
Barriers to Breast Cancer-Screening Adherence in Vulnerable Populations


 ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
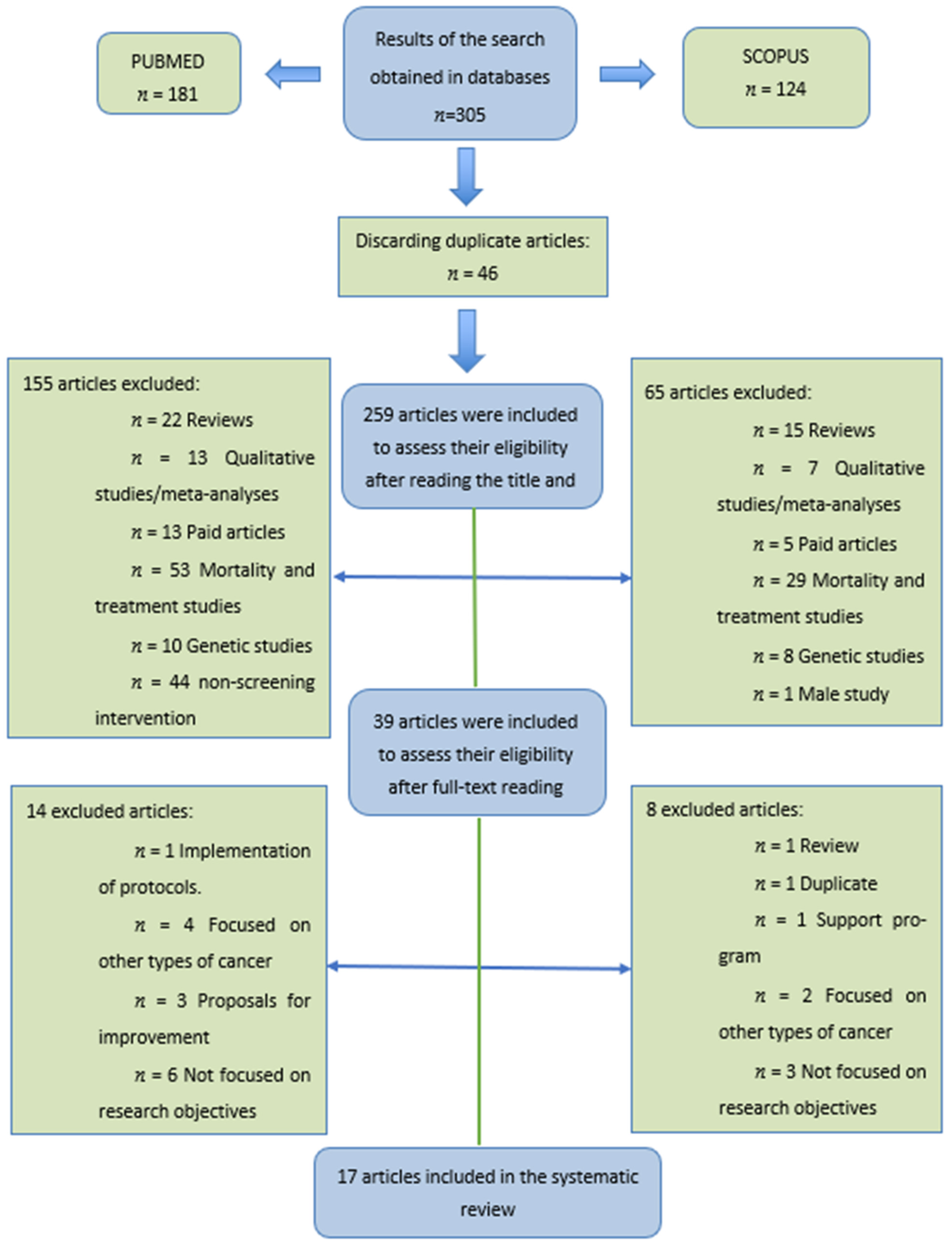
2. Materials and Methods
3. Results
3.1. Adherence to Breast Cancer–Screening Programs
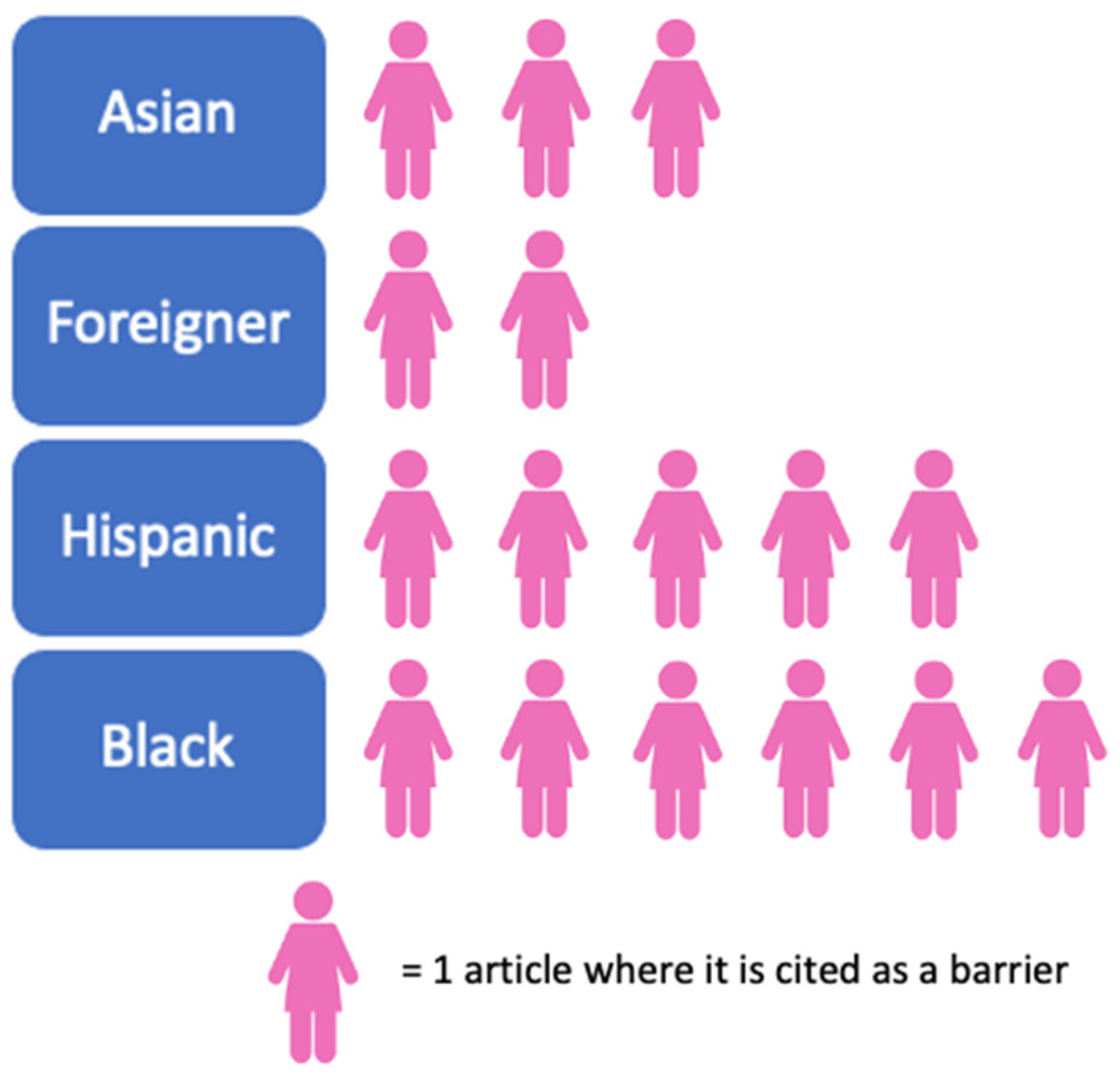
3.2. Race and/or Ethnicity
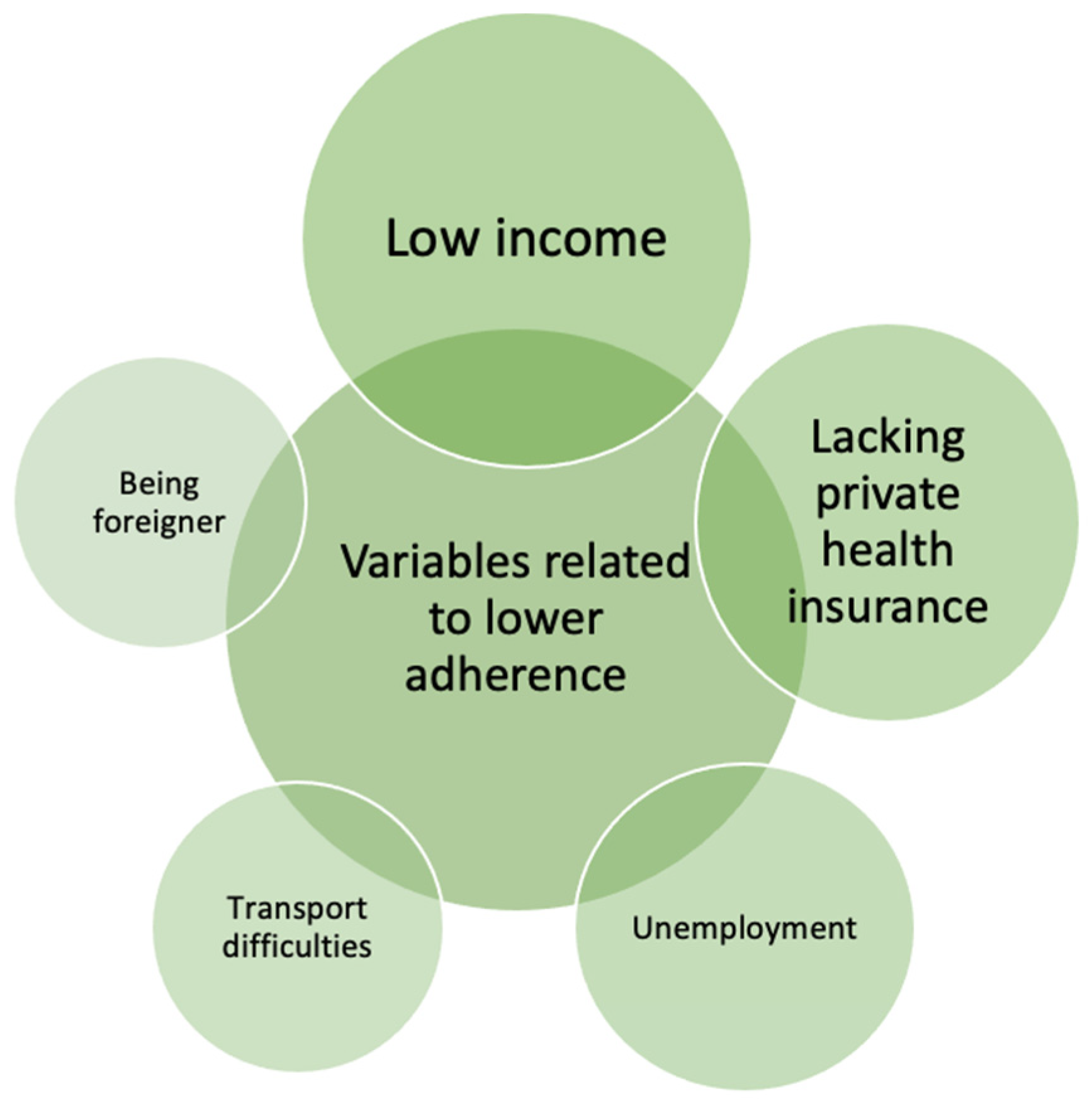
3.3. Socioeconomic Level, Lack of Resources and Lack of Private Health Insurance
3.4. Family and Individual Factors
3.5. Health Information Gap and Medical Mistrust
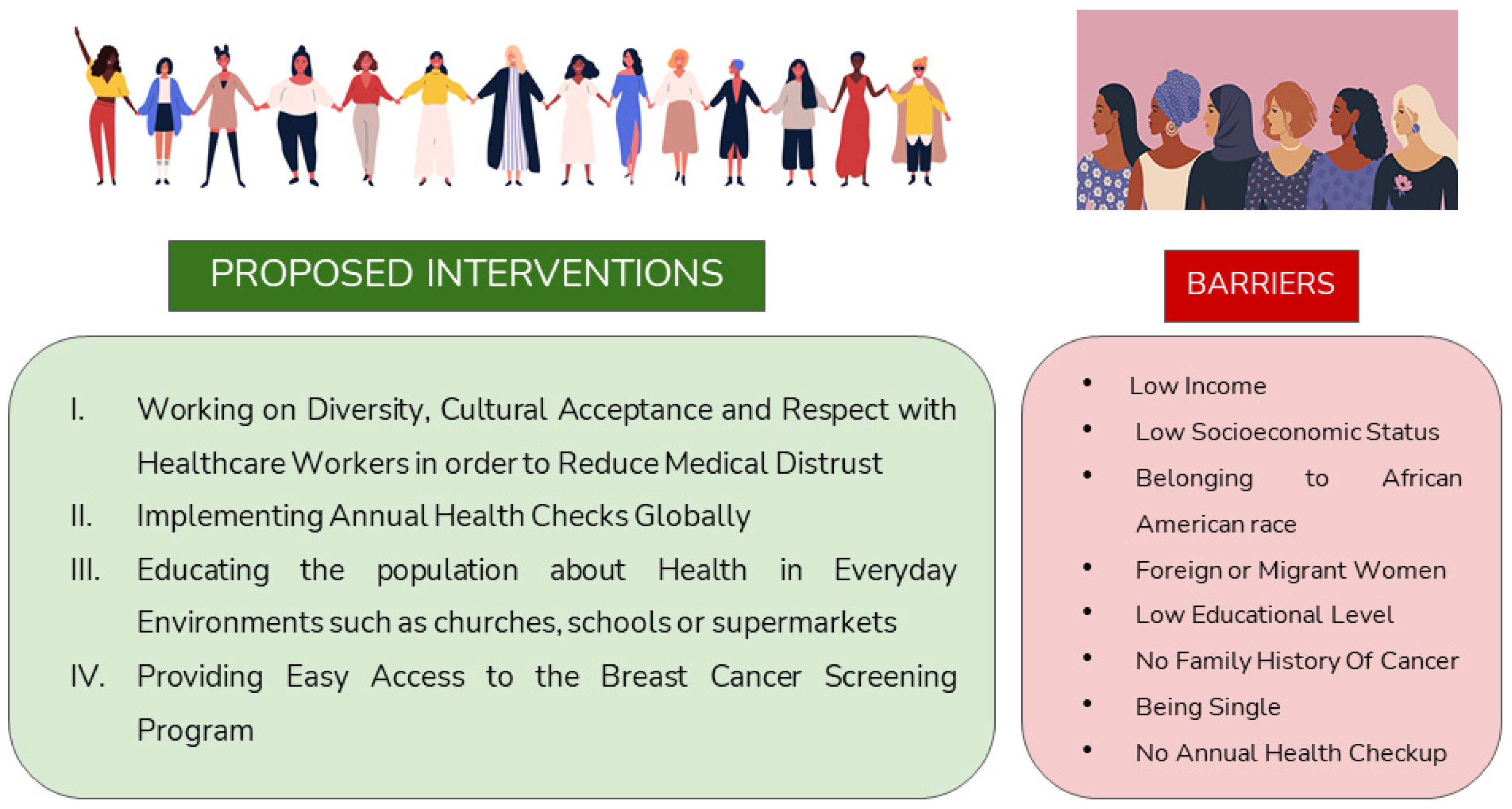
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/es/news-room/fact-sheets/detail/breast-cancer (accessed on 26 March 2021).
- GEICAM association-Breast Cancer Research. Available online: https://www.geicam.org/cancer-de-mama/el-cancer-de-mama-se-puede-prevenir/incidencia-del-cancer-de-mama (accessed on 15 December 2021).
- SEOM (Spanish Society of Medical Oncology). Breast Cancer. Available online: https://seom.org/info-sobre-el-cancer/cancer-de-mama (accessed on 15 December 2021).
- Saz-Parkinson, Z.; Monteagudo-Piqueras, O.; Granados-Ortega, J.; Martínez-Mondéjar, E.; Labrador-Cañadas, M.V. “European Commission Initiative On Breast Cancer”: Recomendaciones Seleccionadas De Cribado De Cáncer De Mama De Las Guías Europeas. Rev. Esp. Salud Pública 2020, 94, e1–e10. [Google Scholar]
- Wu, Z.; Liu, Y.; Li, X.; Song, B.; Ni, C.; Lin, F. Factors associated with breast cancer screening participation among women in mainland China: A systematic review. BMJ Open 2019, 9, e028705. [Google Scholar] [CrossRef]
- Miller, B.C.; Bowers, J.M.; Payne, J.B.; Moyer, A. Barriers to mammography screening among racial and ethnic minority women. Soc. Sci. Med. 2019, 239, 112494. [Google Scholar] [CrossRef] [PubMed]
- Adunlin, G.; Cyrus, J.W.; Asare, M.; Sabik, L.M. Barriers and Facilitators to Breast and Cervical Cancer Screening Among Immigrants in the United States. J. Immigr. Minor. Health 2019, 21, 606–658. [Google Scholar] [CrossRef] [PubMed]
- Oh, K.M.; Taylor, K.L.; Jacobsen, K.H. Breast Cancer Screening Among Korean Americans: A Systematic Review. J. Community Health 2017, 42, 324–332. [Google Scholar] [CrossRef]
- De Cuevas, R.M.A.; Saini, P.; Roberts, D.; Beaver, K.; Chandrashekar, M.; Jain, A.; Kotas, E.; Tahir., N.; Ahmed, S.; Brown, S.L. A systematic review of barriers and enablers to South Asian women’s attendance for asymptomatic screening of breast and cervical cancers in emigrant countries. BMJ Open 2018, 8, e020892. [Google Scholar] [CrossRef]
- Pellom, S.T.; Arnold, T.; Williams, M.; Brown, V.L.; Samuels, A.D. Examining breast cancer disparities in African Americans with suggestions for policy. Cancer Causes Control 2020, 31, 795–800. [Google Scholar] [CrossRef]
- Advani, P.; Advani, S.; Nayak, P.; VonVille, H.M.; Diamond, P.; Burnett, J.; Brewster, A.M.; Vernon, S.W. Racial/ethnic disparities in use of surveillance mammogram among breast cancer survivors: A systematic review. J. Cancer Surviv. 2022, 16, 514–530. [Google Scholar] [CrossRef]
- Zavala, V.A.; Bracci, P.M.; Carethers, J.M.; Carvajal-Carmona, L.; Coggins, N.B.; Cruz-Correa, M.R.; Davis, M.; de Smith, A.J.; Dutil, J.; Figueiredo, J.C.; et al. Cancer health disparities in racial/ethnic minorities in the United States. Br. J. Cancer 2021, 124, 315–332. [Google Scholar] [CrossRef]
- Rollet, Q.; Tron, L.; de Mil, R.; Launoy, G.; Guillaume, É. Contextual factors associated with cancer screening uptake: A systematic review of observational studies. Prev. Med. 2021, 150, 106692. [Google Scholar] [CrossRef]
- Queiro Verdes, M.T.; España Fernández, S.; Cerdá Mota, T. Información a Usuarias Sobre el Cribado de Cáncer en la Mujer: Evaluación de la Situación Actual y Establecimiento de Estándares de Información Basada en la Evidencia; Ministerio de Ciencia e Innovación: Madrid, Spain, 2009.
- Haas, J.S.; Hill, D.A.; Wellman, R.D.; Hubbard, R.A.; Lee, C.I.; Wernli, K.J.; Stout, N.K.; Tosteson, A.N.A.; Henderson, L.M.; Alford-Teaster, J.A.; et al. Disparities in the Use of Screening Magnetic Resonance Imaging of the Breast in Community Practice by Race, Ethnicity, and Socioeconomic Status. Cancer 2016, 122, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Elewonibi, B.R.; Thierry, A.D.; Miranda, P.Y. Examining Mammography Use by Breast Cancer Risk, Race, Nativity, and Socioeconomic Status. J. Immigr. Minor. Health 2018, 20, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Shon, E.J.; Townsend, A.L. Predictors of never having a mammogram among Chinese, Vietnamese, and Korean immigrant women in the U.S. PLoS ONE 2019, 14, e0224505. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.M.; O’Meara, E.S.; Haas, J.S.; Lee, C.I.; Kerlikowske, K.; Sprague, B.L.; Alford-Teaster, J.; Onega, T. The Role of Social Determinants of Health in Self-Reported Access to Health Care among Women Undergoing Screening Mammography. J. Women’s Health 2020, 29, 1437–1446. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.I.; Zhu, W.; Onega, T.; Henderson, L.M.; Kerlikowske, K.; Sprague, B.L.; Rauscher, G.H.; O’Meara, E.S.; Tosteson, A.N.A.; Haas, J.S.; et al. Comparative Access to and Use of Digital Breast Tomosynthesis Screening by Women’s Race/Ethnicity and Socioeconomic Status. JAMA Netw. Open 2021, 4, e2037546. [Google Scholar] [CrossRef] [PubMed]
- Warnecke, R.B.; Campbell, R.T.; Vijayasiri, G.; Barrett, R.E.; Rauscher, G.H. Multilevel examination of health disparity: The role of policy implementation in neighborhood context, in patient resources, and in healthcare facilities on later stage of breast cancer diagnosis. Cancer Epidemiol. Biomark. Prev. 2019, 28, 59–66. [Google Scholar] [CrossRef]
- Gibbons, J. Neighborhood Racial/Ethnic Composition and Medical Discrimination’s Relation to Mammograms: A Philadelphia Case Study. Race Soc. Probl. 2021, 13, 234–244. [Google Scholar] [CrossRef]
- Cullerton, K.; Gallegos, D.; Ashley, E.; Do, H.; Voloschenko, A.; Fleming, M.; Ramsey, R.; Gould, T. Cancer screening education: Can it change knowledge and attitudes among culturally and linguistically diverse communities in Queensland, Australia? Health Promot. J. Aust. 2016, 27, 140–147. [Google Scholar] [CrossRef]
- Molina, Y.; Plascak, J.J.; Patrick, D.L.; Bishop, S.; Coronado, G.D.; Beresford, S.A.A. Neighborhood predictors of mammography barriers among US-based latinas. J. Racial Ethn. Health Disparities 2017, 4, 233–242. [Google Scholar] [CrossRef]
- Kim, S.J.; Glassgow, A.E.; Watson, K.S.; Molina, Y.; Calhoun, E.A. Gendered and racialized social expectations, barriers, and delayed breast cancer diagnosis. Cancer 2018, 124, 4350–4357. [Google Scholar] [CrossRef]
- Jin, S.W.; Lee, H.Y.; Lee, J. Analyzing factors of breast cancer screening adherence among Korean American women using andersen’s behavioral model of healthcare services utilization. Ethn. Dis. 2019, 29, 427–434. [Google Scholar] [CrossRef]
- An, S.; Lee, H.Y.; Choi, Y.J.; Yoon, Y.J. Literacy of Breast Cancer and Screening Guideline in an Immigrant Group: Importance of Health Accessibility. J. Immigr. Minor. Health 2020, 22, 563–570. [Google Scholar] [CrossRef]
- Chan, T.K.C.; Tan, L.W.L.; Van Dam, R.M.; Seow, W.J. Cancer Screening Knowledge and Behavior in a Multi-Ethnic Asian Population: The Singapore Community Health Study. Front. Oncol. 2021, 11, 684917. [Google Scholar] [CrossRef]
- Orji, A.F.; Yamashita, T. Racial disparities in routine health checkup and adherence to cancer screening guidelines among women in the United States of America. Cancer Causes Control 2021, 32, 1247–1256. [Google Scholar] [CrossRef]
- Hong, H.C.; Lee, H.; Collins, E.G.; Park, C.; Quinn, L.; Ferrans, C.E. Factors affecting trust in healthcare among middle-aged to older Korean American women. BMC Women’s Health 2018, 18, 109. [Google Scholar] [CrossRef]
- Agrawal, P.; Chen, T.A.; McNeill, L.H.; Acquati, C.; Connors, S.K.; Nitturi, V.; Robinson, A.S.; Leal, I.M.; Reitzel, L.R. Factors associated with breast cancer screening adherence among church-going African American women. Int. J. Environ. Res. Public Health 2021, 18, 8494. [Google Scholar] [CrossRef]
- Lee, Y.S.; Roh, S.; Moon, H.; Lee, K.H.; McKinley, C.; LaPlante, K. Andersen’s Behavioral Model to Identify Correlates of Breast Cancer Screening Behaviors among Indigenous Women. J. Evid.-Based Soc. Work. 2020, 17, 117–135. [Google Scholar] [CrossRef]
- Krieger, N. ENOUGH: COVID-19, structural racism, police brutality, plutocracy, climate change-and time for health justice, democratic governance, and an equitable, sustainable future. Am. J. Public Health 2020, 110, 1620–1623. [Google Scholar] [CrossRef]
- Johnson-Agbakwu, C.E.; Ali, N.S.; Oxford, C.M.; Wingo, S.; Manin, E.; Coonrod, D. Racism, COVID-19, and Health Inequity in the USA: A Call to Action. J. Racial Ethn. Health Disparities 2022, 9, 52–58. [Google Scholar] [CrossRef]
- Immordino, P.; Genovese, D.; Morales, F.; Casuccio, A.; Amodio, E. Epidemiological Characteristics of COVID-19 Cases in Non-Italian Nationals in Sicily: Identifying Vulnerable Groups in the Context of the COVID-19 Pandemic in Sicily, Italy. Int. J. Environ. Res. Public Health 2022, 19, 5767. [Google Scholar] [CrossRef]
- Ponce-Blandón, J.A.; Romero-Castillo, R.; Jiménez-Picón, N.; Palomo-Lara, J.C.; Castro-Méndez, A.; Pabón-Carrasco, M. Lived experiences of african migrants crossing the strait of gibraltar to europe: A cross-cultural approach to healthcare from a qualitative methodology. Int. J. Environ. Res. Public Health 2021, 18, 9379. [Google Scholar] [CrossRef]
- Williams, D.R.; Lawrence, J.A.; Davis, B.A. Racism and Health: Evidence and Needed Research. Annu. Rev. Public Health 2019, 40, 105–125. [Google Scholar] [CrossRef]
- Molina-Barceló, A.; Moreno Salas, J.; Peiró-Pérez, R.; Arroyo, G.; Ibáñez Cabanell, J.; Vanaclocha Espí, M.; Binefa, G.; García, M.; Trejo, D.S. Desigualdades De Acceso A Los Programas De Cribado Del Cáncer En España Y Cómo Reducirlas: Datos De 2013 Y 2020. Rev. Esp. Salud Pública. 2021, 95, e1–e28. [Google Scholar]
- Zhou, Y.; Guo, Y.; Liu, Y. Health, income and poverty: Evidence from China’s rural household survey. Int. J. Equity Health 2020, 19, 36. [Google Scholar] [CrossRef] [PubMed]
- Shahar, S.; Lau, H.; Puteh, S.E.W.; Amara, S.; Razak, N.A. Health, access and nutritional issues among low-income population in Malaysia: Introductory note. BMC Public Health 2019, 9 (Suppl. 4), 552. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A. (Ed.) Conceptos de Salud Pública y Estrategias Preventivas, 2nd ed.; Elsevier: Madrid España, 2018; pp. 239–241. [Google Scholar]
- Lund, C.; Breen, A.; Flisher, A.J.; Kakuma, R.; Corrigall, J.; Joska, J.A.; Swartz, L.; Patel, V. Poverty and common mental disorders in low and middle income countries: A systematic review. Soc. Sci. Med. 2010, 71, 517–528. [Google Scholar] [CrossRef]
- Ma, C.; Zhang, Y.; Li, Y.; Wang, Y.; Jiang, Y.; Wang, X.; Swartz, L.; Patel, V. Healthcare, Insurance, and Medical Expenditure of the Floating Population in Beijing, China. Front. Public Health 2020, 8, 375. [Google Scholar] [CrossRef]
- DeVoe, J.E.; Baez, A.; Angier, H.; Krois, L.; Edlund, C.; Carney, P.A. Insurance + access ≠ health care: Typology of barriers to health care access for low-income families. Ann. Fam. Med. 2007, 5, 511–518. [Google Scholar] [CrossRef]
- Serral, G.; Borrell, C.; Puigpinós i Riera, R. Desigualdades socioeconómicas en el control mamográfico en mujeres españolas de 45 a 69 años de edad. Gac. Sanit. 2018, 32, 61–67. [Google Scholar] [CrossRef]
- Hahn, R.A.; Truman, B.I. Education improves public health and promotes health equity. Int. J. Health Serv. 2015, 45, 657–678. [Google Scholar] [CrossRef]
- Nagakura, Y.; Kato, H.; Asano, S.; Jinno, Y.; Tanei, S. The significant association between health examination results and population health: A cross-sectional ecological study using a nation-wide health checkup database in Japan. Int. J. Environ. Res. Public Health 2021, 18, 836. [Google Scholar] [CrossRef]
- Cancer screening in the European Union. Report on the Implementation of the Council Recommendation on Cancer Screening (Second Report). 2017. Available online: https://screening.iarc.fr/EUreport.php (accessed on 17 December 2021).
- Alkhasawneh, E.; Al-Farsi, Y.; Al-Simadi, F.; Leocadio, M. Development and validation of a culturally-tailored breast cancer health education programme for Arab women. Sultan. Qaboos Univ. Med. J. 2017, 17, e181–e190. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors/Year/Country 1 | Journal | Title | Main Results |
|---|---|---|---|
| Haas et al. [15]/2016/USA | Cancer | Disparities in the Use of Screening Magnetic Resonance Imaging (MRI) of the Breast in Community Practice by Race, Ethnicity, and Socioeconomic Status | Among patients with a lower risk of developing breast cancer (<20%), non-Hispanic white women were 62% more likely than nonwhite women to undergo MRI (95% CI [1.32–1.98]). Of these, those with higher levels of education (43%), and especially those with academic degrees (132%), were more likely to receive MRI. |
| Elewonibi et al. [16]/2018/USA | Journal of Immigrant and Minority Health | Examining Mammography Use by Breast Cancer Risk, Race, Nativity, and Socioeconomic Status | Being a foreigner is an independent factor that decreases the probability of receiving a mammogram by about 10% (OR: 0.904, p < 0.05). If the variables of socioeconomic status and social resources are added as controls, higher levels are related to higher probability of mammography. |
| Shon et al. [17]/2019/USA | PLoS ONE | Predictors of never having a mammogram among Chinese, Vietnamese, and Korean immigrant women in the U.S. | The odds of never having had a mammogram were higher in Korean women (OR: 1.80, 95% CI [1–3.22]), unmarried women (OR: 1.74, 95% CI [1.08–2.82]) and non-US citizens (OR 2.56, 95% CI [1.44–4.55]). Conversely, they were lower in women aged 50–59 (OR:0.37, 95% CI [0.15–0.89]) and 60–69 years (OR: 0.36, 95% CI [0.17–0.75]) compared with those aged 70–85 years. |
| Henderson et al. [18]/2020/USA | Journal of Women’s Health | The Role of Social Determinants of Health in Self-Reported Access to Health Care Among Women Undergoing Screening Mammography | Compared with white women, more barriers were reported among Black (OR: 1.30) and Hispanic (OR:1.66) women. They were also higher in areas with a high diversity index (OR: 1.28), where they were lower among women with moderate (OR: 0.69) or high incomes (OR: 0.85). |
| Lee et al. [19]/2021/USA | JAMA Network Open | Comparative Access to and Use of Digital Breast Tomosynthesis (DBT) Screening by Women’s Race/Ethnicity and Socioeconomic Status | Black women experienced lower DBT use (RR: 0.83) compared with white women (RR: 0.98); also, women with lower educational attainment (RR: 0.79–0.88) and lower income (RR 0.89) had lower use relative to educated women (RR: 0.90–0.96) and those with the highest income (RR: 0.99). |
| Warnecke et al. [20]/2021/USA | Cancer Epidemiology, Biomarkers and Prevention | Multilevel Examination of Health Disparity: The Role of Policy Implementation in Neighbourhood Context, in Patient Resources, and in Healthcare Facilities on Later Stage of Breast Cancer Diagnosis | After adjusting for setting, mode of detection and resources, no significant differences were found in the late diagnosis of breast cancer among non-Hispanic Black and Hispanic women compared with non-Hispanic white women. |
| Gibbons J. [21]/2021/USA | Race and Social Problems | Neighbourhood Racial/Ethnic Composition and Medical Discrimination’s Relation to Mammograms: A Philadelphia Case Study | Black and Hispanic women were 5 times more likely to have experienced discrimination (11.3% and 11.2%, respectively) than white women (2.2%). Those who had access problems owing to transportation were 26.4% less likely to attend a screening, while those with private insurance were 323.2% more likely. |
| Cullerton et al. [22]/2016/Australia | Health Promotion Journal of Australia | Cancer screening education: can it change knowledge and attitudes among culturally and linguistically diverse communities in Queensland, Australia? | After education sessions, a decrease of 5% (p = 0.04) in the lack of knowledge about breast screening was observed. Likewise, after the session, there was an improvement in the ability to identify the correct age to start screening (14.8% presession vs. 37.7% postsession) and the frequency of screening (39.3% vs. 90.2). |
| Molina et al. [23]/2017/USA | Journal of Racial and Ethnic Health Disparities | Neighbourhood predictors of mammography barriers among US-based Latinas | The proportion of women who reported sociocultural, economic and lack of knowledge reasons for not having undergone mammography were 0.19, 0.31 and 0.35, respectively. Women residing in areas with a lower concentration of Latinos less frequently reported economic and lack of knowledge reasons (p < 0.05). |
| Kim et al. [24]/2018/USA | Cancer | Gendered and Racialized Social Expectations, Barriers, and Delayed Breast Cancer Diagnosis | Women who identified barriers were more likely to receive follow-up mammography screening (31.2% vs. 48.4%, p < 0.01). Black women (prediction value 1.91, p < 0.01), those exhibiting distrust (prediction value 0.92, p < 0.01) and those living in poverty (prediction value 4.69, p < 0.005) were less likely to report barriers. |
| Jin et al. [25]/2019/USA | Ethnicity and Disease | Analyzing Factors of Breast Cancer Screening Adherence among Korean American Women Using Andersen’s Behavioral Model of Healthcare Services Utilization | Personal history of cancer (p = 0.0027), having undergone an annual health checkup (p < 0.0001), having health insurance (p = 0.0025), receiving a recommendation by healthcare personnel (p = 0.0027) and high level of English (p = 0.0021) are related to higher adherence to mammography. |
| Lee et al. [19]/2019/USA | Journal of Evidence-Based Social Work | Andersen’s Behavioral Model to Identify Correlates of Breast Cancer Screening Behaviors among Indigenous Women | Older women (OR: 1.116, p < 0.001), those with a family history of cancer (OR: 2.742, p < 0.05) and those with a school diploma (OR: 13.203, p < 0.01) or academic degree (OR: 6.750, p < 0.01) showed higher levels of mammography use. Those who had heard of the screening program also showed higher levels (OR: 36.250, p < 0.01). |
| An et al. [26]/2020/USA | Journal of Immigrant and Minority Health | Literacy of Breast Cancer and Screening Guideline in an Immigrant Group: Importance of Health Accessibility | Marital status of married (OR: 29.152, p < 0.01) and having undergone an annual health checkup (OR: 16.148, p < 0.05) is related to a higher level of awareness of breast cancer–screening programs. |
| Chan et al. [27]/2021/Singapore | Frontiers in Oncology | Cancer Screening Knowledge and Behavior in a Multi-Ethnic Asian Population: The Singapore Community Health Study | Of the participants, only 35.1% claimed to have participated in a breast cancer–screening program. Participants with higher educational levels showed a 22% higher participation rate (aPR: 1.22, p < 0.032), as did those with high income by 7.1% (aPR: 1.71, p < 0.001). |
| Orji et al. [28]/2021/USA | Cancer Causes and Control | Racial disparities in routine health checkup and adherence to cancer screening guidelines among women in the United States of America | Women who had received an annual health examination were more likely to participate in cervical (OR: 3.24, p < 0.05) and breast (OR: 5.86, p < 0.05) cancer–screening programs, compared with those who did not receive screening—with the exception of Hispanic women, in whom this relationship was not observed. |
| Hong et al. [29]/2018/USA | BMC Women’s Health | Factors affecting trust in healthcare among middle-aged to older Korean American women | A longer stay in the US increases the level of trust in the health system (p < 0.001). The feeling of discrimination causes distrust in the health system (p < 0.001). Acculturation was related to a higher level of trust in healthcare providers (p = 0.002). |
| Agrawal et al. [30]/2021/USA | Int. Journal of Environmental Research and Public Health | Factors Associated with Breast Cancer Screening Adherence among Church-Going African American Women | Older age (OR: 1.015), having health insurance (OR: 2.388), having a good doctor–patient relationship (OR: 1.485) and having a previous diagnosis of cancer (OR: 2.244) were associated with a higher level of adherence. |
| Barriers to Adherence | n 1 | % 2 |
|---|---|---|
| Race and/or ethnicity and/or foreign nationality | 8 | 47 |
| Low socioeconomic level and lack of resources | 6 | 35.3 |
| Low educational level | 5 | 29.4 |
| No family history and being single | 5 | 29.4 |
| Health information gap and medical mistrust | 4 | 23.5 |
| Failure to attend annual health checkups | 3 | 17.6 |
| Lack of private health insurance | 3 | 17.6 |
| Authors/Year/Country | MS 1 | PC 2 | Age | HE 3 | ES 4 | KP 5 |
|---|---|---|---|---|---|---|
| Agrawal et al./2021/USA [30] |  | | | |||
| An et al./2020/USA [26] | | |||||
| Jin et al./2019/USA [25] | | | | | | |
| Lee et al./2019/USA [31] | | | | | ||
| Shon et al./2019/USA [17] | | | ||||
| Lee et al./2021/USA [19] | | |||||
| Chan et al./2021/Singapore [27] | | |||||
| Haas et al./2016/USA [15] | |
= Higher adherence.| Authors/Year/Country | RHC 1 | EBCS 2 | MM 3 | A 4 | AHC 5 |
|---|---|---|---|---|---|
| Agrawal et al./2021/USA [30] | | ||||
| Orji et al./2021/USA [28] | | ||||
| An et al./2020/USA [26] | | | |||
| Jin et al./2019/USA [25] | | | |||
| Kim et al./2018/USA [24] | |||||
| Hong et al./2018/USA [29] | | ||||
| Cullerton et al./2016/Australia [22] | |
= Higher adherence.Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ponce-Chazarri, L.; Ponce-Blandón, J.A.; Immordino, P.; Giordano, A.; Morales, F. Barriers to Breast Cancer-Screening Adherence in Vulnerable Populations. Cancers 2023, 15, 604. https://doi.org/10.3390/cancers15030604
Ponce-Chazarri L, Ponce-Blandón JA, Immordino P, Giordano A, Morales F. Barriers to Breast Cancer-Screening Adherence in Vulnerable Populations. Cancers. 2023; 15(3):604. https://doi.org/10.3390/cancers15030604
Chicago/Turabian StylePonce-Chazarri, Laura, Jose Antonio Ponce-Blandón, Palmira Immordino, Antonio Giordano, and Fátima Morales. 2023. "Barriers to Breast Cancer-Screening Adherence in Vulnerable Populations" Cancers 15, no. 3: 604. https://doi.org/10.3390/cancers15030604
APA StylePonce-Chazarri, L., Ponce-Blandón, J. A., Immordino, P., Giordano, A., & Morales, F. (2023). Barriers to Breast Cancer-Screening Adherence in Vulnerable Populations. Cancers, 15(3), 604. https://doi.org/10.3390/cancers15030604