
Dosimetric Impact of Intrafraction Prostate Motion and Interfraction Anatomical Changes in Dose-Escalated Linac-Based SBRT

 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort and Treatment Protocol
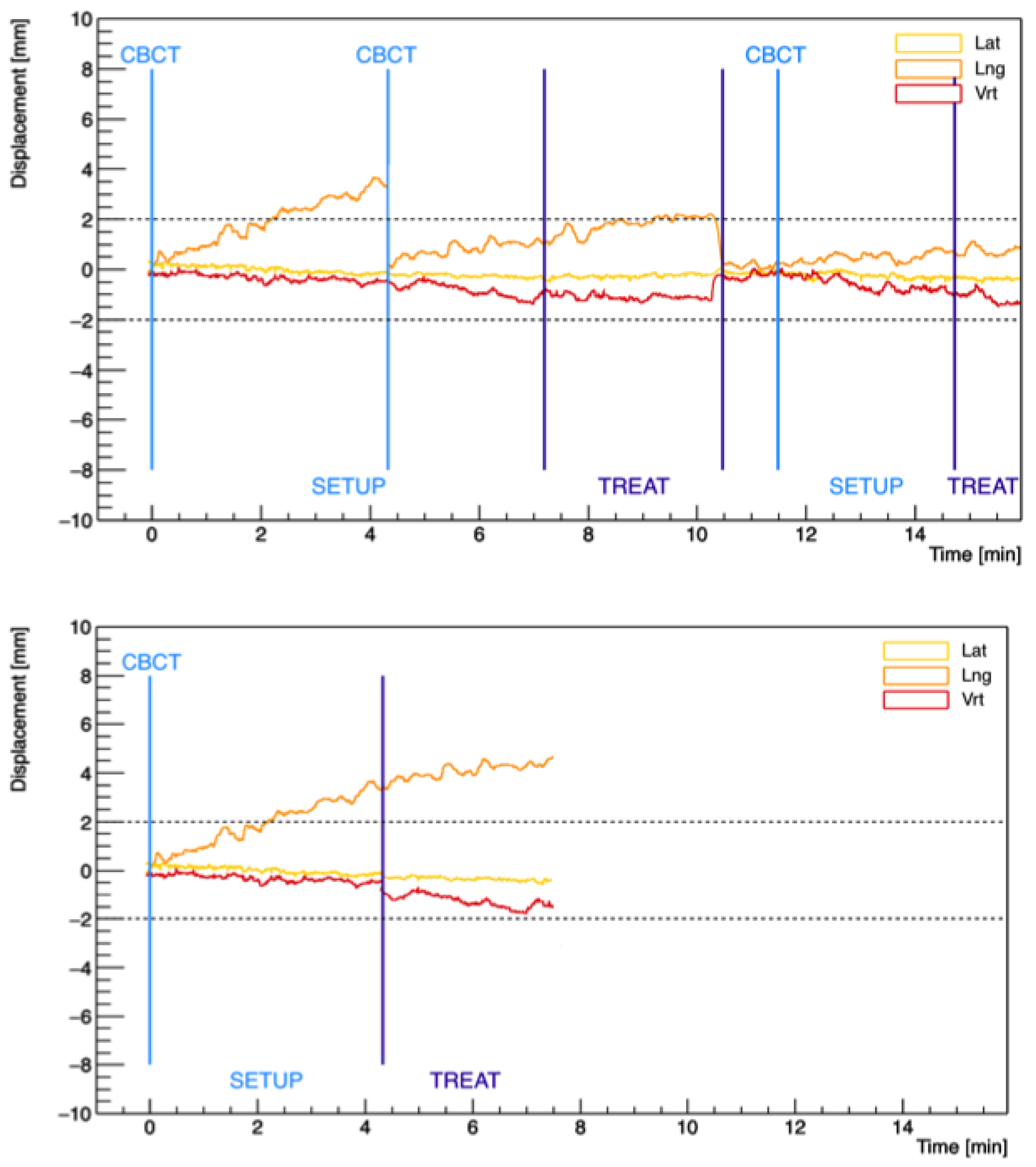
2.2. Intrafraction Prostate Trajectories and Simulation of Non-Gated Treatments
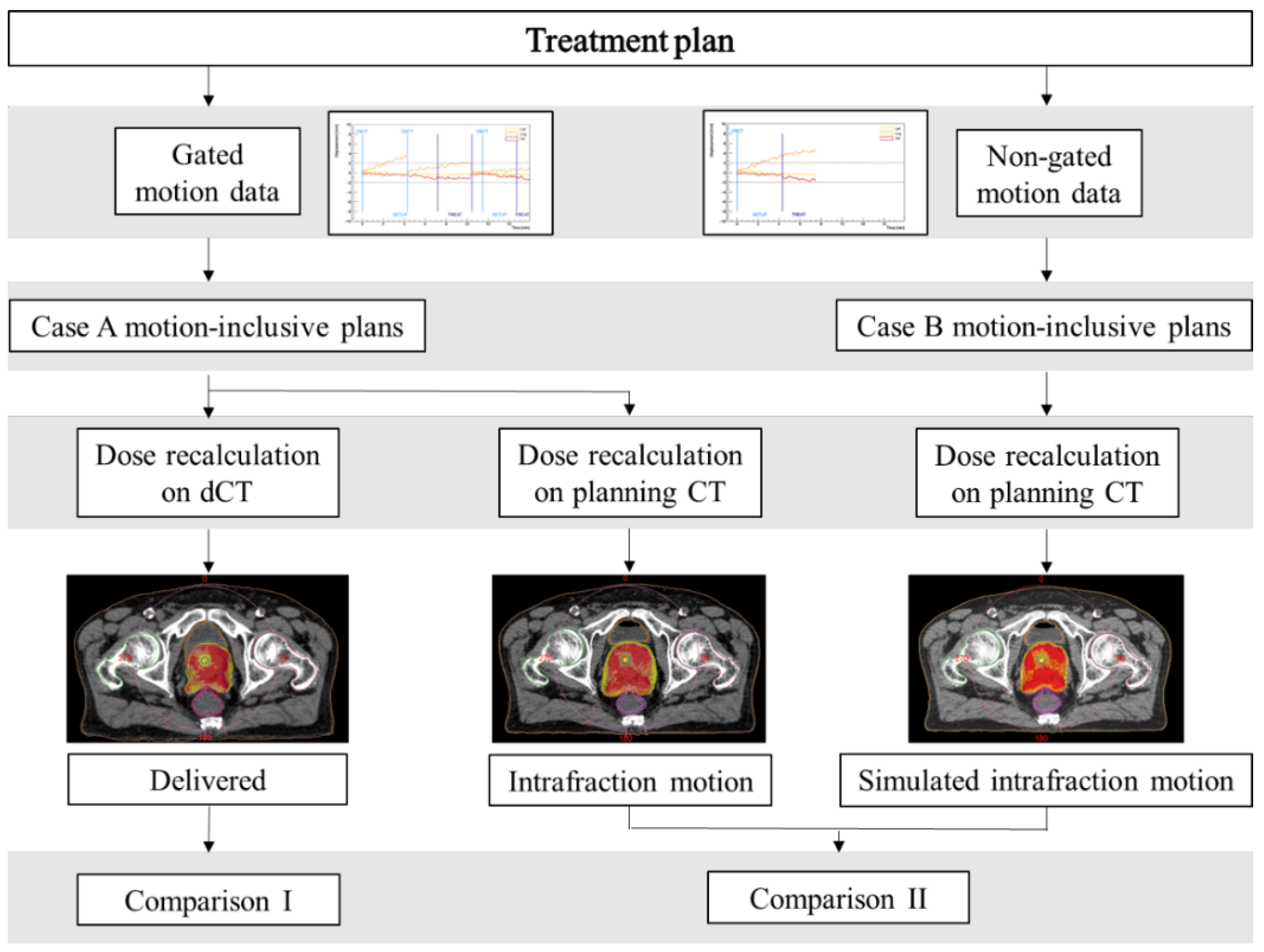
2.3. Motion-Inclusive Reconstruction Method and Dose Calculation
2.4. Data Analysis and Statistical Tests
3. Results
3.1. Intrafraction Prostate Motion
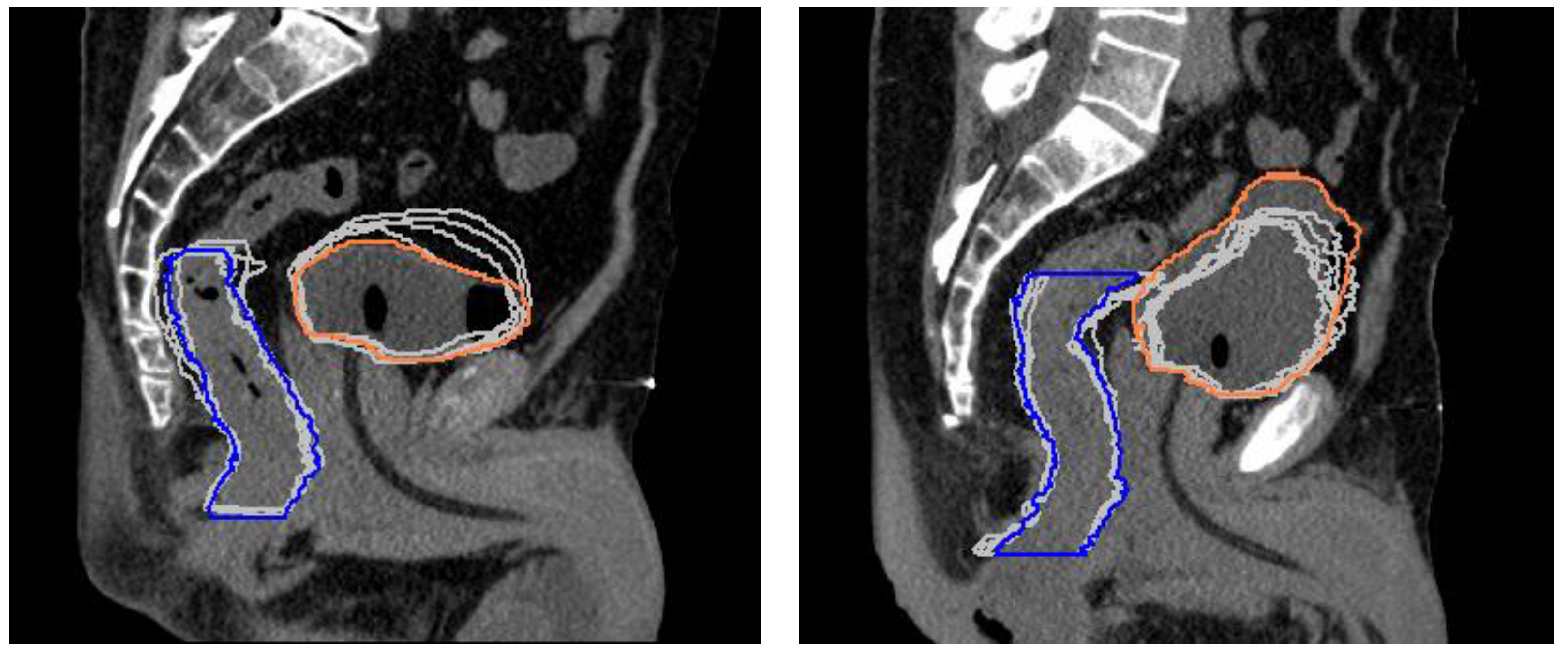
3.2. CTV, Rectum, and Bladder Volume Changes
3.3. Dosimetric Analysis
3.3.1. Comparison I: Delivered vs. Planned Dose Distributions
3.3.2. Comparison II: Case B vs. Case A Motion-Inclusive Dose Distributions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Metric | Individual Fractions | p-Value | Cumulative Treatments | |
|---|---|---|---|---|
| CTV | Dmean | +0.1% [−0.7–2.3] | 0.522 | +0.1% [−0.1–0.5] |
| D99% | −0.2% [−5.1–5.1] | 0.392 | +0.0% [−1.8–1.1] | |
| D2% | +0.3% [−0.4–4.4] | 0.086 | −0.4% [−0.7–0.1] | |
| PTV | Dmean | 0.0% [−0.7–2.0] | 0.875 | 0.0% [−0.4–0.4] |
| D95% | −0.4% [−3.7–1.4] | 0.136 | −0.2% [−1.6–0.8] | |
| D2% | +0.4% [−0.4–4.3] | 0.056 | −0.4% [−0.7–0.1] | |
| PTV—CTV | Dmean | −0.1% [−1.5–1.0] | 0.907 | −0.1% [−1.0–0.3] |
| D95% | −1.0% [−12.1–7.1] | 0.337 | −1.1% [−7.8–2.5] | |
| Urethra PRV | D0.035 cc | +0.7% [−0.8–6.4] | 0.168 | −0.2% [−0.6–0.4] |
| D10% | +0.6% [−0.9–5.4] | 0.175 | +0.1% [−0.3–0.9] | |
| Rectum | D5% | −1.7% [−14.4–11.5] | 0.419 | −2.5% [−8.8–3.1] |
| D10% | −2.3% [−16.7–14.2] | 0.526 | −2.9% [−9.7–3.8] | |
| D20% | −2.9% [−39.8–13.6] | 0.592 | −3.1% [−10.4–4.9] | |
| D50% | −1.3% [−12.5–6.2] | 0.852 | −1.8% [−7.6–2.2] | |
| Rectum wall | D0.035 cc | −0.6% [−7.9–5.3] | 0.584 | −1.6% [−4.8–1.7] |
| Rectum mucosa | D0.035 cc | −1.1% [−13.5–14.0] | 0.507 | −2.3% [−8.3–3.3] |
| Bladder | D0.035 cc | +0.3% [−1.9–3.3] | 0.580 | −0.2% [−1.1–1.1] |
| D10% | +0.2% [−11.7–11.4] | 0.926 | +1.2% [−4.9–7.5] | |
| D40% | +1.4 [−18.7–37.7] | 0.907 | +5.1% [−7.8–25.1] |
References
- Proust-Lima, C.; Taylor, J.M.; Sécher, S.; Sandler, H.; Kestin, L.; Pickles, T.; Bae, K.; Allison, R.; Williams, S. Confirmation of a Low α/β Ratio for Prostate Cancer Treated by External Beam Radiation Therapy Alone Using a Post-Treatment Repeated-Measures Model for PSA Dynamics. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Miralbell, R.; Roberts, S.A.; Zubizarreta, E.; Hendry, J.H. Dose-Fractionation Sensitivity of Prostate Cancer Deduced from Radiotherapy Outcomes of 5969 Patients in Seven International Institutional Datasets: α/β = 1.4 (0.9–2.2) Gy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e17–e24. [Google Scholar] [CrossRef] [PubMed]
- Dasu, A.; Toma-Dasu, I. Prostate alpha/beta revisited—An analysis of clinical results from 14 168 patients. Acta Oncol. 2012, 51, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Morgan, S.C.; Hoffman, K.; Loblaw, D.A.; Buyyounouski, M.K.; Patton, C.; Barocas, D.; Bentzen, S.; Chang, M.; Efstathiou, J.; Greany, P.; et al. Hypofractionated radiation therapy for localized prostate cancer: An ASTRO, ASCO, and AUA evidence-based guideline. Pract. Radiat. Oncol. 2018, 8, 354–360. [Google Scholar] [CrossRef]
- King, C.R.; Freeman, D.; Kaplan, I.; Fuller, D.; Bolzicco, G.; Collins, S.; Meier, R.; Wang, J.; Kupelian, P.; Steinberg, M.; et al. Stereotactic body radiotherapy for localized prostate cancer: Pooled analysis from a multi-institutional consortium of prospective phase II trials. Radiother. Oncol. 2013, 109, 217–221. [Google Scholar] [CrossRef]
- Katz, A.J.; Kang, J. Stereotactic Body Radiotherapy as Treatment for Organ Confined Low- and Intermediate-Risk Prostate Carcinoma, a 7-Year Study. Front. Oncol. 2014, 4, 240. [Google Scholar] [CrossRef]
- Alayed, Y.; Cheung, P.; Pang, G.; Mamedov, A.; D’Alimonte, L.; Deabreu, A.; Commisso, K.; Commisso, A.; Zhang, L.; Quon, H.C.; et al. Dose escalation for prostate stereotactic ablative radiotherapy (SABR): Late outcomes from two prospective clinical trials. Radiother. Oncol. 2018, 127, 213–218. [Google Scholar] [CrossRef]
- Langen, K.; Jones, D. Organ motion and its management. Int. J. Radiat. Oncol. Biol. Phys. 2001, 50, 265–278. [Google Scholar] [CrossRef]
- Kron, T.; Thomas, J.; Fox, C.; Thompson, A.; Owen, R.; Herschtal, A.; Haworth, A.; Tai, K.-H.; Foroudi, F. Intra-fraction prostate displacement in radiotherapy estimated from pre- and post-treatment imaging of patients with implanted fiducial markers. Radiother. Oncol. 2010, 95, 191–197. [Google Scholar] [CrossRef]
- Ballhausen, H.; Li, M.; Hegemann, N.-S.; Ganswindt, U.; Belka, C. Intra-fraction motion of the prostate is a random walk. Phys. Med. Biol. 2015, 60, 549–563. [Google Scholar] [CrossRef]
- Legge, K.; Nguyen, D.; Ng, J.A.; Wilton, L.; Richardson, M.; Booth, J.; Keall, P.; O’Connor, D.J.; Greer, P.; Martin, J. Real-time intrafraction prostate motion during linac based stereotactic radiotherapy with rectal displacement. J. Appl. Clin. Med. Phys. 2017, 18, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Gorovets, D.; Burleson, S.; Jacobs, L.; Ravindranath, B.; Tierney, K.; Kollmeier, M.; McBride, S.; Happersett, L.; Hunt, M.; Zelefsky, M. Prostate SBRT With Intrafraction Motion Management Using a Novel Linear Accelerator–Based MV-kV Imaging Method. Pract. Radiat. Oncol. 2020, 10, e388–e396. [Google Scholar] [CrossRef] [PubMed]
- Panizza, D.; Faccenda, V.; Lucchini, R.; Daniotti, M.C.; Trivellato, S.; Caricato, P.; Pisoni, V.; De Ponti, E.; Arcangeli, S. Intrafraction Prostate Motion Management During Dose-Escalated Linac-Based Stereotactic Body Radiation Therapy. Front. Oncol. 2022, 12, 883725. [Google Scholar] [CrossRef] [PubMed]
- Lucchini, R.; Panizza, D.; Colciago, R.R.; Vernier, V.; Daniotti, M.C.; Faccenda, V.; Arcangeli, S. Treatment outcome and compliance to dose-intensified linac-based SBRT for unfavorable prostate tumors using a novel real-time organ-motion tracking. Radiat. Oncol. 2021, 16, 180. [Google Scholar] [CrossRef] [PubMed]
- Kupelian, P.A.; Langen, K.M.; Zeidan, O.A.; Meeks, S.L.; Willoughby, T.R.; Wagner, T.H.; Jeswani, S.; Ruchala, K.J.; Haimerl, J.; Olivera, G.H. Daily variations in delivered doses in patients treated with radiotherapy for localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Colvill, E.; Poulsen, P.R.; Booth, J.T.; O’Brien, R.T.; Ng, J.A.; Keall, P.J. DMLC tracking and gating can improve dose coverage for prostate VMAT. Med. Phys. 2014, 41, 091705. [Google Scholar] [CrossRef]
- McParland, N.; Pearson, M.; Wong, J.; Sigur, I.; Stenger, C.; Tyldesley, S. Quantifying daily variation in volume and dose to the prostate, rectum and bladder using cone-beam computerised tomography. J. Radiother. Pract. 2014, 13, 79–86. [Google Scholar] [CrossRef]
- Lovelock, D.M.; Messineo, A.P.; Cox, B.W.; Kollmeier, M.A.; Zelefsky, M.J. Continuous Monitoring and Intrafraction Target Position Correction During Treatment Improves Target Coverage for Patients Undergoing SBRT Prostate Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 588–594. [Google Scholar] [CrossRef]
- Pearson, D.; Gill, S.K.; Campbell, N.; Reddy, K. Dosimetric and volumetric changes in the rectum and bladder in patients receiving CBCT-guided prostate IMRT: Analysis based on daily CBCT dose calculation. J. Appl. Clin. Med. Phys. 2016, 17, 107–117. [Google Scholar] [CrossRef]
- Wahl, M.; Descovich, M.; Shugard, E.; Pinnaduwage, D.; Sudhyadhom, A.; Chang, A.; Roach, M.; Gottschalk, A.; Chen, J. Interfraction Anatomical Variability Can Lead to Significantly Increased Rectal Dose for Patients Undergoing Stereotactic Body Radiotherapy for Prostate Cancer. Technol. Cancer Res. Treat. 2017, 16, 178–187. [Google Scholar] [CrossRef]
- Vanhanen, A.; Poulsen, P.; Kapanen, M. Dosimetric effect of intrafraction motion and different localization strategies in prostate SBRT. Phys. Med. 2020, 75, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Devlin, L.; Dodds, D.; Sadozye, A.; McLoone, P.; MacLeod, N.; Lamb, C.; Currie, S.; Thomson, S.; Duffton, A. Dosimetric impact of organ at risk daily variation during prostate stereotactic ablative radiotherapy. Br. J. Radiol. 2020, 93, 20190789. [Google Scholar] [CrossRef]
- Litzenberg, D.W.; Hadley, S.W.; Tyagi, N.; Balter, J.M.; Haken, R.K.T.; Chetty, I.J. Synchronized dynamic dose reconstruction. Med. Phys. 2007, 34, 91–102. [Google Scholar] [CrossRef]
- Li, H.S.; Chetty, I.J.; Enke, C.A.; Foster, R.D.; Willoughby, T.R.; Kupellian, P.A.; Solberg, T.D. Dosimetric Consequences of Intrafraction Prostate Motion. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 801–812. [Google Scholar] [CrossRef] [PubMed]
- Langen, K.M.; Lü, W.; Ngwa, W.; Willoughby, T.R.; Chauhan, B.; Meeks, S.L.; Kupelian, A.P.; Olivera, G. Correlation between dosimetric effect and intrafraction motion during prostate treatments delivered with helical tomotherapy. Phys. Med. Biol. 2008, 53, 7073–7086. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Mah, D.; Happersett, L.; Cox, B.; Hunt, M.; Mageras, G. Determination of action thresholds for electromagnetic tracking system-guided hypofractionated prostate radiotherapy using volumetric modulated arc therapy. Med. Phys. 2011, 38, 4001–4008. [Google Scholar] [CrossRef] [PubMed]
- Adamson, J.; Wu, Q.; Yan, D. Dosimetric Effect of Intrafraction Motion and Residual Setup Error for Hypofractionated Prostate Intensity-Modulated Radiotherapy with Online Cone Beam Computed Tomography Image Guidance. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 453–461. [Google Scholar] [CrossRef]
- van de Water, S.; Valli, L.; Aluwini, S.; Lanconelli, N.; Heijmen, B.; Hoogeman, M. Intrafraction Prostate Translations and Rotations During Hypofractionated Robotic Radiation Surgery: Dosimetric Impact of Correction Strategies and Margins. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 1154–1160. [Google Scholar] [CrossRef]
- Azcona, J.D.; Xing, L.; Chen, X.; Bush, K.; Li, R. Assessing the Dosimetric Impact of Real-Time Prostate Motion During Volumetric Modulated Arc Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 1167–1174. [Google Scholar] [CrossRef]
- Russo, S.; Ricotti, R.; Molinelli, S.; Patti, F.; Barcellini, A.; Mastella, E.; Pella, A.; Paganelli, C.; Marvaso, G.; Pepa, M.; et al. Dosimetric Impact of Inter-Fraction Anatomical Changes in Carbon Ion Boost Treatment for High-Risk Prostate Cancer (AIRC IG 14300). Front. Oncol. 2021, 11, 740661. [Google Scholar] [CrossRef]
- Poulsen, P.R.; Schmidt, M.L.; Keall, P.; Worm, E.S.; Fledelius, W.; Hoffmann, L. A method of dose reconstruction for moving targets compatible with dynamic treatments. Med. Phys. 2012, 39, 6237–6246. [Google Scholar] [CrossRef] [PubMed]
- Richter, A.; Hu, Q.; Steglich, D.; Baier, K.; Wilbert, J.; Guckenberger, M.; Flentje, M. Investigation of the usability of conebeam CT data sets for dose calculation. Radiat. Oncol. 2008, 3, 42. [Google Scholar] [CrossRef] [PubMed]
- Hatton, J.; McCurdy, B.; Greer, P. Cone beam computerized tomography: The effect of calibration of the Hounsfield unit number to electron density on dose calculation accuracy for adaptive radiation therapy. Phys. Med. Biol. 2009, 54, N329–N346. [Google Scholar] [CrossRef] [PubMed]
- Varadhan, R.; Hui, S.K.; Way, S.; Nisi, K. Assessing prostate, bladder and rectal doses during image guided radiation therapy-need for plan adaptation? J. Appl. Clin. Med. Phys. 2009, 10, 56–74. [Google Scholar] [CrossRef]
- Fotina, I.; Hopfgartner, J.; Stock, M.; Steininger, T.; Lütgendorf-Caucig, C.; Georg, D. Feasibility of CBCT-based dose calculation: Comparative analysis of HU adjustment techniques. Radiother. Oncol. 2012, 104, 249–256. [Google Scholar] [CrossRef]
- Nicosia, L.; Sicignano, G.; Rigo, M.; Figlia, V.; Cuccia, F.; De Simone, A.; Giaj-Levra, N.; Mazzola, R.; Naccarato, S.; Ricchetti, F.; et al. Daily dosimetric variation between image-guided volumetric modulated arc radiotherapy and MR-guided daily adaptive radiotherapy for prostate cancer stereotactic body radiotherapy. Acta Oncol. 2020, 60, 215–221. [Google Scholar] [CrossRef]
- Chen, S.; Quan, H.; Qin, A.; Yee, S.; Yan, D. MR image-based synthetic CT for IMRT prostate treatment planning and CBCT image-guided localization. J. Appl. Clin. Med. Phys. 2016, 17, 236–245. [Google Scholar] [CrossRef]
- Imae, T.; Haga, A.; Watanabe, Y.; Takenaka, S.; Shiraki, T.; Nawa, K.; Ogita, M.; Takahashi, W.; Yamashita, H.; Nakagawa, K.; et al. Retrospective dose reconstruction of prostate stereotactic body radiotherapy using cone-beam CT and a log file during VMAT delivery with flattening-filter-free mode. Radiol. Phys. Technol. 2020, 13, 238–248. [Google Scholar] [CrossRef]
- Juneja, P.; Colvill, E.; Kneebone, A.; Eade, T.; Ng, J.A.; Thwaites, D.I.; Keall, P.; Kaur, R.; Poulsen, P.R.; Booth, J.T. Quantification of intrafraction prostate motion and its dosimetric effect on VMAT. Australas. Phys. Eng. Sci. Med. 2017, 40, 317–324. [Google Scholar] [CrossRef]
- Jaccard, M.; Ehrbar, S.; Miralbell, R.; Hagen, T.; Koutsouvelis, N.; Poulsen, P.; Rouzaud, M.; Tanadini-Lang, S.; Tsoutsou, P.; Guckenberger, M.; et al. Single-fraction prostate stereotactic body radiotherapy: Dose reconstruction with electromagnetic intrafraction motion tracking. Radiother. Oncol. 2021, 156, 145–152. [Google Scholar] [CrossRef]
- Brock, K.K.; Mutic, S.; McNutt, T.R.; Li, H.; Kessler, M.L. Use of image registration and fusion algorithms and techniques in radiotherapy: Report of the AAPM Radiation Therapy Committee Task Group No. 132. Med. Phys. 2017, 44, e43–e76. [Google Scholar] [CrossRef]
- Gunnlaugsson, A.; Kjellén, E.; Hagberg, O.; Thellenberg-Karlsson, C.; Widmark, A.; Nilsson, P. Change in prostate volume during extreme hypo-fractionation analysed with MRI. Radiat. Oncol. 2014, 9, 22. [Google Scholar] [CrossRef]
- Ma, T.M.; Neylon, J.; Casado, M.; Sharma, S.; Sheng, K.; Low, D.; Yang, Y.; Steinberg, M.L.; Lamb, J.; Cao, M.; et al. Dosimetric impact of interfraction prostate and seminal vesicle volume changes and rotation: A post-hoc analysis of a phase III randomized trial of MRI-guided versus CT-guided stereotactic body radiotherapy. Radiother. Oncol. 2021, 167, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Schaeffrer, E.; Srinivas, S.; Adra, N.; An, Y.; Barocas, D.; Bitting, R.; Bryce, A.; Chapin, B.; Cheng, H.H.; D’Amico, A.V.; et al. Prostate cancer, version 1.2023 featured updates to the NCCN guidelines. J. Natl. Compr. Cancer Netw. 2022, 20, 1288–1298. [Google Scholar] [CrossRef]
- Pawlowski, J.M.; Yang, E.S.; Malcolm, A.W.; Coffey, C.W.; Ding, G.X. Reduction of Dose Delivered to Organs at Risk in Prostate Cancer Patients via Image-Guided Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 924–934. [Google Scholar] [CrossRef]
- Hatton, J.A.; Greer, P.B.; Tang, C.; Wright, P.; Capp, A.; Gupta, S.; Parker, J.; Wratten, C.; Denham, J.W. Does the planning dose–volume histogram represent treatment doses in image-guided prostate radiation therapy? Assessment with cone-beam computerised tomography scans. Radiother. Oncol. 2011, 98, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Kishan, A.U.; Ma, T.M.; Lamb, J.M.; Casado, M.; Wilhalme, H.; Low, D.A.; Sheng, K.; Sharma, S.; Nickols, N.G.; Pham, J.; et al. Magnetic Resonance Imaging–Guided vs Computed Tomography–Guided Stereotactic Body Radiotherapy for Prostate Cancer: The MIRAGE Randomized Clinical Trial. JAMA Oncol. 2023. [Google Scholar] [CrossRef]
- Brennan, V.S.; Burleson, S.; Kostrzewa, C.; Scripes, P.G.; Subashi, E.; Zhang, Z.; Tyagi, N.; Zelefsky, M.J. SBRT focal dose intensification using an MR-Linac adaptive planning for intermediate-risk prostate cancer: An analysis of the dosimetric impact of intra-fractional organ changes. Radiother. Oncol. 2022, 179, 109441. [Google Scholar] [CrossRef] [PubMed]



| Direction | Mean [Range] | Mean Abs | Mean Diff [Range] | Mean Abs Diff |
|---|---|---|---|---|
| Lateral | −0.5 [−3.1–0.8] | 0.7 | −0.3 [−1.6–0.3] | 0.3 |
| Longitudinal | −0.4 [−4.2–3.7] | 1.4 | −0.4 [−2.8–2.4] | 0.7 |
| Vertical | −1.2 [−3.5–1.9] | 1.6 | −0.7 [−1.8–0.7] | 0.7 |
| 3D | 2.6 [0.7–5.1] | 1.3 [0.3–2.8] |
| Mean (SD) | Median [Range] | CV [Range] | |
|---|---|---|---|
| CTV | −1.3% (4.0) | −0.1% [−12.6–2.2] | 2.3% [0.4–4.2] |
| Rectum | −3.5% (10.1) | −3.8% [−19.9–27.3] | 5.7% [2.3–8.5] |
| Bladder | +8.9% (42.0) | +8.7% [−60.9–117.6] | 19.6% [13.5–28.3] |
| Comparison I | Comparison II | ||||||
|---|---|---|---|---|---|---|---|
| Metrics | Individual Fractions | p-Value | Cumulative Treatments | Individual Fractions | p-Value | Cumulative Treatments | |
| CTV | Dmean | −0.5% [−2.0–1.2] | 0.416 | −0.5% [−1.4–0.2] | −0.2% [−2.3–0.8] | 0.312 | 0.0% [−0.5–1.2] |
| D99% | −3.0% [−18.5–2.8] | 0.001 | −3.1% [−13.2–0.5] | −2.8% [−16.3–1.1] | 0.020 | −1.3% [−8.3–0.2] | |
| D2% | −0.4% [−1.6–2.8] | 0.028 | −0.4% [−1.2–0.1] | −0.1% [−4.2–0.6] | 1.000 | +0.1% [−0.7–1.3] | |
| 0.284 | |||||||
| PTV | Dmean | −0.7% [−2.9–1.2] | 0.059 | −0.6% [−1.9–0.2] | −0.4% [−2.1–0.8] | 0.284 | −0.1% [−0.6–1.4] |
| D95% | −2.6% [−17.8–1.0] | 0.000 | −2.7% [−11.9–−0.2] | −2.4% [−11.9–0.9] | 0.002 | −1.0% [−5.3–0.6] | |
| D2% | −0.4% [−1.5–2.7] | 0.074 | −0.3% [−1.1–0.2] | −0.4% [−4.1–0.6] | 0.926 | +0.1% [−0.8–1.4] | |
| PTV—CTV | Dmean | −1.2% [−5.8–1.3] | 0.059 | −1.2% [−3.9–0.5] | −0.8% [−3.6–0.6] | 0.270 | −0.2% [−1.5–1.8] |
| D95% | −4.8% [−27.3–6.4] | 0.001 | −4.9% [−19.3–3.6] | −5.6% [−23.7–1.9] | 0.013 | −2.0% [−8.9–1.1] | |
| Urethra PRV | D0.035 cc | +1.0% [−1.6–5.6] | 0.046 | +1.1% [−0.7–2.2] | +0.4% [−5.3–2.9] | 0.333 | +0.2% [−0.6–0.8] |
| D10% | +0.7% [−1.2–4.9] | 0.158 | +0.7% [−0.6–1.3] | +0.6% [−5.0–6.3] | 0.312 | +0.2% [−0.7–1.0] | |
| Rectum | D5% | −4.7% [−35.9–24.6] | 0.163 | −4.7% [−27.7–12.0] | −4.3% [−30.8–13.0] | 0.240 | −1.8% [−9.6–5.7] |
| D10% | −5.0% [−41.7–31.7] | 0.371 | −5.1% [−33.5–14.6] | −4.6% [−33.8–27.5] | 0.248 | −2.0% [−10.5–6.6] | |
| D20% | −3.6% [−38.4–39.0] | 0.514 | −3.7% [−31.3–15.5] | −4.8% [−31.2–38.0] | 0.343 | −2.0% [−11.5–7.3] | |
| D50% | −1.5% [−24.1–38.8] | 0.792 | −1.5% [−18.9–16.1] | −1.9% [−22.1–25.1] | 0.742 | −0.9% [−8.8–8.2] | |
| Rectum wall | D0.035 cc | −0.8% [−13.5–12.6] | 0.921 | −0.5% [−5.9–8.7] | −3.0% [−25.2–4.7] | 0.177 | −1.4% [−12.0–3.3] |
| Rectum mucosa | D0.035 cc | +0.8% [−27.1–33.9] | 0.560 | +1.0% [−10.5–22.6] | −3.9% [−30.3–8.6] | 0.338 | −1.8% [−10.9–4.7] |
| Bladder | D0.035 cc | −0.8% [−7.0–1.2] | 0.123 | −0.8% [−2.4–0.4] | +0.3% [−6.3–3.0] | 0.445 | +0.3% [−1.2–3.2] |
| D10% | −4.6% [−44.6–38.0] | 0.077 | −4.6% [−27.6–20.5] | +3.1% [−13.8–24.6] | 0.421 | +0.9% [−4.2–5.4] | |
| D40% | +2.6% [−74.0–319.9] | 0.019 | −0.9% [−52.7–234.4] | +11.6% [−22.8–83.5] | 0.680 | +3.2% [−9.8–17.7] | |
| Planning | Treatment | |||||
|---|---|---|---|---|---|---|
| Dose Constraints | Patients Failing | Infringement Rate | Major Deviations | Patients Failing | Infringement Rate | Major Deviations |
| PTV D95% < 95% | 0 | 0% | - | 7 | 54% | 1 |
| CTV D95% < 95% | - | - | - | 4 | 31% | - |
| Rectum wall D0.035 cc | 0 | 0% | - | 2 | 15% | - |
| Rectum mucosa D0.035 cc | 6 | 46% | - | 5 | 38% | 2 |
| Bladder D40% | 1 | 8% | 1 | 1 | 8% | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faccenda, V.; Panizza, D.; Daniotti, M.C.; Pellegrini, R.; Trivellato, S.; Caricato, P.; Lucchini, R.; De Ponti, E.; Arcangeli, S. Dosimetric Impact of Intrafraction Prostate Motion and Interfraction Anatomical Changes in Dose-Escalated Linac-Based SBRT. Cancers 2023, 15, 1153. https://doi.org/10.3390/cancers15041153
Faccenda V, Panizza D, Daniotti MC, Pellegrini R, Trivellato S, Caricato P, Lucchini R, De Ponti E, Arcangeli S. Dosimetric Impact of Intrafraction Prostate Motion and Interfraction Anatomical Changes in Dose-Escalated Linac-Based SBRT. Cancers. 2023; 15(4):1153. https://doi.org/10.3390/cancers15041153
Chicago/Turabian StyleFaccenda, Valeria, Denis Panizza, Martina Camilla Daniotti, Roberto Pellegrini, Sara Trivellato, Paolo Caricato, Raffaella Lucchini, Elena De Ponti, and Stefano Arcangeli. 2023. "Dosimetric Impact of Intrafraction Prostate Motion and Interfraction Anatomical Changes in Dose-Escalated Linac-Based SBRT" Cancers 15, no. 4: 1153. https://doi.org/10.3390/cancers15041153
APA StyleFaccenda, V., Panizza, D., Daniotti, M. C., Pellegrini, R., Trivellato, S., Caricato, P., Lucchini, R., De Ponti, E., & Arcangeli, S. (2023). Dosimetric Impact of Intrafraction Prostate Motion and Interfraction Anatomical Changes in Dose-Escalated Linac-Based SBRT. Cancers, 15(4), 1153. https://doi.org/10.3390/cancers15041153