
Hepatitis C Virus Elimination Using Direct Acting Antivirals after the Radical Cure of Hepatocellular Carcinoma Suppresses the Recurrence of the Cancer


 , , ,
, , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Enrollment and Study Design
2.2. Diagnosis, Treatment, and Assessment of Treatment Effect in HCC and Follow-Up Schedule
2.3. Treatment Using DAA
2.4. Collection of Clinical and Laboratory Data
2.5. PSM Analysis
2.6. Statistical Analysis
3. Results
3.1. Background Factors
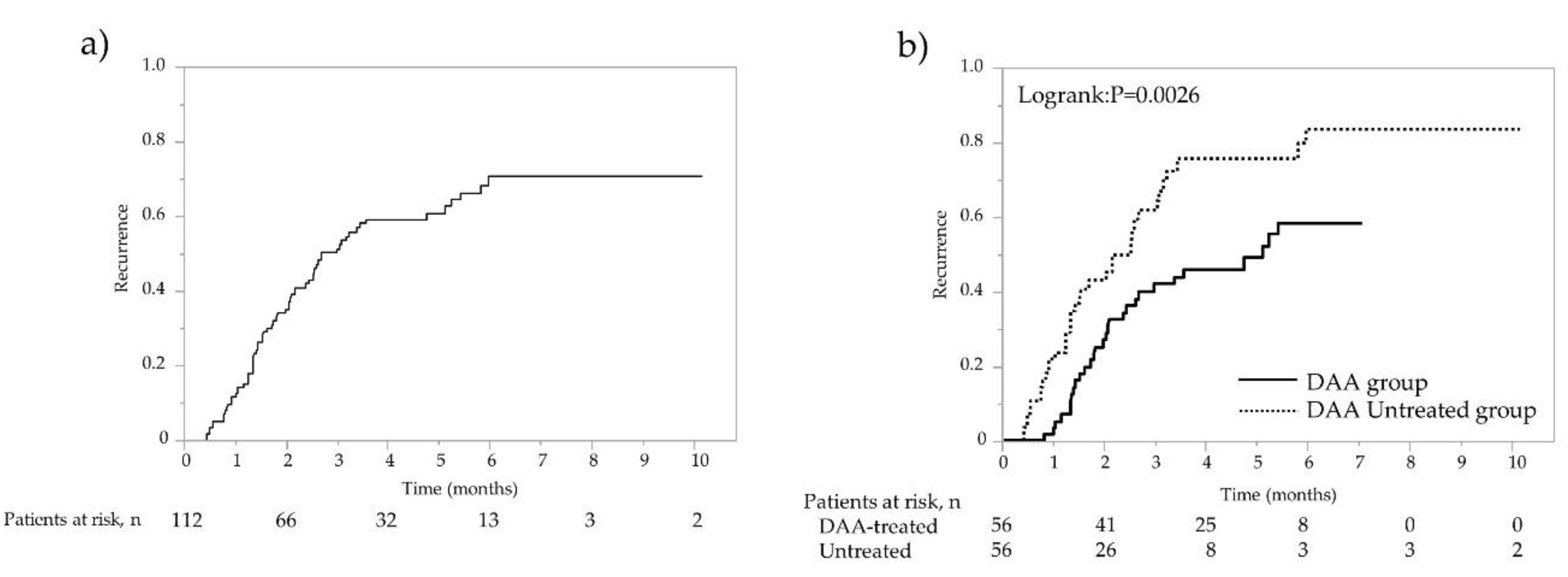
3.2. Comparison of Recurrence Rates in the DAA-Treated Group and Non-DAA-Treated Group after PSM
3.3. Factors Contributing to Recurrence-Free and Second-Recurrence-Free Survival after PSM
3.4. Factors Contributing to Recurrence-Free and Second-Recurrence-Free Survival in the Daa-Treated Group after PSM
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Charlton, M.; Everson, G.T.; Flamm, S.L.; Kumar, P.; Landis, C.; Brown, R.S., Jr.; Fried, M.W.; Terrault, N.A.; O’Leary, J.G.; Vargas, H.E.; et al. Ledipasvir and sofosbuvir plus ribavirin for treatment of HCV infection in patients with advanced liver disease. Gastroenterology 2015, 149, 649–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itokawa, N.; Atsukawa, M.; Tsubota, A.; Ikegami, T.; Shimada, N.; Kato, K.; Abe, H.; Okubo, T.; Arai, T.; Iwashita, A.N.; et al. Efficacy of direct-acting antiviral treatment in patients with compensated liver cirrhosis: A multicenter study. Hepatol. Res. 2019, 49, 125–135. [Google Scholar] [CrossRef]
- Knop, V.; Mauss, S.; Goeser, T.; Geier, A.; Zimmermann, T.; Herzer, K.; Postel, N.; Friedrich-Rust, M.; Hofmann, W.P. Dynamics of liver stiffness by transient elastography in patients with chronic hepatitis C virus infection receiving direct-acting antiviral therapy-results from the German Hepatitis C-Registry. J. Viral Hepat. 2020, 27, 690–698. [Google Scholar] [CrossRef] [PubMed]
- Backus, L.I.; Belperio, P.S.; Shahoumian, T.A.; Mole, L.A. Direct-acting antiviral sustained virologic response: Impact on mortality in patients without advanced liver disease. Hepatology 2018, 68, 827–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvaruso, V.; Cabibbo, G.; Cacciola, I.; Petta, S.; Madonia, S.; Bellia, A.; Tinè, F.; Distefano, M.; Licata, A.; Giannitrapani, L.; et al. Incidence of hepatocellular carcinoma in patients with HCV-associated cirrhosis treated with direct-acting antiviral agents. Gastroenterology 2018, 155, 411–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ioannou, G.N.; Beste, L.A.; Green, P.K.; Singal, A.G.; Tapper, E.B.; Waljee, A.K. Increased risk for hepatocellular carcinoma persists up to 10 Years after HCV eradication in patients with baseline cirrhosis or high FIB-4 scores. Gastroenterology 2019, 157, 1264–1278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ide, T.; Koga, H.; Nakano, M.; Hashimoto, S.; Yatsuhashi, H.; Higuchi, N.; Nakamuta, M.; Oeda, S.; Eguchi, Y.; Shakado, S.; et al. Direct-acting antiviral agents do not increase the incidence of hepatocellular carcinoma development: A prospective, multicenter study. Hepatol. Int. 2019, 13, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Cabibbo, G.; Celsa, C.; Calvaruso, V.; Petta, S.; Cacciola, I.; Cannavo, M.R.; Madonia, S.; Rossi, M.; Magro, B.; Rini, F.; et al. Direct-acting antivirals after successful treatment of early hepatocellular carcinoma improve survival in HCV-cirrhotic patients. J. Hepatol. 2019, 71, 265–273. [Google Scholar] [CrossRef]
- Huang, A.C.; Mehta, N.; Dodge, J.L.; Yao, F.Y.; Terrault, N.A. Direct-acting antivivals do not increase the risk of hepatocellular carcinoma recurrence after local-regional therapy or liver transplant waitlist dropout. Hepatology 2018, 68, 449–461. [Google Scholar] [CrossRef]
- Lin, W.C.; Lin, Y.S.; Chang, C.W.; Chang, C.W.; Wang, T.E.; Wang, H.Y.; Chen, M.J. Impact of direct-acting antiviral therapy for hepatitis C-related hepatocellular carcinoma. PLoS ONE 2020, 15, e0233212. [Google Scholar] [CrossRef]
- Reig, M.; Marino, Z.; Perello, C.; Iñarrairaegui, M.; Ribeiro, A.; Lens, S.; Díaz, A.; Vilana, R.; Darnell, A.; Varela, M.; et al. Unexpected high rate of early tumor recurrence in patients with HCV-related HCC undergoing interferon-free therapy. J. Hepatol. 2016, 65, 719–726. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, K.; Kawamura, Y.; Kobayashi, M.; Kominami, Y.; Fujiyama, S.; Sezaki, H.; Hosaka, T.; Akuta, N.; Saitoh, S.; Suzuki, F.; et al. Direct-acting antivirals decreased tumor recurrence after initial treatment of hepatitis C virus-related hepatocellular carcinoma. Dig. Dis. Sci. 2017, 62, 2932–2942. [Google Scholar] [CrossRef]
- Virlogeux, V.; Pradat, P.; Hartig-Lavie, K.; Bailly, F.; Maynard, M.; Ouziel, G.; Poinsot, D.; Lebossé, F.; Ecochard, M.; Radenne, S.; et al. Direct-acting antiviral therapy decreases hepatocellular carcinoma recurrence rate in cirrhotic patients with chronic hepatitis C. Liver Int. 2017, 37, 1122–1127. [Google Scholar] [CrossRef]
- Ochi, H.; Hiraoka, A.; Hirooka, M.; Koizumi, Y.; Amano, M.; Azemoto, N.; Watanabe, T.; Yoshida, O.; Tokumoto, Y.; Mashiba, T.; et al. Direct-acting antivirals improve survival and recurrence rates after treatment of hepatocellular carcinoma within the Milan criteria. J. Gastroenterol. 2021, 56, 90–100. [Google Scholar] [CrossRef]
- Tsuda, H.; Oda, T.; Sakamoto, M.; Hirohashi, S. Different pattern of chromosomal allele loss in multiple hepatocellular carcinomas as evidence of their multifocal origin. Cancer Res. 1992, 52, 1504–1509. [Google Scholar] [PubMed]
- Tokushige KHashimoto, E.; Kodama, K. Hepatocarcinogenesis in non-alcoholic fatty liver disease in Japan. J. Gastroenterol. Hepatol. 2013, 28 (Suppl. S4), 88–92. [Google Scholar] [CrossRef] [Green Version]
- Hino-Arinaga, T.; Ide, T.; Kuromatsu, R.; Miyajima, I.; Ogata, K.; Kuwahara, R.; Hisamochi, A.; Torimura, T.; Sata, M. Risk factors for hepatocellular carcinoma in Japanese patients with autoimmune hepatitis type 1. J. Gastroenterol. 2012, 47, 569–576. [Google Scholar] [CrossRef]
- Oikawa, T.; Ojima, H.; Yamasaki, S.; Takayama, T.; Hirohashi, S.; Sakamoto, M. Multistep and multicentric development of hepatocellular carcinoma: Histological analysis of 980 resected nodules. J. Hepatol. 2005, 42, 225–229. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Fujii, H.; Matsuda, M.; Kono, H. Multicentric occurrence of hepatocellular carcinoma: Diagnosis and clinical significance. J. Hepatobiliary Pancreat. Surg. 2001, 8, 435–440. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Makuuchi, M.; Kokudo, N.; Arii, S.; Futagawa, S.; Kaneko, S.; Kawasaki, S.; Matsuyama, Y.; Okazaki, M.; Okita, K.; Omata, M.; et al. Development of evidence-based clinical guidelines for the diagnosis and treatment of hepatocellular carcinoma in Japan. Hepatol. Res. 2008, 38, 37–51. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Tsuji, K.; Takaguchi, K.; Itobayashi, E.; Kariyama, K.; Ochi, H.; Tajiri, K.; Hirooka, M.; Shimada, N.; et al. Varidation of modified ALBI grade for more detailed assessment of hepatic function in hepatocellular carcinoma patients: A multicenter analysis. Liver Cancer 2019, 8, 121–129. [Google Scholar] [CrossRef]
- Ikeda, K.; Saitoh, S.; Arase, Y.; Chayama, K.; Suzuki, Y.; Kobayashi, M.; Tsubota, A.; Nakamura, I.; Murashima, N.; Kumada, H.; et al. Effect of interferon therapy on hepatocellular carcinogenesis in patients with chronic hepatitis type C: A long-term observation study of 1,643 patients using statistical bias correction with proportional hazard analysis. Hepatology 1999, 29, 1124–1130. [Google Scholar] [CrossRef]
- Bruno, S.; Stroffolini, T.; Colombo, M.; Bollani, S.; Benvegnu, L.; Mazzella, G.; Ascione, A.; Santantonio, T.; Piccinino, F.; Andreone, P.; et al. Sustained virological response to interferon-alpha is associated with improved outcome in HCV-related cirrhosis: A retrospective study. Hepatology 2007, 45, 579–587. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Romito, R.; Chiavo, M.; Mariani, L.; Camerini, T.; Bhoori, S.; Capussotti, L.; Calise, F.; Pellicci, R.; Belli, G.; et al. Prevention of hepatocellular carcinoma recurrence with alpha-interferon after liver resection in HCV cirrhosis. Hepatology 2006, 44, 1543–1554. [Google Scholar] [CrossRef]
- Shiratori, Y.; Shiina, S.; Teratani, T.; Imamura, M.; Obi, S.; Sato, S.; Koike, Y.; Yoshida, H.; Omata, M. Interferon therapy after tumor ablation improves prognosis in patients with hepatocellular carcinoma associated with hepatitis C virus. Ann. Intern. Med. 2003, 138, 299–306. [Google Scholar] [CrossRef]
- Shen, Y.C.; Hsu, C.; Chen, L.T.; Cheng, C.C.; Hu, F.C.; Cheng, A.L. Adjuvant interferon therapy after curative therapy for hepatocellular carcinoma (HCC): A meta-regression approach. J. Hepatol. 2010, 52, 889–894. [Google Scholar] [CrossRef]
- Sakae, M.; Kubo, S.; Takemura, S.; Sakata, C.; Uenishi, T.; Kodai, S.; Shinkawa, H.; Urata, Y.; Ohata, K.; Kaneda, K.; et al. Effect of interferon therapy on first and second recurrence after resection of hepatitis C virus-related hepatocellular carcinoma. Hepatol. Res. 2012, 42, 564–573. [Google Scholar] [CrossRef]
- Singal, A.G.; Rich, N.E.; Mehta, N.; Branch, A.; Pillai, A.; Hoteit, M.; Volk, M.; Odewole, M.; Scaglione, S.; Guy, J.; et al. Direct-acting antiviral therapy not associated with recurrence of hepatocellular carcinoma in a multicenter North American cohort study. Gastroenterology 2019, 156, 1683–1692. [Google Scholar] [CrossRef]
- Kinoshita, M.N.; Minami, T.; Tateishi, R.; Wake, T.; Nakagomi, R.; Fujiwara, N.; Sato, M.; Uchino, K.; Enooku, K.; Nakagawa, H.; et al. Impact of direct-acting antivirals on early recurrence of HCV-related HCC: Comparison with interferon-based therapy. J. Hepatol. 2018, 70, 78–86. [Google Scholar] [CrossRef]
- ANRS Collaborative Study Group on Hepatocellular Carcinoma. Lack of evidence of an effect of direct-acting antivirals on the recurrence of hepatocellular carcinoma: Data from three ANRS cohorts. J. Hepatol. 2016, 65, 734–740. [Google Scholar] [CrossRef] [Green Version]
- Zou, W.Y.; Choi, K.; Kramer, J.R.; Yu, X.; Cao, Y.; El-Serag, H.B.; Kanwal, F. Risk of hepatocellular cancer recurrence in hepatitis C virus+ patients treated with direct-acting antiviral agents. Dig. Dis. Sci. 2019, 64, 3328–3336. [Google Scholar] [CrossRef]
- Nagata, H.; Nakagawa, M.; Asahina, Y.; Sato, A.; Asano, Y.; Tsunoda, T.; Miyoshi, M.; Kaneko, S.; Otani, S.; Kawai-Kitahata, F.; et al. Effect of interferon-based and -free therapy on early occurrence and recurrence of hepatocellular carcinoma in chronic hepatitis C. J. Hepatol. 2017, 67, 933–939. [Google Scholar] [CrossRef]
- Hiramatsu, N.; Oze, T.; Takehara, T. Suppression of hepatocellular carcinoma development in hepatitis C patients given interferon based antiviral therapy. Hepatol. Res. 2015, 45, 152–161. [Google Scholar] [CrossRef]
- Ikeda, K.; Arase, Y.; Saitoh, S.; Kobayashi, M.; Suzuki, Y.; Suzuki, F.; Tsubota, A.; Chayama, K.; Murashima, N.; Kumada, H. Interferon beta prevents recurrence of hepatocellular carcinoma after complete resection or ablation of the primary tumor-A prospective randomized study of hepatitis C virus-related liver cancer. Hepatology 2000, 32, 228–232. [Google Scholar] [CrossRef]
- Kudo, M.; Sakaguchi, Y.; Chung, H.; Hatanaka, K.; Hagiwara, S.; Ishikawa, E.; Takahashi, S.; Kitai, S.; Inoue, T.; Minami, Y.; et al. Long-term interferon maintenance therapy improves survival in patients with HCV-related hepatocellular carcinoma after curative radiofrequency ablation. A matched case-control study. Oncology 2007, 72 (Suppl. S1), 132–138. [Google Scholar] [CrossRef]
- Váncsa, S.; Németh, D.; Hegyi, P.; Szakács, Z.; Farkas, Á.; Kiss, S.; Hegyi, P.J.; Kanjo, A.; Sarlós, P.; Erőss, B.; et al. Diabetes mellitus increases the risk of hepatocellular carcinoma after direct-acting antiviral therapy: Systemic review and meta-analysis. Front. Med. 2021, 8, 744512. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | All Patients (n = 190) | Patients Treated with DAAs (n = 70) | Untreated Patients | p-Value |
|---|---|---|---|---|
| (n = 120) | ||||
| Age | 72 (44–93) | 71 (56–88) | 77 (54–93) | 0.0002 |
| Sex (Male/Female) | 101/89 | 41/29 | 60/60 | 0.2534 |
| HBsAg (+/−) | 3/187 | 1/69 | 2/118 | 0.8989 |
| Alcohol history (+/−/unknown) | 28/156/6 | 12/56/2 | 16/100/4 | 0.4824 |
| Diabetes mellitus (+/−/unknown) | 51/137/2 | 19/50/1 | 32/87/1 | 0.9236 |
| IFN treatment history (+/−) | 37/153 | 20/50 | 17/103 | 0.0156 |
| Child–Pugh score (5/6/7) | 94/66/30 | 36/24/10 | 58/42/20 | 0.8821 |
| ALBI score | −2.309 (−3.296 to −1.056) | −2.340 (−3.296 to −1.056) | −2.275 (−3.216 to −1.155) | 0.5778 |
| FIB-4 index | 5.04 (1.03–27.64) | 4.93 (1.03–18.67) | 5.19 (1.10–27.64) | 0.5969 |
| Platelet count (×104/mm3) | 10.8 (2.5–37) | 10.7 (2.5–36.1) | 10.8 (3.1–37) | 0.9028 |
| Albumin (g/dL) | 3.62 (2.44–4.7) | 3.65 (2.44–4.6) | 3.59 (2.59–4.7) | 0.666 |
| AST (IU/L) | 51 (18–169) | 52 (19–169) | 48 (18–141) | 0.1599 |
| ALT (IU/L) | 40.5 (6–224) | 46.5 (11–224) | 37 (6–124) | 0.0114 |
| Tumor size (mm) | 17 (8–45) | 16 (8–42) | 18 (9–45) | 0.1288 |
| Tumor numbers (1/2/3) | 139/35/16 | 1955/9/6 | 84/26/10 | 0.3151 |
| AFP (ng/mL) | 11.5 (1.2–8461) | 9.0 (1.5–553) | 13.6 (1.2–8461) | 0.4003 |
| DCP (mAU/mL) | 24 (3–1657) | 22 (3.9–246) | 27.5 (3–1657) | 0.0199 |
| HCC treatment (Resection/RFA) | 52/138 | 18/52 | 34/86 | 0.6961 |
| Observation Period (months) | 48.9 (12.2–121.8) | 57.2 (14.4–84.6) | 45.0 (12.2–121.8) | 0.3071 |
| Characteristic | All Patients (n = 112) | SVR with DAAs (n = 56) | Non-DAA (n = 56) | p-Value |
|---|---|---|---|---|
| Age | 73 (55–93) | 69.5 (56–85) | 76.5 (55–93) | 0.0002 |
| Sex (Male/Female) | 56/56 | 32/24 | 24/32 | 0.1306 |
| HBsAg (+/−) | 1/111 | 1/55 | 0/56 | 0.3151 |
| Alcohol history (+/−/unknown) | 14/95/3 | 10/45/1 | 4/50/2 | 0.0928 |
| Diabetes mellitus (+/−/unknown) | 34/77/1 | 16/40/0 | 18/37/1 | 0.6349 |
| IFN treatment history (+/−) | 26/86 | 18/38 | 8/48 | 0.0252 |
| Child–Pugh score (5/6/7) | 52/43/17 | 29/20/7 | 23/23/10 | 0.4889 |
| ALBI score | −2.276 (−3.295 to −1.056) | −2.321 (−3.295 to −1.056) | −2.240 (−3.216 to −1.329) | 0.4885 |
| FIB-4 index | 5.42 (1.03–27.64) | 4.89 (1.03–18.67) | 6.26 (1.61–27.64) | 0.1067 |
| Platelet count (×104/mm3) | 10.2 (2.5–36.1) | 10.7 (2.5–36.1) | 9.8 (3.1–23.8) | 0.1669 |
| Albumin (g/dL) | 3.59 (2.44–4.6) | 3.64 (2.44–4.6) | 3.48 (2.77–4.6) | 0.5482 |
| AST (IU/L) | 52 (19–169) | 53 (19–169) | 52 (19–141) | 0.8376 |
| ALT (IU/L) | 43 (10–224) | 45.5 (11–224) | 41 (10–124) | 0.2791 |
| Tumor size (mm) | 17 (8–45) | 15.5 (8–42) | 18 (10–45) | 0.3952 |
| Tumor numbers (1/2/3) | 80/23/9 | 1944/7/5 | 36/16/4 | 0.109 |
| AFP (ng/mL) | 13.6 (1.2–553) | 13.4 (1.5–553) | 13.8 (1.2–258) | 0.2827 |
| DCP (mAU/mL) | 22 (3–1657) | 23 (3.9–246) | 20.5 (3–1657) | 0.2902 |
| HCC treatment (Resection/RFA) | 25/87 | 15/41 | 10/46 | 0.2565 |
| Observation Period (months) | 50.5 (14.4–121.8) | 57.8 (14.4–84.6) | 45.3 (15.8–121.8) | 0.4241 |
| Variable | Category | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Age | ≤74 | 1 1.265 (0.78–2.04) | 0.3375 | ||
| >74 | |||||
| Sex | Male Female | 1 1.149 (0.71–1.86) | 0.5711 | ||
| HBsAg | Positive Negative | 5.4571 × 10−9 (0–0) 1 | 0.9989 | ||
| DAA | Untreated Treated | 1 0.480 (0.29–0.78) | 0.0032 | 1 0.463 (0.28–0.77) | 0.0034 |
| Alcohol history | + − | 0.850 (0.41–1.78) 1 | 0.6665 | ||
| Diabetes mellitus | + − | 1.435 (0.86–2.38) 1 | 0.1636 | 1.277 (0.74–2.21) 1 | 0.3807 |
| IFN | + − | 0.706 (0.40–1.26) 1 | 0.2376 | ||
| treatment history | |||||
| Child–Pugh | 5 6–7 | 0.764 (0.47–1.24) 1 | 0.2747 | ||
| ALBI score | 1–2a 2b–3 | 0.730 (0.45–1.18) 1 | 0.1985 | 1.260 (0.70–2.29) 1 | 0.4417 |
| FIB-4 index | ≤3.25 >3.25 | 0.649 (0.31–1.36) 1 | 0.2524 | ||
| Platelet count | ≤15.8 >15.8 | 1 0.526 (0.24–1.15) | 0.1083 | 1 0.719 (0.30–1.70) | 0.4517 |
| (× 104/mm3) | |||||
| Albumin (g/dL) | ≤3.8 >3.8 | 1 0.733 (0.42–1.27) | 0.2699 | ||
| AST (IU/L) | ≤42 >42 | 0.871 (0.52–1.47) 1 | 0.6038 | ||
| ALT (IU/L) | ≤39 >39 | 0.889 (0.55–1.45) 1 | 0.6367 | ||
| Tumor size (mm) | ≤20 >20 | 0.936 (0.54–1.61) 1 | 0.8118 | ||
| Tumor number | Single Multiple | 0.467 (0.28–0.77) 1 | 0.003 | 0.558 (0.33–0.96) 1 | 0.0344 |
| AFP (ng/mL) | ≤10 >10 | 0.575 (0.35–0.95) 1 | 0.0304 | 0.595 (0.32–1.10) 1 | 0.098 |
| DCP (mAU/mL) | ≤40 >40 | 0.720 (0.41–1.25) 1 | 0.244 | ||
| Variable | Category | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Age | ≤74 >74 | 1 1.546 (0.72–3.30) | 0.2601 | ||
| Sex | Male Female | 1 0.669 (0.31–1.44) | 0.3059 | ||
| HBsAg | Positive Negative | 1.4839 × 10−8 (0–0) | 0.9991 | ||
| DAA | Untreated Treated | 1 0.387 (0.18–0.84) | 0.0613 | 1 0.424 (0.19–0.96) | 0.0394 |
| Alcohol history | + − | 1.544 (0.62–3.85) 1 | 0.3511 | ||
| Diabetes mellitus | + − | 1.431 (0.64–3.20) 1 | 0.3827 | ||
| IFN treatment history | + − | 0.648 (0.26–1.61) 1 | 0.3504 | ||
| Child–Pugh | 5 6–7 | 0.422 (0.19–0.94) 1 | 0.0355 | 0.563 (0.24–1.33) 1 | 0.1918 |
| mALBI grade | 1–2a 2b–3 | 0.534 (0.25–1.15) 1 | 0.1075 | ||
| FIB-4 index | ≤3.25 >3.25 | 0.704 (0.21–2.34) 1 | 0.5665 | ||
| Platelet count(× 104/mm3) | ≤15.8 >15.8 | 1 0.723 (0.25–2.09) | 0.5493 | ||
| Albumin (g/dL) | ≤3.8 >3.8 | 1 0.791 (0.35–1.81) | 0.5784 | ||
| AST (IU/L) | ≤42 >42 | 0.755 (0.32–1.79) 1 | 0.5234 | ||
| ALT (IU/L) | ≤39 >39 | 1.021 (0.47–2.23) 1 | 0.9581 | ||
| Tumor size (mm) | ≤20 >20 | 0.699 (0.31–1.56) 1 | 0.3808 | ||
| Tumor number | Single Multiple | 0.307 (0.14–0.66) 1 | 0.0023 | 0.462 (0.21–1.04) 1 | 0.0609 |
| AFP (ng/mL) | ≤10 >10 | 0.378 (0.16–0.90) | 0.0271 | 0.542 (0.21–1.40) 1 | 0.2064 |
| 1 | |||||
| DCP (mAU/mL) | ≤40 >40 | 0.999 (0.40–2.48) 1 | 0.9994 | ||
| Variable | Category | 1st HCC Recurrence-Free Survival | 2nd HCC Recurrence-Free Survival | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | ||||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Age | ≤74 >74 | 1 1.289 (0.59–2.84) | 0.5283 | 1 1.383 (0.40–4.74) | 0.606 | ||||
| Sex | Male Female | 1 10.45 (0.50–2.18) | 0.906 | 1 1.374 (0.42–4.52) | 0.6007 | ||||
| HBsAg | Positive Negative | 5.3772 × 10−9 (0–0) 1 | 0.9991 | 3.9605 × 10−8 (0–0) 1 | 0.9991 | ||||
| Alcohol history | + − | 0.628 (0.22–1.81) 1 | 1.3894 | 0.733 (0.16–3.42) | 0.6931 | ||||
| Diabetes mellitus | + − | 1.347 (0.62–2.90) 1 | 0.4473 | 1.761 (0.51–6.03) 1 | 0.3675 | ||||
| IFN treatment history | + − | 0.760 (0.34–1.68) 1 | 0.4972 | 0.359 (0.08–1.68) 1 | 0.1985 | 0.245 (0.05–1.18) 1 | 0.0789 | ||
| Child–Pugh | 5 6–7 | 1.024 (0.49–2.13) 1 | 0.9486 | 1.032 (0.31–3.40) 1 | 0.9585 | ||||
| mALBI grade | 1–2a 2b-3 | 0.804 (0.39–1.67) 1 | 0.5591 | 0.669 (0.20–2.22) 1 | 0.5113 | ||||
| FIB-4 index | ≤3.25 >3.25 | 0.914 (0.35–2.40) 1 | 0.8554 | 1.118 (0.24–5.20) 1 | 0.887 | ||||
| Platelet count(× 104/mm3) | ≤15.8 >15.8 | 1 0.450 (0.13–1.49) | 0.1903 | 1 0.387 (0.12–1.30) | 0.1243 | 1 0.671 (0.14–3.12) | 0.611 | ||
| Albumin (g/dL) | ≤3.8 >3.8 | 1 0.639 (0.28–1.44) | 0.2816 | 1 0.605 (0.16–2.29) | 0.4584 | ||||
| AST (IU/L) | ≤42 >42 | 0.964 (0.44–2.12) 1 | 0.9261 | 0.770 (0.20–2.91) 1 | 0.7004 | ||||
| ALT (IU/L) | ≤39 >39 | 1.111 (0.52–2.35) 1 | 0.7839 | 0.625 (0.17–2.35) 1 | 0.4882 | ||||
| Tumor size (mm) | ≤20 >20 | 1.104 (0.45–2.72) 1 | 0.8294 | 1.689 (0.36–7.82) 1 | 0.5032 | ||||
| Tumor number | Single Multiple | 0.540 (0.24–1.22) 1 | 0.1388 | 0.469 (0.20–1.07) 1 | 0.0731 | 0.180 (0.05–0.60) 1 | 0.0051 | 0.141 (0.04–0.48) 1 | 0.0016 |
| AFP (ng/mL) | ≤10 >10 | 0.670 (0.31–1.44) 1 | 0.3066 | 0.454 (0.12–1.72) 1 | 0.2451 | ||||
| DCP (mAU/mL) | ≤40 >40 | 0.788 (0.34–1.85) 1 | 0.5839 | 1.750 (0.38–8.14) 1 | 0.4755 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuromatsu, R.; Ide, T.; Okamura, S.; Noda, Y.; Kamachi, N.; Nakano, M.; Shirono, T.; Shimose, S.; Iwamoto, H.; Kuwahara, R.; et al. Hepatitis C Virus Elimination Using Direct Acting Antivirals after the Radical Cure of Hepatocellular Carcinoma Suppresses the Recurrence of the Cancer. Cancers 2022, 14, 2295. https://doi.org/10.3390/cancers14092295
Kuromatsu R, Ide T, Okamura S, Noda Y, Kamachi N, Nakano M, Shirono T, Shimose S, Iwamoto H, Kuwahara R, et al. Hepatitis C Virus Elimination Using Direct Acting Antivirals after the Radical Cure of Hepatocellular Carcinoma Suppresses the Recurrence of the Cancer. Cancers. 2022; 14(9):2295. https://doi.org/10.3390/cancers14092295
Chicago/Turabian StyleKuromatsu, Ryoko, Tatsuya Ide, Shusuke Okamura, Yu Noda, Naoki Kamachi, Masahito Nakano, Tomotake Shirono, Shigeo Shimose, Hideki Iwamoto, Reiichiro Kuwahara, and et al. 2022. "Hepatitis C Virus Elimination Using Direct Acting Antivirals after the Radical Cure of Hepatocellular Carcinoma Suppresses the Recurrence of the Cancer" Cancers 14, no. 9: 2295. https://doi.org/10.3390/cancers14092295
APA StyleKuromatsu, R., Ide, T., Okamura, S., Noda, Y., Kamachi, N., Nakano, M., Shirono, T., Shimose, S., Iwamoto, H., Kuwahara, R., Arinaga-Hino, T., Niizeki, T., Zaizen, Y., Takaki, H., Shirachi, M., Koga, H., & Torimura, T. (2022). Hepatitis C Virus Elimination Using Direct Acting Antivirals after the Radical Cure of Hepatocellular Carcinoma Suppresses the Recurrence of the Cancer. Cancers, 14(9), 2295. https://doi.org/10.3390/cancers14092295