
Patients with Very High Risk of Cardiovascular Adverse Events during Carfilzomib Therapy: Prevention and Management of Events in a Single Center Experience

 , ,
, ,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Cardiovascular Assessments
2.3. Cardiovascular Adverse Events Definition
2.4. Statistical Analysis
3. Results
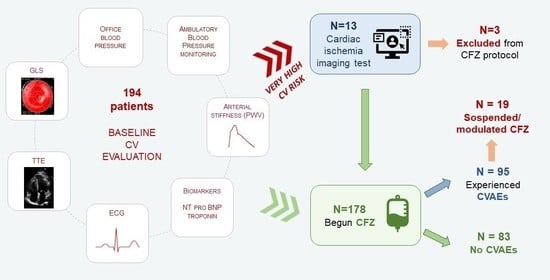
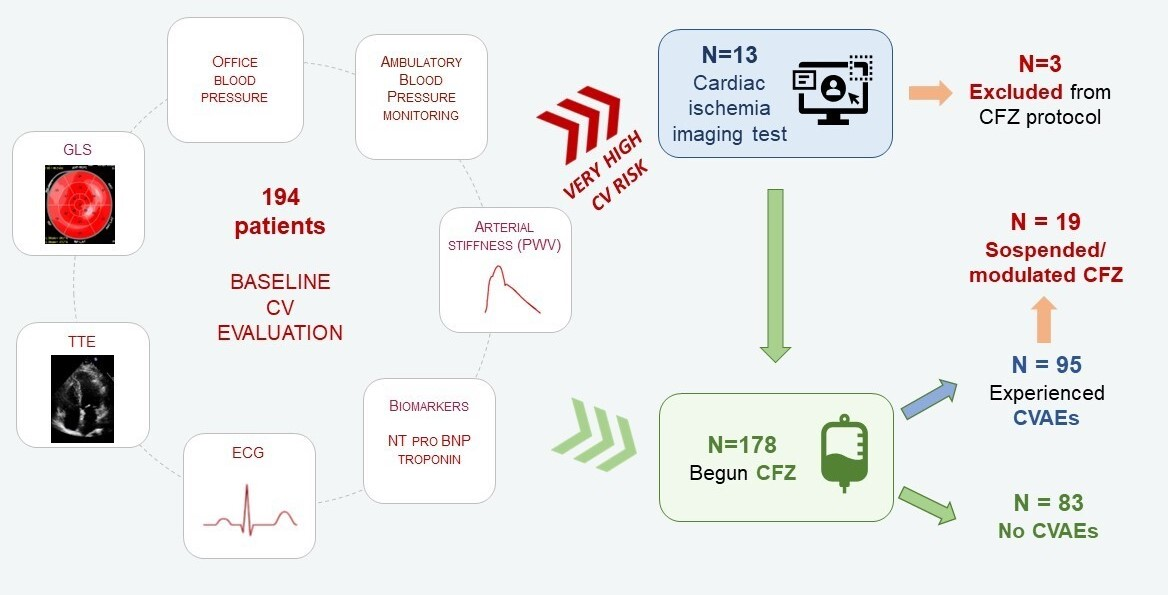
3.1. Baseline Cardiovascular Risk Evaluation
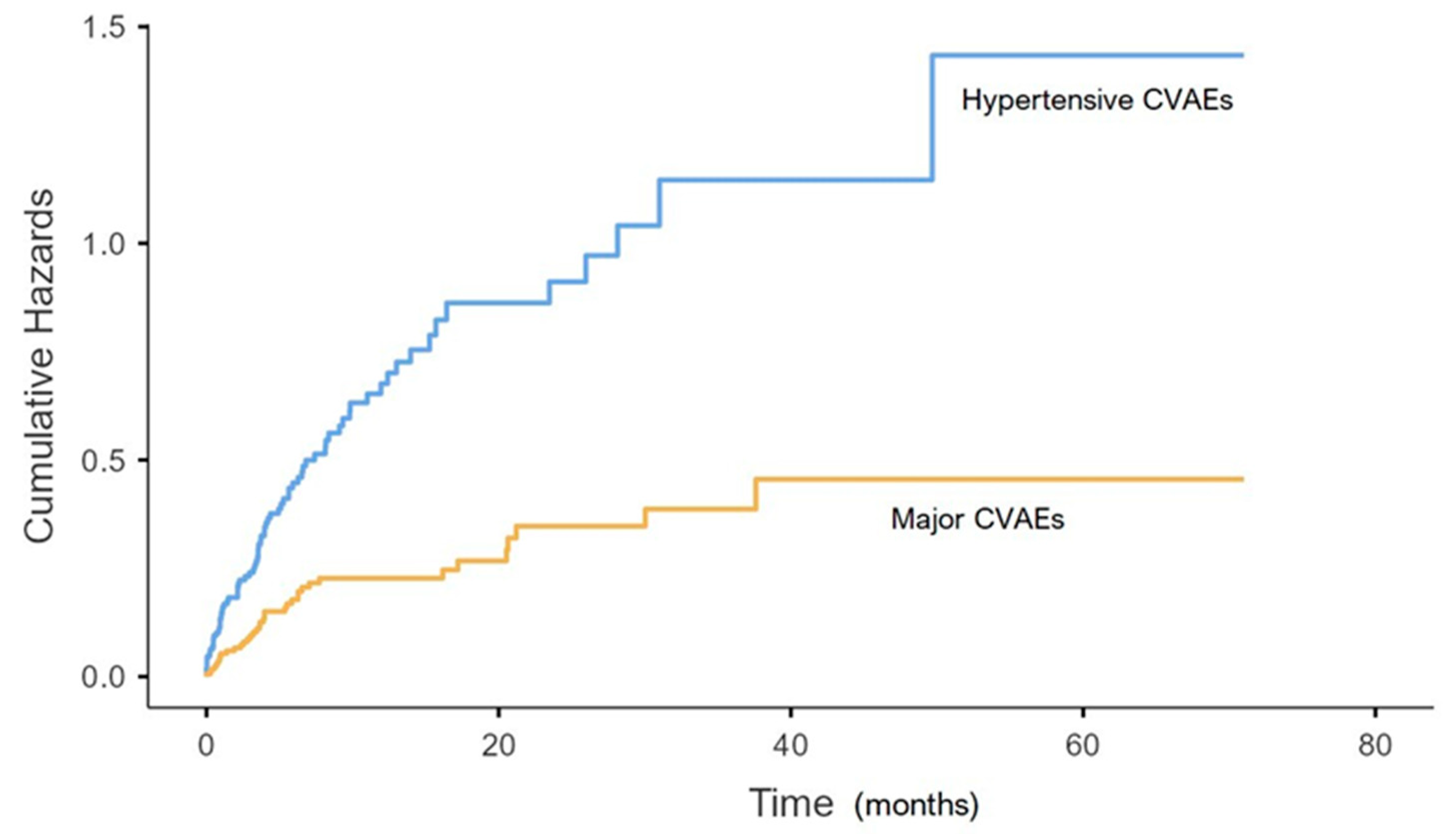
3.2. CVAES Incidence and Management
3.2.1. Hypertension-Related CVAEs
3.2.2. Major CVAES
3.2.3. Cardiotoxicity on Echocardiography
4. Discussion
4.1. Prevention of CVAEs
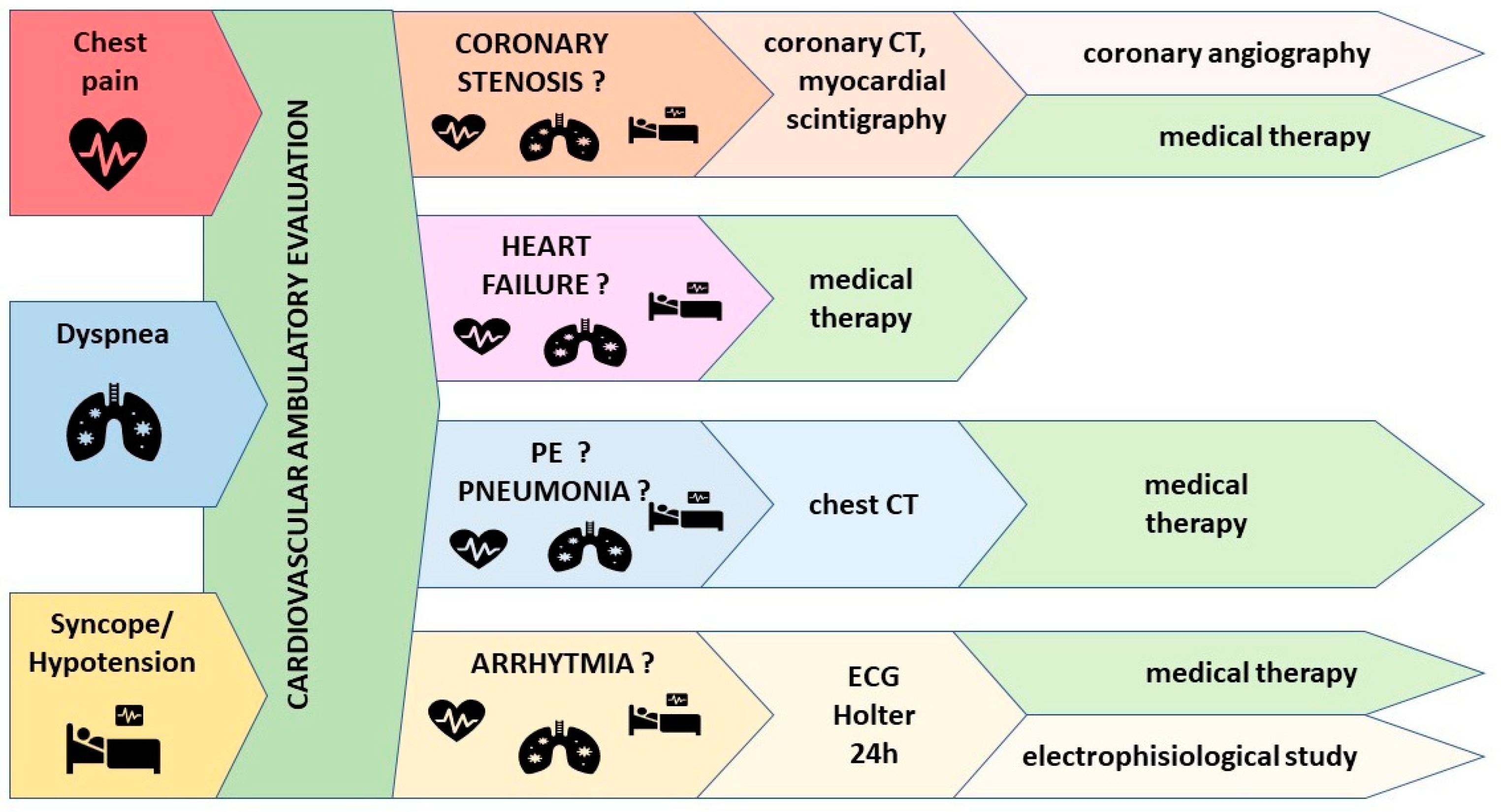
4.2. Management of CVAEs
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Details on Cardiovascular Assessments
Appendix B
Cardiovascular Adverse Events Definitions
References
- Yee, A.J. The Role of Carfilzomib in Relapsed/Refractory Multiple Myeloma. Ther. Adv. Hematol. 2021, 12, 20406207211019612. [Google Scholar] [CrossRef] [PubMed]
- Franken, B.; van de Donk, N.W.C.J.; Cloos, J.C.; Zweegman, S.; Lokhorst, H.M. A Clinical Update on the Role of Carfilzomib in the Treatment of Relapsed or Refractory Multiple Myeloma. Ther. Adv. Hematol. 2016, 7, 330–344. [Google Scholar] [CrossRef] [PubMed]
- Steiner, R.E.; Manasanch, E.E. Carfilzomib Boosted Combination Therapy for Relapsed Multiple Myeloma. OncoTargets Ther. 2017, 10, 895–907. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Dasgupta, S.; Gong, Y.; AShah, U.; Fradley, M.G.; Cheng, R.K.; Roy, B.; Guha, A. Cardiotoxicity as an Adverse Effect of Immunomodulatory Drugs and Proteasome Inhibitors in Multiple Myeloma: A Network Meta-Analysis of Randomized Clinical Trials. Hematol. Oncol. 2021, 40, 233–242. [Google Scholar] [CrossRef]
- Imtiaz, H.; Khan, M.; Ehsan, H.; Wahab, A.; Rafae, A.; Khan, A.Y.; Jamil, A.; Sana, M.K.; Jamal, A.; Ali, T.J.; et al. Efficacy and Toxicity Profile of Carfilzomib-Based Regimens for Treatment of Newly Diagnosed Multiple Myeloma: A Systematic Review. Onco. Targets Ther. 2021, 14, 4941–4960. [Google Scholar] [CrossRef]
- Zhai, Y.; Ye, X.; Hu, F.; Xu, J.; Guo, X.; Cao, Y.; Lin, Z.; Zhou, X.; Guo, Z.; He, J. Cardiovascular Toxicity of Carfilzomib: The Real-World Evidence Based on the Adverse Event Reporting System Database of the FDA, the United States. Front. Cardiovasc. Med. 2021, 8, 5466. [Google Scholar] [CrossRef]
- Muchtar, E.; Gertz, M.A.; Magen, H. A Practical Review on Carfilzomib in Multiple Myeloma. Eur. J. Haematol. 2016, 96, 564–577. [Google Scholar] [CrossRef]
- Stewart, A.K.; Rajkumar, S.V.; Dimopoulos, M.A.; Masszi, T.; Špička, I.; Oriol, A.; Hájek, R.; Rosiñol, L.; Siegel, D.S.; Mihaylov, G.G.; et al. Carfilzomib, Lenalidomide, and Dexamethasone for Relapsed Multiple Myeloma. N. Engl. J. Med. 2015, 372, 142–152. [Google Scholar] [CrossRef]
- A Dimopoulos, M.; Moreau, P.; Palumbo, A.; Joshua, D.; Pour, L.; Hájek, R.; Facon, T.; Ludwig, H.; Oriol, A.; Goldschmidt, H.; et al. Carfilzomib and dexamethasone versus bortezomib and dexamethasone for patients with relapsed or refractory multiple myeloma (ENDEAVOR): A randomised, phase 3, open-label, multicentre study. Lancet. Oncol. 2016, 17, 27–38. [Google Scholar] [CrossRef]
- Waxman, A.J.; Clasen, S.; Hwang, W.T.; Garfall, A.; Vogl, D.T.; Carver, J.; O’Quinn, R.; Cohen, A.D.; Stadtmauer, E.A.; Ky, B.; et al. Carfilzomib-Associated Cardiovascular Adverse Events a Systematic Review and Meta-Analysis. JAMA Oncol. 2018, 4, 4519. [Google Scholar] [CrossRef]
- Bringhen, S.; Milan, A.; Ferri, C.; Wäsch, R.; Gay, F.; Larocca, A.; Salvini, M.; Terpos, E.; Goldschmidt, H.; Cavo, M.; et al. Cardiovascular Adverse Events in Modern Myeloma Therapy—Incidence and Risks. A Review from the European Myeloma Network (EMN) and Italian Society of Arterial Hypertension (SIIA). Haematologica 2018, 103, 1422–1432. [Google Scholar] [CrossRef] [PubMed]
- Milan, A.; Puglisi, E.; Ferrari, L.; Bruno, G.; Losano, I.; Veglio, F. Arterial Hypertension and Cancer. Int. J. Cancer 2014, 134, 2269–2277. [Google Scholar] [CrossRef] [PubMed]
- Chen-Scarabelli, C.; Corsetti, G.; Pasini, E.; Dioguardi, F.S.; Sahni, G.; Narula, J.; Gavazzoni, M.; Patel, H.; Saravolatz, L.; Knight, R.; et al. Spasmogenic Effects of the Proteasome Inhibitor Carfilzomib on Coronary Resistance, Vascular Tone and Reactivity. eBioMedicine 2017, 21, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Heckmann, M.B.; Doroudgar, S.; Katus, H.A.; Lehmann, L.H. Cardiovascular Adverse Events in Multiple Myeloma Patients. J. Thorac. Dis. 2018, 10, S4296–S4305. [Google Scholar] [CrossRef]
- Cornell, R.F.; Ky, B.; Weiss, B.M.; Dahm, C.N.; Gupta, D.K.; Du, L.; Carver, J.R.; Cohen, A.D.; Engelhardt, B.G.; Garfall, A.L.; et al. Prospective Study of Cardiac Events during Proteasome Inhibitor Therapy for Relapsed Multiple Myeloma. J. Clin. Oncol. Am. Soc. Clin. Oncol. 2019, 37, 1946–1955. [Google Scholar] [CrossRef]
- Bishnoi, R.; Xie, Z.; Shah, C.; Bian, J.; Murthy, H.S.; Wingard, J.R.; Farhadfar, N. Real-World Experience of Carfilzomib-Associated Cardiovascular Adverse Events: SEER-Medicare Data Set Analysis. Cancer Med. 2021, 10, 70–78. [Google Scholar] [CrossRef]
- Astarita, A.; Mingrone, G.; Airale, L.; Vallelonga, F.; Covella, M.; Catarinella, C.; Cesareo, M.; Bruno, G.; Leone, D.; Giordana, C.; et al. Multiple Myeloma Patients Undergoing Carfilzomib: Development and Validation of a Risk Score for Cardiovascular Adverse Events Prediction. Cancers 2021, 13, 1631. [Google Scholar] [CrossRef]
- Mingrone, G.; Astarita, A.; Airale, L.; Maffei, I.; Cesareo, M.; Crea, T.; Bruno, G.; Leone, D.; Avenatti, E.; Catarinella, C.; et al. Effects of Carfilzomib Therapy on Left Ventricular Function in Multiple Myeloma Patients. Front. Cardiovasc. Med. 2021, 8, 5678. [Google Scholar] [CrossRef]
- Iannaccone, A.; Bruno, G.; Ravera, A.; Gay, F.; Salvini, M.; Bringhen, S.; Sabia, L.; Avenatti, E.; Veglio, F.; Milan, A. Evaluation of Cardiovascular Toxicity Associated with Treatments Containing Proteasome Inhibitors in Multiple Myeloma Therapy. High Blood Press Cardiovasc. Prev. 2018, 25, 209–218. [Google Scholar] [CrossRef]
- Edvardsen, T.; Asch, F.M.; Davidson, B.; Delgado, V.; DeMaria, A.; Dilsizian, V.; Gaemperli, O.; Garcia, M.J.; Kamp, O.; Lee, D.C.; et al. Non-Invasive Imaging in Coronary Syndromes: Recommendations of the European Association of Cardiovascular Imaging and the American Society of Echocardiography, in Collaboration with the American Society of Nuclear Cardiology, Society of Cardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance. Eur. Heart. J. Cardiovasc. Imaging 2022, 23, e6–e33. [Google Scholar] [CrossRef]
- Almeida, A.G.; Carpenter, J.P.; Cameli, M.; Donal, E.; Dweck, M.R.; Flachskampf, F.A.; Maceira, A.M.; Muraru, D.; Neglia, D.; Pasquet, A.; et al. Multimodality Imaging of Myocardial Viability: An Expert Consensus Document from the European Association of Cardiovascular Imaging (EACVI). Eur. Heart J. Cardiovasc. Imaging 2021, 22, E97–E125. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.K.; de Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.S.; Protogerou, A.D.; et al. Expert Consensus Document on the Measurement of Aortic Stiffness in Daily Practice Using Carotid-Femoral Pulse Wave Velocity. J. Hypertens. 2012, 30, 445–448. [Google Scholar] [CrossRef]
- Bruno, G.; Bringhen, S.; Maffei, I.; Iannaccone, A.; Crea, T.; Ravera, A.; Astarita, A.; Vallelonga, F.; Salvini, M.; Gay, F.; et al. Cardiovascular Organ Damage and Blood Pressure Levels Predict Adverse Events in Multiple Myeloma Patients Undergoing Carfilzomib Therapy. Cancers 2019, 11, 622. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Victor, M.A.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Čelutkienė, J.; Pudil, R.; López-Fernández, T.; Grapsa, J.; Nihoyannopoulos, P.; Bergler-Klein, J.; Cohen-Solal, A.; Farmakis, D.; Tocchetti, C.G.; von Haehling, S.; et al. Role of Cardiovascular Imaging in Cancer Patients Receiving Cardiotoxic Therapies: A Position Statement on Behalf of the Heart Failure Association (HFA), the European Association of Cardiovascular Imaging (EACVI) and the Cardio-Oncology Council of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2020, 22, 1504–1524. [Google Scholar] [CrossRef]
- Voigt, J.-U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a Common Standard for 2D Speckle Tracking Echocardiography: Consensus Document of the EACVI/ASE/Industry Task Force to Standardize Deformation Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 183–193. [Google Scholar] [CrossRef]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on Cardio-Oncology Developed in Collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Cancer Therapy Evaluation Program (CTEP): Common Terminology Criteria for Adverse Events (CTCAE) v.5.0. Cancer Ther. Eval. Progr. 2020. Update. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf (accessed on 1 March 2020).
- Lyon, A.R.; Dent, S.; Stanway, S.; Earl, H.; Brezden-Masley, C.; Cohen-Solal, A.; Tocchetti, C.G.; Moslehi, J.J.; Groarke, J.D.; Bergler-Klein, J.; et al. Baseline Cardiovascular Risk Assessment in Cancer Patients Scheduled to Receive Cardiotoxic Cancer Therapies: A Position Statement and New Risk Assessment Tools from the Cardio-Oncology Study Group of the Heart Failure Association of the European Society of Cardiology in Collaboration with the International Cardio-Oncology Society. Eur. J. Heart Fail. 2020, 22, 1945–1960. [Google Scholar] [CrossRef]
- Milan, A.; Bruno, G.; Maffei, I.; Iannaccone, A.; Ravera, A.; Schiavone, D.; Veglio, F. Arterial Hypertension and Multiple Myeloma: Physiopathology and Cardiovascular Risk and ‘Practical’ Indications in Patients Receiving Carfilzomib. Curr. Hypertens. Rev. 2018, 15, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Bringhen, S.; Milan, A.; D’Agostino, M.; Ferri, C.; Wäsch, R.; Gay, F.; Larocca, A.; Offidani, M.; Zweegman, S.; Terpos, E.; et al. Prevention, Monitoring and Treatment of Cardiovascular Adverse Events in Myeloma Patients Receiving Carfilzomib A Consensus Paper by the European Myeloma Network and the Italian Society of Arterial Hypertension. J. Intern. Med. 2019, 286, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Mingrone, G.; Coletti Moia, E.; Delsignore, E.; Demicheli, G.; Destefanis, P.; Forno, D.; Giglio Tos, G.; Luciano, A.; Pinna, G.; Ravera, L.; et al. Risk Stratification and Management of Arterial Hypertension and Cardiovascular Adverse Events Related to Cancer Treatments: An Oncology Network from Piedmont and Aosta Valley (North-Western Italy) Consensus Document. Hearts 2021, 2, 61–73. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| General Characteristics | Population n = 194 |
|---|---|
| Age, years | 67.1 ± 8.4 |
| Male sex, n (%) | 110 (56.7) |
| Weight, kg | 73.4 ± 14.2 |
| Height, cm | 163.1 ± 10.4 |
| BSA, m2 | 1.8 ± 0.2 |
| BMI, kg/m2 | 27.5 ± 4.4 |
| Cardiovascular risk factors, n (%) | |
| Tobacco use (past/current) | 98 (50.5) |
| Arterial hypertension (history) | 100 (51.5) |
| Obesity (BMI > 30 kg/m2) | 63 (32.5) |
| Diabetes mellitus | 21 (10.8) |
| Chronic kidney disease | 29 (14.9) |
| Dyslipidemia | 27 (13.9) |
| Previous cardiovascular events, n (%) | |
| Previous AF | 8 (4.1) |
| Previous stroke | 4 (2.1) |
| Previous coronary artery disease | 6 (3.1) |
| Anti-hypertensive drugs *, n (%) | 95 (48.9) |
| Beta-blockers | 40 (20.6) |
| ACE-inhibitors/angiotensin receptor blockers | 65 (33.5) |
| Thiazide diuretics/Loop diuretics | 36 (18.6) |
| Mineralcorticoid receptor antagonists | 6 (3.1) |
| Calcium channel blockers | 31 (16) |
| Oncological history | |
| MM duration, years | 4.1 [1.6–6.9] |
| Relapsed/Refractory MM, n (%) | 175 (90.2) |
| Newly diagnosed MM, n (%) | 19 (9.8) |
| Previous therapy * | |
| Previous lines of therapy, n | 1 [1; 3] |
| Anthracyclines, n (%) | 45 (23.2) |
| Alkylating agents, n (%) | 126 (64.9) |
| Immunomodulating agents, n (%) | 131 (67.5) |
| Bortezomib, n (%) | 136 (70.1) |
| Auto-transplantation, n (%) | 126 (64.9) |
| Baseline Parameters | Global Population n = 181 | Very-High-Risk Population n = 13 | p Value |
|---|---|---|---|
| Office BP values | |||
| SBP, mmHg | 128.8 ± 17.6 | 139.4 ± 17.3 | 0.04 |
| DBP, mmHg | 76.5 ± 11.4 | 79.4 ± 11.9 | 0.38 |
| ABPM * | |||
| Daytime SBP, mmHg | 125.5 ± 13.2 | 126.5 ± 15.1 | 0.82 |
| Daytime DBP, mmHg | 74.7 ± 9.2 | 71.4 ± 8.9 | 0.25 |
| 24 h SBP, mmHg | 121.2 ± 12.5 | 123.2 ± 16 | 0.64 |
| 24 h DBP, mmHg | 71.3 ± 8.2 | 68.9 ± 9.3 | 0.36 |
| BP variation, mmHg | 9.3 ± 3.5 | 9.6 ± 3.1 | 0.83 |
| Transthoracic echocardiography | |||
| Left ventricular mass, g/m2 | 87 ± 19.8 | 123.6 ± 40.4 | <0.001 |
| LVEF, % | 62.5 ± 6.8 | 55.1 ± 9.3 | <0.001 |
| GLS †, % | −21.6 ± 2.5 | −18.2 ± 2.8 | <0.001 |
| Arterial stiffness | |||
| PWV ‡, m/s | 8.1 ± 1.9 | 9.9 ± 1.6 | 0.006 |
| CVAEs risk score × | 42.2 [32.7; 58.9] | 60.1 [51.7; 75.3] | 0.009 |
| Cardiovascular Adverse Events * | Population, n = 178 |
|---|---|
| Total CVAEs (%) | 95 (48.7) |
| Events related to arterial hypertension (%) | 82 (46) |
| New onset or worsening of arterial hypertension (%) | 69 (38.8) |
| Arterial hypertension before Carfilzomib infusion: (%) | 42 (23.6) |
| 33 (18.5) 19 (10.7) |
| Arterial hypertension after Carfilzomib infusion (%) | 23 (12.9) |
| Uncontrolled arterial hypertension (>180/100) with symptoms (%) | 6 (3.4) |
| Hypertensive emergency (%) | 0 (0) |
| Major cardiovascular events (%) | 37 (20.8) |
| Dyspnea (%) | 7 (3.9) |
| Arrhythmia (%) | 12 (6.7) |
| Severe hypotension (%) | 6 (3.4) |
| Heart failure (%) | 11 (6.2) |
| Typical chest pain (%) | 8 (4.5) |
| STEMI (%) | 1 (0.6) |
| NSTEMI (%) | 7 (3.9) |
| Syncope (%) | 1 (0.6) |
| Sudden cardiac death (%) | 1 (0.6) |
| Both major and hypertensive events (%) | 23 (12.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mingrone, G.; Astarita, A.; Colomba, A.; Catarinella, C.; Cesareo, M.; Airale, L.; Paladino, A.; Leone, D.; Vallelonga, F.; Bringhen, S.; et al. Patients with Very High Risk of Cardiovascular Adverse Events during Carfilzomib Therapy: Prevention and Management of Events in a Single Center Experience. Cancers 2023, 15, 1149. https://doi.org/10.3390/cancers15041149
Mingrone G, Astarita A, Colomba A, Catarinella C, Cesareo M, Airale L, Paladino A, Leone D, Vallelonga F, Bringhen S, et al. Patients with Very High Risk of Cardiovascular Adverse Events during Carfilzomib Therapy: Prevention and Management of Events in a Single Center Experience. Cancers. 2023; 15(4):1149. https://doi.org/10.3390/cancers15041149
Chicago/Turabian StyleMingrone, Giulia, Anna Astarita, Anna Colomba, Cinzia Catarinella, Marco Cesareo, Lorenzo Airale, Arianna Paladino, Dario Leone, Fabrizio Vallelonga, Sara Bringhen, and et al. 2023. "Patients with Very High Risk of Cardiovascular Adverse Events during Carfilzomib Therapy: Prevention and Management of Events in a Single Center Experience" Cancers 15, no. 4: 1149. https://doi.org/10.3390/cancers15041149
APA StyleMingrone, G., Astarita, A., Colomba, A., Catarinella, C., Cesareo, M., Airale, L., Paladino, A., Leone, D., Vallelonga, F., Bringhen, S., Gay, F., Veglio, F., & Milan, A. (2023). Patients with Very High Risk of Cardiovascular Adverse Events during Carfilzomib Therapy: Prevention and Management of Events in a Single Center Experience. Cancers, 15(4), 1149. https://doi.org/10.3390/cancers15041149