
Where Do We Stand in the Management of Oligometastatic Prostate Cancer? A Comprehensive Review

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Evidence Acquisition
3. Evidence Synthesis
3.1. Prevalence of OMPC
3.2. Defining Oligometastatic Disease
3.3. Imaging Modalities in the Detection of Oligometastatic Disease

{kind=link}
| Imaging Techniques | Sensitivity | Specificity | Change in Management | ||||
|---|---|---|---|---|---|---|---|
| LN Staging | M Staging | Overall | LN Staging | M Staging | Overall | ||
| CT [19] | 38% | 38% | 38% | 98% | 98% | 98% | NA |
| Bone scan [19] | NA | 79% | 79% | NA | 82% | 82% | NA |
| Whole-body MRI [26] | 41% | 85% | 60% | 92% | 85% | 95% | NR |
| Fluciclovine PET [21] | NR | NR | 87% | NR | NR | 66% | NR |
| Choline PET [20] | 62% | 80% | 89% | 92% | 89% | 89% | 18–48% * |
| PSMA PET [24] | 65% | 92% | 86% | 94% | 92% | 86% | 21–41% * |
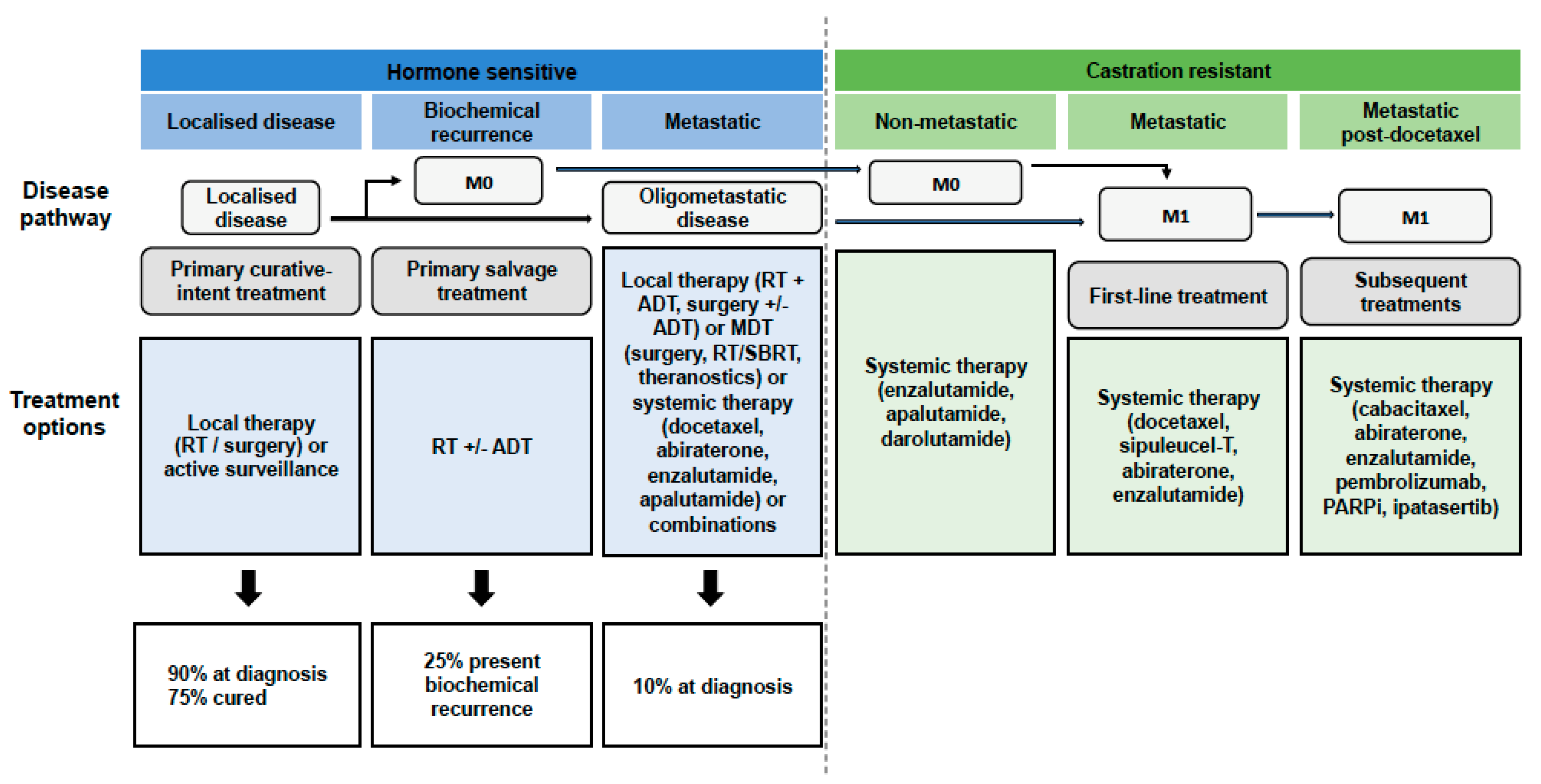
3.4. Treatment
3.4.1. Local Therapy to the Primary Tumour
RT of Primary Prostate Tumour + ADT
Surgery on Primary Prostate Tumours
3.4.2. MDT
Resection of Distant Metastases
SBRT
Theragnostics
3.4.3. Systemic Therapy
Chemotherapy Agents (Docetaxel)
New Androgen Receptor-Targeted Agents
Combinations
Genomics and New Agents
| Treatments | Studies | Outcomes | |
|---|---|---|---|
| Local therapy | RT | HORRADS (RCT) [34] | OS: HR 1.11; 95%CI, 0.87–1.43; p = 4. * OS < 5 lesions (HR, 0.68; 95%CI, 0.42–1.10), 5 to 15 (HR 1.18; 95%CI, 0.74–1.89) and >15 (HR 0.93; 95%CI, 0.66–1.32). |
| STAMPEDE (arm M) (RCT) [35] | OS: HR 0.92; 95%CI, 0.80–1.06; p = 0.266. PFS: HR 0.76; 95%CI, 0.68–0.84; p < 0.0001. * PFS low metastatic burden: HR 0.59; 95%CI, 0.49–0.72; p = 0.0001. * 3-year OS low metastatic burden: (81% vs. 73%; HR 0.68; 95%CI, 0.52–0.90; p = 0.007). | ||
| Surgery of primary tumour | Culp et al. (SEER datebase) [33] | OS: 67 vs 22.5% p < 0.001. CSS: 75 vs 48% p < 0.001. | |
| Heidenreich et al. (retrospective case-control) [37] | CSS: 96% vs. 84%, median of 34.5 months. | ||
| Heidenreich et al. (retrospective cohort) [38] | OS: 85% with RP + ADT. | ||
| TRoMbone (RCT) [41] | Feasibility to randomise: demonstrated. QoL: 0% erectile function, 16.7% incontinent six months after surgery, 41.7% positive margin rate, 82.6% Gleason 8–10, 87.5% pT3. | ||
| MDT | Surgery (sLND) | Suardi et al. (prospective study) [48] | 8-year clinical recurrence-free survival: 38% |
| Rigatti et al. (prospective study) [49] | 5-year clinical recurrence-free survival: 34% | ||
| SBRT | STOMP (RCT) [51,52] | ADT-free survival: HR 0.60; 80%CI, 0.40–0.90; p = 0.11. Five-year ADT-free survival: 8% surveillance vs. 34% MDT (HR: 0.57; 80%CI, 0.38–0.84; p = 0.06). | |
| ORIOLE (RCT) [53] | PFS: HR: 0.30; 0.11–0.81; p = 0.002. | ||
| POPSTAR (RCT) [54] | Feasibility rate: 97%; 95%CI, 84–100%. ADT free 24 months: 48%; 95%CI, 31–75%. | ||
| Theragnostics | Privé et al. (Pilot study) [63] | Stabilisation of PSA velocity: 10/10 PSA decline > 50%: 5/10 PSA decline after 24 weeks: 3/10 Biochemical complete response: 1/10 | |
| Systemic therapy | Chemotherapy (Docetaxel) | GETUG-AFU 15 (RCT) [69] | OS: HR 1.01; 95%CI, 0.75–1.36. |
| CHAARTED (RCT) [67] | OS: HR 0.72; 95%CI, 0.59–0.89; p < 0.001. * OS HV: HR 0.63; 95%CI, 0.50–0.79. * OS LV: HR 1.04; 95%CI, 0.70–1.55. | ||
| STAMPEDE (arm C) (RCT) [68] | OS: HR 0.81; 95%CI, 0.69–0.95; p = 0.009. | ||
| Abiraterone | LATITUDE (RCT) [71] | OS: HR 0.62; 95%CI, 0.56–0.78; p < 0.001. rPFS: HR 0.47; 95%CI, 0.39–0.55. | |
| STAMPEDE (arm G) (RCT) [72] | OS: HR 0.63; 95%CI, 0.52–0.76. * OS HR M1: HR 0.54; 95%CI, 0.43–0.69. * OS LR M1: HR 0.55; 95%CI, 0.41–0.76. | ||
| Enzalutamide | ARCHES (RCT) [74] | OS: HR 0.81; 95%CI, 0.53–1.25. | |
| ENZAMET (RCT) [75] | OS: HR 0.67; 95%CI, 0.52–0.86. * OS HV: HR 0.65; 95%CI, 0.42–0.99. * OS LV: HR 0.38; 95%CI, 0.21–0.69. | ||
| Apalutamide | TITAN (RCT) [76,77] | OS: HR 0.65; 95%CI, 0.53–0.79. OS adjusted by crossover: 0.52. * OS HV: HR 0.70; 95%CI, 0.56–0.88. * OS LV: HR 0.52; 95%CI, 0.35–0.79. rPFS: HR 0.48; 95%CI, 0.39–0.60. | |
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hellman, S.; Weichselbaum, R.R. Oligometastases. J. Clin. Oncol. 1995, 13, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Gillessen, S.; Omlin, A.; Attard, G.; de Bono, J.S.; Efstathiou, E.; Fizazi, K.; Halabi, S.; Nelson, P.S.; Sartor, O.; Smith, M.R.; et al. Management of patients with advanced prostate cancer: Recommendations of the St Gallen Advanced Prostate Cancer Consensus Conference (APCCC) 2015. Ann. Oncol. 2015, 26, 1589–1604. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.; Vapiwala, N.; Schaeffer, E.M.; Ryan, C.J. Oligometastatic Prostate Cancer: A Shrinking Subset or an Opportunity for Cure? Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Reyes, D.K.; Pienta, K.J. The biology and treatment of oligometastatic cancer. Oncotarget 2015, 6, 8491–8524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tosoian, J.J.; Gorin, M.A.; Ross, A.E.; Pienta, J.J.T.M.A.G.A.E.R.K.J.; Tran, P.T.; Schaeffer, E.M. Oligometastatic prostate cancer: Definitions, clinical outcomes, and treatment considerations. Nat. Rev. Urol. 2016, 14, 15–25. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2018: GLO-BOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar]
- Kelly, S.P.; Anderson, W.F.; Rosenberg, P.S.; Cook, M.B. Past, Current, and Future Incidence Rates and Burden of Metastatic Prostate Cancer in the United States. Eur. Urol. Focus 2018, 4, 121–127. [Google Scholar] [CrossRef]
- Soloway, M.S.; Hardeman, S.W.; Hickey, D.; Todd, B.; Soloway, S.; Raymond, J.; Moinuddin, M. Stratification of patients with metastatic prostate cancer based on extent of disease on initial bone scan. Cancer 1988, 61, 195–202. [Google Scholar] [CrossRef]
- Ost, P.; Jereczek-Fossa, B.A.; Van As, N.; Zilli, T.; Muacevic, A.; Olivier, K.; Henderson, D.; Casamassima, F.; Orecchia, R.; Surgo, A.; et al. Progression-free survival following stereotactic body radiotherapy for oligometastatic prostate cancer treat-ment-naive recurrence: A multi-institutional analysis. Eur. Urol. 2016, 69, 9–12. [Google Scholar] [CrossRef]
- Francini, E.; Gray, K.P.; Xie, W.; Shaw, G.K.; Valença, L.; Bernard, B.; Albiges, L.; Harshman, L.C.; Kantoff, P.W.; Taplin, M.E.; et al. Time of metastatic disease presentation and volumen of disease are prognostic for metastatic hormone sensitive prostate cancer. Prostate 2018, 78, 889–895. [Google Scholar] [CrossRef]
- Lussier, Y.A.; Xing, H.R.; Salama, J.K.; Khodarev, N.N.; Huang, Y.; Zhang, Q.; Khan, S.A.; Yang, X.; Hasselle, M.D.; Darga, T.E.; et al. MicroRNA expression characterises oligometastasis(es). PLoS ONE 2011, 6, e28650. [Google Scholar] [CrossRef] [PubMed]
- Rubin, P.; Brasacchio, R.; Katz, A. Solitary Metastases: Illusion Versus Reality. Semin. Radiat. Oncol. 2006, 16, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Gillessen, S.; Attard, G.; Beer, T.M.; Beltran, H.; Bossi, A.; Bristow, R.; Carver, B.; Castellano, D.; Chung, B.H.; Clarke, N.; et al. Management of patients with advanced prostate cancer: The report of the Advanced Prostate Cancer Consensus Confer-ence (APCCC) 2017. Eur. Urol. 2018, 73, 178–211. [Google Scholar] [CrossRef] [Green Version]
- Kyriakopoulos, C.E.; Chen, Y.H.; Carducci, M.A.; Liu, G.; Jarrard, D.F.; Hahn, N.M.; Shevrin, D.H.; Dreicer, R.; Hussain, M.; Eisenberger, M.; et al. Chemohormonal therapy in metastatic hormone sensitive prostate cancer: Long term survival analysis of the randomised phase III E3805 chaarted trial. J. Clin. Oncol. 2018, 36, 1080–1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fizazi, K.; Tran, N.; Fein, L.; Matsubara, N.; Rodriguez-Antolin, A.; Alekseev, B.Y.; Özgüroglu, M.; Ye, D.; Feyerabend, S.; Protheroe, A.; et al. Abiraterone acetate plus prednisone in patients with newly diagnosed high risk metastatic castration sen-sitive prostate cancer (LATITUDE): Final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet 2019, 20, 686–700. [Google Scholar] [CrossRef]
- Gandaglia, G.; Karakiewicz, P.I.; Briganti, A.; Passoni, N.M.; Schiffmann, J.; Trudeau, V.; Graefen, M.; Montorsi, F.; Sun, M. Impact of the side of metastases on survival in patients with metastatic prostate cancer. Eur. Urol. 2015, 68, 325–334. [Google Scholar] [CrossRef]
- Mahjoub, S.; Heidenreich, A. Oligometastatic prostate cancer: Definition and the role of local and systemic therapy: A narra-tive review. Transl. Androl. Urol. 2021, 10, 3167–3175. [Google Scholar] [CrossRef]
- Weber, M.; Kurek, C.E.; Barbato, F.; Eiber, M.; Maurer, T.; Nader, M.; Hadaschik, B.; Grünwald, V.; Herrmann, K.; Wetter, A.; et al. PSMA-Ligand PET for Early Castration-Resistant Prostate Cancer: A Retrospective Single-Center Study. J. Nucl. Med. 2020, 62, 88–91. [Google Scholar] [CrossRef]
- Thomas, L.; Balmus, C.; Ahmadzadehfar, H.; Essler, M.; Strunk, H.; Bundschuh, R.A. Assesment of bone metastases in pa-tients with prostate cancer. A comparison between 99mTc-bone-scintigraphy and [68Ga]Ga-PSMA PET/CT. Pharmaceuticals 2017, 10, 68. [Google Scholar] [CrossRef] [Green Version]
- Fanti, S.; Minozzi, S.; Castellucci, P.; Balduzzi, S.; Herrmann, K.; Krause, B.J.; Oyen, W.; Chiti, A. PET/CT with 11C-choline for evaluation of prostate cancer patients with biochemical recurrence: Meta-analysis and critical review of available data. Eur. J. Pediatr. 2015, 43, 55–69. [Google Scholar] [CrossRef]
- Ren, J.; Yuan, L.; Wen, G.; Yang, J. The value of anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid PET/CT in the diagnosis of recurrent prostate carcinoma: A meta-analysis. Acta Radiol. 2015, 57, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.D.; Jethwa, K.R.; Ost, P.; Williams, S.; Kwon, E.D.; Lowe, V.J.; Davis, B.J. Prostate cancer–specific PET radiotracers: A review on the clinical utility in recurrent disease. Pract. Radiat. Oncol. 2018, 8, 28–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afshar-Oromieh, A.; Hetzheim, H.; Kratochwil, C.; Benesova, M.; Eder, M.; Neels, O.C.; Eisenhut, M.; Kübler, W.; Hol-land-Letz, T.; Giesel, F.L.; et al. The theranostic PSMA ligand PSMA-617 in the diagnosis of prostate cancer by PET/CT: Bio-distribution in humans, radiation dosimetry and first evaluation of tumor lesions. J. Nucl. Med. 2015, 56, 1697–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perera, M.; Papa, N.; Christidis, D.; Wetherell, D.; Hofman, M.S.; Murphy, D.G.; Bolton, D.; Lawrentschuk, N. Sensitivity, Specificity, and Predictors of Positive 68 Ga–Prostate-specific Membrane Antigen Positron Emission Tomography in Advanced Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. 2016, 70, 926–937. [Google Scholar] [CrossRef]
- Jadvar, H. Is there use for FDG-PET in prostate cancer? Semin. Nucl. Med. 2016, 46, 502–506. [Google Scholar] [CrossRef] [Green Version]
- Larbi, A.; Dallaudière, B.; Pasoglou, V.; Padhani, A.; Michoux, N.; Berg, B.C.V.; Tombal, B.; Lecouvet, F.E. Whole body MRI (WB-MRI) assessment of metastatic spread in prostate cancer: Therapeutic perspectives on targeted management of oli-gometastatic disease. Prostate 2016, 76, 1024–1033. [Google Scholar] [CrossRef]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative intent surgery or radiotherapy (proPSMA): A prostective, randomised, multicentre study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef]
- Hicks, R.J.; Murphy, D.G.; Williams, S.G. Seduction by sensibility: Reality, ilusión or delusion? The challenge of assessing outcomes after PSMA imaging selection of patiens for treatment. J. Nucl. Med. 2017, 58, 1969–1971. [Google Scholar] [CrossRef] [Green Version]
- Phillips, R.; Shi, W.Y.; Deek, M.; Radwan, N.; Lim, S.J.; Antonarakis, E.S.; Rowe, S.P.; Ross, A.E.; Gorin, M.A.; Deville, C.; et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer. JAMA Oncol. 2020, 6, 650–659. [Google Scholar] [CrossRef] [Green Version]
- Mottet, N.; van den Bergh, R.C.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-ESTRO-ESUR-SIOG. Guidelines on Prostate Cancer. Eur. Urol. 2021, 79, 243–262. [Google Scholar]
- Kadmon, D.; Heston, W.D.; Fair, W.R. Treatment of a Metastatic Prostate Derived Tumor with Surgery and Chemotherapy. J. Urol. 1982, 127, 1238–1242. [Google Scholar] [CrossRef]
- Erler, J.T.; Bennewith, K.L.; Cox, T.R.; Lang, G.; Bird, D.; Koong, A.; Le, Q.-T.; Giaccia, A.J. Hypoxia-Induced Lysyl Oxidase Is a Critical Mediator of Bone Marrow Cell Recruitment to Form the Premetastatic Niche. Cancer Cell 2009, 15, 35–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deek, M.P.; Phillips, R.M.; Tran, P.T. Local therapies in oligometastatic and olioprogressive prostate cancer. Semin. Radiat. Oncol. 2021, 31, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Culp, S.H.; Schellhammer, P.F.; Williams, M.B. Might Men Diagnosed with Metastatic Prostate Cancer Benefit from Definitive Treatment of the Primary Tumor? A SEER-Based Study. Eur. Urol. 2014, 65, 1058–1066. [Google Scholar] [CrossRef] [PubMed]
- Boevé, L.M.; Hulshof, M.C.; Vis, A.N.; Zwinderman, A.H.; Twisk, J.W.; Witjes, W.P.; Delaere, K.P.; Van Moorselaar, R.J.A.; Verhagen, P.C.; Van Andel, G. Effect on Survival of Androgen Deprivation Therapy Alone Compared to Androgen Deprivation Therapy Combined with Concurrent Radiation Therapy to the Prostate in Patients with Primary Bone Metastatic Prostate Cancer in a Prospective Randomised Clinical Trial: Data from the HORRAD Trial. Eur. Urol. 2018, 75, 410–418. [Google Scholar] [CrossRef]
- Parker, C.C.; James, N.D.; Brawley, C.D.; Clarke, N.W.; Hoyle, A.P.; Ali, A.; Ritchie, A.W.S.; Attard, G.; Chowdhury, S.; Cross, W.; et al. Systemic Therapy for Advanced or Metastatic Prostate cancer: Evaluation of Drug Efficacy (STAMPEDE) investi-gators. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomised controlled phase 3 trial. Lancet 2018, 392, 2353–2366. [Google Scholar] [CrossRef] [Green Version]
- Burdett, S.; Boevé, L.M.; Ingleby, F.C.; Fisher, D.; Rydzewska, L.H.; Vale, C.; van Andel, G.; Clarke, N.W.; Hulshof, M.C.; James, N.D.; et al. STOPCAP M1 Radiotherapy Collaborators. Prostate Radiotherapy for Metastatic Hormone-sensitive Pros-tate Cancer: A STOPCAP Systematic Review and Meta-analysis. Eur. Urol. 2019, 76, 115–124. [Google Scholar] [CrossRef] [Green Version]
- Heidenreich, A.; Pfister, D.; Porres, D. Cytoreductive Radical Prostatectomy in Patients with Prostate Cancer and Low Volume Skeletal Metastases: Results of a Feasibility and Case-Control Study. J. Urol. 2014, 193, 832–838. [Google Scholar] [CrossRef]
- Heidenreich, A.; Fossati, N.; Pfister, D.; Suardi, N.; Montorsi, F.; Shariat, S.; Grubmüller, B.; Gandaglia, G.; Briganti, A.; Karnes, R.J. Cytoreductive Radical Prostatectomy in Men with Prostate Cancer and Skeletal Metastases. Eur. Urol. Oncol. 2018, 1, 46–53. [Google Scholar] [CrossRef]
- Jang, W.S.; Kim, M.S.; Jeong, W.S.; Chang, K.D.; Cho, K.S.; Ham, W.S.; Rha, K.H.; Hong, S.J.; Choi, Y.D. Does robot-assisted radical prostatectomy benefit patients with prostate cancer and bone oligometastases? BJU Int. 2018, 121, 225–231. [Google Scholar] [CrossRef]
- Dai, B.; Zhang, J.; Wang, H.; Wang, Q.; Kong, Y.; Zhu, Y.; Qin, X.; Lin, G.; Ye, D. 618MO Local therapy to the primary tumour for newly diagnosed, oligo-metastatic prostate cancer: A prospective randomized, phase II, open-label trial. Ann. Oncol. 2020, 31, S512. [Google Scholar] [CrossRef]
- Sooriakumaran, P.; Wilson, C.; Rombach, I.; Hassanali, N.; Aning, J.; Lamb, A.D.; Cathcart, P.; Eden, C.; Ahmad, I.; Rajan, P.; et al. Feasibility and safety of radical prostatectomy for oligo-metastatic prostate cancer: The Testing Radical prostatectomy in men with prostate cancer and oligo-Metastases to the bone (TRoMbone) trial. Br. J. Urol. 2021. [Google Scholar] [CrossRef] [PubMed]
- O’Shaughnessy, M.J.; McBride, S.M.; Vargas, H.A.; Touijer, K.A.; Morris, M.J.; Danila, D.C.; Laudone, V.P.; Bochner, B.; Sheinfeld, J.; Dayan, E.S.; et al. A Pilot Study of a Multimodal Treatment Paradigm to Accelerate Drug Evaluations in Early-stage Metastatic Prostate Cancer. Urology 2016, 102, 164–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NCT03678025. Standard Systemic Therapy with or without Definitive Treatment in Treating Participants with Metastatic Prostate Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03678025 (accessed on 12 March 2022).
- NCT02454543. Impact of Radical Prostatectomy as Primary Treatment in Patients with Prostate Cancer with Limited Bone Metastases. Available online: https://clinicaltrials.gov/ct2/show/NCT02454543 (accessed on 12 March 2022).
- ISRCTN15704862. Testing Radical Prostatectomy in Men with Prostate Cancer and OligoMetastases to bone (TRoMbone) Trial. Available online: https://clinicaltrials.gov/ct2/show/ISRCTN15704862 (accessed on 12 March 2022).
- Fossati, N.; Giannarini, G.; Joniau, S.; Sedelaar, M.; Sooriakumaran, P.; Spahn, M.; Rouprêt, M. Newly Diagnosed Oligometastatic Prostate Cancer: Current Controversies and Future Developments. Eur. Urol. Oncol. 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Ost, P.; Bossi, A.; Decaestecker, K.; De Meerleer, G.; Giannarini, G.; Karnes, R.J.; Roach, M., 3rd; Briganti, A. Metastasis-directed therapy of regional and distant recurrences after curative treatment of prostate cancer: A systematic review of the literature. Eur. Urol. 2015, 67, 852–863. [Google Scholar] [CrossRef]
- Suardi, N.; Gandaglia, G.; Gallina, A.; Di Trapani, E.; Scattoni, V.; Vizziello, D.; Cucchiara, V.; Bertini, R.; Colombo, R.; Picchio, M.; et al. Long-term outcomes of salvage lymph node dissection for clinically recurrent prostate cancer: Results of a sin-gle-institution series with a minimum follow-up of 5 years. Eur. Urol. 2015, 67, 299–309. [Google Scholar] [CrossRef] [Green Version]
- Rigatti, P.; Suardi, N.; Briganti, A.; Da Pozzo, L.F.; Tutolo, M.; Villa, L.; Gallina, A.; Capitanio, U.; Abdollah, F.; Scattoni, V.; et al. Pelvic/retroperitoneal salvage lymph node dissection for patients treated with radical prostatectomy with biochemical re-currence and nodal recurrence detected by [11C]choline positron emission tomography/computed tomography. Eur. Urol. 2011, 60, 935–943. [Google Scholar] [CrossRef]
- Fossati, N.; Suardi, N.; Gandaglia, G.; Bravi, C.A.; Soligo, M.; Karnes, R.J.; Shariat, S.; Battaglia, A.; Everaerts, W.; Joniau, S.; et al. Identifying the Optimal Candidate for Salvage Lymph Node Dissection for Nodal Recurrence of Prostate Cancer: Re-sults from a Large, Multi-institutional Analysis. Eur. Urol. 2019, 75, 176–183. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, P.G.B.; Yaremko, B.P.; et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): A randomised, phase 2, open-label trial. Lancet 2019, 393, 2051–2058. [Google Scholar] [CrossRef]
- Ost, P.; Reynders, D.; Decaestecker, K.; Fonteyne, V.; Lumen, N.; De Bruycker, A.; Lambert, B.; Delrue, L.; Bultijnck, R.; Claeys, T.; et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J. Clin. Oncol. 2018, 36, 446–453. [Google Scholar] [CrossRef] [Green Version]
- Ost, P.; Reynders, D.; Decaestecker, K.; Fonteyne, V.; Lumen, N.; De Bruycker, A.; Lambert, B.; Delrue, L.; Bultijnck, R.; Goe-tghebeur, E.; et al. Surveillance or metastasis-directed therapy for oligometastatic prostate cancer recurrence (STOMP): Five-year results of a randomised phase II trial. J. Clin. Oncol. 2020, 38, 6. [Google Scholar] [CrossRef]
- Siva, S.; Bressel, M.; Murphy, D.G.; Shaw, M.; Chander, S.; Violet, J.; Tai, K.H.; Udovicich, C.; Lim, A.; Selbie, L.; et al. Stere-otactic ablative body radiotherapy (SABR) for oligometastatic prostate cancer: A prospective clinical trial. Eur. Urol. 2018, 74, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Preisser, F.; Banek, S.; Wenzel, M.; Graefen, M.; Steuber, T.; Tilki, D.; Mandel, P. Management and treatment options for patients with the novo and recurrent hormone-sensible oligometastatic prostate cancer. Prostate Int. 2021, 9, 113–118. [Google Scholar] [CrossRef]
- Viani, G.A.; Arruda, C.V.; Hamamura, A.C.; Faustino, A.C.; Freitas Bendo Danelichen, A.; Guimarães, F.S. Body Radiotherapy for Oligometastatic Prostate Cancer Recurrence: A Meta-analysis. Am. J. Clin. Oncol. 2020, 43, 73. [Google Scholar] [CrossRef] [PubMed]
- NC03569241. The Multicenter, Randomized, Phase 2 PEACE V-STORM Trial: Defining the Best Salvage Treatment for Oligorecurrent Nodal Prostate Cancer Metastases. Available online: https://clinicaltrials.gov/ct2/show/NCT03569241 (accessed on 12 March 2022).
- NCT03902951. Antiandrogen Therapy and SBRT in Treating Patients with Recurrent Metastatic Prostate Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03902951 (accessed on 12 March 2022).
- NCT03795207. Prostate Cancer with Oligometastatic Relapse: Combining Stereotactic Ablative Radiotherapy and Durval-umab (MEDI4736) (POSTCARD). Available online: https://clinicaltrials.gov/ct2/show/NCT0379527 (accessed on 12 March 2022).
- NCT04641078. Stereotactic Body Radiotherapy with or without Darolutamide for OligoRecurrent Prostate Cancer (DART). Available online: https://clinicaltrials.gov/ct2/show/NCT04641078 (accessed on 12 March 2022).
- NCT04423211. Treating Prostate Cancer that Has Come Back after Surgery with Apalutamide and Targeted Radiation Using PET/CT Imaging. Available online: https://clinicaltrials.gov/ct2/show/NCT04423211 (accessed on 12 March 2022).
- Plichta, K.A.; Graves, S.A.; Buatti, J.M. Prostate-specific membrane antigen (PSMA) theranostics for treatment of oligometa-static prostate cancer. Int. J. Mol. Sci. 2021, 22, 12095. [Google Scholar] [CrossRef] [PubMed]
- Silver, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-specific membrane antigen expresión in normal and malignant human tissues. Clin. Cancer Res. 1997, 3, 81–85. [Google Scholar] [PubMed]
- Okamoto, S.; Thieme, A.; Allmann, J.; D’Alessandria, C.; Maurer, T.; Retz, M.; Tauber, R.; Heck, M.M.; Wester, H.J.; Tamaki, N.; et al. Radiation dosimetry for 177Lu-PSMA I&T in metastatic castration resistant prostate cancer. Absorbed doce in nor-mal organs and tumor lesions. J. Nucl. Med. 2017, 58, 445. [Google Scholar]
- Privé, B.M.; Peters, S.M.; Muselaers, C.H.J.; van Oort, I.M.; Janssen, M.J.; Sedelaar, J.M.; Konijnenberg, M.W.; Zámecnik, P.; Uijen, M.J.; Schilham, M.G.; et al. Lutetium-177-PSMA-617 in low volumen hormone-sensitive metastatic prostate cancer: A prospective pilot study. Clin. Cancer Res. 2021, 27, 3595–3601. [Google Scholar] [CrossRef]
- Privé, B.M.; Janssen, M.J.; Van Oort, I.M.; Muselaers, C.H.; Jonker, M.A.; De Groot, M.; Mehra, N.; Verzijlbergen, J.F.; Scheenen, T.W.; Zámecnik, P.; et al. Lutetium-177-PSMA I&T as metastases directed therapy in oligometatatic hormone sen-sitive prostate cancer, a randomised controlled trial. BMC Cancer 2020, 20, 884. [Google Scholar]
- NCT04343885. In Men with Metastatic Prostate Cancer, What Is the Safety and Benefit of Lutetium-177 PSMA Radionuclide Treatment in Addition to Chemotherapy. Available online: https://ClinicalTrials.gov/show/NCT04343885 (accessed on 12 March 2022).
- NCT04720157. An International Prospective Open Label, Radomized, Pase II Study Comparing 177Lu-PSMA-167 in Com-binations with SoC versus SoC alone, in Adults Male Patients with mHSPC. Available online: https://ClinicalTrials.gov/show/NCT04720157 (accessed on 12 March 2022).
- James, N.D.; Sydes, M.R.; Clarke, N.W.; Mason, M.D.; Dearnaley, D.P.; Spears, M.R.; Ritchie, A.W.S.; Parker, C.C.; Russell, J.M.; Attard, G.; et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): Survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet 2016, 387, 1163–1177. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, C.J.; Chen, Y.-H.; Carducci, M.; Liu, G.; Jarrard, D.F.; Eisenberger, M.; Wong, Y.-N.; Hahn, N.; Kohli, M.; Cooney, M.M.; et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N. Engl. J. Med. 2015, 373, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Gravis, G.; Fizazi, K.; Joly, F.; Oudard, S.; Priou, F.; Esterni, B.; Latorzeff, I.; Delva, R.; Krakowski, I.; Laguerre, B.; et al. An-drogen-deprivation therapy alone or with docetaxel in non-castrate metastatic prostate cancer (GETUG-AFU 15): A random-ised, open-label, phase 3 trial. Lancet 2013, 14, 149–158. [Google Scholar] [CrossRef]
- Vale, C.L.; Burdett, S.; Rydzewska, L.H.M.; Albiges, L.; Clarke, N.W.; Fisher, D.; Fizazi, K.; Gravis, G.; James, N.D.; Mason, M.D.; et al. Addition of docetaxel or bisphosphonates to standard of care in men with localised or metastatic, hormone-sensitive prostate cancer: A systematic review and meta-analyses of aggregate data. Lancet Oncol. 2016, 17, 243–256, Correction to Lancet Oncol. 2016, 17, 248–252. [Google Scholar] [CrossRef] [Green Version]
- Fizazi, K.; Tran, N.; Fein, L.; Matsubara, N.; Rodriguez-Antolin, A.; Alekseev, B.Y.; Özgüroğlu, M.; Ye, D.; Feyerabend, S.; Protheroe, A.; et al. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N. Engl. J. Med. 2017, 377, 352–360. [Google Scholar] [CrossRef]
- James, N.D.; De Bono, J.S.; Spears, M.R.; Clarke, N.W.; Mason, M.D.; Dearnaley, D.P.; Ritchie, A.W.S.; Amos, C.L.; Gilson, C.; Jones, R.J.; et al. Abiraterone for Prostate Cancer Not Previously Treated with Hormone Therapy. N. Engl. J. Med. 2017, 377, 338–351. [Google Scholar] [CrossRef]
- Rydzewska, L.H.; Burdett, S.; Vale, C.; Clarke, N.W.; Fizazi, K.; Kheoh, T.; Mason, M.D.; Miladinovic, B.; James, N.D.; Parmar, M.K.; et al. Adding abiraterone to androgen deprivation therapy in men with metastatic hormone-sensitive prostate cancer: A systematic review and meta-analysis. Eur. J. Cancer 2017, 84, 88–101. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, A.J.; Szmulewitz, R.Z.; Petrylak, D.P.; Holzbeierlein, J.; Villers, A.; Azad, A.; Alcaraz, A.; Alekseev, B.; Iguchi, T.; Shore, N.D.; et al. ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy With Enzalutamide or Placebo in Men With Metastatic Hormone-Sensitive Prostate Cancer. J. Clin. Oncol. 2019, 37, 2974–2986. [Google Scholar] [CrossRef]
- Davis, I.D.; Martin, A.J.; Stockler, M.R.; Begbie, S.; Chi, K.N.; Chowdhury, S.; Coskinas, X.; Frydenberg, M.; Hague, W.E.; Horvath, L.G.; et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N. Engl. J. Med. 2019, 381, 121–131. [Google Scholar] [CrossRef]
- Chi, K.N.; Agarwal, N.; Bjartell, A.; Chung, B.H.; Pereira de Santana Gomes, A.J.; Given, R.; Juárez Soto, Á.; Merseburger, A.S.; Özgüroğlu, M.; Uemura, H.; et al. Apalutamide for Metastatic, Castration- Sensitive Prostate Cancer. N. Engl. J. Med. 2019, 381, 13–24. [Google Scholar] [CrossRef]
- Chi, K.N.; Chowdhury, S.; Bjartell, A.; Chung, B.H.; Gomes, A.J.P.D.S.; Given, R.; Soto, J.; Merseburger, A.S.; Ozguroglu, M.; Uemura, H.; et al. Final analysis results from TITAN: A phase III study of apalutamide (APA) versus placebo (PBO) in patients (pts) with metastatic castration-sensitive prostate cancer (mCSPC) receiving androgen deprivation therapy (ADT). J. Clin. Oncol. 2021, 39, 11. [Google Scholar] [CrossRef]
- Wang, L.; Paller, C.J.; Hong, H.; De Felice, A.; Alexander, G.C.; Brawley, O. Comparison of Systemic Treatments for Metastatic Castration-Sensitive Prostate Cancer A Systematic Review and Network Meta-analysis. JAMA Oncol. 2021, 7, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Ferro, M.; Lucarelli, G.; Crocetto, F.; Dolce, P.; Verde, A.; La Civita, E.; Zappavigna, S.; de Cobelli, O.; Di Lorenzo, G.; Facchini, B.A.; et al. First-line systemic therapy for metastatic castration-sensitive prostate cancer: An updated systematic review with novel findings. Crit. Rev. Oncol. 2020, 157, 103198. [Google Scholar] [CrossRef] [PubMed]
- Sathianathen, N.J.; Koschel, S.; Thangasamy, I.; Teh, J.; Alghazo, O.; Butcher, G.; Howard, H.; Kapoor, J.; Lawrentschuk, N.; Siva, S.; et al. Indirect Comparisons of Efficacy between Combination Approaches in Metastatic Hormone-sensitive Prostate Cancer: A Systematic Review and Network Meta-analysis. Eur. Urol. 2019, 77, 365–372. [Google Scholar] [CrossRef] [PubMed]
- NCT02799602. ODM-201 in Addition to Standard ADT and Docetaxel in Metastatic Castration Sensitive Prostate Cancer (ARASENS). Available online: https://clinicaltrials.gov/ct2/show/NCT02799602 (accessed on 12 March 2022).
- NCT01957436. A Phase III Study for Patients with Metastatic Hormone-Naïve Prostate Cancer (PEACE1). Available online: https://clinicaltrials.gov/ct2/show/NCT01957436 (accessed on 12 March 2022).
- NCT00268476. Systemic Therapy in Advancing or Metastatic Prostate Cancer: Evaluation of Drug Efficacy (STAMPEDE). Available online: https://clinicaltrials.gov/ct2/show/NCT00268476 (accessed on 12 March 2022).
- Robinson, D.; Van Allen, E.M.; Wu, Y.-M.; Schultz, N.; Lonigro, R.J.; Mosquera, J.-M.; Montgomery, B.; Taplin, M.-E.; Pritchard, C.C.; Attard, G.; et al. Integrative Clinical Genomics of Advanced Prostate Cancer. Cell 2015, 162, 454. [Google Scholar] [CrossRef] [Green Version]
- Pritchard, C.C.; Mateo, J.; Walsh, M.F.; De Sarkar, N.; Abida, W.; Beltran, H.; Garofalo, A.; Gulati, R.; Carreira, S.; Eeles, R.; et al. Inherited DNA-Repair Gene Mutations in Men with Metastatic Prostate Cancer. N. Engl. J. Med. 2016, 375, 443–453. [Google Scholar] [CrossRef]
- Sokolova, A.O.; Cheng, H.H. Genetic Testing in Prostate Cancer. Curr. Oncol. Rep. 2020, 22, 5. [Google Scholar] [CrossRef]
- Mateo, J.; Lord, C.J.; Serra, V.; Tutt, A.; Balmaña, J.; Castroviejo-Bermejo, M.; Cruz, C.; Oaknin, A.; Kaye, S.B.; de Bono, J.S. A decade of clinical development of PARP inhibitors in perspective. Ann. Oncol. 2019, 30, 1437–1447. [Google Scholar] [CrossRef] [Green Version]
- NCT03395197. Talazoparib + Enzalutamide vs Enzalutamide Monotherapy in Patients with Metastatic Castration-Resistant Prostate Cancer (TALAPRO-2). Available online: https://clinicaltrials.gov/ct2/show/NCT03395197 (accessed on 12 March 2022).
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [Green Version]
- Carver, B.S.; Chapinski, C.; Wongvipat, J.; Hieronymus, H.; Chen, Y.; Chandarlapaty, S.; Arora, V.K.; Le, C.; Koutcher, J.; Scher, H.; et al. Reciprocal Feedback Regulation of PI3K and Androgen Receptor Signaling in PTEN-Deficient Prostate Cancer. Cancer Cell 2011, 19, 575–586. [Google Scholar] [CrossRef] [Green Version]
- NCT04493853. Capivasertib + Abiraterone as Treatment for Patients with Hormone-Sensitive Metastatic Prostate Cancer and PTEN Deficiency (CAPItello-281). Available online: https://clinicaltrials.gov/ct2/show/NCT04493853 (accessed on 12 March 2022).
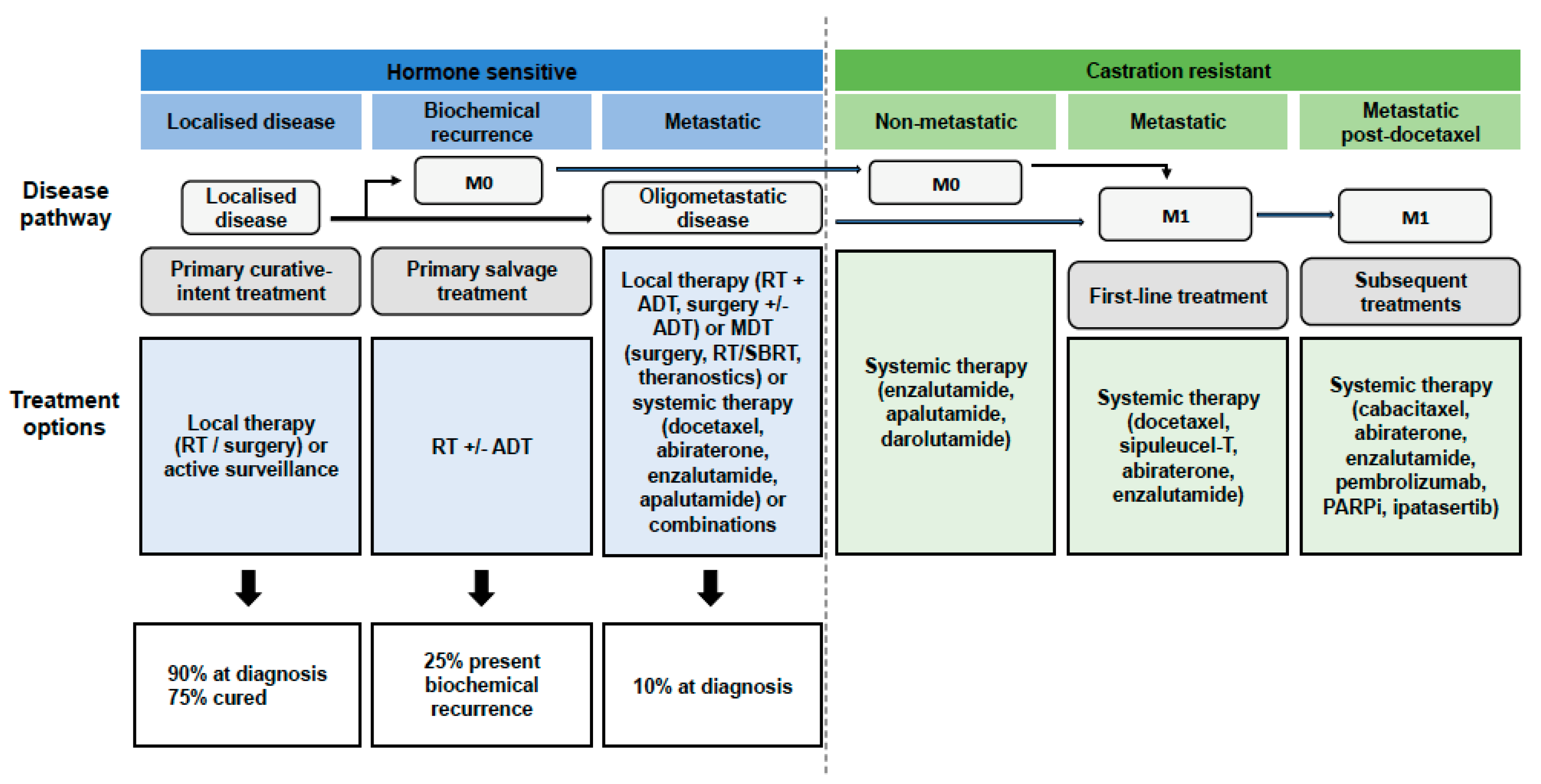
| OMPC is defined by the presence of five or fewer metastases on imaging and is a transitional state between localised and M1 disease. |
| OMPC is a clinical state with inherently more indolent tumour biology susceptible to MDT. |
| New generation imaging based on PET/CT/MRI scanning has allowed better detection of oligometastatic lesions. |
| Identifying the 4 clinical scenarios based on risk tumour volume and the diagnosis of de novo or metachronous metastases has been key to guiding treatment. |
| Local cytoreductive therapies, such as RP with or without pelvis LN dissection and RT, seem to be well tolerated. |
| MDT (RT/SBRT or surgery) has been reported as a feasible and safe treatment option. |
| Systemic therapy with chemotherapy (docetaxel) or ARTA (abiraterone, enzalutamide, apalutamide) with ADT has been demonstrated to improve outcomes. |
| A multimodal approach to patients with OMPC is needed, with evidence of surgery, RT and systemic therapy, alone or in combination, improving patient outcomes. |
| Further prospective data are needed to best select patients most likely to benefit from a given therapeutic approach. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juan, G.R.; Laura, F.H.; Javier, P.V.; Natalia, V.C.; Mᵃ Isabel, G.R.; Enrique, R.G.; José Luis, S.P.; Pablo, A.L.; Noelia, S.S.; Roser, V.D.; et al. Where Do We Stand in the Management of Oligometastatic Prostate Cancer? A Comprehensive Review. Cancers 2022, 14, 2017. https://doi.org/10.3390/cancers14082017
Juan GR, Laura FH, Javier PV, Natalia VC, Mᵃ Isabel GR, Enrique RG, José Luis SP, Pablo AL, Noelia SS, Roser VD, et al. Where Do We Stand in the Management of Oligometastatic Prostate Cancer? A Comprehensive Review. Cancers. 2022; 14(8):2017. https://doi.org/10.3390/cancers14082017
Chicago/Turabian StyleJuan, Gómez Rivas, Fernández Hernández Laura, Puente Vázquez Javier, Vidal Casinello Natalia, Galante Romo Mᵃ Isabel, Redondo González Enrique, Senovilla Pérez José Luis, Abad López Pablo, Sanmamed Salgado Noelia, Vives Dilme Roser, and et al. 2022. "Where Do We Stand in the Management of Oligometastatic Prostate Cancer? A Comprehensive Review" Cancers 14, no. 8: 2017. https://doi.org/10.3390/cancers14082017
APA StyleJuan, G. R., Laura, F. H., Javier, P. V., Natalia, V. C., Mᵃ Isabel, G. R., Enrique, R. G., José Luis, S. P., Pablo, A. L., Noelia, S. S., Roser, V. D., & Jesús, M.-S. (2022). Where Do We Stand in the Management of Oligometastatic Prostate Cancer? A Comprehensive Review. Cancers, 14(8), 2017. https://doi.org/10.3390/cancers14082017