
Feasibility of Tumor Treating Fields with Pemetrexed and Platinum-Based Chemotherapy for Unresectable Malignant Pleural Mesothelioma: Single-Center, Real-World Data

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sayan, M.; Eren, M.F.; Gupta, A.; Ohri, N.; Kotek, A.; Babalioglu, I.; Oskeroglu Kaplan, S.; Duran, O.; Derinalp Or, O.; Cukurcayir, F.; et al. Current treatment strategies in malignant pleural mesothelioma with a treatment algorithm. Adv. Respir. Med. 2019, 87, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Delgermaa, V.; Takahashi, K.; Park, E.K.; Le, G.V.; Hara, T.; Sorahan, T. Global mesothelioma deaths reported to the World Health Organization between 1994 and 2008. Bull. World Health Organ. 2011, 89, 716–724, 724A–724C. [Google Scholar] [CrossRef] [PubMed]
- Vogelzang, N.J.; Rusthoven, J.J.; Symanowski, J.; Denham, C.; Kaukel, E.; Ruffie, P.; Gatzemeier, U.; Boyer, M.; Emri, S.; Manegold, C.; et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J. Clin. Oncol. 2003, 21, 2636–2644. [Google Scholar] [CrossRef] [PubMed]
- Zalcman, G.; Mazieres, J.; Margery, J.; Greillier, L.; Audigier-Valette, C.; Moro-Sibilot, D.; Molinier, O.; Corre, R.; Monnet, I.; Gounant, V.; et al. Bevacizumab for newly diagnosed pleural mesothelioma in the Mesothelioma Avastin Cisplatin Pemetrexed Study (MAPS): A randomised, controlled, open-label, phase 3 trial. Lancet 2016, 387, 1405–1414. [Google Scholar] [CrossRef]
- Kotecha, R.; Tonse, R.; Rubens, M.; Appel, H.; Albrecht, F.; Kaywin, P.; Alley, E.W.; Tom, M.C.; Mehta, M.P. Meta-Analysis of Survival and Development of a Prognostic Nomogram for Malignant Pleural Mesothelioma Treated with Systemic Chemotherapy. Cancers 2021, 13, 2186. [Google Scholar] [CrossRef]
- Kindler, H.L.; Ismaila, N.; Armato, S.G., 3rd; Bueno, R.; Hesdorffer, M.; Jahan, T.; Jones, C.M.; Miettinen, M.; Pass, H.; Rimner, A.; et al. Treatment of Malignant Pleural Mesothelioma: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1343–1373. [Google Scholar] [CrossRef]
- Parikh, K.; Hendriks, L.E.L.; Bironzo, P.; Remon, J. Immune checkpoint inhibitors a new player in the therapeutic game of mesothelioma: New reality with new challenges. Cancer Treat. Rev. 2021, 99, 102250. [Google Scholar] [CrossRef]
- Kirson, E.D.; Gurvich, Z.; Schneiderman, R.; Dekel, E.; Itzhaki, A.; Wasserman, Y.; Schatzberger, R.; Palti, Y. Disruption of cancer cell replication by alternating electric fields. Cancer Res. 2004, 64, 3288–3295. [Google Scholar] [CrossRef] [Green Version]
- Mumblat, H.; Martinez-Conde, A.; Braten, O.; Munster, M.; Dor-On, E.; Schneiderman, R.S.; Porat, Y.; Voloshin, T.; Davidi, S.; Blatt, R.; et al. Tumor Treating Fields (TTFields) downregulate the Fanconi Anemia-BRCA pathway and increase the efficacy of chemotherapy in malignant pleural mesothelioma preclinical models. Lung Cancer 2021, 160, 99–110. [Google Scholar] [CrossRef]
- Giladi, M.; Weinberg, U.; Schneiderman, R.S.; Porat, Y.; Munster, M.; Voloshin, T.; Blatt, R.; Cahal, S.; Itzhaki, A.; Onn, A.; et al. Alternating electric fields (tumor-treating fields therapy) can improve chemotherapy treatment efficacy in non-small cell lung cancer both in vitro and in vivo. Semin. Oncol. 2014, 41 (Suppl. S6), S35–S41. [Google Scholar] [CrossRef] [Green Version]
- Ceresoli, G.L.; Aerts, J.G.; Dziadziuszko, R.; Ramlau, R.; Cedres, S.; van Meerbeeck, J.P.; Mencoboni, M.; Planchard, D.; Chella, A.; Crino, L.; et al. Tumour Treating Fields in combination with pemetrexed and cisplatin or carboplatin as first-line treatment for unresectable malignant pleural mesothelioma (STELLAR): A multicentre, single-arm phase 2 trial. Lancet Oncol. 2019, 20, 1702–1709. [Google Scholar] [CrossRef]
- Byrne, M.J.; Nowak, A.K. Modified RECIST criteria for assessment of response in malignant pleural mesothelioma. Ann. Oncol. 2004, 15, 257–260. [Google Scholar] [CrossRef] [PubMed]
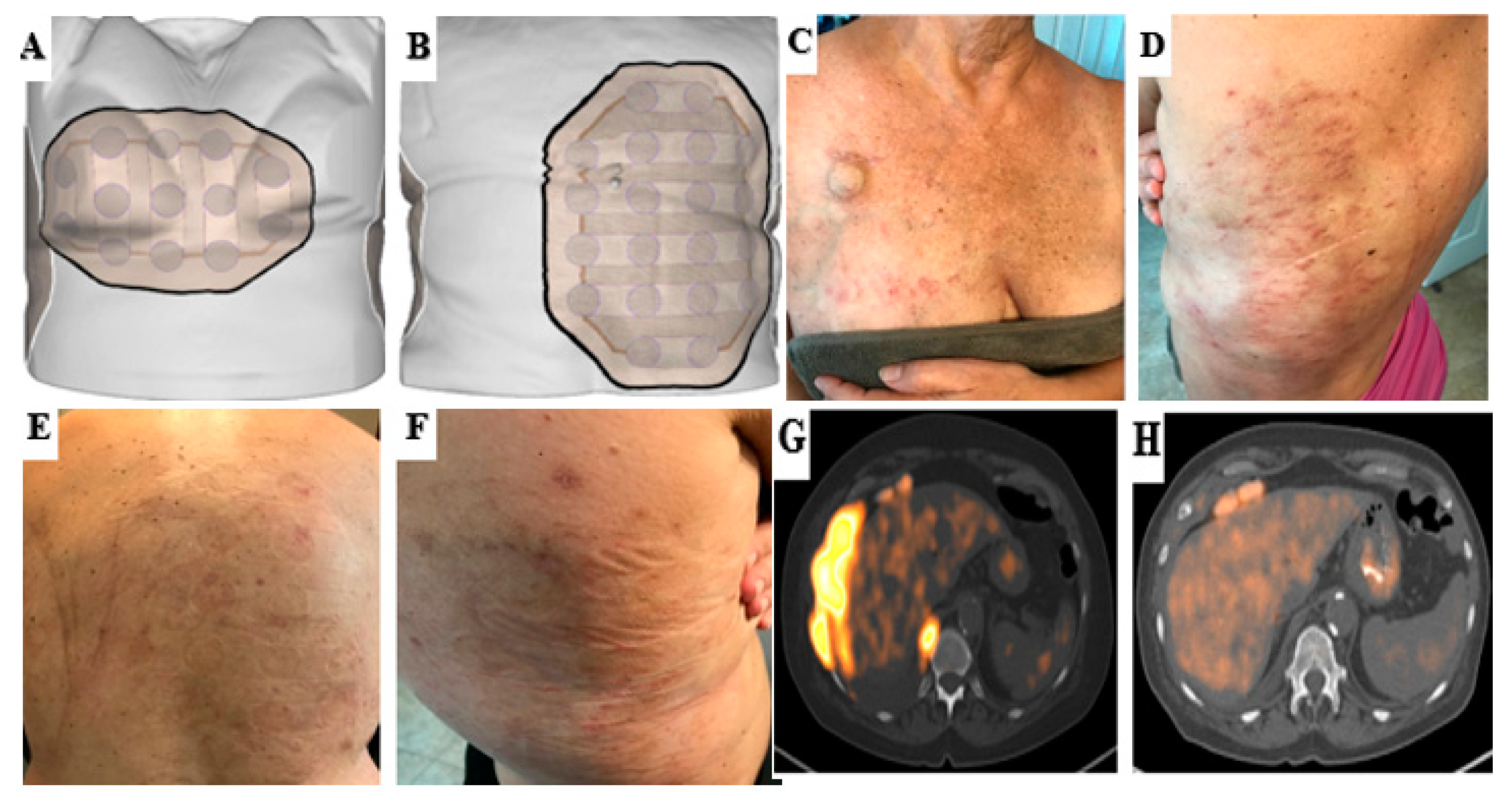
- Lacouture, M.E.; Anadkat, M.J.; Ballo, M.T.; Iwamoto, F.; Jeyapalan, S.A.; La Rocca, R.V.; Schwartz, M.; Serventi, J.N.; Glas, M. Prevention and Management of Dermatologic Adverse Events Associated with Tumor Treating Fields in Patients with Glioblastoma. Front. Oncol. 2020, 10, 1045. [Google Scholar] [CrossRef]
- Rice, D.C.; Smythe, W.R.; Liao, Z.; Guerrero, T.; Chang, J.Y.; McAleer, M.F.; Jeter, M.D.; Correa, A.; Vaporciyan, A.A.; Liu, H.H.; et al. Dose-dependent pulmonary toxicity after postoperative intensity-modulated radiotherapy for malignant pleural mesothelioma. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Carrieri, F.A.; Smack, C.; Siddiqui, I.; Kleinberg, L.R.; Tran, P.T. Tumor Treating Fields: At the Crossroads between Physics and Biology for Cancer Treatment. Front. Oncol. 2020, 10, 575992. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, D.S.; Wood, D.E.; Akerley, W.; Bazhenova, L.A.; Borghaei, H.; Camidge, D.R.; Cheney, R.T.; Chirieac, L.R.; D’Amico, T.A.; Dilling, T.; et al. NCCN Guidelines Insights: Malignant Pleural Mesothelioma, Version 3.2016. J. Natl. Compr. Cancer Netw. 2016, 14, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Baas, P.; Scherpereel, A.; Nowak, A.K.; Fujimoto, N.; Peters, S.; Tsao, A.S.; Mansfield, A.S.; Popat, S.; Jahan, T.; Antonia, S.; et al. First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743): A multicentre, randomised, open-label, phase 3 trial. Lancet 2021, 397, 375–386. [Google Scholar] [CrossRef]
- Voloshin, T.; Kaynan, N.; Davidi, S.; Porat, Y.; Shteingauz, A.; Schneiderman, R.S.; Zeevi, E.; Munster, M.; Blat, R.; Tempel Brami, C.; et al. Tumor-treating fields (TTFields) induce immunogenic cell death resulting in enhanced antitumor efficacy when combined with anti-PD-1 therapy. Cancer Immunol. Immunother. 2020, 69, 1191–1204. [Google Scholar] [CrossRef] [Green Version]
- Mrugala, M.M.; Engelhard, H.H.; Dinh Tran, D.; Kew, Y.; Cavaliere, R.; Villano, J.L.; Annenelie Bota, D.; Rudnick, J.; Love Sumrall, A.; Zhu, J.J.; et al. Clinical practice experience with NovoTTF-100A system for glioblastoma: The Patient Registry Dataset (PRiDe). Semin. Oncol. 2014, 41 (Suppl. S6), S4–S13. [Google Scholar] [CrossRef] [Green Version]
- Kanner, A.A.; Wong, E.T.; Villano, J.L.; Ram, Z.; Investigators, E.F. Post Hoc analyses of intention-to-treat population in phase III comparison of NovoTTF-100A system versus best physician’s choice chemotherapy. Semin. Oncol. 2014, 41 (Suppl. S6), S25–S34. [Google Scholar] [CrossRef] [Green Version]
- Toms, S.A.; Kim, C.Y.; Nicholas, G.; Ram, Z. Increased compliance with tumor treating fields therapy is prognostic for improved survival in the treatment of glioblastoma: A subgroup analysis of the EF-14 phase III trial. J. Neurooncol. 2019, 141, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivera, F.; Benavides, M.; Gallego, J.; Guillen-Ponce, C.; Lopez-Martin, J.; Kung, M. Tumor treating fields in combination with gemcitabine or gemcitabine plus nab-paclitaxel in pancreatic cancer: Results of the PANOVA phase 2 study. Pancreatology 2019, 19, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Vergote, I.; von Moos, R.; Manso, L.; Van Nieuwenhuysen, E.; Concin, N.; Sessa, C. Tumor Treating Fields in combination with paclitaxel in recurrent ovarian carcinoma: Results of the INNOVATE pilot study. Gynecol. Oncol. 2018, 150, 471–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stupp, R.; Wong, E.T.; Kanner, A.A.; Steinberg, D.; Engelhard, H.; Heidecke, V.; Kirson, E.D.; Taillibert, S.; Liebermann, F.; Dbaly, V.; et al. NovoTTF-100A versus physician’s choice chemotherapy in recurrent glioblastoma: A randomised phase III trial of a novel treatment modality. Eur. J. Cancer 2012, 48, 2192–2202. [Google Scholar] [CrossRef] [Green Version]
- Stupp, R.; Taillibert, S.; Kanner, A.; Read, W.; Steinberg, D.; Lhermitte, B.; Toms, S.; Idbaih, A.; Ahluwalia, M.S.; Fink, K.; et al. Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs Maintenance Temozolomide Alone on Survival in Patients with Glioblastoma: A Randomized Clinical Trial. JAMA 2017, 318, 2306–2316. [Google Scholar] [CrossRef] [Green Version]
- Pless, M.; Droege, C.; von Moos, R.; Salzberg, M.; Betticher, D. A phase I/II trial of Tumor Treating Fields (TTFields) therapy in combination with pemetrexed for advanced non-small cell lung cancer. Lung Cancer 2013, 81, 445–450. [Google Scholar] [CrossRef]
- Lacouture, M.E.; Davis, M.E.; Elzinga, G.; Butowski, N.; Tran, D.; Villano, J.L.; DiMeglio, L.; Davies, A.M.; Wong, E.T. Characterization and management of dermatologic adverse events with the NovoTTF-100A System, a novel anti-mitotic electric field device for the treatment of recurrent glioblastoma. Semin. Oncol. 2014, 41 (Suppl. S4), S1–S14. [Google Scholar] [CrossRef] [Green Version]
- Di Maio, M.; Perrone, F.; Conte, P. Real-World Evidence in Oncology: Opportunities and Limitations. Oncologist 2020, 25, e746–e752. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | Gender | Race | Primary Histology | ECOG Status | Smoking Status | AJCC 8th Edition Stage | Disease Status at the Time of TTFields Treatment | |
|---|---|---|---|---|---|---|---|---|
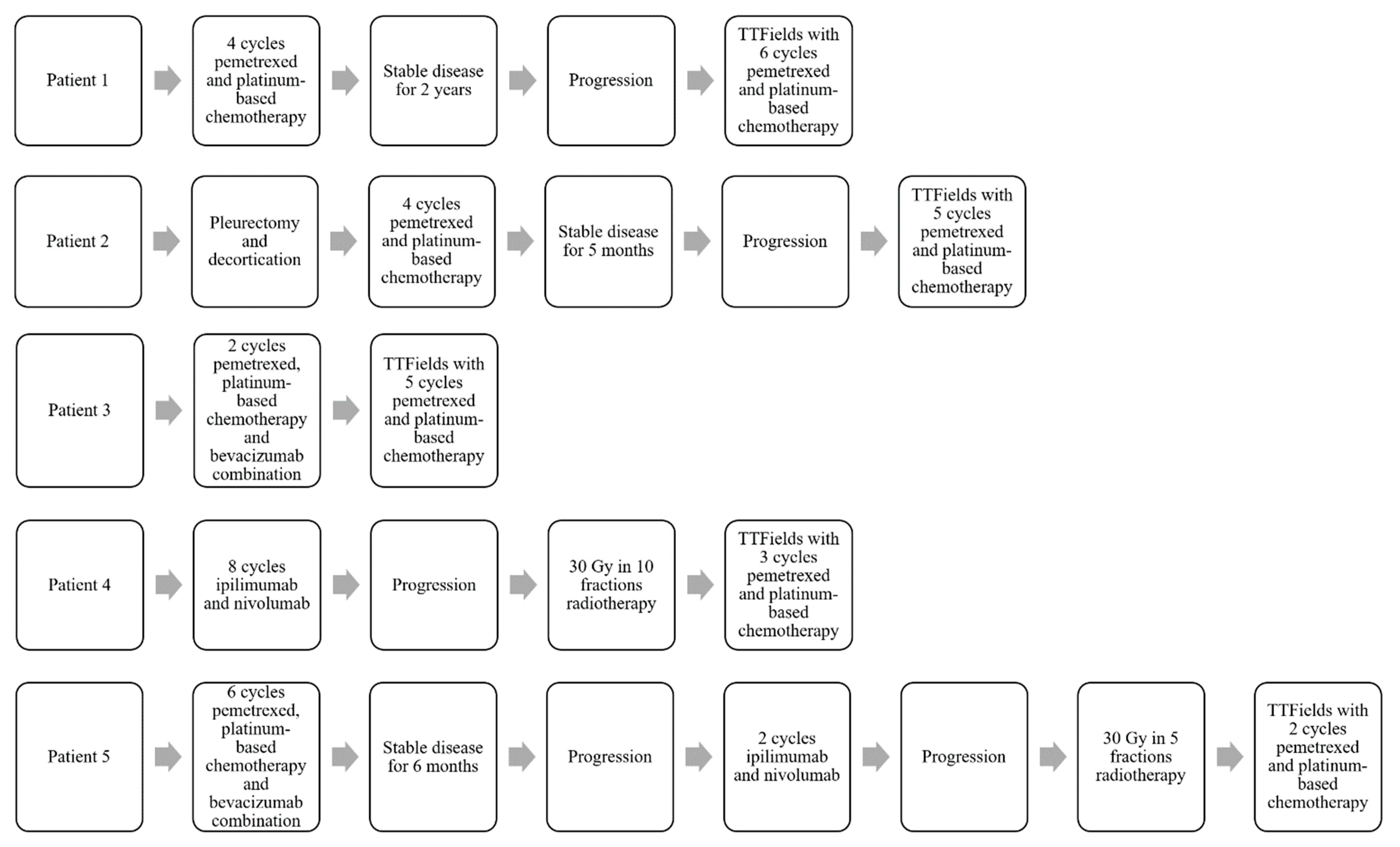
| Patient 1 | 84 | Male | White Hispanic | Epithelioid | 1 | Non-smoker | T2N0M0 (Stage IB) | Recurrent disease |
| Patient 2 | 69 | Male | White Caucasian | Epithelioid | 0 | Non-smoker | T4N2M0 (Stage IIIB) | Recurrent disease |
| Patient 3 | 67 | Female | White Caucasian | Epithelioid | 1 | Former smoker (20 pack/year) | T3N1M0 (Stage IIIA) | Newly diagnosed |
| Patient 4 | 75 | Male | White Hispanic | Sarcomatoid | 1 | Non-smoker | T2N0M0 (Stage IB) | Recurrent disease |
| Patient 5 | 64 | Female | White Hispanic | Epithelioid | 1 | Former smoker (10 pack/year) | T2N1M0 (Stage II) | Recurrent disease |
| Grade 1 | Grade 2 | Grade 3 | Grade 4–5 | |
|---|---|---|---|---|
| Dermatitis | 2 (40%) | 3 (60%) | 0 | 0 |
| Neutropenia | 0 | 1 (20%) | 1 (20%) | 0 |
| Anemia | 3 (60%) | 2 (40%) | 0 | 0 |
| Fatigue | 3 (60%) | 2 (40%) | 0 | 0 |
| Oliguria | 0 | 1 (20%) | 0 | 0 |
| Pain | 0 | 1 (20%) | 0 | 0 |
| Renal toxicity | 0 | 1 (20%) | 0 | 0 |
| Pneumonitis | 0 | 1 (20%) | 0 | 0 |
| Diagnosis | N | Patients with Skin Side Effect (N, %) | Patients with Grade 3 Skin Side Effects (N, %) | TTFields Device Usage Rate | |
|---|---|---|---|---|---|
| Stupp et al. (EF-11) [24] | Recurrent GBM | 116 | 19 (16%) | 0 | 86% |
| Stupp et al. (EF-14) [25] | Newly diagnosed GBM | 456 | 237 (52%) | 9 (2%) | 75% of patients used ≥18 h/d (first 3 months of treatment) |
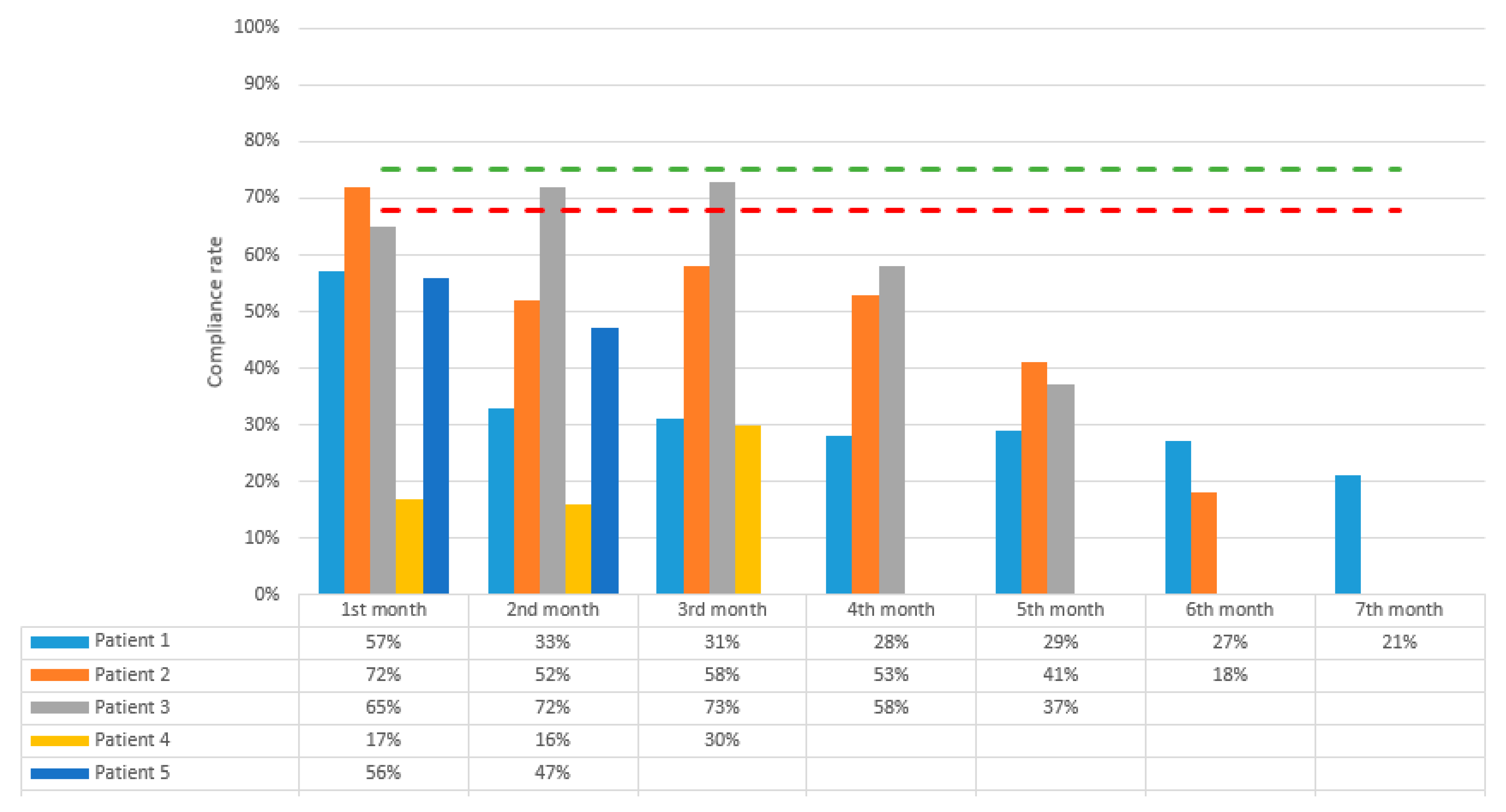
| Ceresoli et al. (STELLAR) [11] | Unresectable MPM | 80 | 57 (71%) | 4 (5%) | 68% (first 3 months) |
| Rivera et al. (PANOVA) [22] | Locally advanced or metastatic pancreas adenocarcinoma | 40 | 21 (53%) | 7 (18%) | 58% (TTFields with gemcitabine alone) 51% (TTFields plus gemcitabine and nab-paclitaxel) |
| Vergote et al. (INNOVATE) [23] | Recurrent ovarian carcinoma | 31 | 28 (90%) | 2 (6%) | 58% |
| Pless et al. [26] | Inoperable stage III and stage IV NSCLC | 42 | 18 (43%) | 1 (2%) | 47% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kutuk, T.; Appel, H.; Avendano, M.C.; Albrecht, F.; Kaywin, P.; Ramos, S.; Suarez-Murias, M.E.; Mehta, M.P.; Kotecha, R. Feasibility of Tumor Treating Fields with Pemetrexed and Platinum-Based Chemotherapy for Unresectable Malignant Pleural Mesothelioma: Single-Center, Real-World Data. Cancers 2022, 14, 2020. https://doi.org/10.3390/cancers14082020
Kutuk T, Appel H, Avendano MC, Albrecht F, Kaywin P, Ramos S, Suarez-Murias ME, Mehta MP, Kotecha R. Feasibility of Tumor Treating Fields with Pemetrexed and Platinum-Based Chemotherapy for Unresectable Malignant Pleural Mesothelioma: Single-Center, Real-World Data. Cancers. 2022; 14(8):2020. https://doi.org/10.3390/cancers14082020
Chicago/Turabian StyleKutuk, Tugce, Haley Appel, Maria Carolina Avendano, Federico Albrecht, Paul Kaywin, Suyen Ramos, Melanie E. Suarez-Murias, Minesh P. Mehta, and Rupesh Kotecha. 2022. "Feasibility of Tumor Treating Fields with Pemetrexed and Platinum-Based Chemotherapy for Unresectable Malignant Pleural Mesothelioma: Single-Center, Real-World Data" Cancers 14, no. 8: 2020. https://doi.org/10.3390/cancers14082020
APA StyleKutuk, T., Appel, H., Avendano, M. C., Albrecht, F., Kaywin, P., Ramos, S., Suarez-Murias, M. E., Mehta, M. P., & Kotecha, R. (2022). Feasibility of Tumor Treating Fields with Pemetrexed and Platinum-Based Chemotherapy for Unresectable Malignant Pleural Mesothelioma: Single-Center, Real-World Data. Cancers, 14(8), 2020. https://doi.org/10.3390/cancers14082020