
Evidence for Choosing Qigong as an Integrated Intervention in Cancer Care: An Umbrella Review

 , , , and
, , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
Qigong
2. Materials and Methods
2.1. Umbrella Review Methods
2.2. Inclusion Criteria
2.2.1. Participants
2.2.2. Phenomena of Interest
2.2.3. Types of Studies
2.3. Information Sources, Search Strategy, and Data Extraction
2.4. Assessment of the Methodological Quality of Systematic Reviews
3. Results
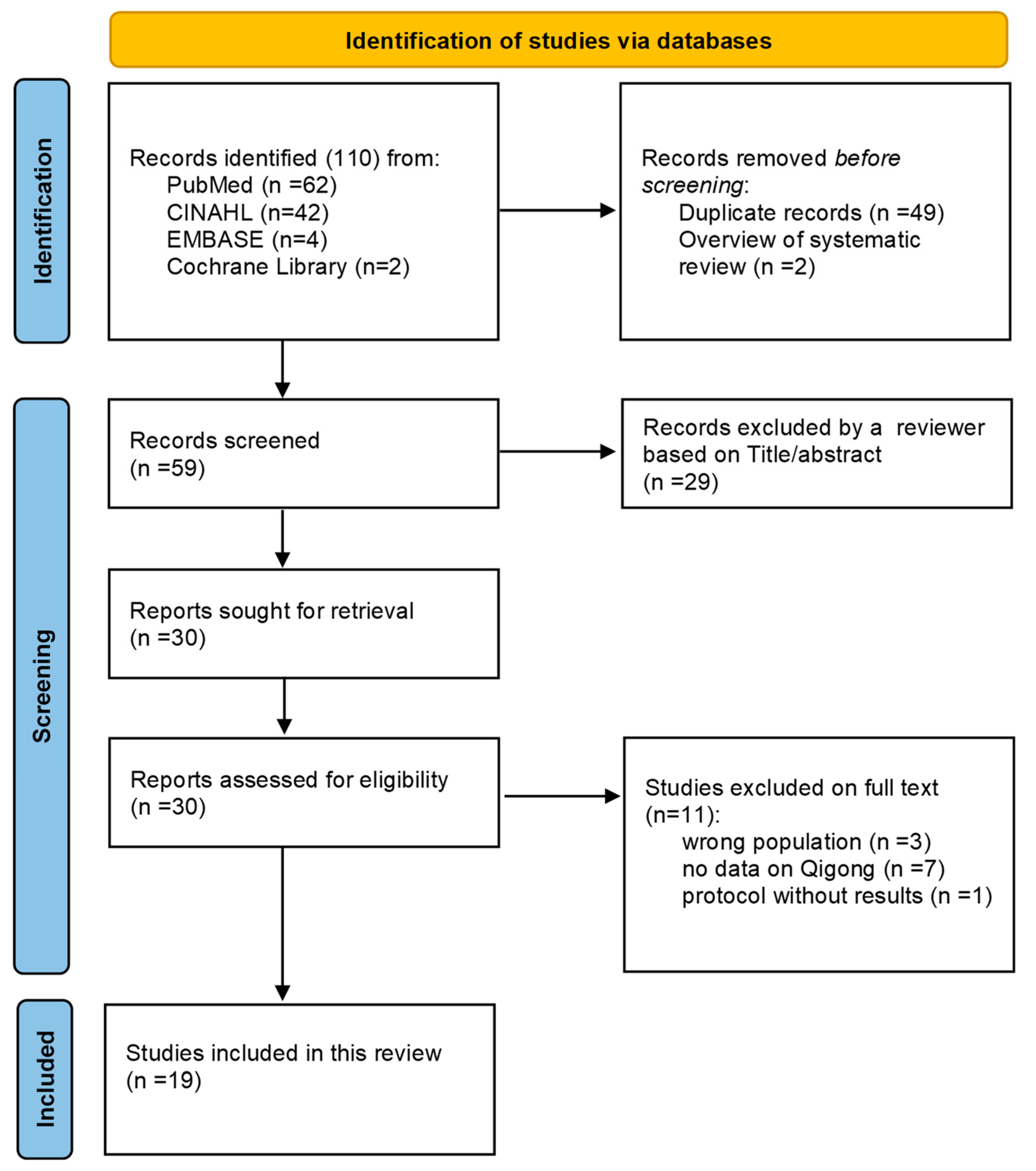
3.1. Search Strategy Outcome
3.2. Qigong Styles
3.3. Methodological Quality
3.4. Outcomes
3.4.1. Quality of Life
3.4.2. Sleep Quality
3.4.3. Cancer-Related Fatigue
3.4.4. Depression
3.4.5. Anxiety
3.4.6. Stress/Distress
3.4.7. Cognitive Impairment
3.4.8. Biological Outcomes
3.4.9. Other Cancer-Related Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 8 January 2023).
- Rahib, L.; Wehner, M.R.; Matrisian, L.M.; Nead, K.T. Estimated Projection of US Cancer Incidence and Death to 2040. JAMA Netw. Open 2021, 4, e214708. [Google Scholar] [CrossRef]
- Scott, A.R.; Stoltzfus, K.C.; Tchelebi, L.T.; Trifiletti, D.M.; Lehrer, E.J.; Rao, P.; Bleyer, A.; Zaorsky, N.G. Trends in Cancer Incidence in US Adolescents and Young Adults, 1973–2015. JAMA Netw. Open 2020, 3, e2027738. [Google Scholar] [CrossRef]
- Wu, S.; Zhu, W.; Thompson, P.; Hannun, Y.A. Evaluating intrinsic and non-intrinsic cancer risk factors. Nat. Commun. 2018, 9, 3490. [Google Scholar] [CrossRef]
- Cole, S.W. The Conserved Transcriptional Response to Adversity. Curr. Opin. Behav. Sci. 2019, 28, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Bottaccioli, A.G.; Bottaccioli, F. PsychoNeuroEndocrineImmunology and the Science of Integrated Care. The Manual; Edra: Pisa, Italy, 2020. [Google Scholar]
- Moraes, L.J.; Miranda, M.B.; Loures, L.F.; Mainieri, A.G.; Mármora, C.H.C. A systematic review of psychoneuroimmunology-based interventions. Psychol. Health Med. 2018, 23, 635–652. [Google Scholar] [CrossRef]
- Liu, T.; Qiang, X.M. Chinese Medical Qigong; Singing Dragon: London, UK, 2013; ISBN 978-1-84819-096-2. [Google Scholar]
- Leung, K.-C.W.; Yang, Y.-J.; Hui, S.S.-C.; Woo, J. Mind-Body Health Benefits of Traditional Chinese Qigong on Women: A Systematic Review of Randomized Controlled Trials. Evid. Based Complement. Altern. Med. ECAM 2021, 2021, 7443498. [Google Scholar] [CrossRef] [PubMed]
- Casuso-Holgado, M.J.; Heredia-Rizo, A.M.; Gonzalez-Garcia, P.; Muñoz-Fernández, M.J.; Martinez-Calderon, J. Mind-body practices for cancer-related symptoms management: An overview of systematic reviews including one hundred twenty-nine meta-analyses. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2022, 30, 10335–10357. [Google Scholar] [CrossRef]
- Amatya, B.; Khan, F.; Lew, T.E.; Dickinson, M. Rehabilitation in patients with lymphoma: An overview of Systematic Reviews. J. Rehabil. Med. 2021, 53, 1–15. [Google Scholar] [CrossRef]
- Chapter 10: Umbrella Reviews-JBI Manual for Evidence Synthesis-JBI Global Wiki. Available online: https://jbi-global-wiki.refined.site/space/MANUAL/4687363/Chapter+10%3A+Umbrella+reviews (accessed on 8 January 2023).
- Klein, P.J.; Schneider, R.; Rhoads, C.J. Qigong in cancer care: A systematic review and construct analysis of effective Qigong therapy. Support. Care Cancer 2016, 24, 3209–3222. [Google Scholar] [CrossRef] [PubMed]
- Henshall, C.L.; Allin, L.; Aveyard, H. A Systematic Review and Narrative Synthesis to Explore the Effectiveness of Exercise-Based Interventions in Improving Fatigue, Dyspnea, and Depression in Lung Cancer Survivors. Cancer Nurs. 2019, 42, 295–306. [Google Scholar] [CrossRef]
- Lee, M.S.; Chen, K.W.; Sancier, K.M.; Ernst, E. Qigong for cancer treatment: A systematic review of controlled clinical trials. Acta Oncol. Stockh. Swed. 2007, 46, 717–722. [Google Scholar] [CrossRef]
- Matthews, E.E.; Janssen, D.W.; Djalilova, D.M.; Berger, A.M. Effects of Exercise on Sleep in Women with Breast Cancer: A Systematic Review. Sleep Med. Clin. 2018, 13, 395–417. [Google Scholar] [CrossRef]
- Van Vu, D.; Molassiotis, A.; Ching, S.S.Y.; Le, T.T. Effects of Qigong on symptom management in cancer patients: A systematic review. Complement. Ther. Clin. Pract. 2017, 29, 111–121. [Google Scholar] [CrossRef]
- Chan, C.L.W.; Wang, C.-W.; Ho, R.T.H.; Ng, S.-M.; Chan, J.S.M.; Ziea, E.T.C.; Wong, V.C.W. A systematic review of the effectiveness of qigong exercise in supportive cancer care. Support. Care Cancer 2012, 20, 1121–1133. [Google Scholar] [CrossRef] [PubMed]
- Farahani, M.A.; Soleimanpour, S.; Mayo, S.J.; Myers, J.S.; Panesar, P.; Ameri, F. The effect of mind-body exercise on cognitive function in cancer survivors: A systematic review. Can. Oncol. Nurs. J. Rev. Can. Nurs. Oncol. 2022, 32, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Tao, W.-W.; Jiang, H.; Tao, X.-M.; Jiang, P.; Sha, L.-Y.; Sun, X.-C. Effects of Acupuncture, Tuina, Tai Chi, Qigong, and Traditional Chinese Medicine Five-Element Music Therapy on Symptom Management and Quality of Life for Cancer Patients: A Meta-Analysis. J. Pain Symptom Manag. 2016, 51, 728–747. [Google Scholar] [CrossRef] [PubMed]
- Wayne, P.M.; Lee, M.S.; Novakowski, J.; Osypiuk, K.; Ligibel, J.; Carlson, L.E.; Song, R. Tai Chi and Qigong for cancer-related symptoms and quality of life: A systematic review and meta-analysis. J. Cancer Surviv. Res. Pract. 2018, 12, 256–267. [Google Scholar] [CrossRef]
- Wu, C.; Zheng, Y.; Duan, Y.; Lai, X.; Cui, S.; Xu, N.; Tang, C.; Lu, L. Nonpharmacological Interventions for Cancer-Related Fatigue: A Systematic Review and Bayesian Network Meta-Analysis. Worldviews Evid. Based Nurs. 2019, 16, 102–110. [Google Scholar] [CrossRef]
- Kuo, C.-C.; Wang, C.-C.; Chang, W.-L.; Liao, T.-C.; Chen, P.-E.; Tung, T.-H. Clinical Effects of Baduanjin Qigong Exercise on Cancer Patients: A Systematic Review and Meta-Analysis on Randomized Controlled Trials. Evid. Based Complement. Altern. Med. ECAM 2021, 2021, 6651238. [Google Scholar] [CrossRef]
- Meng, T.; Hu, S.; Cheng, Y.; Ye, M.; Wang, B.; Wu, J.; Chen, H. Qigong for women with breast cancer: An updated systematic review and meta-analysis. Complement. Ther. Med. 2021, 60, 102743. [Google Scholar] [CrossRef]
- Zeng, Y.; Luo, T.; Xie, H.; Huang, M.; Cheng, A.S.K. Health benefits of qigong or tai chi for cancer patients: A systematic review and meta-analyses. Complement. Ther. Med. 2014, 22, 173–186. [Google Scholar] [CrossRef]
- Cheung, D.S.T.; Takemura, N.; Smith, R.; Yeung, W.F.; Xu, X.; Ng, A.Y.M.; Lee, S.F.; Lin, C.-C. Effect of qigong for sleep disturbance-related symptom clusters in cancer: A systematic review and meta-analysis. Sleep Med. 2021, 85, 108–122. [Google Scholar] [CrossRef]
- Lin, W.-F.; Zhong, M.-F.; Zhou, Q.-H.; Zhang, Y.-R.; Wang, H.; Zhao, Z.-H.; Cheng, B.-B.; Ling, C.-Q. Efficacy of complementary and integrative medicine on health-related quality of life in cancer patients: A systematic review and meta-analysis. Cancer Manag. Res. 2019, 11, 6663–6680. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.-X.; Ren, Z.-Y.; Vafaei, S.; Zhang, J.-M.; Song, Y.; Wang, Y.-X.; Song, P.-G. Effectiveness of Baduanjin Exercise on Quality of Life and Psychological Health in Postoperative Patients With Breast Cancer: A Systematic Review and Meta-analysis. Integr. Cancer Ther. 2022, 21, 15347354221104092. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liu, J.-E.; Chen, S.; Zhao, F.; Chen, L.; Li, R. Effectiveness of Nonpharmacologic Interventions for Chemotherapy-Related Cognitive Impairment in Breast Cancer Patients: A Systematic Review and Network Meta-analysis. Cancer Nurs. 2022, 10–1097. [Google Scholar] [CrossRef]
- Wang, R.; Huang, X.; Wu, Y.; Sun, D. Efficacy of Qigong Exercise for Treatment of Fatigue: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 684058. Available online: https://www.frontiersin.org/articles/10.3389/fmed.2021.684058 (accessed on 8 January 2023). [CrossRef]
- Zeng, Y.; Xie, X.; Cheng, A.S.K. Qigong or Tai Chi in Cancer Care: An Updated Systematic Review and Meta-analysis. Curr. Oncol. Rep. 2019, 21, 48. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Haraldstad, K.; Wahl, A.; Andenæs, R.; Andersen, J.R.; Andersen, M.H.; Beisland, E.; Borge, C.R.; Engebretsen, E.; Eisemann, M.; Halvorsrud, L.; et al. A systematic review of quality of life research in medicine and health sciences. Qual. Life Res. 2019, 28, 2641–2650. [Google Scholar] [CrossRef]
- Nelson, K.L.; Davis, J.E.; Corbett, C.F. Sleep quality: An evolutionary concept analysis. Nurs. Forum 2022, 57, 144–151. [Google Scholar] [CrossRef]
- Stone, P.C.; Minton, O. Cancer-related fatigue. Eur. J. Cancer Oxf. Engl. 1990 2008, 44, 1097–1104. [Google Scholar] [CrossRef]
- Radbruch, L.; Strasser, F.; Elsner, F.; Gonçalves, J.F.; Løge, J.; Kaasa, S.; Nauck, F.; Stone, P.; Research Steering Committee of the European Association for Palliative Care (EAPC). Fatigue in palliative care patients--an EAPC approach. Palliat. Med. 2008, 22, 13–32. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Fang, P. The Impact of the Digital Traditional Qigong Regimen Exercises on Quality of Life and Sleep Disturbance in Head and Neck Cancer Patients Undergoing Radiotherapy. Master’s Thesis, Kaohsihung Medical University Hospital, Kaohsiung, Taiwan, 2018. [Google Scholar]
- Chen, Z.; Meng, Z.; Milbury, K.; Bei, W.; Zhang, Y.; Thornton, B.; Liao, Z.; Wei, Q.; Chen, J.; Guo, X.; et al. Qigong improves quality of life in women undergoing radiotherapy for breast cancer: Results of a randomized controlled trial. Cancer 2013, 119, 1690–1698. [Google Scholar] [CrossRef]
- Lam, W.-Y.; Lin, H.Y. A Randomised, Controlled Trial of Guolin Qigong in Patients Receiving Transcatheter Arterial Chemoembolisation for Unresectablehepatocellular Carcinoma. Master’s Thesis, The University of Hong Kong, Pokfulam, Hong Kong, 2004. [Google Scholar] [CrossRef]
- Robins, J.L.W.; McCain, N.L.; Elswick, R.K.; Walter, J.M.; Gray, D.P.; Tuck, I. Psychoneuroimmunology-Based Stress Management during Adjuvant Chemotherapy for Early Breast Cancer. Evid. Based Complement. Altern. Med. ECAM 2013, 2013, 372908. [Google Scholar] [CrossRef] [PubMed]
- Larkey, L.K.; Roe, D.J.; Weihs, K.L.; Jahnke, R.; Lopez, A.M.; Rogers, C.E.; Oh, B.; Guillen-Rodriguez, J. Randomized Controlled Trial of Qigong/Tai Chi Easy on Cancer-Related Fatigue in Breast Cancer Survivors. Ann. Behav. Med. 2015, 49, 165–176. [Google Scholar] [CrossRef]
- Loh, S.Y.; Lee, S.Y.; Murray, L. The Kuala Lumpur Qigong Trial for Women in the Cancer Survivorship Phase-Efficacy of a Three-Arm RCT to Improve QOL. Asian Pac. J. Cancer Prev. 2014, 15, 8127–8134. [Google Scholar] [CrossRef] [PubMed]
- APA Dictionary of Psychology. Available online: https://dictionary.apa.org/ (accessed on 8 January 2023).
- Stress. Available online: https://www.who.int/news-room/questions-and-answers/item/stress (accessed on 8 January 2023).
- Goldstein, D.S.; McEwen, B. Allostasis, homeostats, and the nature of stress. Stress Amst. Neth. 2002, 5, 55–58. [Google Scholar] [CrossRef]
- Holland, J.C.; Bultz, B.D. The NCCN Guideline for Distress Management: A Case for Making Distress the Sixth Vital Sign. J. Natl. Compr. Canc. Netw. 2007, 5, 3–7. [Google Scholar] [CrossRef]
- Pendergrass, J.C.; Targum, S.D.; Harrison, J.E. Cognitive Impairment Associated with Cancer: A Brief Review. Innov. Clin. Neurosci. 2018, 15, 36–44. [Google Scholar]
- Oh, B.; Butow, P.N.; Mullan, B.A.; Clarke, S.J.; Beale, P.J.; Pavlakis, N.; Lee, M.S.; Rosenthal, D.S.; Larkey, L.; Vardy, J. Effect of medical Qigong on cognitive function, quality of life, and a biomarker of inflammation in cancer patients: A randomized controlled trial. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2012, 20, 1235–1242. [Google Scholar] [CrossRef]
- Kang, D.-H.; Rice, M.; Park, N.-J.; Turner-Henson, A.; Downs, C. Stress and inflammation: A biobehavioral approach for nursing research. West. J. Nurs. Res. 2010, 32, 730–760. [Google Scholar] [CrossRef] [PubMed]
- Oh, B.; Butow, P.; Mullan, B.; Clarke, S.; Beale, P.; Pavlakis, N.; Kothe, E.; Lam, L.; Rosenthal, D. Impact of medical Qigong on quality of life, fatigue, mood and inflammation in cancer patients: A randomized controlled trial. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2010, 21, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Oh, B.; Butow, P.; Mullan, B.; Clarke, S. Medical Qigong for cancer patients: Pilot study of impact on quality of life, side effects of treatment and inflammation. Am. J. Chin. Med. 2008, 36, 459–472. [Google Scholar] [CrossRef]
- Liu, P.; You, J.; Loo, W.T.Y.; Sun, Y.; He, Y.; Sit, H.; Jia, L.; Wong, M.; Xia, Z.; Zheng, X.; et al. RETRACTED ARTICLE: The efficacy of Guolin-Qigong on the body-mind health of Chinese women with breast cancer: A randomized controlled trial. Qual. Life Res. 2017, 26, 2321–2331. [Google Scholar] [CrossRef]
- Lan, H. The Effects of Baduanjin on the Climacteric Syndrome and Inflammatory Factors in Breast Cancer Patients Treated with Aromatase Inhibitors. Master’s Thesis, Guangzhou Sport University, Guangzhou, China, 2019. [Google Scholar]
- Tsang, H.W.H.; Fung, K.M.T. A review on neurobiological and psychological mechanisms underlying the anti-depressive effect of qigong exercise. J. Health Psychol. 2008, 13, 857–863. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Clark, J.; Siskind, D.; Williams, G.M.; Byrne, G.; Yang, J.L.; Doi, S.A. A systematic review and meta-analysis of the effects of Qigong and Tai Chi for depressive symptoms. Complement. Ther. Med. 2015, 23, 516–534. [Google Scholar] [CrossRef]
- Quigley, K.S.; Kanoski, S.; Grill, W.M.; Barrett, L.F.; Tsakiris, M. Functions of Interoception: From Energy Regulation to Experience of the Self. Trends Neurosci. 2021, 44, 29–38. [Google Scholar] [CrossRef]
- Quadt, L.; Critchley, H.D.; Garfinkel, S.N. The neurobiology of interoception in health and disease. Ann. N. Y. Acad. Sci. 2018, 1428, 112–128. [Google Scholar] [CrossRef] [PubMed]
- Bonaz, B.; Lane, R.D.; Oshinsky, M.L.; Kenny, P.J.; Sinha, R.; Mayer, E.A.; Critchley, H.D. Diseases, Disorders, and Comorbidities of Interoception. Trends Neurosci. 2021, 44, 39–51. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Authors | Study Design | Number of Studies | Population | Qigong Styles in Exposure Group | Control Group | Outcome | Results |
|---|---|---|---|---|---|---|---|
| Klein 2016 [13] | Systematic review | 11 RCTs | 831 cancer patients (50% breast) | Guolin Qigong, Kuala Lumpur Qigong, Medical Qigong | Any type of control | Non-biological outcomes (fatigue, QOL, depression, mood, anxiety, distress, sleep quality, cognition, systolic blood pressure, and survival rate). Biological marker outcomes of inflammation and immune function | Significant effect of Qigong on: Fatigue: (p < 0.03) in 4/5 studies; Mood: (p = 0.021) in 1/1 study; Cognition: (p = 0.014) in 1/1 study; Social/family well-being: (p = 0.022) in 1/1 study; QoL: (p < 0.05) in 4/5 studies. Cardiovascular (systolic BP): (p = 0.002); Inflammatory response/immune support: (p < 0.05) in 6/10 studies No significant effect of Qigong on: Survival rate, sleep, anxiety, depression (except for 1/5 studies), and distress. |
| Henshall 2019 [14] | Systematic review | 3 RCTs; 7 pre–post test | 516 cancer patients (58% lung) | Medical Qigong (style n.r.) | n.r. | Dyspnea, fatigue, depression | Significant effect of Qigong at 10 weeks post-intervention on: Fatigue: (MD = 5.70 [95% CI, 3.32–8.09]) Depression: (MD = 2.56 [95% CI = 5.14–0.01]; p = 0.029) No effect of Qigong on: Dyspnea. |
| Lee 2007 [15] | Systematic review | 4 RCTs; 5 CCTs | 871 cancer patients | Internal Qigong (style n.r.) | Any type of control | Treatment effects | Significant effect of Qigong on: Fatigue (p < 0.05); Nausea, vomiting, and stomatitis (p < 0.05); Distress (p < 0.01). |
| Matthews 2018 [16] | Systematic review | 12 RCTs; 3 quasi-experimental designs | 1691 breast cancer women | Qigong (style n.r.) | Exercise, usual care | Sleep quality | Significant effect of Qigong on: Fatigue: decrease at post-intervention (p = 0.005) and 3-month follow-up (p = 0.024); decrease in people with fewer depressive symptoms at the RXT onset; Depression: decrease over time in both Qigong + Tai Chi and Qigong Shame (p < 0.05) compared to the control group; QoL: better QoL in people with fewer depressive symptoms at the RXT onset. No effect of Qigong on: Sleep quality |
| Van Vu 2017 [17] | Systematic review | 14 RCTs; 7 CCTs; 1 quasi-CCT | 1751 cancer patients | Guolin New Qigong, Tai Chi Qigong, 18 forms of Tai Chi Qigong, Yudong Kong exercise, Zhi Neng Qigong, Chan-Chuang Qigong, Medical/exercise Qigong (style n.r.), Sporting Qigong (style n.r.), | Any type of control | Physical symptoms, psychological symptoms, quality of life, adverse events | Significant effect of Qigong on: Fatigue: lower in 7/10 studies; QoL: improved in 6/10 studies; Neuropathy symptoms; Muscular strength; Cervical spine range of motion and shoulder complex range of motion; Frailty; Cognitive function; 6 min walking. No effect of Qigong on: Pain; Dyspnea; Cortisol rhythm; Temporomandibular joint mobility: Tumor size; Survival rate. Conflicting results on: Psychological symptoms; Sleep quality; Gastrointestinal symptoms. |
| Chan 2012 [18] | Systematic review | 8 RCTs; 15 CCTs | Studies on physical and psychosocial outcomes covered 572 cancer patients in Qigong groups and 595 cancer patients in control groups; the studies on biomedical outcomes covered 656 cancer patients in Qigong groups and 601 cancer patients in control groups | Medical/exercise Qigong (style n.r.), Guolin Qigong, Chan-Chuan Qigong, YoudoKong, a series of Qigong exercises (Jing Yang Gong, Fong Song Gong, Zhen Qu Yun Sing Gong, Zi Ti Sun Taiji Gong), multi-style Qigong | Any type of control and treatment | Self-perceived symptoms, quality of life, psychological distress, survival rate, response rate, fatigue, physical functioning, body weight, tumor size, “inflammatory markers” (C-reactive protein), parameters of immunity such as immunoglobulin and complement, the numbers or proportions of blood cells or their antioxidant capacity, and hepatic function | Significant effect of Qigong on: Symptoms (strength, appetite, diarrhea, or irregular defecation); Inflammation; Overall QOL (FACT-G); Mood disturbance; Increase in the number or levels of components in peripheral blood; Increase in the 5-year survival rate. Significant effect of Qigong on: Fatigue; Physical functioning (SF-36); Treatment side effects; Nausea and vomiting after 4 weeks (not significant after 8 weeks). No significant effect on: Psychological distress; Anxiety; Depression; Symptoms after 2.5 months. |
| Farahani 2022 [19] | Systematic review | 9 RCTs; 1 pilot study; 1 feasibility study | 1032 cancer survivors (85.8% breast cancer women) | Medical Qigong (style n.r.), Six Healing Sounds | Waitlist control, active control, usual care | Cognitive function | Significant effect of Qigong on: Subjective self-reported cognitive functions (in 6 out of 11 studies): for significant studies p < 0.05; Objective cognitive performance (in 1 out of 2 studies): processing speed (p = 0.007); executive function (p = n.r., Cohen’s d = −0.43 in favor of Qigong group); improvement in cognitive function (p = 0.014). |
| Tao 2016 [20] | Meta-analysis | 67 RCTs | 5465 adults with cancer | Qigong (style n.r.) | Usual care and active control conditions | HRQOL at post-treatment, cancer-related symptoms, and therapy-related adverse events | Significant effect of Qigong on: Sleep disturbance: positive effect of Qigong on Z = 3.02 (p = 0.003). No effect of Qigong on: QoL: Z = 0.98 (p = 0.33). |
| Wayne 2018 [21] | Systematic review and meta-analysis | 15 RCTs; 7 studies with non-randomized design or no control group | 1571 cancer patients | Qigong (style n.r.) | Active control; no treatment control | Cancer symptoms | Significant effect of Tai Chi Qigong on: Sleep difficulty: reduction in difficulties (Hedges’ g = −0.49, 95% CI −0.89 to −0.09, p = 0.018); Fatigue: reduction in fatigue (Hedges’ g = −0.53, 95% CI −0.97 to −0.28, p < 0.001); Depression: reduction in depression (Hedges’ g = −0.27, 95% CI −0.44 to −0.11, p = 0.001); QoL: (Hedges’ g = 0.33, 95% CI 0.10 to 0.56, p = 0.004). No effect of Tai Chi Qigong on: Cancer-related pain (Hedges’ g = −0.38, 95% CI −0.89 to 0.12, p = 0.136). |
| Wu 2019 [22] | Systematic review and Bayesian network meta-analysis | 182 RCTs | 18,491 cancer patients (45.05% studies on women with breast cancer, 25.27% studies on patients with multiple forms of cancer) | Qigong (style n.r.) | Placebo, usual care control, no intervention, waitlist control, or other non-pharmacological intervention | Cancer-related fatigue | Significant effect of Qigong on: Fatigue: lower level of fatigue compared to the control group (MD [95% CI], −2.03 [−3.36, −0.68]) |
| Kuo 2021 [23] | Systematic review and meta-analysis | 10 RCTs | 811 cancer patients | Baduanjin Qigong | Routine care; active exercise | Cancer-related fatigue, sleep quality, QoL | Significant effect of Qigong on: Cancer-related fatigue: significantly less in the Baduanjin Qigong group compared with the control group (odds ratio = 0.27; 95% CI [0.17, 0.42]; test for overall effect: Z = 5.81, p < 0.00001; Heterogeneity I2 = 0%); QoL: Baduanjin Qigong exercise has a positive effect on breast cancer patients’ QoL: From EORTC-C30: MD = 13.13 (95% CI [1.87, 24.40]; Z = 2.29, p = 0.02; Heterogeneity I2 = 92%); From FACT-B: MD = 11.04 (95% CI [9.56, 12.53] Z = 14.57, p < 0.00001; Heterogeneity I2= 88%); Sleep Quality: Baduanjin Qigong exercise has a positive effect on breast cancer patients’ sleep quality: MD = −2.89 (95% CI [−3.48, −2.30] Z = 9.55, p < 0.001; Heterogeneity I2 = 0%). |
| Meng 2021 [24] | Systematic review and meta-analysis | 14 RCTs; 3 CCTs | 1236 breast cancer women | Chan-Chuang Qigong, Guolin New Qigong, Tai Chi Qigong, Kuala Lumpur Qigong, Sporting Qigong, Baduanjin | Any type of control | QoL, fatigue, sleep disturbance, cancer-related emotional disturbance | Significant effect of Qigong on: QoL: positive effect of Qigong compared to control procedures (n = 950, SMD = 0.65, 95% CI 0.23–1.08, p = 0.002); Depression: (n = 540, SMD = −0.32, 95% CI −0.59 to −0.04, p = 0.02, I2 = 59%); Anxiety-related serum protein (1 study): positive rate was significantly lower in the Qigong group than in the control group (p < 0.01); Immune responses (2 studies): significant reduction in IL-2, IFN-γ, IL-6, IL-1β, and TNF-α levels in Qigong group. No effect of Qigong on: Sleep disturbance: (n = 298, SMD = −0.11, 95% CI −0.74 to −0.52, p = 0.73, I2 = 86%); Cancer-related fatigue: (n = 206; SMD = −0.32, 95 % CI −0.71 to 0.07, p = 0.11, I2 = 73%); Anxiety: (n = 439, SMD = −0.71, 95% CI −1.32 to −0.10, p = 0.02, I2 = 89%). |
| Zeng 2014 [25] | Systematic review and meta-analysis | 13 RCTs | 592 cancer patients | Guolin Qigong, Medical Qigong | Any type of control | Body fat mass (BFM) and body mass index (BMI); anxiety and depression, biomarkers (cortisol levels, C-reactive protein (CRP)), and QOL | Significant effect of Qigong/Tai Chi on: Cancer-specific QOL (Z = 4.00 (p < 0.0001), I2 = 95%); Fatigue (Z = 2.09, p = 0.04, I2 = 90%); Immune function; Cortisol level: (Z = 1.97 (p = 0.05), I2 = 0%). |
| Cheung 2021 [26] | Systematic review and meta-analysis | 11 RCTs | 907 cancer patients | Guolin Qigong, Chan-Chuang Qigong, Xianggong, Baduanjin, General Qigong (style n.r.) | Placebo or usual care | Sleep quality and fatigue/depressive symptoms | Significant effect of Qigong on: Improving post-intervention: Sleep quality: (SMD = −1.28, 95% CI: −2.01, −0.55; p = n.r.; I2 = 95%); Fatigue: (SMD = −0.89, 95% CI: −1.59, −0.19; p = n.r.; I2 = 94%) in cancer patients post-intervention. Qigong’s effect on sleep was significantly mediated by its effect on fatigue (b = 1.27, SE = 0.24, p = 0.002), but not depressive symptoms (b = 0.53, SE = 0.26, p = 0.106). No effect of Qigong: Beneficial effects on sleep and fatigue became non-significant after 3 months. No effect of Qigong post-intervention on: Depressive symptoms: (SMD = −0.69, 95% CI: −1.81, 0.42; p = n.r.; I2 = 95%). |
| Lin 2019 [27] | Systematic review and meta-analysis | 34 RCTs | 3010 cancer patients (92% female) | Qigong (style n.r.) | No intervention | HRQoL | Significant improvement over usual care on: HRQOL - CH (MD = 6.03 [0.15–11.92]); - Qigong + MM (MD = 12.66 [8.75–16.57]) |
| Ye 2022 [28] | Systematic review and meta-analysis | 7 RCTs | 450 postoperative breast cancer patients | Baduanjin Qigong | Any type of control | QoL, anxiety, depression | Significant effect of Qigong on: General QoL (FACT-B): (WMD = 5.70, 95% CI [3.11–8.29], Z = 4.32, p < 0.0001, I2 = 35%); Physical well-being (FACT-B): (WMD = 1.83, 95% CI [1.13, 2.53], Z = 5.15, p < 0.00001, I2 = 0%); Functional well-being (FACT-B): (WMD = 1.58, 95% CI [0.77–2.39], Z = 3.83 p = 0.0001, I2 = 0%); Role-physical QoL (SF-36): (WMD = 11.49, 95% CI [8.86, 14.13], Z = 8.55, p < 0.00001, I2 = 0%); Vitality (fatigue) (SF-36): (WMD = 8.58, 95% CI [5.60–11.56], Z = 5.65, p < 0.00001, I2 = 0%); Anxiety: (WMD = −8.02, 95% CI [−9.27- −6.78], Z = 12.62, p < 0.00001, I2 = 10%); Depression: (WMD = −4.45, 95%CI [−5.62–−3.28], Z = 7.45, p < 0.00001, I2 = 32%). No significant difference in: Social and emotional well-being (FACT-B); Physical functioning (SF-36); Bodily pain (SF-36); Social functioning (SF-36); General health (SF-36); Mental health (SF-36). |
| Liu 2022 [29] | Systematic review and network meta-analysis | 12 RCTs | 818 female breast cancer patients | Internal Qigong (style n.r.) | Routine nursing or treatments (e.g., placebo, usual care, no intervention, waitlist control, supportive therapy or other nonpharmacologic intervention) | Chemotherapy-related cognitive impairment (CRCI) | Significant effect of Qigong on: CRCI: improvement in the objective outcome of CRCI compared to psychotherapy (SMD = 1.27; 95% CI, 0.13–2.41) and to music therapy (SMD = 1.69; 95% CI, 0.10–3.28). No significant effect of Qigong compared with the non-pharmacological and control interventions on: CRCI: subjective outcomes. |
| Wang 2021 [30] | Systematic review and meta-analysis | 16 RCTs | 1313 patients (339 cancer patients) | Baduanjin, Six Healing Sounds Qigong, Wu Xing Ping Heng Gong, Shaolin Qigong Exercises, Self-improving exercise (style n.r.), Wuqinxi, Yijinjing | Any type of control | Fatigue | Significant effect of Qigong on: Cancer-related fatigue (total, physical, and mental): SMD−0.75 (−1.37 to−0.13) p = 0.02 I2 = 86%. |
| Zeng 2019 [31] | Systematic review and meta-analysis | 12 RCTs | 915 cancer patients | Qigong (style n.r.), Medical Qigong (style n.r.) | Usual care, support groups, waitlist control, or sham Qigong control | Treatment effects | Significant effect of Qigong on: Fatigue: (MD = 2.05, 95% CI [0.63, 3.47]; Z = 2.83 p = 0.005, I2 = 96%); Sleep difficulties (MD = 344.17, 95% CI [316.95, 371.39]; Z = 24.78, p = 0.00001, I2 0%). No effect of Qigong on: Stress (MD = −8.56, 95% CI [−17.56, 0.44]; Z = 1.86, p = 0.06, I2 = 74%); Anxiety: (MD = −1.26, 95% CI [−3.73, 1.20]; Z = 1.00, p = 0.32, I2 = 43%); Depression: (MD = −2.58, 95% CI [−7.33, 2.17]; Z = 1.06, p = 0.29, I2 = 88%). |
| Number of Quality Assessment Criteria Satisfied by the Studies | Studies That Satisfy the Criteria |
|---|---|
| 14/16 | Klein et al., 2013 [13] Chan et al., 2012 [18] Meng et al., 2021 [24] Lin et al., 2019 [27] |
| 13/16 | Lee et al., 2007 [15] Farahani et al., 2022 [19] Wayne et., 2018 [21] Cheung et al., 2021 [26] Ye et al., 2022 [28] Wang et al., 2021 [30] |
| 12/16 | Henshall et al., 2019 [14] Van Vu et al., 2017 [17] Kuo et al., 2021 [23] Zeng et al., 2014 [25] Liu et al., 2022 [29] |
| 11/16 | Tao et al., 2016 [20] |
| 10/16 | Matthews et al., 2018 [16] |
| 9/16 | Wu et al., 2019 [22] |
| 8/16 | Zeng Y et al., 2019 [31] |
| Systematic Review/Meta-Analysis | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Q15 | Q16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Klein PJ et al. 2016 [13] | Y | N | Y | PY | Y | Y | Y | PY | Y | N | NA | NA | Y | Y | NA | Y |
| Henshall CL et al. 2019 [14] | Y | N | Y | PY | N | Y | N | PY | Y | N | Y | Y | Y | Y | Y | Y |
| Lee MS et al. 2007 [15] | Y | PY | N | Y | Y | Y | N | Y | Y | N | NA | NA | Y | Y | NA | Y |
| Matthews EE et al. 2018 [16] | Y | N | N | PY | Y | Y | N | Y | Y | N | NA | NA | Y | N | NA | N |
| Van Vu D et al. 2017 [17] | Y | PY | N | PY | Y | Y | N | PY | Y | N | NA | NA | Y | Y | NA | N |
| Chan CL et al. 2012 [18] | Y | Y | Y | PY | N | Y | PY | Y | PY | N | NA | NA | Y | Y | NA | Y |
| Farahani MA 2022 [19] | Y | PY | N | PY | Y | Y | N | PY | Y | N | NA | NA | Y | Y | NA | Y |
| Tao WW et al. 2016 [20] | Y | N | N | PY | Y | Y | N | PY | Y | N | Y | Y | Y | Y | N | Y |
| Wayne PM et al. 2018 [21] | Y | N | Y | PY | Y | Y | N | PY | Y | N | Y | Y | Y | Y | Y | Y |
| Wu C et al. 2019 [22] | Y | N | Y | PY | N | Y | N | N | Y | N | Y | Y | Y | N | N | Y |
| Kuo CC et al. 2021 [23] | Y | N | N | PY | Y | Y | N | PY | Y | N | Y | Y | Y | Y | Y | Y |
| Meng T et al. 2021 [24] | Y | N | Y | PY | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Zeng Y et al. 2014 [25] | Y | N | Y | PY | Y | N | N | PY | Y | N | Y | Y | Y | Y | Y | Y |
| Cheung DST et al. 2021 [26] | Y | N | Y | PY | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y |
| Lin WF et al. 2019 [27] | Y | Y | Y | PY | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y |
| Ye XX et al. 2022 [28] | Y | PY | N | PY | Y | Y | N | PY | Y | N | Y | Y | Y | Y | Y | Y |
| Liu Y et al. 2022 [29] | Y | PY | N | PY | Y | Y | N | PY | Y | N | Y | Y | Y | Y | Y | N |
| Wang R et al. 2021 [30] | Y | Y | N | PY | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y |
| Zeng Y et al. 2019 [31] | Y | N | N | N | N | N | N | PY | Y | N | Y | Y | Y | Y | N | Y |
| Outcome | Evidence Supporting Qi Gong Integration |
|---|---|
| Quality of life | YES |
| Sleep quality | YES * |
| Cancer-related fatigue | YES |
| Depression | Uncertain |
| Anxiety | Uncertain |
| Stress/distress | NO |
| Cognitive impairment | YES ** |
| Cancer-related symptoms: dyspnea | NO |
| Cancer-related symptoms: pain | NO |
| Cancer-related symptoms: nausea and vomiting | YES * |
| Cancer-related symptoms: appetite, bowel function | YES * |
| Biological Marker | Meaning | Evidence Supporting Qigong Integration |
|---|---|---|
| Cortisol level | Hypothalamic–pituitary–adrenal activity | NO |
| IL-2 | Inflammation response | Uncertain |
| IL-6 | Inflammation response | Uncertain |
| TNF-a | Inflammation response | Uncertain |
| CRP | Inflammation response | YES * |
| IFN-y | Inflammation response | NO |
| WBC | Immune response | YES |
| RBC, Hb | Erythropoiesis | YES |
| α-Naphthyl butyrate esterase (ANAE) | Immune response | YES |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazzocco, K.; Milani, A.; Ciccarelli, C.; Marzorati, C.; Pravettoni, G. Evidence for Choosing Qigong as an Integrated Intervention in Cancer Care: An Umbrella Review. Cancers 2023, 15, 1176. https://doi.org/10.3390/cancers15041176
Mazzocco K, Milani A, Ciccarelli C, Marzorati C, Pravettoni G. Evidence for Choosing Qigong as an Integrated Intervention in Cancer Care: An Umbrella Review. Cancers. 2023; 15(4):1176. https://doi.org/10.3390/cancers15041176
Chicago/Turabian StyleMazzocco, Ketti, Alessandra Milani, Chiara Ciccarelli, Chiara Marzorati, and Gabriella Pravettoni. 2023. "Evidence for Choosing Qigong as an Integrated Intervention in Cancer Care: An Umbrella Review" Cancers 15, no. 4: 1176. https://doi.org/10.3390/cancers15041176
APA StyleMazzocco, K., Milani, A., Ciccarelli, C., Marzorati, C., & Pravettoni, G. (2023). Evidence for Choosing Qigong as an Integrated Intervention in Cancer Care: An Umbrella Review. Cancers, 15(4), 1176. https://doi.org/10.3390/cancers15041176