
Association of Dipeptidyl Peptidase-4 Inhibitors Use with Reduced Risk of Hepatocellular Carcinoma in Type 2 Diabetes Patients with Chronic HBV Infection


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Resource
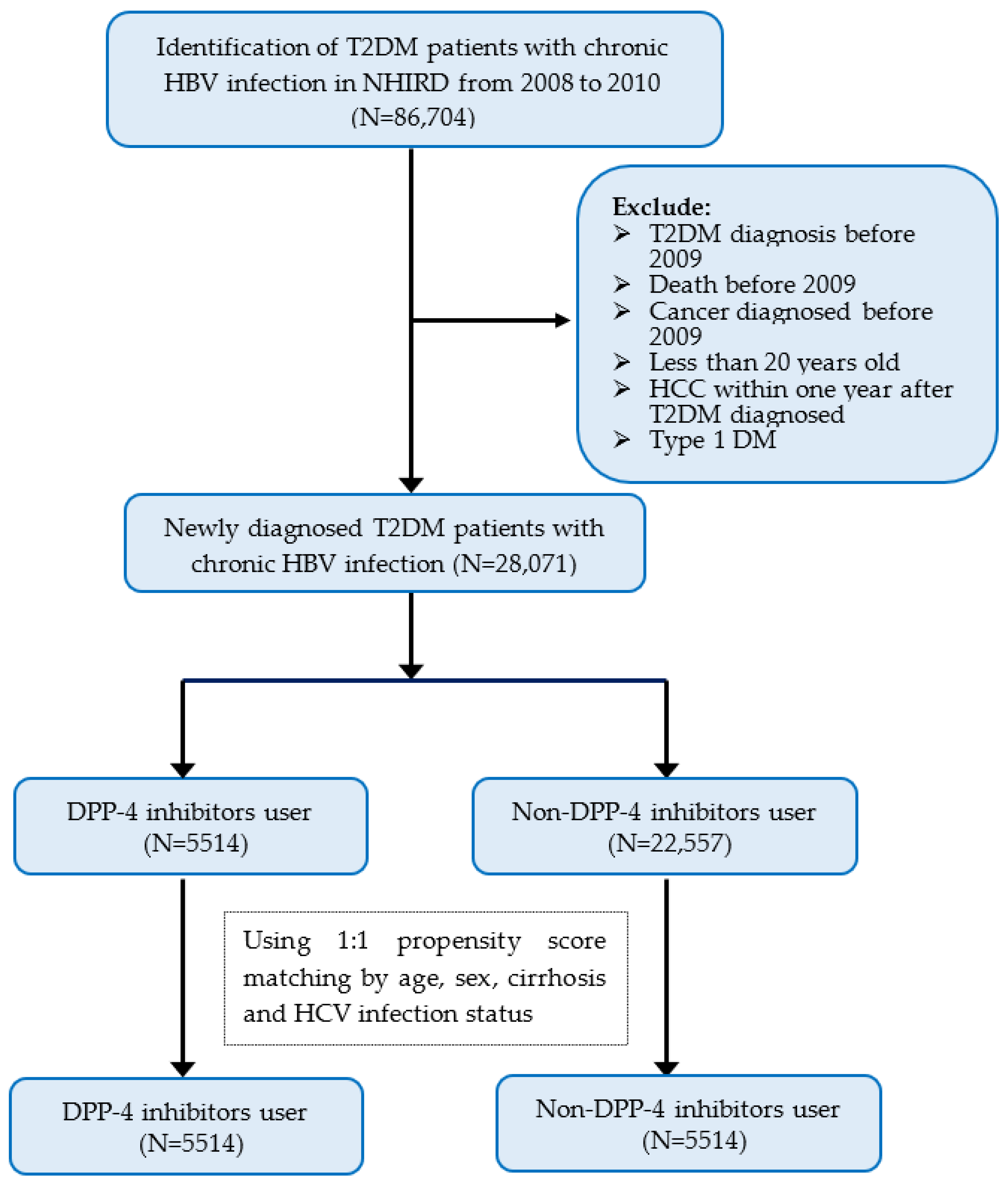
2.2. Study Population
2.3. Definition of DPP4 Inhibitors Use and Comorbidities
2.4. Follow-Up to Newly Diagnosed HCC
2.5. Study Design
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
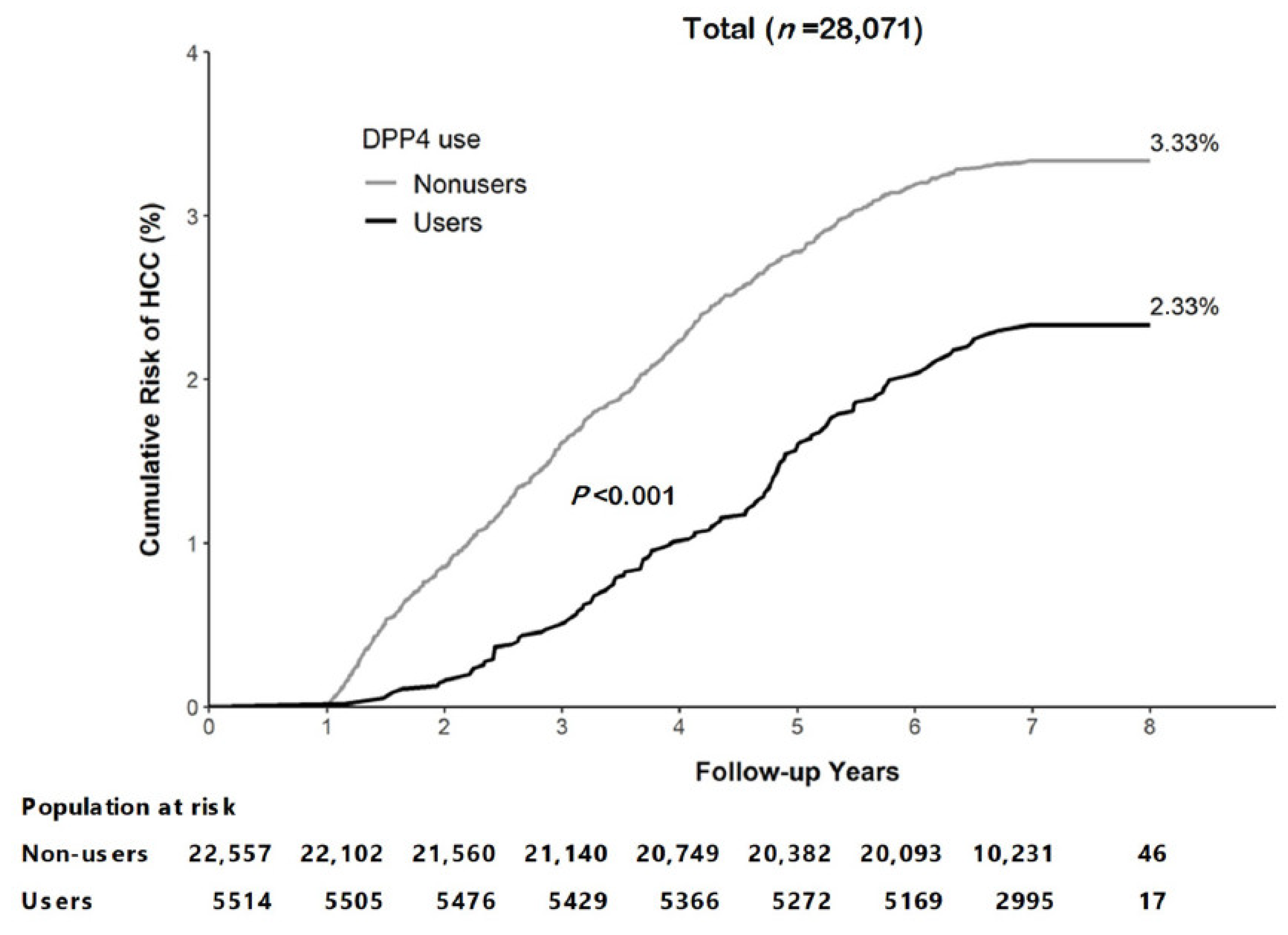
3.2. Incidence of HCC
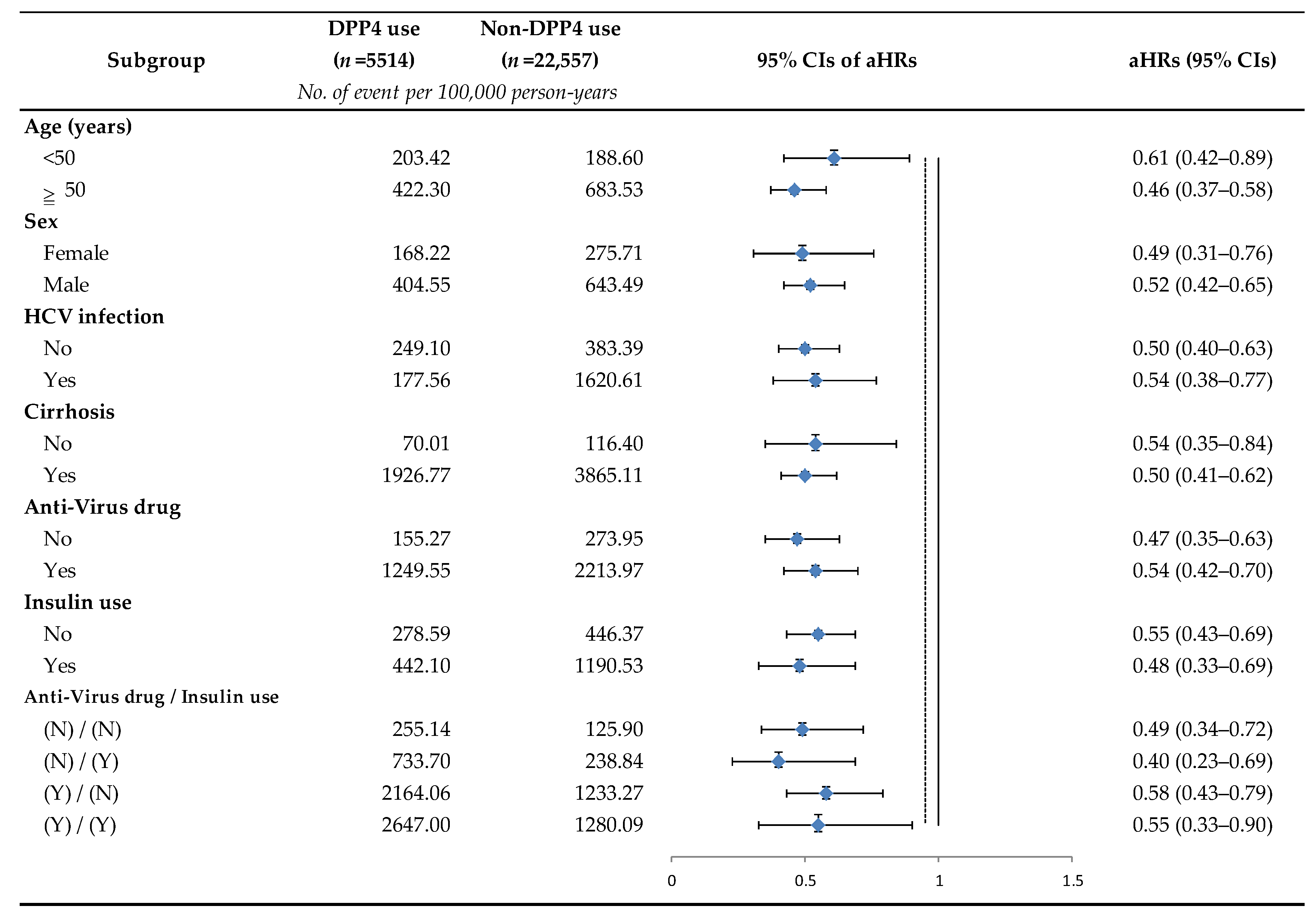
3.3. Relative Risk of HCC with and without Treatment with DPP-4 Inhibitors
4. Discussion
The Limitations of Our Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.H.; Wong, G.; Gane, E.; Kao, J.H.; Dusheiko, G. Hepatitis B Virus: Advances in Prevention, Diagnosis, and Therapy. Clin. Microbiol. Rev. 2020, 33, e00046-19. [Google Scholar] [CrossRef] [PubMed]
- Campbell, C.; Wang, T.; McNaughton, A.L.; Barnes, E.; Matthews, P.C. Risk factors for the development of hepatocellular carcinoma (HCC) in chronic hepatitis B virus (HBV) infection: A systematic review and meta-analysis. J. Viral Hepat. 2021, 28, 493–507. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.J. Global elimination of viral hepatitis and hepatocellular carcinoma: Opportunities and challenges. Gut 2018, 67, 595–598. [Google Scholar] [CrossRef] [PubMed]
- WHO. Hepatitis B Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 18 December 2022).
- Stevens, C.E.; Beasley, R.P.; Tsui, J.; Lee, W.C. Vertical transmission of hepatitis B antigen in Taiwan. N. Engl. J. Med. 1975, 292, 771–774. [Google Scholar] [CrossRef]
- Stevens, C.E.; Toy, P.; Kamili, S.; Taylor, P.E.; Tong, M.J.; Xia, G.L.; Vyas, G.N. Eradicating hepatitis B virus: The critical role of preventing perinatal transmission. Biologicals 2017, 50, 3–19. [Google Scholar] [CrossRef]
- Lu, F.T.; Ni, Y.H. Elimination of Mother-to-Infant Transmission of Hepatitis B Virus: 35 Years of Experience. Pediatr. Gastroenterol. Hepatol. Nutr. 2020, 23, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Yang, H.I.; Lee, M.H.; Lu, S.N.; Jen, C.L.; Wang, L.Y.; You, S.L.; Iloeje, U.H.; Chen, C.J. Incidence and determinants of spontaneous hepatitis B surface antigen seroclearance: A community-based follow-up study. Gastroenterology 2010, 139, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.W.; Wang, T.C.; Lin, S.C.; Chang, H.Y.; Chen, D.S.; Hu, J.T.; Yang, S.S.; Kao, J.H. Increased risk of cirrhosis and its decompensation in chronic hepatitis B patients with newly diagnosed diabetes: A nationwide cohort study. Clin. Infect. Dis. 2013, 57, 1695–1702. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109–119. [Google Scholar] [CrossRef]
- Sheen, Y.J.; Hsu, C.C.; Jiang, Y.D.; Huang, C.N.; Liu, J.S.; Sheu, W.H. Trends in prevalence and incidence of diabetes mellitus from 2005 to 2014 in Taiwan. J. Formos. Med. Assoc. 2019, 118 (Suppl. 2), S66–S73. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, P.; Henshaw, C.; Youlden, D.R.; Clark, P.J.; Aitken, J.F.; Baade, P.D. Global Trends in Incidence Rates of Primary Adult Liver Cancers: A Systematic Review and Meta-Analysis. Front. Oncol. 2020, 10, 171. [Google Scholar] [CrossRef] [PubMed]
- McGlynn, K.A.; Petrick, J.L.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma. Hepatology 2021, 73 (Suppl. 1), 4–13. [Google Scholar] [CrossRef] [PubMed]
- Ko, W.H.; Chiu, S.Y.; Yang, K.C.; Chen, H.H. Diabetes, hepatitis virus infection and hepatocellular carcinoma: A case-control study in hepatitis endemic area. Hepatol. Res. 2012, 42, 774–781. [Google Scholar] [CrossRef]
- Kim, J.H.; Sinn, D.H.; Gwak, G.Y.; Kang, W.; Paik, Y.H.; Choi, M.S.; Lee, J.H.; Koh, K.C.; Paik, S.W. Insulin resistance and the risk of hepatocellular carcinoma in chronic hepatitis B patients. J. Gastroenterol. Hepatol. 2017, 32, 1100–1106. [Google Scholar] [CrossRef]
- Mao, D.; Lau, E.S.H.; Wu, H.; Yang, A.; Shi, M.; Fan, B.; Tam, C.H.T.; Chow, E.; Kong, A.P.S.; Ma, R.C.W.; et al. Risk associations of long-term HbA1c variability and obesity on cancer events and cancer-specific death in 15,286 patients with diabetes-A prospective cohort study. Lancet Reg. Health West. Pac. 2022, 18, 100315. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Targher, G. Type 2 diabetes mellitus and risk of hepatocellular carcinoma: Spotlight on nonalcoholic fatty liver disease. Ann. Transl. Med. 2017, 5, 270. [Google Scholar] [CrossRef] [PubMed]
- Lomonaco, R.; Godinez Leiva, E.; Bril, F.; Shrestha, S.; Mansour, L.; Budd, J.; Portillo Romero, J.; Schmidt, S.; Chang, K.L.; Samraj, G.; et al. Advanced Liver Fibrosis Is Common in Patients With Type 2 Diabetes Followed in the Outpatient Setting: The Need for Systematic Screening. Diabetes Care 2021, 44, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.; Wei, S.; Zhang, W.; Yang, J.; Yang, J.; Yan, L. Type 2 diabetes mellitus increases the risk of hepatocellular carcinoma in subjects with chronic hepatitis B virus infection: A meta-analysis and systematic review. Cancer Manag. Res. 2019, 11, 705–713. [Google Scholar] [CrossRef]
- Singh, S.; Singh, P.P.; Singh, A.G.; Murad, M.H.; Sanchez, W. Anti-diabetic medications and the risk of hepatocellular cancer: A systematic review and meta-analysis. Am. J. Gastroenterol. 2013, 108, 881–891. [Google Scholar] [CrossRef]
- Kramer, J.R.; Natarajan, Y.; Dai, J.; Yu, X.; Li, L.; El-Serag, H.B.; Kanwal, F. Effect of diabetes medications and glycemic control on risk of hepatocellular cancer in patients with nonalcoholic fatty liver disease. Hepatology 2022, 75, 1420–1428. [Google Scholar] [CrossRef] [PubMed]
- Yen, F.S.; Hsu, C.C.; Wei, C.C.; Hou, M.C.; Hwu, C.M. Selection and Warning of Evidence-Based Antidiabetic Medications for Patients With Chronic Liver Disease. Front. Med. 2022, 9, 839456. [Google Scholar] [CrossRef] [PubMed]
- Chu, W.-M.; Ho, H.-E.; Huang, K.-H.; Tsan, Y.-T.; Liou, Y.-S.; Wang, Y.-H.; Lee, M.-C.; Li, Y.-C. The prescribing trend of oral antidiabetic agents for type 2 diabetes in Taiwan: An 8-year population-based study. Medicine 2017, 96, e8257. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Wang, L.J.; Jiang, B.; Li, X.Q.; Guo, C.L.; Guo, S.J.; Shi, D.Y. Recent progress of the development of dipeptidyl peptidase-4 inhibitors for the treatment of type 2 diabetes mellitus. Eur. J. Med. Chem. 2018, 151, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Gangopadhyay, K.K.; Singh, P. Consensus Statement on Dose Modifications of Antidiabetic Agents in Patients with Hepatic Impairment. Indian J. Endocrinol. Metab. 2017, 21, 341–354. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Gu, H.; Li, K.; Lin, J.; Zhu, Y.; Deng, W. DPP4 inhibitor reduces portal hypertension in cirrhotic rats by normalizing arterial hypocontractility. Life Sci. 2021, 284, 119895. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.C.; Hsu, S.J.; Chuang, C.L.; Hsiung, S.Y.; Chang, C.C.; Hou, M.C.; Lee, F.Y. Effects of dipeptidyl peptidase-4 inhibition on portal hypertensive and cirrhotic rats. J. Chin. Med. Assoc. 2021, 84, 1092–1099. [Google Scholar] [CrossRef]
- Shimada, S.; Kamiyama, T.; Orimo, T.; Nagatsu, A.; Kamachi, H.; Taketomi, A. High HbA1c is a risk factor for complications after hepatectomy and influences for hepatocellular carcinoma without HBV and HCV infection. Hepatobiliary Surg. Nutr. 2021, 10, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.H.; Sue, S.P.; Liang, H.L.; Tseng, C.W.; Lin, H.C.; Wen, W.L.; Lee, M.Y. Dipeptidyl Peptidase 4 Inhibitors Decrease the Risk of Hepatocellular Carcinoma in Patients With Chronic Hepatitis C Infection and Type 2 Diabetes Mellitus: A Nationwide Study in Taiwan. Front. Public Health 2021, 9, 711–723. [Google Scholar] [CrossRef]
- Yip, T.C.; Wong, V.W.; Chan, H.L.; Tse, Y.K.; Hui, V.W.; Liang, L.Y.; Lee, H.W.; Lui, G.C.; Kong, A.P.; Wong, G.L. Thiazolidinediones reduce the risk of hepatocellular carcinoma and hepatic events in diabetic patients with chronic hepatitis B. J. Viral Hepat. 2020, 27, 904–914. [Google Scholar] [CrossRef]
- Sheu, M.J.; Liang, F.W.; Li, S.T.; Li, C.Y.; Lu, T.H. Validity of ICD-10-CM Codes Used to Identify Patients with Chronic Hepatitis B and C Virus Infection in Administrative Claims Data from the Taiwan National Health Insurance Outpatient Claims Dataset. Clin. Epidemiol. 2020, 12, 185–192. [Google Scholar] [CrossRef]
- Yen, F.S.; Chiang, J.H.; Hwu, C.M.; Yen, Y.H.; Lin, B.J.; Wei, J.C.; Hsu, C.C. All-cause mortality of insulin plus dipeptidyl peptidase-4 inhibitors in persons with type 2 diabetes. BMC Endocr. Disord. 2019, 19, 3. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.J.; Wang, Y.W.; Lee, W.C. Taiwan’s Nationwide Cancer Registry System of 40 years: Past, present, and future. J. Formos. Med. Assoc. 2019, 118, 856–858. [Google Scholar] [CrossRef] [PubMed]
- Health Promotion Administration. Cancer Registry Annual Report, 2020 Taiwan. Available online: https://www.hpa.gov.tw/File/Attach/16434/File_20339.pdf (accessed on 18 December 2022).
- Xie, J.; Strauss, V.Y.; Martinez-Laguna, D.; Carbonell-Abella, C.; Diez-Perez, A.; Nogues, X.; Collins, G.S.; Khalid, S.; Delmestri, A.; Turkiewicz, A.; et al. Association of Tramadol vs Codeine Prescription Dispensation With Mortality and Other Adverse Clinical Outcomes. JAMA 2021, 326, 1504–1515. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ke, J.; Zhu, Y.J.; Cao, B.; Yin, R.L.; Wang, Y.; Wei, L.L.; Zhang, L.J.; Yang, L.Y.; Zhao, D. Dipeptidyl peptidase-4 (DPP4) inhibitor sitagliptin alleviates liver inflammation of diabetic mice by acting as a ROS scavenger and inhibiting the NFκB pathway. Cell Death Discov. 2021, 7, 236. [Google Scholar] [CrossRef]
- Nishina, S.; Yamauchi, A.; Kawaguchi, T.; Kaku, K.; Goto, M.; Sasaki, K.; Hara, Y.; Tomiyama, Y.; Kuribayashi, F.; Torimura, T.; et al. Dipeptidyl Peptidase 4 Inhibitors Reduce Hepatocellular Carcinoma by Activating Lymphocyte Chemotaxis in Mice. Cell Mol. Gastroenterol. Hepatol. 2018, 7, 115–134. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Virmani, T.; Sharma, A.; Chhabra, V.; Kumar, G.; Pathak, K.; Alhalmi, A. Potential Effect of DPP-4 Inhibitors Towards Hepatic Diseases and Associated Glucose Intolerance. Diabetes Metab. Syndr. Obes. 2022, 15, 1845–1864. [Google Scholar] [CrossRef]
- Sumida, Y.; Seko, Y.; Yoneda, M. Novel antidiabetic medications for non-alcoholic fatty liver disease with type 2 diabetes mellitus. Hepatol. Res. 2017, 47, 266–280. [Google Scholar] [CrossRef]
- Bica, C.; Sandu, C.; Suceveanu, A.I.; Sarbu, E.; Stoica, R.A.; Gherghiceanu, F.; Bohiltea, R.E.; Stefan, S.D.; Stoian, A.P. Non-alcoholic fatty liver disease: A major challenge in type 2 diabetes mellitus (Review). Exp. Ther. Med. 2020, 20, 2387–2391. [Google Scholar] [CrossRef]
- Miao, L.; Xu, J.; Targher, G.; Byrne, C.D.; Zheng, M.H. Old and new classes of glucose-lowering agents as treatments for non-alcoholic fatty liver disease: A narrative review. Clin. Mol. Hepatol. 2022, 28, 725–738. [Google Scholar] [CrossRef]
- Shih, Y.F.; Liu, C.J. Mother-to-infant transmission of hepatitis B virus: Challenges and perspectives. Hepatol. Int. 2017, 11, 481–484. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Before Propensity Score Matching | After Propensity Score Matching | ||||
|---|---|---|---|---|---|---|
| DPP-4 Inhibitors Use | Non-Use | p Value | DPP-4 Inhibitors Use | Non-Use | p Value | |
| (N = 5514) | (N = 22,557) | (N = 5514) | (N = 5514) | |||
| Age (Years) | ||||||
| 20–29 | 780 (14.15) | 3388 (15.02) | <0.0001 | 780 (14.15) | 779 (14.13) | - |
| 30–39 | 1679 (30.45) | 5571 (24.70) | 1679 (30.45) | 1679 (30.45) | ||
| 40–49 | 1789 (32.44) | 7365 (32.65) | 1789 (32.44) | 1789 (32.44) | ||
| 50–59 | 904 (16.39) | 4061 (18.00) | 904 (16.39) | 905 (16.41) | ||
| 60+ | 362 (6.57) | 2172 (9.63) | 362 (6.57) | 362 (6.57) | ||
| Mean ± SD | 51.53 ± 11.24 | 52.65 ± 12.32 | <0.0001 | 51.53 ± 11.24 | 51.50 ± 11.51 | - |
| Sex | ||||||
| Female | 1886 (34.20) | 9726 (43.12) | <0.0001 | 1886 (34.20) | 1886 (34.20) | - |
| Male | 3628 (65.80) | 12,831 (56.88) | 3628 (65.80) | 3628 (65.80) | ||
| HCV infection | ||||||
| No | 4981 (90.33) | 20,640 (91.50) | 0.0059 | 4981 (90.33) | 4981 (90.33) | - |
| Yes | 533 (9.67) | 1917 (8.50) | 533 (9.67) | 533 (9.67) | ||
| Cirrhosis | ||||||
| No | 4695 (85.15) | 19,772 (87.65) | <0.0001 | 4695 (85.15) | 4695 (85.15) | - |
| Yes | 819 (14.85) | 2785 (12.35) | 819 (14.85) | 819 (14.85) | ||
| Anti-virus drug | ||||||
| No | 4636 (84.08) | 19,867 (88.07) | <0.0001 | 4636 (84.08) | 4770 (86.51) | 0.0003 |
| Yes | 878 (15.92) | 2690 (11.92) | 878 (15.92) | 744 (13.49) | ||
| Insulin use | ||||||
| No | 3976 (72.11) | 21,270 (94.29) | <0.0001 | 3976 (72.11) | 5160 (93.58) | <0.0001 |
| Yes | 1538 (27.89) | 1287 (5.71) | 1538 (27.89) | 354 (6.42) | ||
| HCC | ||||||
| No | 5391 (97.77) | 21,848 (96.86) | 0.0003 | 5391 (97.77) | 5322 (96.52) | <0.0001 |
| Yes | 123 (2.23) | 709 (3.14) | 123 (2.23) | 192 (3.48) | ||
| Death | ||||||
| No | 5116 (92.78) | 20,167 (89.40) | <0.0001 | 5116 (92.78) | 4910 (89.05) | <0.0001 |
| Yes | 398 (7.22) | 2390 (10.60) | 398 (7.22) | 604 (10.95) | ||
| Baseline Characteristics | Before Propensity Score Matching | After Propensity Score Matching | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of Subjects (N = 28,071) | Number of HCC (N = 832) | Person-Years of Follow-Up | Incidence Rate † | p Value | Number of Subjects (N = 11,028) | Number of HCC (N = 315) | Person-Years of Follow-Up | Incidence Rate † | p Value | |
| DPP-4 inhibitors | ||||||||||
| No | 22,557 | 709 | 147,495 | 480.69 | 0.0003 | 5514 | 192 | 36,050 | 532.59 | <0.0001 |
| Yes | 5514 | 123 | 38,044 | 323.31 | 5514 | 123 | 38,044 | 323.31 | ||
| Age (Years) | ||||||||||
| 20–29 | 4168 | 21 | 28,598 | 73.43 | <0.0001 | 1559 | 10 | 10,728 | 93.21 | <0.0001 |
| 30–39 | 7250 | 128 | 49,054 | 260.94 | 3358 | 74 | 22,808 | 324.45 | ||
| 40–49 | 9154 | 287 | 61,187 | 469.05 | 3578 | 118 | 24,126 | 489.10 | ||
| 50–59 | 4965 | 254 | 32,220 | 788.33 | 1809 | 80 | 12,037 | 664.62 | ||
| 60+ | 2534 | 142 | 14,480 | 980.66 | 724 | 33 | 4394 | 751.02 | ||
| Sex | ||||||||||
| Female | 11,612 | 202 | 78,365 | 257.77 | <0.0001 | 3772 | 58 | 25,780 | 224.98 | <0.0001 |
| Male | 16,459 | 630 | 107,174 | 587.83 | 7256 | 257 | 48,313 | 531.95 | ||
| HCV infection | ||||||||||
| No | 25,621 | 607 | 170,419 | 356.18 | <0.0001 | 9962 | 221 | 67,355 | 328.11 | <0.0001 |
| Yes | 2450 | 225 | 15,119 | 1488.19 | 1066 | 94 | 6739 | 1394.87 | ||
| Cirrhosis | ||||||||||
| No | 24,467 | 178 | 166,015 | 107.22 | <0.0001 | 9390 | 60 | 64,571 | 92.92 | <0.0001 |
| Yes | 3604 | 654 | 19,523 | 3349.89 | 1638 | 255 | 9523 | 2677.73 | ||
| Anti-virus drug | ||||||||||
| No | 24,503 | 411 | 163,978 | 250.64 | <0.0001 | 9406 | 140 | 63,909 | 219.06 | <0.0001 |
| Yes | 3568 | 421 | 21,561 | 1952.60 | 1622 | 175 | 10,185 | 1718.21 | ||
| Insulin | ||||||||||
| No | 25,246 | 705 | 168,330 | 418.82 | <0.0001 | 9136 | 243 | 61,845 | 392.92 | <0.0001 |
| Yes | 2825 | 127 | 17,209 | 737.99 | 1892 | 72 | 12,249 | 587.80 | ||
| Characteristics | Before Propensity Score Matching | After Propensity Score Matching | ||
|---|---|---|---|---|
| Crude HR (95% CI) | Adjusted HR * (95% CI) | Crude HR (95% CI) | Adjusted HR * (95% CI) | |
| DPP-4 inhibitors | ||||
| No | Ref | Ref | Ref | Ref |
| Yes | 0.68 (0.56–0.82) | 0.53 (0.44–0.65) | 0.61 (0.49–0.76) | 0.53 (0.42–0.68) |
| Age (Years) | ||||
| 20–29 | Ref | Ref | Ref | Ref |
| 30–39 | 3.55 (2.24–5.63) | 2.43 (1.53–3.86) | 3.48 (1.80–6.74) | 2.76 (1.42–5.34) |
| 40–49 | 6.38 (4.09–9.93) | 4.01 (2.57–6.25) | 5.26 (2.76–10.02) | 3.90 (2.04–7.46) |
| 50–59 | 10.72 (6.87–16.72) | 5.69 (3.64–8.91) | 7.15 (3.71–13.80) | 5.26 (2.71–10.20) |
| 60+ | 13.25 (8.38–20.95) | 7.24 (4.56–11.50) | 8.04 (3.96–16.31) | 7.32 (3.58–14.96) |
| Sex | ||||
| Female | Ref | Ref | Ref | Ref |
| Male | 2.28(1.95–2.67) | 1.88 (1.60–2.22) | 2.37 (1.78–3.15) | 2.13 (1.59–2.85) |
| HCV infection | ||||
| No | Ref | Ref | Ref | Ref |
| Yes | 4.18 (3.59–4.87) | 2.11 (1.79–2.48) | 4.26 (3.35–5.43) | 2.25 (1.74–2.92) |
| Cirrhosis | ||||
| No | Ref | Ref | Ref | Ref |
| Yes | 31.51 (26.70–37.20) | 16.82 (13.97–20.26) | 29.08 (21.95–38.54) | 15.78 (11.53–21.59) |
| Anti-virus drug | ||||
| No | Ref | Ref | Ref | Ref |
| Yes | 7.80 (6.81–8.94) | 2.37 (2.03–2.76) | 7.87 (6.30–9.83) | 2.61 (2.03–3.35) |
| Insulin use | ||||
| No | Ref | Ref | Ref | Ref |
| Yes | 1.78 (1.47–2.15) | 0.88 (0.72–1.07) | 1.51 (1.16–1.96) | 0.86 (0.65–1.14) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, T.-I.; Lee, F.-J.; Hsu, W.-L.; Chen, Y.-C.; Chen, M. Association of Dipeptidyl Peptidase-4 Inhibitors Use with Reduced Risk of Hepatocellular Carcinoma in Type 2 Diabetes Patients with Chronic HBV Infection. Cancers 2023, 15, 1148. https://doi.org/10.3390/cancers15041148
Chen T-I, Lee F-J, Hsu W-L, Chen Y-C, Chen M. Association of Dipeptidyl Peptidase-4 Inhibitors Use with Reduced Risk of Hepatocellular Carcinoma in Type 2 Diabetes Patients with Chronic HBV Infection. Cancers. 2023; 15(4):1148. https://doi.org/10.3390/cancers15041148
Chicago/Turabian StyleChen, Tzu-I, Fu-Jen Lee, Wan-Lun Hsu, Yong-Chen Chen, and Mingchih Chen. 2023. "Association of Dipeptidyl Peptidase-4 Inhibitors Use with Reduced Risk of Hepatocellular Carcinoma in Type 2 Diabetes Patients with Chronic HBV Infection" Cancers 15, no. 4: 1148. https://doi.org/10.3390/cancers15041148
APA StyleChen, T.-I., Lee, F.-J., Hsu, W.-L., Chen, Y.-C., & Chen, M. (2023). Association of Dipeptidyl Peptidase-4 Inhibitors Use with Reduced Risk of Hepatocellular Carcinoma in Type 2 Diabetes Patients with Chronic HBV Infection. Cancers, 15(4), 1148. https://doi.org/10.3390/cancers15041148