
Current Knowledge on Spinal Meningiomas—Surgical Treatment, Complications, and Outcomes: A Systematic Review and Meta-Analysis (Part 2)

 , and
, and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Databases, Search Strategy, and Study Selection
2.3. Data Extraction
2.4. Individual Evidence Level and Risk of Bias Assessment
2.5. Data Synthesis, Analysis, and Statistics
2.6. Quality of the Pooled Body of Evidence
3. Results and Discussion
3.1. Spinal Meningioma Surgery
3.2. Intraoperative Neurophysiological Monitoring (IONM)
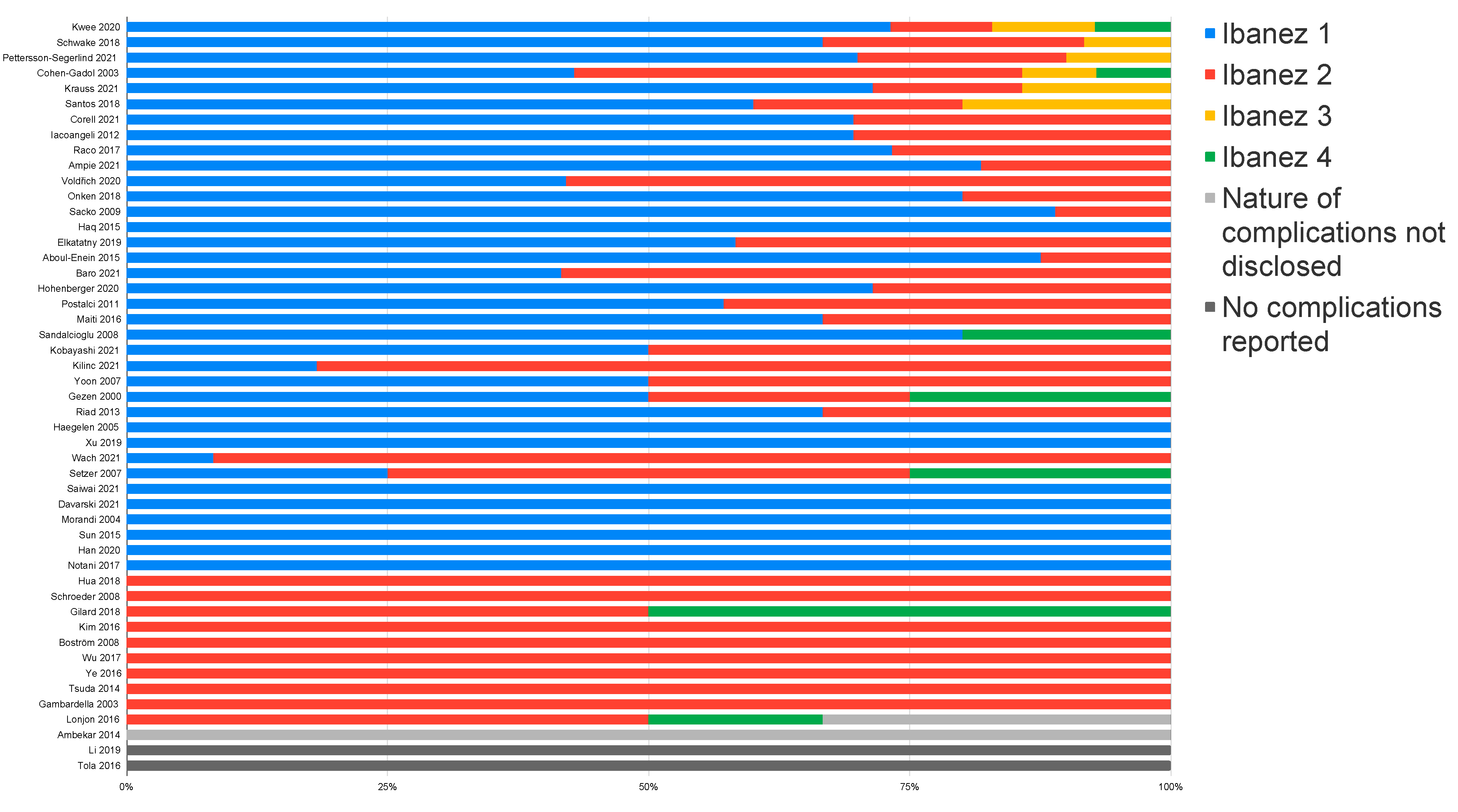
3.3. Operative Complications
3.3.1. Section on the Risk and Severity of Postoperative Complications
3.3.2. Factors Influencing the Complication Rate
3.4. Neurological Outcomes
3.4.1. Neurologic Impairment Scales Used
3.4.2. Postoperative Neurological Outcome
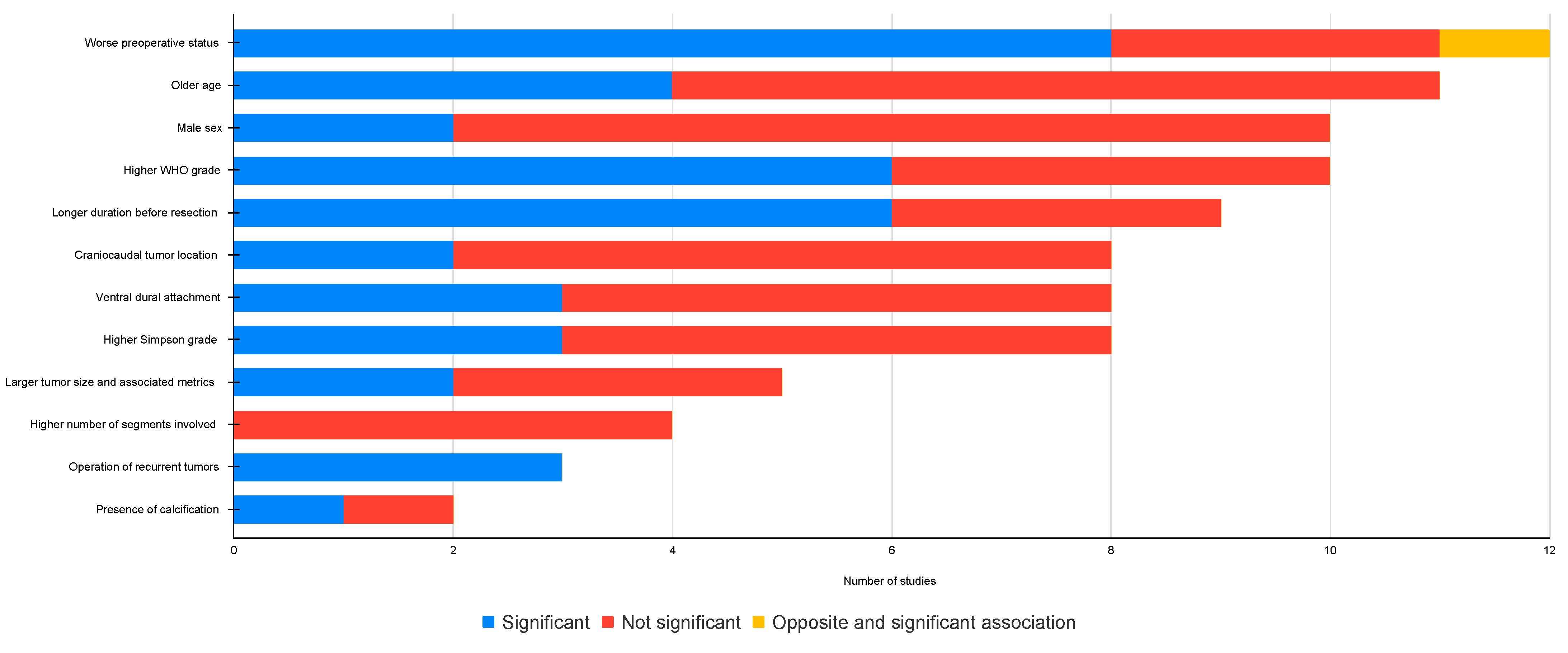
3.4.3. Outcome Predictors
3.5. Tumor Recurrence
3.5.1. Overall Recurrence Rate
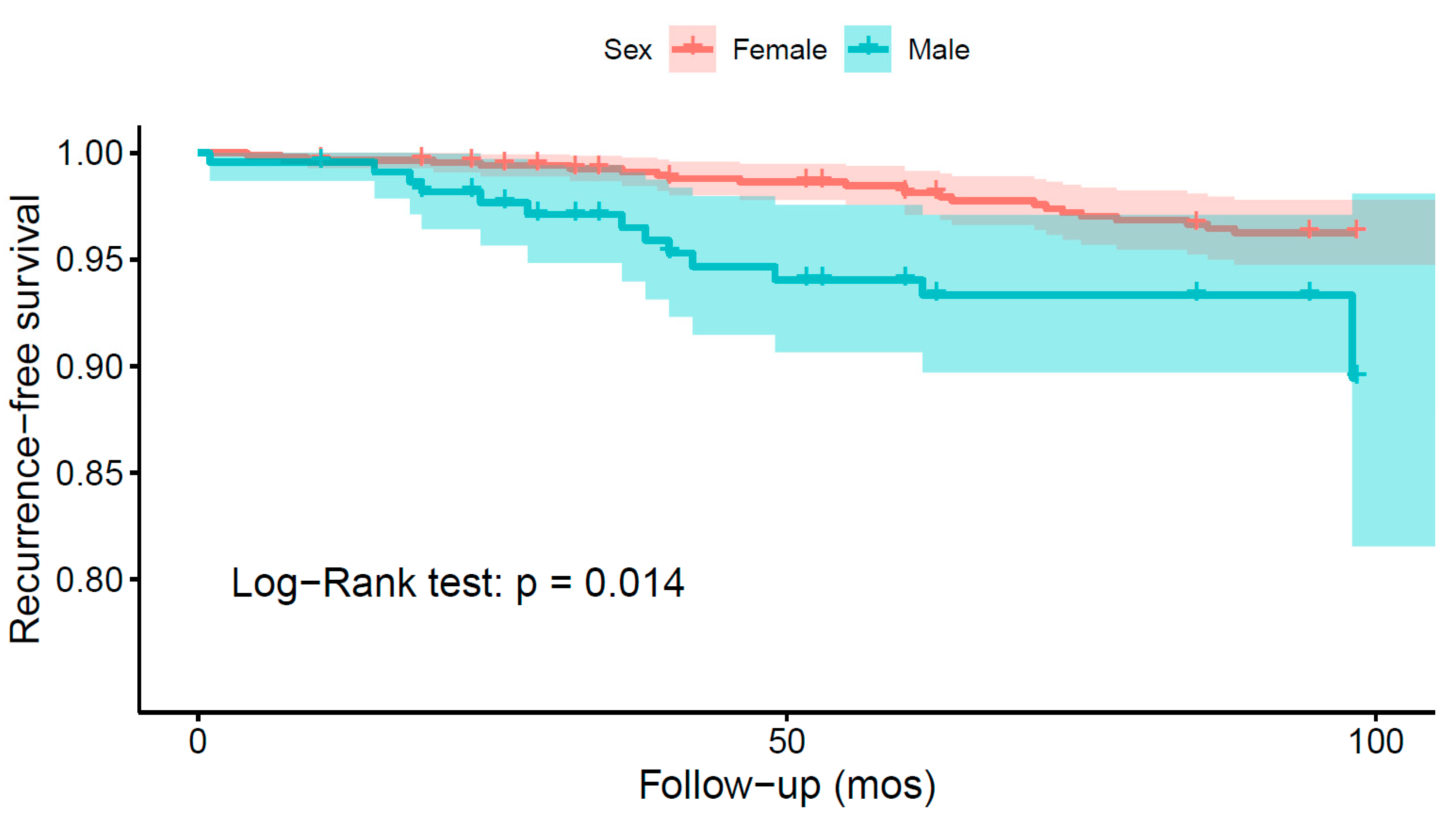
3.5.2. Recurrence and Patient Characteristics
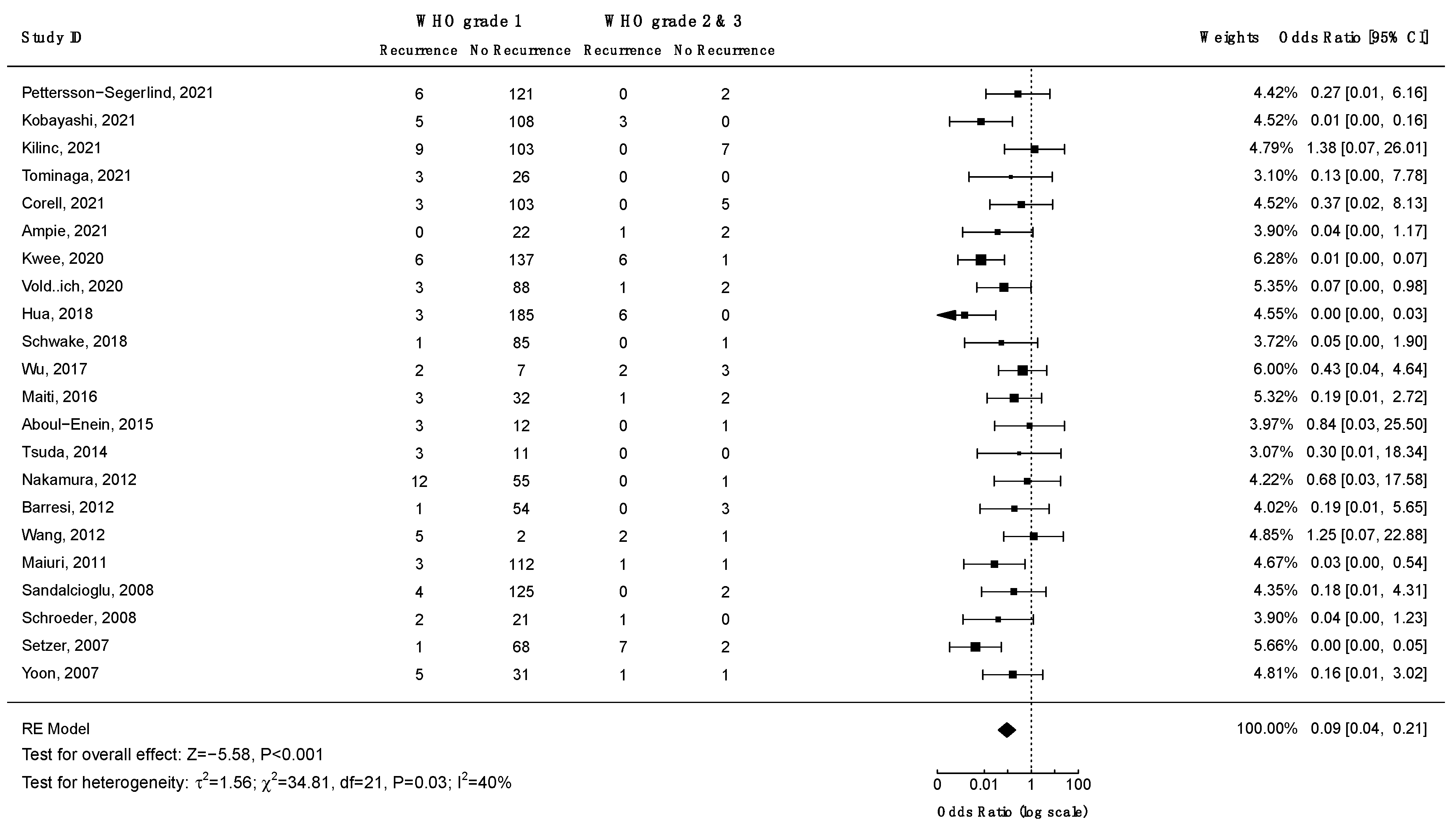
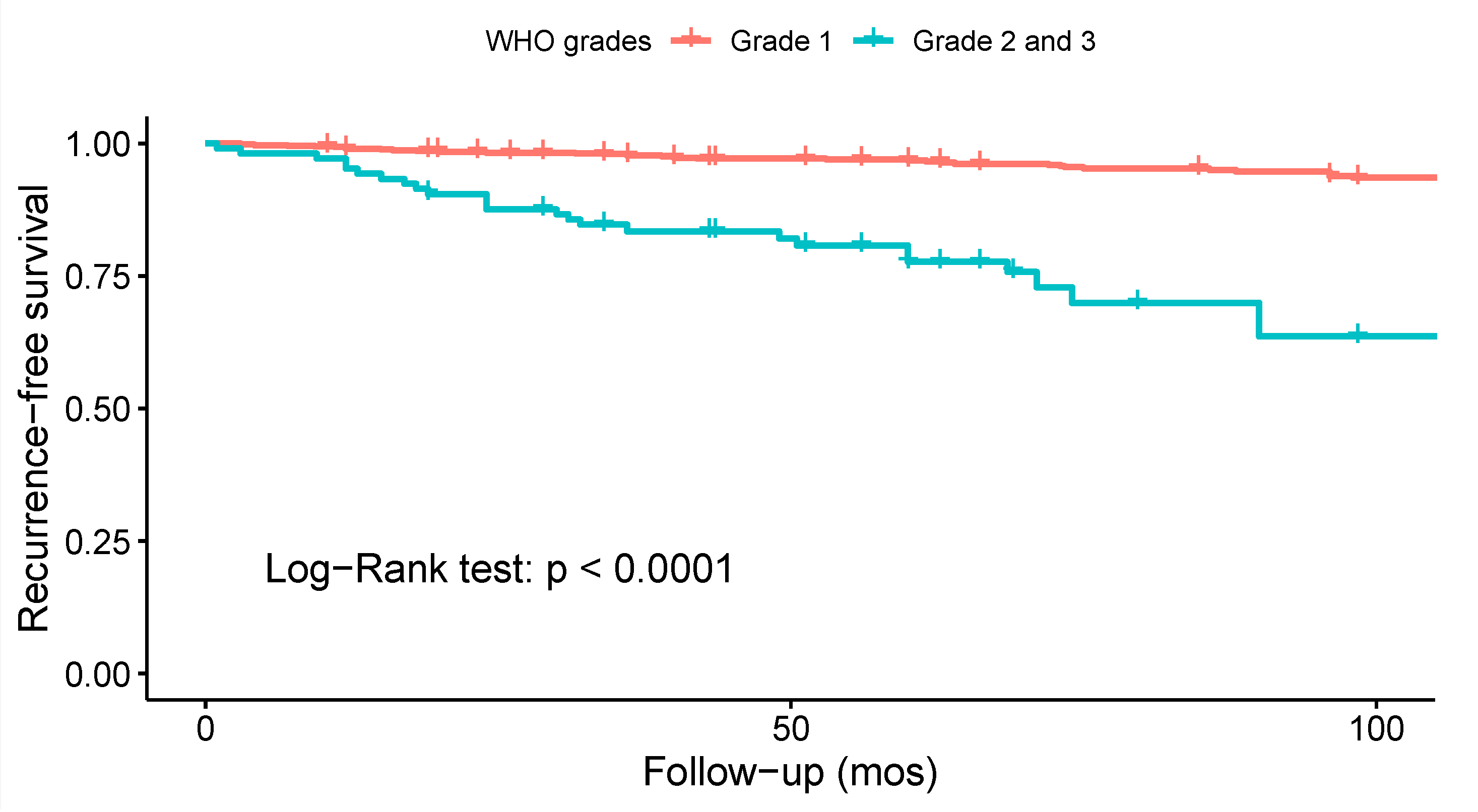
3.5.3. Recurrence and WHO Grade
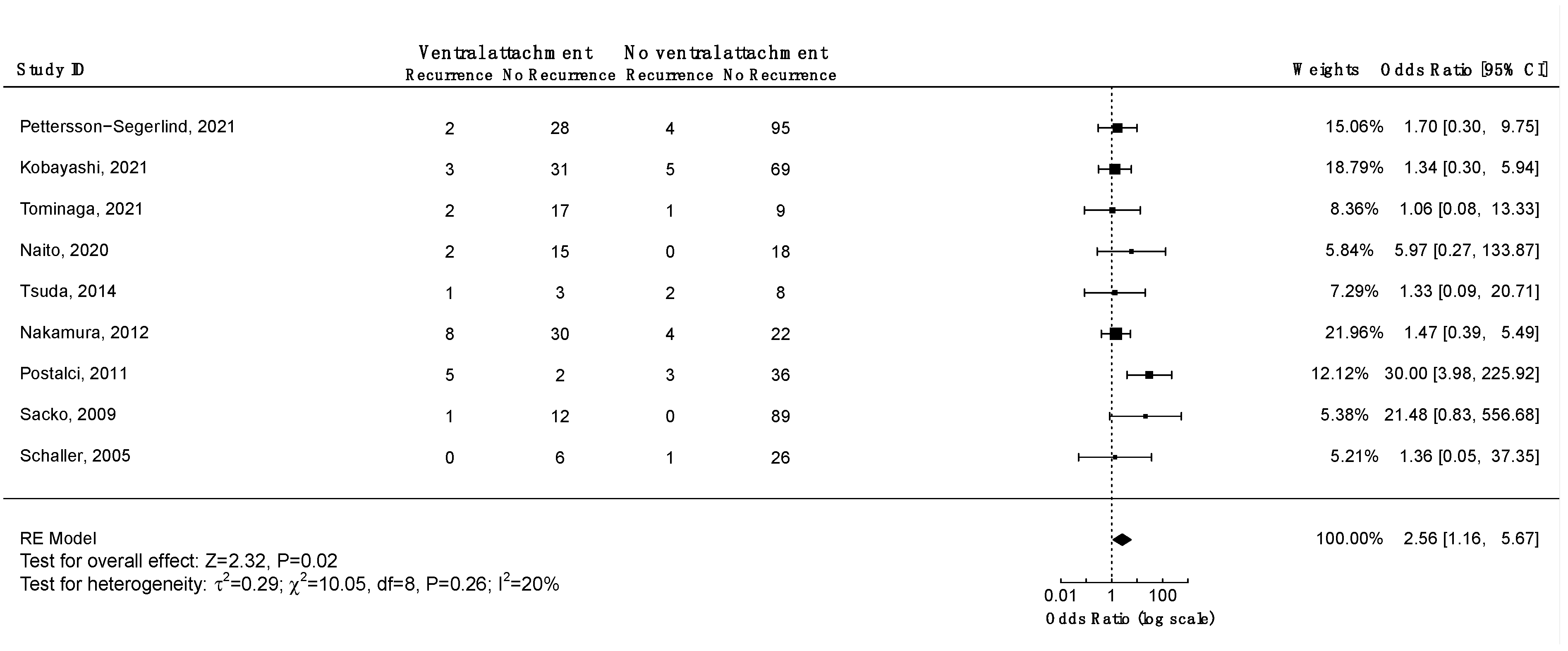
3.5.4. Recurrence and Axial Tumor Location
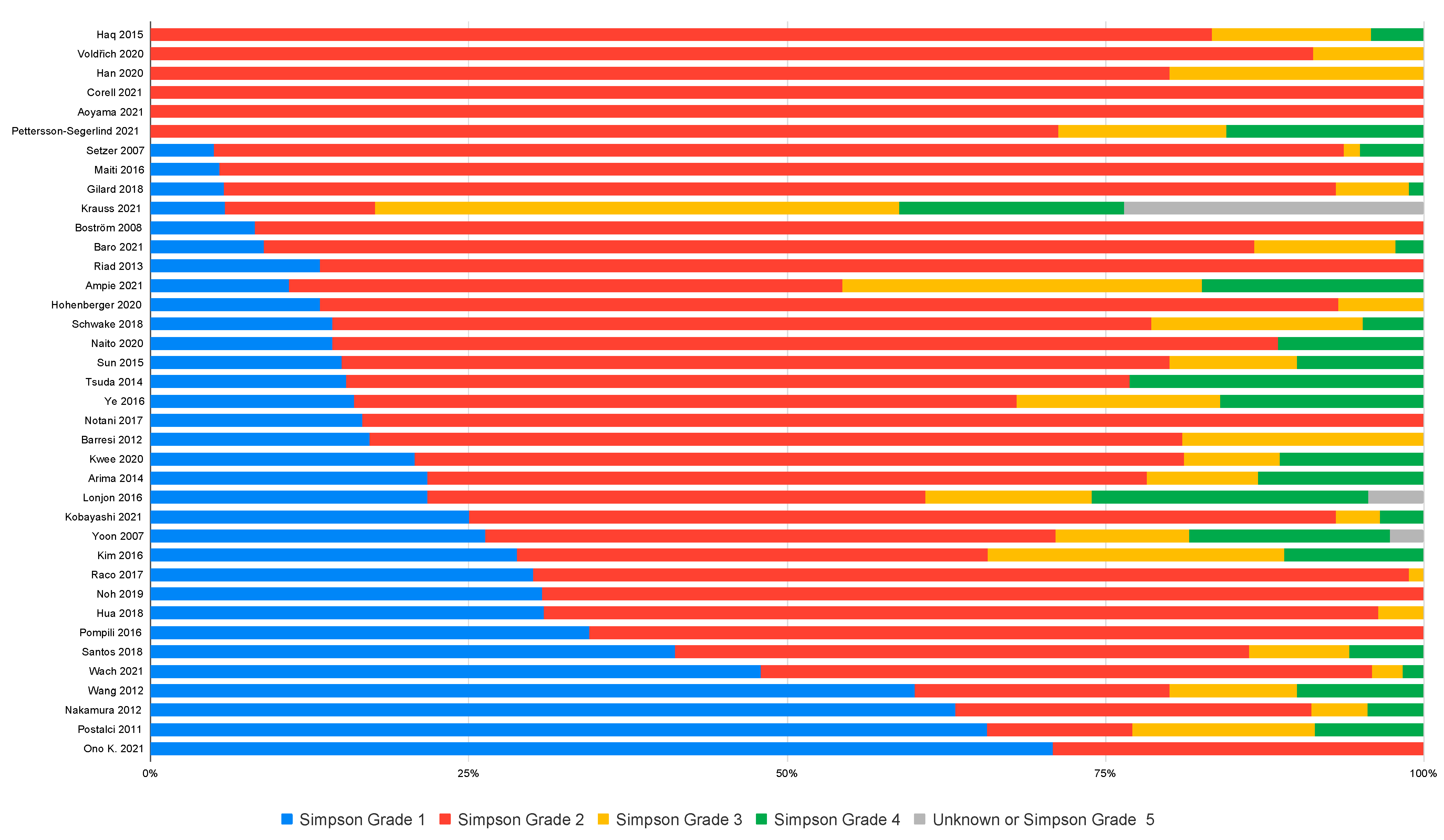
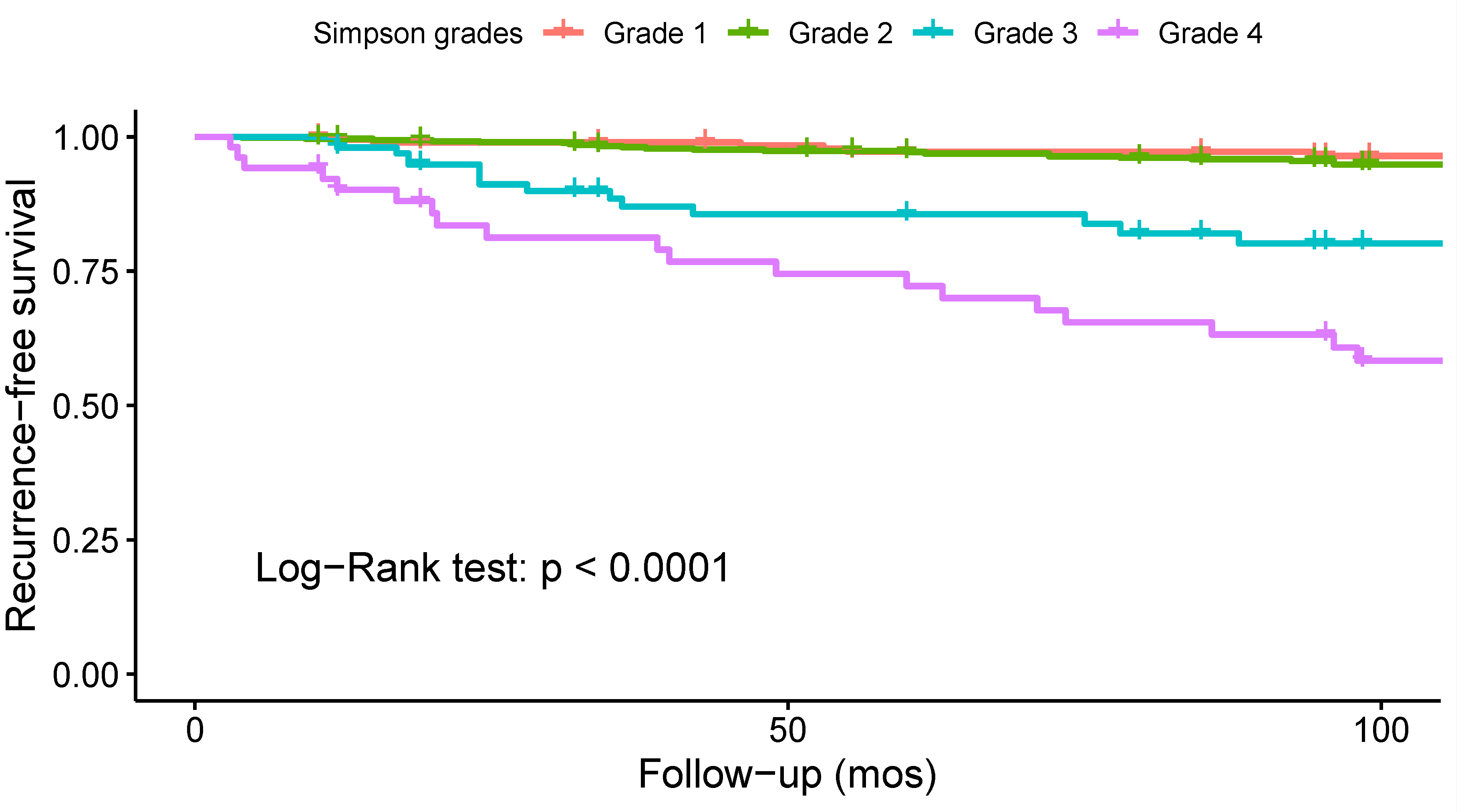
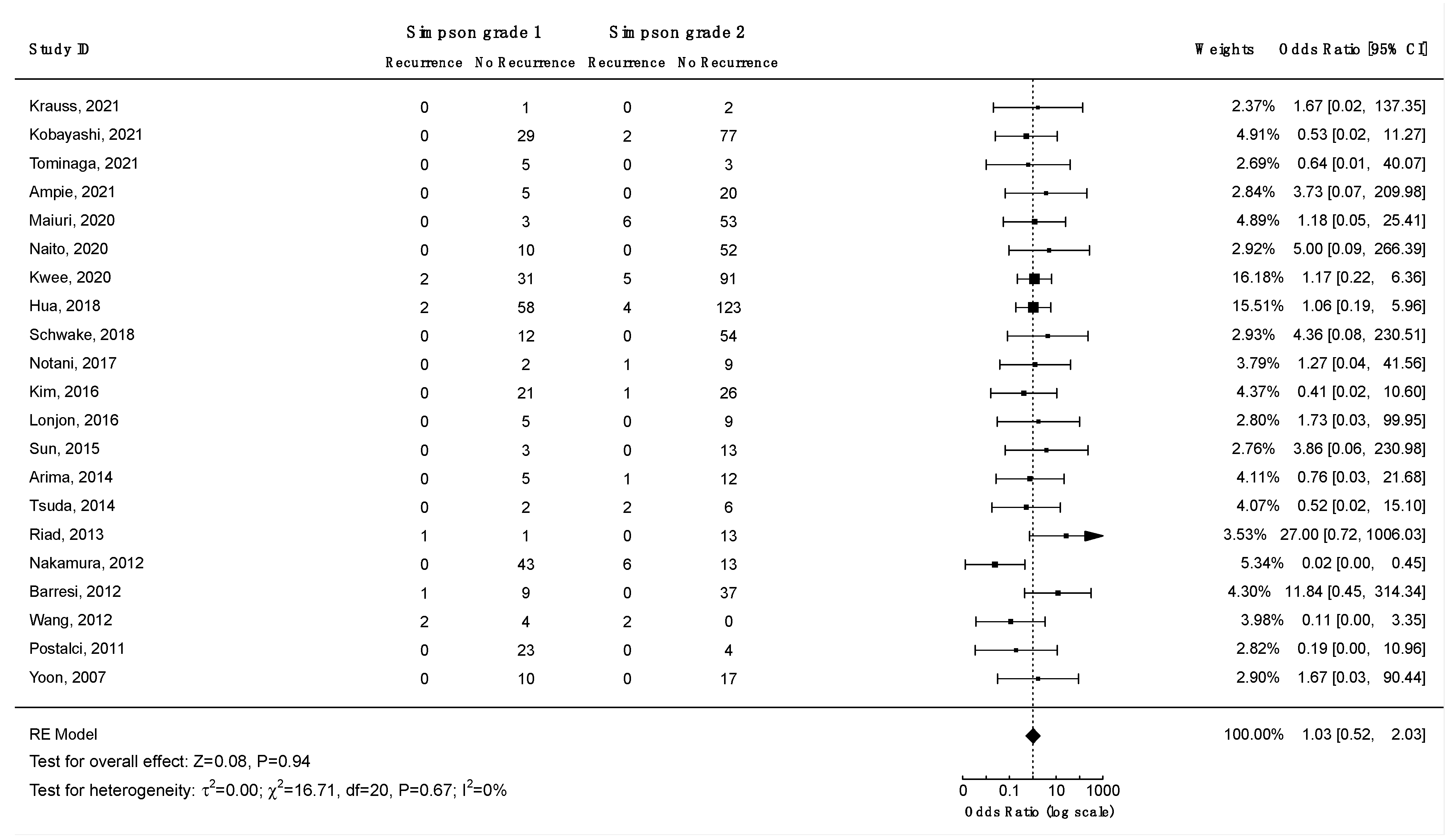
3.5.5. Recurrence and Extent of Resection
3.5.6. Other Risk Factors for Recurrence
3.6. Quality-of-Life after Spinal Meningioma Surgery
3.7. Limitations
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- El-Hajj, V.G.; Fletcher-Sandersjöö, A.; Pettersson-Segerlind, J.; Edström, E.; Elmi-Terander, A. Unsuccessful External Validation of the MAC-Score for Predicting Increased MIB-1 Index in Patients with Spinal Meningiomas. Front. Oncol. 2022, 12, 6749. [Google Scholar] [CrossRef] [PubMed]
- Pettersson-Segerlind, J.; Fletcher-Sandersjoo, A.; Tatter, C.; Burstrom, G.; Persson, O.; Forander, P.; Mathiesen, T.; Bartek, J., Jr.; Edstrom, E.; Elmi-Terander, A. Long-Term Follow-Up and Predictors of Functional Outcome after Surgery for Spinal Meningiomas: A Population-Based Cohort Study. Cancers 2021, 13, 3244. [Google Scholar] [CrossRef] [PubMed]
- Kwee, L.E.; Harhangi, B.S.; Ponne, G.A.; Kros, J.M.; Dirven, C.M.F.; Dammers, R. Spinal Meningiomas: Treatment Outcome and Long-Term Follow-Up. Clin. Neurol. Neurosurg. 2020, 198, 106238. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.H.; Chung, C.K.; Jahng, T.A. Surgical Outcome of Spinal Canal Meningiomas. J. Korean Neurosurg. Soc. 2007, 42, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Tominaga, H.; Kawamura, I.; Ijiri, K.; Yone, K.; Taniguchi, N. Surgical Results of the Resection of Spinal Meningioma with the Inner Layer of Dura More than 10 Years after Surgery. Sci. Rep. 2021, 11, 4050. [Google Scholar] [CrossRef]
- Saito, T.; Arizono, T.; Maeda, T.; Terada, K.; Iwamoto, Y. A Novel Technique for Surgical Resection of Spinal Meningioma. Spine 2001, 26, 1805–1808. [Google Scholar] [CrossRef]
- Tatter, C.; Fletcher-Sandersjöö, A.; Persson, O.; Burström, G.; Grane, P.; Edström, E.; Elmi-Terander, A. Incidence and Predictors of Kyphotic Deformity Following Resection of Cervical Intradural Tumors in Adults: A Population-Based Cohort Study. Acta Neurochir. 2020, 162, 2905–2913. [Google Scholar] [CrossRef]
- Tsuda, K.; Akutsu, H.; Yamamoto, T.; Nakai, K.; Ishikawa, E.; Matsumura, A. Is Simpson Grade I Removal Necessary in All Cases of Spinal Meningioma? Assessment of Postoperative Recurrence during Long-Term Follow-Up. Neurol. Med. Chir. 2014, 54, 907–913. [Google Scholar] [CrossRef]
- Kim, C.H.; Chung, C.K.; Lee, S.H.; Jahng, T.A.; Hyun, S.J.; Kim, K.J.; Yoon, S.H.; Kim, E.S.; Eoh, W.; Kim, H.J.; et al. Long-Term Recurrence Rates after the Removal of Spinal Meningiomas in Relation to Simpson Grades. Eur. Spine J. 2016, 25, 4025–4032. [Google Scholar] [CrossRef]
- Voldřich, R.; Netuka, D.; Beneš, V. Spinal Meningiomas: Is Simpson Grade II Resection Radical Enough? Acta Neurochir. 2020, 162, 1401–1408. [Google Scholar] [CrossRef]
- Nakamura, M.; Tsuji, O.; Fujiyoshi, K.; Hosogane, N.; Watanabe, K.; Tsuji, T.; Ishii, K.; Toyama, Y.; Chiba, K.; Matsumoto, M. Long-Term Surgical Outcomes of Spinal Meningiomas. Spine 2012, 37, E617–E623. [Google Scholar] [CrossRef] [PubMed]
- Viereck, M.J.; Ghobrial, G.M.; Beygi, S.; Harrop, J.S. Improved Patient Quality of Life Following Intradural Extramedullary Spinal Tumor Resection. J. Neurosurg. Spine 2016, 25, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Pettersson-Segerlind, J.; von Vogelsang, A.-C.; Fletcher-Sandersjöö, A.; Tatter, C.; Mathiesen, T.; Edström, E.; Elmi-Terander, A. Health-Related Quality of Life and Return to Work after Surgery for Spinal Meningioma: A Population-Based Cohort Study. Cancers 2021, 13, 6371. [Google Scholar] [CrossRef]
- Zuurveld, M.A.; Peerdeman, S.M.; Bouma, G.J.; Feller, R.E.; Klein, M. Postsurgical Health-Related Quality of Life and Mood in Patients with Spinal Meningioma. Neuro Oncol. 2011, 13, iii122. [Google Scholar] [CrossRef]
- El-Hajj, V.G.; Pettersson Segerlind, J.; Burström, G.; Edström, E.; Elmi-Terander, A. Current Knowledge on Spinal Meningiomas: A Systematic Review Protocol. BMJ Open 2022, 12, e061614. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.G.; Swiontkowski, M.F.; Heckman, J.D. Introducing Levels of Evidence to the Journal. J. Bone Jt. Surg. Am. 2003, 85, 1–3. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 24 July 2022).
- Lasserson, T.J.; Thomas, J.; Higgins, J.P.T. Chapter 1: Starting a Review. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: Alberta, Canada, 2021; Available online: www.training.cochrane.org/handbook (accessed on 10 June 2022).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.r-project.org/ (accessed on 10 June 2022).
- Schünemann, H.; Brożek, J.; Guyatt, G.; Oxman, A. (Eds.) GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations; Updated October 2013; The GRADE Working Group, 2013; Available online: www.guidelinedevelopment.org/handbook (accessed on 2 May 2022).
- GRADEpro GDT: GRADEpro Guideline Development Tool [Software]. McMaster University, 2020. (Developed by Evidence Prime, Inc.). Available online: www.gradepro.org (accessed on 2 May 2022).
- Tola, S.; De Angelis, M.; Bistazzoni, S.; Chiaramonte, C.; Esposito, V.; Paolini, S. Hemilaminectomy for Spinal Meningioma: A Case Series of 20 Patients with a Focus on Ventral- and Ventrolateral Lesions. Clin. Neurol. Neurosurg. 2016, 148, 35–41. [Google Scholar] [CrossRef]
- Kobayashi, K.; Ando, K.; Nakashima, H.; Machino, M.; Kanbara, S.; Ito, S.; Inoue, T.; Yamaguchi, H.; Koshimizu, H.; Segi, N.; et al. Characteristics of Cases with and without Calcification in Spinal Meningiomas. J. Clin. Neurosci. 2021, 89, 20–25. [Google Scholar] [CrossRef]
- Iacoangeli, M.; Gladi, M.; Di Rienzo, A.; Dobran, M.; Alvaro, L.; Nocchi, N.; Maria, L.G.; Somma, D.; Colasanti, R.; Scerrati, M. Minimally Invasive Surgery for Benign Intradural Extramedullary Spinal Meningiomas: Experience of a Single Institution in a Cohort of Elderly Patients and Review of the Literature. Clin. Interv. Aging 2012, 7, 557–564. [Google Scholar] [CrossRef]
- Onken, J.; Obermüller, K.; Staub-Bartelt, F.; Meyer, B.; Vajkoczy, P.; Wostrack, M. Surgical Management of Spinal Meningiomas: Focus on Unilateral Posterior Approach and Anterior Localization. J. Neurosurg. Spine 2018, 30, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Pompili, A.; Caroli, F.; Crispo, F.; Giovannetti, M.; Raus, L.; Vidiri, A.; Telera, S. Unilateral Laminectomy Approach for the Removal of Spinal Meningiomas and Schwannomas: Impact on Pain, Spinal Stability, and Neurologic Results. World Neurosurg. 2016, 85, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Turel, M.K.; D’Souza, W.P.; Rajshekhar, V. Hemilaminectomy Approach for Intradural Extramedullary Spinal Tumors: An Analysis of 164 Patients. Neurosurg. Focus 2015, 39, E9. [Google Scholar] [CrossRef] [PubMed]
- Schwake, M.; Adeli, A.; Sporns, P.; Ewelt, C.; Schmitz, T.; Sicking, J.; Hess, K.; Spille, D.C.; Paulus, W.; Stummer, W.; et al. Spinal Meningiomas—Risks and Potential of an Increasing Age at the Time of Surgery. J. Clin. Neurosci. 2018, 57, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Sandalcioglu, I.E.; Hunold, A.; Müller, O.; Bassiouni, H.; Stolke, D.; Asgari, S. Spinal Meningiomas: Critical Review of 131 Surgically Treated Patients. Eur. Spine J. 2008, 17, 1035–1041. [Google Scholar] [CrossRef]
- Boström, A.; Bürgel, U.; Reinacher, P.; Krings, T.; Rohde, V.; Gilsbach, J.M.; Hans, F.J. A Less Invasive Surgical Concept for the Resection of Spinal Meningiomas. Acta Neurochir. 2008, 150, 551–556; discussion 556. [Google Scholar] [CrossRef]
- Xu, J.; Yu, B.F.; Zheng, W.; Xiao, Y.H.; Lin, Y.; Tian, J.P. Microscopic Keyhole Technique for Surgical Resection of Thoracic Spinal Meningioma via an Oblique Placing Tube. Zhonghua Yi Xue Za Zhi 2019, 99, 983–987. [Google Scholar]
- Saiwai, H.; Okada, S.; Hayashida, M.; Harimaya, K.; Matsumoto, Y.; Kawaguchi, K.I.; Iida, K.I.; Kobayakawa, K.; Yokota, K.; Maeda, T.; et al. Long-Term Outcomes of Spinal Meningioma Resection with Outer Layer of Dura Preservation Technique. J. Clin. Neurosci. 2021, 83, 68–70. [Google Scholar] [CrossRef]
- Aboul-Enein, H.A.; Khidr, W.M.; Abdeen, K.M.; Madawi, A.A. Surgical Management of Ventrally Based Lower Cervical (Subaxial) Meningiomas through the Lateral Approach: Report on 16 Cases. Clin. Neurol. Neurosurg. 2015, 139, 152–158. [Google Scholar] [CrossRef]
- Gambardella, G.; Gervasio, O.; Zaccone, C.; Haase, J. Approaches and Surgical Results in the Treatment of Ventral Thoracic Meningiomas. Review of Our Experience with a Postero-Lateral Combined Transpedicular-Transarticular Approach. Acta Neurochir. 2003, 145, 385–392. [Google Scholar] [CrossRef]
- Gezen, F.; Kahraman, S.; Canakci, Z.; Bedük, A. Review of 36 Cases of Spinal Cord Meningioma. Spine 2000, 25, 727–731. [Google Scholar] [CrossRef]
- Harel, R.; Schleifer, D.; Appel, S.; Attia, M.; Cohen, Z.R.; Knoller, N. Spinal Intradural Extramedullary Tumors: The Value of Intraoperative Neurophysiologic Monitoring on Surgical Outcome. Neurosurg. Rev. 2017, 40, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Abdelmonam Abdelaziz Mostafa Elkatatny, A.; Ramadan, M.; Gouda, A.H.; MHamdy, T.; Samir Fahmy, R.; Farid El Emady, M.; Salaheldin, A. Surgical Outcome of Spinal Meningioma, Single Institute Experience. Pharmacophore 2019, 10, 7–17. [Google Scholar]
- Hohenberger, C.; Gugg, C.; Schmidt, N.O.; Zeman, F.; Schebesch, K.M. Functional Outcome after Surgical Treatment of Spinal Meningioma. J. Clin. Neurosci. 2020, 77, 62–66. [Google Scholar] [CrossRef]
- Khan, H.M.; ul Haq, N.; Ali, M.; Usman, M.; Shah, R. Outcome of Surgical Management in Spinal Meningioma: A Study of 48 Cases. Gomal J. Med. Sci. 2015, 13, 49–53. [Google Scholar]
- Kobayashi, K.; Ando, K.; Matsumoto, T.; Sato, K.; Kato, F.; Kanemura, T.; Yoshihara, H.; Sakai, Y.; Hirasawa, A.; Nakashima, H.; et al. Clinical Features and Prognostic Factors in Spinal Meningioma Surgery from a Multicenter Study. Sci. Rep. 2021, 11, 11630. [Google Scholar] [CrossRef] [PubMed]
- Jesse, C.M.; Abut, P.A.; Wermelinger, J.; Raabe, A.; Schär, R.T.; Seidel, K. Functional Outcome in Spinal Meningioma Surgery and Use of Intraoperative Neurophysiological Monitoring. Cancers 2022, 14, 3989. [Google Scholar] [CrossRef]
- Ambekar, S.; Sharma, M.; Kukreja, S.; Nanda, A. Complications and Outcomes of Surgery for Spinal Meningioma: A Nationwide Inpatient Sample Analysis from 2003 to 2010. Clin. Neurol. Neurosurg. 2014, 118, 65–68. [Google Scholar] [CrossRef]
- Morandi, X.; Haegelen, C.; Riffaud, L.; Amlashi, S.; Adn, M.; Brassier, G. Results in the Operative Treatment of Elderly Patients with Spinal Meningiomas. Spine 2004, 29, 2191–2194. [Google Scholar] [CrossRef]
- Sacko, O.; Haegelen, C.; Mendes, V.; Brenner, A.; Sesay, M.; Brauge, D.; Lagarrigue, J.; Loiseau, H.; Roux, F.E. Spinal Meningioma Surgery in Elderly Patients with Paraplegia or Severe Paraparesis: A Multicenter Study. Neurosurgery 2009, 64, 503–509; discussion 509–510. [Google Scholar] [CrossRef]
- Notani, N.; Miyazaki, M.; Kanezaki, S.; Ishihara, T.; Kawano, M.; Tsumura, H. Surgical Management of Ventrally Located Spinal Meningiomas via Posterior Approach. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Wach, J.; Banat, M.; Schuss, P.; Gueresir, E.; Vatter, H.; Scorzin, J. Age at Diagnosis and Baseline Myelomalacia Sign Predict Functional Outcome After Spinal Meningioma Surgery. Front. Surg. 2021, 8, 682930. [Google Scholar] [CrossRef] [PubMed]
- Kilinc, F.; Setzer, M.; Marquardt, G.; Keil, F.; Dubinski, D.; Bruder, M.; Seifert, V.; Behmanesh, B. Functional Outcome and Morbidity after Microsurgical Resection of Spinal Meningiomas. Neurosurg. Focus 2021, 50, E20. [Google Scholar] [CrossRef] [PubMed]
- Raco, A.; Pesce, A.; Toccaceli, G.; Domenicucci, M.; Miscusi, M.; Delfini, R. Factors Leading to a Poor Functional Outcome in Spinal Meningioma Surgery: Remarks on 173 Cases. Neurosurgery 2017, 80, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Hua, L.; Zhu, H.; Deng, J.; Tian, M.; Jiang, X.; Tang, H.; Luan, S.; Wakimoto, H.; Xie, Q.; Gong, Y. Clinical and Prognostic Features of Spinal Meningioma: A Thorough Analysis from a Single Neurosurgical Center. J. Neurooncol. 2018, 140, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhang, S.; Wang, Q.; Cheng, J.; Deng, X.; Wang, Y.; Hui, X. Spinal Clear Cell Meningioma: Clinical Study with Long-Term Follow-Up in 12 Patients. World Neurosurg. 2019, 122, e415–e426. [Google Scholar] [CrossRef]
- Ye, J.; Lv, G.; Qian, J.; Zhu, J.; Han, R.; Luo, C. Clinical Features and Prognostic Factors of WHO II and III Adult Spinal Meningiomas: Analysis of 25 Cases in a Single Center. J. Neurooncol. 2016, 128, 349–356. [Google Scholar] [CrossRef]
- Sun, S.Q.; Cai, C.; Ravindra, V.M.; Gamble, P.; Yarbrough, C.K.; Dacey, R.G.; Dowling, J.L.; Zipfel, G.J.; Wright, N.M.; Santiago, P.; et al. Simpson Grade I–III Resection of Spinal Atypical (World Health Organization Grade II) Meningiomas Is Associated With Symptom Resolution and Low Recurrence. Neurosurgery 2015, 76, 739–746. [Google Scholar] [CrossRef]
- Krauss, W.E.; Yolcu, Y.U.; Alvi, M.A.; Moinuddin, F.M.; Goyal, A.; Clarke, M.J.; Marsh, W.R.; Bydon, M. Clinical Characteristics and Management Differences for Grade II and III Spinal Meningiomas. J. Neurooncol. 2021, 153, 313–320. [Google Scholar] [CrossRef]
- Han, B.; Zhang, L.; Jia, W.; Yang, J. Clinical Features and Surgical Outcomes of High-Grade Spinal Meningiomas: Report of 19 Cases and Literature Review. J. Clin. Neurosci. 2020, 72, 264–269. [Google Scholar] [CrossRef]
- McCormick, P.C.; Torres, R.; Post, K.D.; Stein, B.M. Intramedullary Ependymoma of the Spinal Cord. J. Neurosurg. 1990, 72, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Karnofsky, D.A.; Abelmann, W.H.; Craver, L.F.; Burchenal, J.H. The Use of the Nitrogen Mustards in the Palliative Treatment of Carcinoma. With Particular Reference to Bronchogenic Carcinoma. Cancer 1945, 14, 634–656. [Google Scholar] [CrossRef]
- Frankel, H.L.; Hancock, D.O.; Hyslop, G.; Melzak, J.; Michaelis, L.S.; Ungar, G.H.; Vernon, J.D.S.; Walsh, J.J. The Value of Postural Reduction in the Initial Management of Closed Injuries of the Spine with Paraplegia and Tetraplegia. I. Paraplegia 1969, 7, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Golanov, A.V.; Konovalov, N.A.; Antipina, N.A.; Vetlova, E.R.; Zolotova, S.V.; Galkin, M.V.; Arutiunov, N.V.; Chamorsov, A.I.; Krasnianskiĭ, S.A.; Nazarenko, A.G.; et al. Stereotactic Radiotherapy for Spinal Meningiomas and Neurinomas. Zh Vopr Neirokhir Im N N Burdenko 2015, 79, 4–13. [Google Scholar] [CrossRef]
- Cohen-Gadol, A.A.; Zikel, O.M.; Koch, C.A.; Scheithauer, B.W.; Krauss, W.E. Spinal Meningiomas in Patients Younger than 50 Years of Age: A 21-Year Experience. J. Neurosurg. 2003, 98, 258–263. [Google Scholar] [CrossRef]
- Gilard, V.; Goia, A.; Ferracci, F.X.; Marguet, F.; Magne, N.; Langlois, O.; Perez, A.; Derrey, S. Spinal Meningioma and Factors Predictive of Post-Operative Deterioration. J. Neurooncol. 2018, 140, 49–54. [Google Scholar] [CrossRef]
- Noh, S.H.; Kim, K.H.; Shin, D.A.; Park, J.Y.; Yi, S.; Kuh, S.U.; Kim, K.N.; Chin, D.K.; Kim, K.S.; Yoon, D.H.; et al. Treatment Outcomes of 17 Patients with Atypical Spinal Meningioma, Including 4 with Metastases: A Retrospective Observational Study. Spine J. 2019, 19, 276–284. [Google Scholar] [CrossRef]
- Voulgaris, S.; Alexiou, G.A.; Mihos, E.; Karagiorgiadis, D.; Zigouris, A.; Fotakopoulos, G.; Drosos, D.; Pahaturidis, D. Posterior Approach to Ventrally Located Spinal Meningiomas. Eur. Spine J. 2010, 19, 1195–1199. [Google Scholar] [CrossRef]
- Wang, X.Q.; Zeng, X.W.; Zhang, B.Y.; Dou, Y.F.; Wu, J.S.; Jiang, C.C.; Zhong, P.; Chen, H. Spinal Meningioma in Childhood: Clinical Features and Treatment. Child’s Nerv. Syst. 2012, 28, 129–136. [Google Scholar] [CrossRef]
- Wu, L.; Yang, C.; Liu, T.; Fang, J.; Yang, J.; Xu, Y. Clinical Features and Long-Term Outcomes of Pediatric Spinal Meningiomas. J. Neurooncol. 2017, 133, 347–355. [Google Scholar] [CrossRef]
- Newman, W.C.; Berry-Candelario, J.; Villavieja, J.; Reiner, A.S.; Bilsky, M.H.; Laufer, I.; Barzilai, O. Improvement in Quality of Life Following Surgical Resection of Benign Intradural Extramedullary Tumors: A Prospective Evaluation of Patient-Reported Outcomes. Neurosurgery 2021, 88, 989–995. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | Nature of the Complication | Example of Complication |
|---|---|---|
| 1 | Any medical or surgical non–life-threatening deviation from normal operative/postoperative course, requiring either non-invasive treatment or no treatment at all. |
|
| 2 | Medical or surgical complication requiring invasive treatment, with or without general anesthesia. |
|
| 3 | Medical or surgical life-threatening complications requiring ICU care, with either single or multi-organ failure. |
|
| 4 | Any medical or surgical complication leading to operative or postoperative death. | Perioperative death as the ultimate endpoint |
| Number of Studies | Certainty Assessment | Impact | Certainty | Importance | |||||
|---|---|---|---|---|---|---|---|---|---|
| Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | ||||
| (1) Worse preoperative status | |||||||||
| 12 | Observational studies | Not serious | Serious a | Serious b | Not serious | Strong association | There seems to be evidence linking worse preoperative status to unfavorable outcomes, knowing that most of the studies taking part in this analysis had low risks of bias and showed statistically significant results. | ⨁⨁⨁◯ Moderate | CRITICAL |
| (2) Older age | |||||||||
| 11 | Observational studies | Not serious | Very serious c | Not serious | Not serious | None | The body of evidence supporting older age as a marker of unfavorable outcomes is mostly relying on studies with statistically insignificant results, hence the low certainty level. | ⨁⨁◯◯ Low | NOT IMPORTANT |
| (3) Male sex | |||||||||
| 10 | Observational studies | Not serious | Very serious c | Not serious | Serious d | None | The evidence suggesting male sex as an indicator of poor outcome is backed by a majority of studies showing insignificant results, which is reflected by very low certainty levels. | ⨁◯◯◯ Very low | NOT IMPORTANT |
| (4) Higher WHO grade | |||||||||
| 10 | Observational studies | Not serious | Serious a | Not serious | Serious d | None | There seems to be weak evidence linking tumors with higher WHO grades to unfavorable postoperative outcomes, especially that most studies studying this association revealed insignificant results. | ⨁⨁◯◯ Low | IMPORTANT |
| (5) Longer duration of symptoms or longer waiting time before surgery | |||||||||
| 9 | Observational studies | Not serious | Serious a | Serious b | Not serious | Strong association | The evidence supporting longer timespans before surgery as a marker for poor postoperative outcomes seems to be of moderate strength. Studies that supported this claim were unbiased, and most of them had initially concluded significant results. | ⨁⨁⨁◯ Moderate | CRITICAL |
| (6) Craniocaudal tumor location | |||||||||
| 8 | Observational studies | Not serious | Very serious c | Not serious | Not serious | None | The claim that spinal meningiomas of specific spinal levels may be associated to worse postoperative outcomes is based on studies revealing statistically insignificant results, hence justifying the low level of certainty towards the evidence. | ⨁⨁◯◯ Low | NOT IMPORTANT |
| (7) Ventral attachment | |||||||||
| 8 | Observational studies | Not serious | Very serious c | Not serious | Not serious | None | There is low-certainty evidence backing up the association between tumors of ventral origin and unfavorable postoperative outcomes, mainly stemming from the insignificant results found by most studies included in the synthesis. | ⨁⨁◯◯ Low | NOT IMPORTANT |
| (8) Higher Simpson grade | |||||||||
| 8 | Observational studies | Not serious | Very serious c | Not serious | Not serious | None | There is low-certainty evidence backing up the association between a higher Simpson resection grade and unfavorable postoperative outcomes, mainly stemming from the insignificant results found by most studies included in the synthesis. | ⨁⨁◯◯ Low | NOT IMPORTANT |
| (9) Larger tumor size and spinal cord compression | |||||||||
| 5 | Observational studies | Not serious | Very serious c | Very serious b | Not serious | None | The evidence suggesting larger tumor sizes as an indicator of poor outcome is backed by a majority of studies showing insignificant results, which is reflected by very low certainty levels. | ⨁◯◯◯ Very low | NOT IMPORTANT |
| (10) Surgery for recurrent tumor | |||||||||
| 3 | Observational studies | Not serious | Not serious | Not serious | Serious e | Strong association | There seems to be strong evidence suggesting that the reoperation of tumors may be associated with unfavorable postoperative outcomes. | ⨁⨁⨁⨁ High | CRITICAL |
| (11) Presence of calcification | |||||||||
| 2 | Observational studies | Not serious | Very serious c | Not serious | Very serious d,e | None | There seems to be poor evidence suggesting an association between tumor calcification and worse postoperative outcomes, as there were only two studies that addressed this aspect with mixed-significance results. | ⨁◯◯◯ Very low | NOT IMPORTANT |
| Certainty Assessment | No. of Patients | Effect | Certainty | Significance and Importance | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of Studies | Mean Follow-Up (mos) | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Simpson Grade 1 | Simpson Grade 2 | Relative (95% CI) | Absolute (95% CI) | ||
| (1) Simpson grades 1 or 2 vs. Simpson grades 3, 4 or 5 resection of spinal meningiomas | |||||||||||||
| 25 | 62.4 | Observational studies | Not serious | Not serious | Not serious | Not serious | Very strong association | 41/1326 (3.1%) | 74/266 (27.8%) | OR 0.08 (0.04 to 0.15) | 248 fewer per 1000 (from 263 fewer to 224 fewer) | ⨁⨁⨁⨁High | SIGNIFICANT, CRITICAL |
| (2) WHO grade 1 vs. WHO grade 2 or 3 spinal meningiomas | |||||||||||||
| 22 | 53.2 | Observational studies | Not serious | Not serious | Not serious | Not serious | Very strong association | 83/1591 (5.2%) | 32/69 (46.4%) | OR 0.09 (0.04 to 0.21) | 392 fewer per 1000 (from 430 fewer to 310 fewer) | ⨁⨁⨁⨁High | SIGNIFICANT, CRITICAL |
| (3) Ventral vs. non-ventral spinal meningiomas | |||||||||||||
| 9 | 70.9 | Observational studies | Not serious | Not serious | Not serious | Not serious | Strong association | 20/392 (5.1%) | 24/168 (14.3%) | OR 2.56 (1.16 to 5.67) | 156 more per 1000 (from 19 more to 343 more) | ⨁⨁⨁◯Moderate | SIGNIFICANT, CRITICAL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Hajj, V.G.; Pettersson-Segerlind, J.; Fletcher-Sandersjöö, A.; Edström, E.; Elmi-Terander, A. Current Knowledge on Spinal Meningiomas—Surgical Treatment, Complications, and Outcomes: A Systematic Review and Meta-Analysis (Part 2). Cancers 2022, 14, 6221. https://doi.org/10.3390/cancers14246221
El-Hajj VG, Pettersson-Segerlind J, Fletcher-Sandersjöö A, Edström E, Elmi-Terander A. Current Knowledge on Spinal Meningiomas—Surgical Treatment, Complications, and Outcomes: A Systematic Review and Meta-Analysis (Part 2). Cancers. 2022; 14(24):6221. https://doi.org/10.3390/cancers14246221
Chicago/Turabian StyleEl-Hajj, Victor Gabriel, Jenny Pettersson-Segerlind, Alexander Fletcher-Sandersjöö, Erik Edström, and Adrian Elmi-Terander. 2022. "Current Knowledge on Spinal Meningiomas—Surgical Treatment, Complications, and Outcomes: A Systematic Review and Meta-Analysis (Part 2)" Cancers 14, no. 24: 6221. https://doi.org/10.3390/cancers14246221
APA StyleEl-Hajj, V. G., Pettersson-Segerlind, J., Fletcher-Sandersjöö, A., Edström, E., & Elmi-Terander, A. (2022). Current Knowledge on Spinal Meningiomas—Surgical Treatment, Complications, and Outcomes: A Systematic Review and Meta-Analysis (Part 2). Cancers, 14(24), 6221. https://doi.org/10.3390/cancers14246221