Scudder, S.; Russell, A.H. Endometriosis-related malignancies. Int. J. Gynecol. Cancer 2003, 13, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Soliman, N.F.; Evans, A.J. Malignancy arising in residual endometriosis following hysterectomy and hormone replacement therapy. J. Br. Menopause Soc. 2004, 10, 123–124. [Google Scholar] [CrossRef]
- Karanjgaokar, V.C.; Murphy, D.J.; Samra, J.S.; Mann, C.H. Malignant transformation of residual endometriosis after hysterectomy: A case series. Fertil. Steril. 2009, 92, 2037.e19–2037.e21. [Google Scholar] [CrossRef]
- Matorras, R.; Elorriaga, M.A.; Pijoan, J.I.; Ramón, O.; Rodríguez-Escudero, F.J. Recurrence of endometriosis in women with bilateral adnexectomy (with or without total hysterectomy) who received hormone replacement therapy. Fertil. Steril. 2002, 77, 303–308. [Google Scholar] [CrossRef]
- Al Kadri, H.; Hassan, S.; Al-Fozan, H.M.; Hajeer, A. Hormone therapy for endometriosis and surgical menopause. Cochrane Database Syst. Rev. 2009, CD005997. [Google Scholar] [CrossRef]
- Marjoribanks, J.; Farquhar, C.; Roberts, H.; Lethaby, A.; Lee, J. Long-term hormone therapy for perimenopausal and postmenopausal women. Cochrane Database Syst. Rev. 2017, 1, CD004143. [Google Scholar] [CrossRef]
- Becker, C.M.; Bokor, A.; Heikinheimo, O.; Horne, A.; Jansen, F.; Kiesel, L.; King, K.; Kvaskoff, M.; Nap, A.; Petersen, K.; et al. ESHRE guideline: Endometriosis. Hum. Reprod. Open 2022, 2022, hoac009. [Google Scholar] [CrossRef] [PubMed]
- Zanetta, G.M.; Webb, M.J.; Li, H.; Keeney, G.L. Hyperestrogenism: A relevant risk factor for the development of cancer from endometriosis. Gynecol. Oncol. 2000, 79, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Fedele, L.; Bianchi, S.; Raffaelli, R.; Zanconato, G. Comparison of transdermal estradiol and tibolone for the treatment of oophorectomized women with deep residual endometriosis. Maturitas 1999, 32, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.; Kim, J.A.; Kim, S. A guide for the utilization of Health Insurance Review and Assessment Service National Patient Samples. Epidemiol. Health 2014, 36, e2014008. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing, R Version 3.5.1; R Foundation for Statistical Computing: Vienna, Austria, 2022.
- SAS Institute Inc. SAS 9.4 Software, SAS Institute Inc.: Cary, NC, USA, 2020.
- Kim, Y.T.; Cha, C.; Lee, M.R. Factors related to age at menopause among Korean women: The Korean Longitudinal Survey of Women and Families. Menopause 2019, 26, 492–498. [Google Scholar] [CrossRef]
- Gemmill, J.A.; Stratton, P.; Cleary, S.D.; Ballweg, M.L.; Sinaii, N. Cancers, infections, and endocrine diseases in women with endometriosis. Fertil. Steril. 2010, 94, 1627–1631. [Google Scholar] [CrossRef]
- Collinet, P.; Fritel, X.; Revel-Delhom, C.; Ballester, M.; Bolze, P.A.; Borghese, B.; Bornsztein, N.; Boujenah, J.; Brillac, T.; Chabbert-Buffet, N.; et al. Management of endometriosis: CNGOF/HAS clinical practice guidelines—Short version. J. Gynecol. Obstet. Hum. Reprod. 2018, 47, 265–274. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | HRT (−) | HRT (+) | |||
|---|---|---|---|---|---|
| n = 20,608 (100.0%) | n = 10,304 (50.0%) | n = 10,304 (50.0%) | OR (95% CI) | p Value a | |
| Age at last clinic visit (years) | 55.0 ± 4.6 | 55.0 ± 4.6 | 55.0 ± 4.6 | ||
| SES at last clinic visit | |||||
| Mid- or high-SES | 20,078 (97.4) | 10,067 (97.7) | 10,011 (97.2) | ref | |
| Low SES | 530 (2.6) | 237 (2.3) | 293 (2.8) | 1.243 (1.045–1.479) | 0.014 |
| CCI at last clinic visit | |||||
| 0 | 11,675 (56.7) | 5963 (57.9) | 5712 (55.4) | ref | |
| 1 | 4601 (22.3) | 2258 (21.9) | 2343 (22.7) | 1.083 (1.012–1.160) | 0.022 |
| 2 | 2446 (11.9) | 1168 (11.3) | 1278 (12.4) | 1.142 (1.047–1.246) | 0.003 |
| 3 | 1028 (5.0) | 491 (4.8) | 537 (5.2) | 1.142 (1.005–1.297) | 0.042 |
| Over 4 | 858 (4.2) | 424 (4.1) | 434 (4.2) | 1.069 (0.930–1.228) | 0.349 |
| Age at endometriosis diagnosis (years) | 49.3 ± 5.7 | 49.6 ± 5.7 | 48.9 ± 5.8 | 0.978 (0.973–0.982) | <0.001 |
| Year of endometriosis diagnosis | |||||
| 2008 | 1670 (8.1) | 703 (6.8) | 967 (9.4) | ref | |
| 2009 | 1543 (7.5) | 710 (6.9) | 833 (8.1) | 0.853 (0.742–0.981) | 0.025 |
| 2010 | 1576 (7.7) | 701 (6.8) | 875 (8.5) | 0.907 (0.790–1.043) | 0.171 |
| 2011 | 1369 (6.6) | 630 (6.1) | 739 (7.2) | 0.853 (0.738–0.985) | 0.030 |
| 2012 | 1217 (5.9) | 561 (5.4) | 656 (6.4) | 0.850 (0.733–0.985) | 0.030 |
| 2013 | 1442 (7.0) | 701 (6.8) | 741 (7.2) | 0.769 (0.667–0.886) | 0.001 |
| 2014 | 1725 (8.4) | 835 (8.1) | 890 (8.6) | 0.775 (0.677–0.887) | 0.001 |
| 2015 | 1401 (6.8) | 700 (6.8) | 701 (6.8) | 0.728 (0.631–0.840) | <0.001 |
| 2016 | 1297 (6.3) | 674 (6.5) | 623 (6.1) | 0.672 (0.581–0.778) | <0.001 |
| 2017 | 1931 (9.4) | 1050 (10.2) | 881 (8.6) | 0.610 (0.535–0.696) | <0.001 |
| 2018 | 2244 (10.9) | 1230 (11.9) | 1014 (9.8) | 0.599 (0.527–0.681) | <0.001 |
| 2019 | 1795 (8.7) | 991 (9.6) | 804 (7.8) | 0.590 (0.516–0.675) | <0.001 |
| 2020 | 1398 (6.8) | 818 (7.9) | 580 (5.6) | 0.516 (0.446–0.595) | <0.001 |
| Number of surgeries for endometriosis | |||||
| 1 | 20,050 (97.3) | 10,088 (97.9) | 9962 (96.7) | ref | |
| 2 | 544 (2.6) | 214 (2.1) | 330 (3.2) | 1.562 (1.312–1.859) | <0.001 |
| Over 3 | 14 (0.1) | 2 (0.0) | 12 (0.1) | 6.076 (1.360–27.139) | 0.018 |
| Methods of surgery for endometriosis | |||||
| Fulguration | 655 (3.2) | 311 (3.0) | 344 (3.3) | 1.121 (0.959–1.310) | 0.150 |
| Ovarian cystectomy | 13,302 (64.6) | 6536 (63.4) | 6766 (65.7) | 1.115 (1.058–1.176) | 0.001 |
| BSO or USO | 2839 (13.8) | 1373 (13.3) | 1466 (14.2) | 1.090 (1.008–1.180) | 0.031 |
| Hysterectomy | 5329 (25.9) | 2919 (28.3) | 2410 (23.4) | 0.788 (0.741–0.839) | <0.001 |
| Hysterectomy for disease except ovarian cancer | 5311 (25.8) | 2909 (28.2) | 2402 (23.3) | 0.773 (0.726–0.823) | <0.001 |
| Duration of HRT (years) | 1.4 ± 2.2 | ||||
| Types of HRT medication | |||||
| Combined estrogen and progesterone | 3672 (35.6) | ||||
| Estrogen alone | 4622 (44.9) | ||||
| Tibolone | 5265 (51.1) | ||||
| Time between endometriosis diagnosis and beginning of HRT | |||||
| Rate of HRT use before endometriosis diagnosis | 2680 (26.0) | ||||
| Time of HRT use before endometriosis diagnosis (years) | 0.9 ± 1.9 | ||||
| Time of HRT use after endometriosis diagnosis (years) | 1.8 ± 2.1 | ||||
| Rate of HRT use after endometriosis diagnosis | 7624 (74.0) | ||||
| Time of HRT use after endometriosis diagnosis (years) | 1.3 ± 1.9 |
| Total n = 20,608 (100.0%) | HRT (−) n = 10,304 (50.0%) | HRT (+) n = 10,304 (50.0%) | OR (95% CI) | p Value | Adjusted OR (95% CI) a | p Value a | |
|---|---|---|---|---|---|---|---|
| Ovarian cancer | |||||||
| Negative | 20,529 (99.6) | 10,258 (99.6) | 10,271 (99.7) | ref | 0.145 | ref | 0.283 |
| Positive | 79 (0.4) | 46 (0.5) | 33 (0.3) | 0.717 (0.458–1.121) | 0.780 (0.495–1.146) | ||
| Time between endometriosis diagnosis and ovarian cancer diagnosis (years) | 1.8 ± 2.8 | 1.7 ± 2.7 | 1.9 ± 2.9 | 0.867 | |||
| Time between beginning of HRT and ovarian cancer diagnosis (years) | 5.7 ± 3.4 | ||||||
| Duration of HRT use in women with ovarian cancer (years) | 2.2 ± 2.9 | ||||||
| Age at ovarian cancer diagnosis (years) | 55.8 ± 7.4 | 56.1 ± 7.0 | 55.4 ± 8.1 | 0.663 | |||
| Total | HRT (−) | HRT (+) | ||||
|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Unadjusted HR | ||||||
| Age at endometriosis diagnosis per 5 years (years) | 1.064 (1.037–1.091) | <0.001 | 1.053 (1.016–1.091) | 0.004 | 1.074 (1.034–1.115) | 0.001 |
| Year of endometriosis diagnosis | 1.153 (1.086–1.223) | <0.001 | 1.085 (1.001–1.176) | 0.047 | 1.232 (1.124–1.350) | <0.001 |
| Number of surgeries for endometriosis | 3.816 (1.941–7.500) | 0.001 | 6.116 (2.558–14.624) | <0.001 | 2.599 (0.863–7.829) | 0.070 |
| Hysterectomy for disease except ovarian cancer | 0.289 (0.126–0.667) | 0.004 | 0.106 (0.026–0.442) | 0.002 | 0.791 (0.277–2.264) | 0.662 |
| HRT | 0.718 (0.459–1.123) | 0.147 | ||||
| Duration of HRT per year | 1.026 (0.917–1.149) | 0.651 | ||||
| Types of HRT medication | ||||||
| Combined estrogen and progesterone | 1.044 (0.525–2.077) | 0.902 | ||||
| Estrogen alone | 2.737 (1.272–5.892) | 0.010 | ||||
| Tibolone | 0.766 (0.384–1.528) | 0.449 | ||||
| Adjusted HR a, b | ||||||
| Age at endometriosis diagnosis per 5 years (years) | 1.056 (1.021–1.091) a | 0.001 a | 1.066 (1.022–1.111) b | 0.003 b | 1.025 (0.966–1.087) b | 0.414 b |
| Year of endometriosis diagnosis | 1.273 (1.174–1.380) a | <0.001 a | 1.216 (1.099–1.347) b | 0.001 b | 1.385 (1.210–1.585) b | <0.001 b |
| Number of surgeries for endometriosis | 6.375 (3.186–12.757) a | <0.001 a | 7.605 (3.230–17.905) b | <0.001 b | 5.206 (1.631–16.612) b | 0.005 b |
| Hysterectomy for disease except ovarian cancer | 0.064 (0.027–0.153) a | <0.001 a | 0.031 (0.007–0.137) b | <0.001 b | 0.111 (0.036–0.344) b | 0.001 b |
| HRT | 0.937 (0.592–1.483) a | 0.782 a | ||||
| Duration of HRT per year | 0.974 (0.857–1.107) b | 0.684 b | ||||
| Types of HRT medication | ||||||
| Combined estrogen and progesterone | 1.127 (0.539–2.357) b | 0.751 b | ||||
| Estrogen alone | 2.898 (1.251–6.715) b | 0.013 b | ||||
| Tibolone | 1.057 (0.495–2.257) b | 0.886 b | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.J.; Lee, B.; Choi, H.; Kim, T.; Kim, Y.; Kim, Y.B. Impact of Hormone Replacement Therapy on Risk of Ovarian Cancer in Postmenopausal Women with De Novo Endometriosis or a History of Endometriosis. Cancers 2023, 15, 1708. https://doi.org/10.3390/cancers15061708
Lee HJ, Lee B, Choi H, Kim T, Kim Y, Kim YB. Impact of Hormone Replacement Therapy on Risk of Ovarian Cancer in Postmenopausal Women with De Novo Endometriosis or a History of Endometriosis. Cancers. 2023; 15(6):1708. https://doi.org/10.3390/cancers15061708
Chicago/Turabian StyleLee, Hee Joong, Banghyun Lee, Hangseok Choi, Taehee Kim, Yejeong Kim, and Yong Beom Kim. 2023. "Impact of Hormone Replacement Therapy on Risk of Ovarian Cancer in Postmenopausal Women with De Novo Endometriosis or a History of Endometriosis" Cancers 15, no. 6: 1708. https://doi.org/10.3390/cancers15061708
APA StyleLee, H. J., Lee, B., Choi, H., Kim, T., Kim, Y., & Kim, Y. B. (2023). Impact of Hormone Replacement Therapy on Risk of Ovarian Cancer in Postmenopausal Women with De Novo Endometriosis or a History of Endometriosis. Cancers, 15(6), 1708. https://doi.org/10.3390/cancers15061708