
The Lymphatic System, Lymphoedema, and Medical Curricula–Survey of Australian Medical Graduates

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Respondents and Participant Characteristics
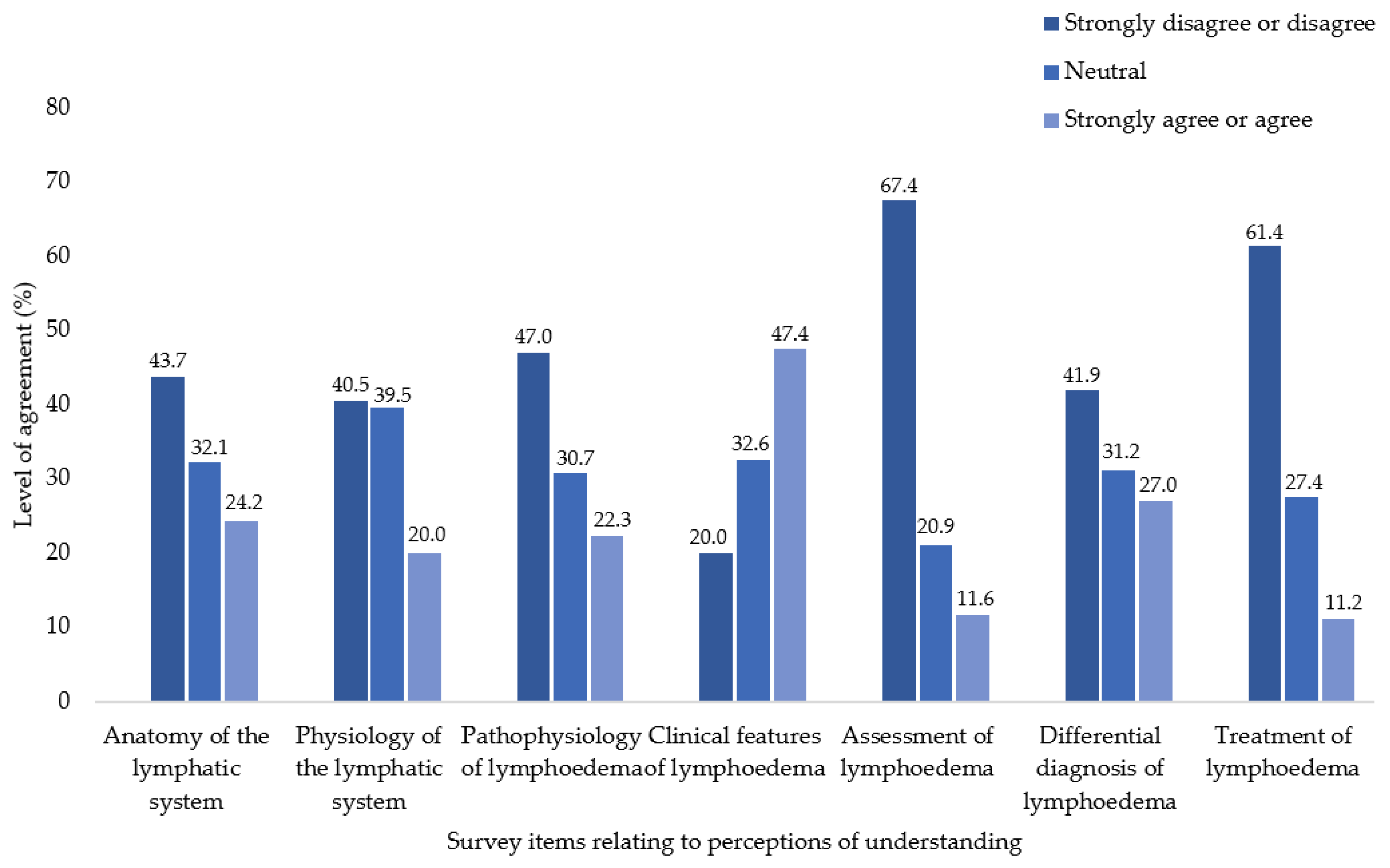
3.2. Perceptions of Understanding
3.3. Perceptions of Medical Curricula
3.4. Perceptions of Appropriateness for Clinical Practice
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lymphoedema Framework. Best Practice for the Management of Lymphoedema; MEP Ltd: London, UK, 2006. [Google Scholar]
- World Health Organization. Lymphatic Filariasis—Managing Morbidity and Preventing Disability: An Aide-Mémoire for National Programme Managers, 2nd ed.; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Moffatt, C.; Keeley, V.; Quéré, I. The Concept of Chronic Edema—A Neglected Public Health Issue and an International Response: The LIMPRINT Study. Lymphat. Res. Biol. 2019, 17, 121–126. [Google Scholar] [CrossRef] [PubMed]
- DiSipio, T.; Rye, S.; Newman, B.; Hayes, S. Incidence of unilateral arm lymphoedema after breast cancer: A systematic review and meta-analysis. Lancet Oncol. 2013, 14, 500–515. [Google Scholar] [CrossRef] [PubMed]
- Moffatt, C.J.; Gaskin, R.; Sykorova, M.; Dring, E.; Aubeeluck, A.; Franks, P.J.; Windrum, P.; Mercier, G.; Pinnington, L.; Quéré, I. Prevalence and Risk Factors for Chronic Edema in U.K. Community Nursing Services. Lymphat. Res. Biol. 2019, 17, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Gordon, S.J.; Murray, S.G.; Sutton, T.; Coulombe, M.-M.; James, S.J.; Van Zanten, M.; Lawson, J.K.; Moffatt, C. LIMPRINT in Australia. Lymphat. Res. Biol. 2019, 17, 173–177. [Google Scholar] [CrossRef]
- Mercier, G.; Pastor, J.; Moffatt, C.; Franks, P.; Quéré, I. LIMPRINT: Health-Related Quality of Life in Adult Patients with Chronic Edema. Lymphat. Res. Biol. 2019, 17, 163–167. [Google Scholar] [CrossRef]
- Lee, B.-B.; Rockson, S.G.; Bergan, J. Lymphedema: A Concise Compendium of Theory and Practice; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar] [CrossRef]
- Pearce, J.; Gordon, K.; Mortimer, P. Vascular and lymphatic abnormalities. Medicine 2021, 49, 404–406. [Google Scholar] [CrossRef]
- International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema: 2016 Consensus Document of the International Society of Lymphology. Acta Angiol. 2017, 23, 171–182. [Google Scholar]
- Burian, E.A.; Karlsmark, T.; Franks, P.J.; Keeley, V.; Quéré, I.; Moffatt, C.J. Cellulitis in chronic oedema of the lower leg: An international cross-sectional study. Br. J. Dermatol. (1951) 2021, 185, 110–118. [Google Scholar] [CrossRef]
- Raff, A.B.; Kroshinsky, D. Cellulitis: A review. JAMA 2016, 316, 325–337. [Google Scholar] [CrossRef]
- Mortimer, P.S.; Rockson, S.G. New developments in clinical aspects of lymphatic disease. J. Clin. Investig. 2014, 124, 915–921. [Google Scholar] [CrossRef]
- Koelmeyer, L.A.; Borotkanics, R.J.; Alcorso, J.; Prah, P.; Winch, C.J.; Nakhel, K.; Dean, C.M.; Boyages, J. Early surveillance is associated with less incidence and severity of breast cancer–related lymphedema compared with a traditional referral model of care. Cancer 2019, 125, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Webb, E.; Neeman, T.; Bowden, F.J.; Gaida, J.; Mumford, V.; Bissett, B. Compression Therapy to Prevent Recurrent Cellulitis of the Leg. N. Engl. J. Med. 2020, 383, 630–639. [Google Scholar] [CrossRef]
- Webb, E.; Bissett, B.; Neeman, T.; Bowden, F.; Preston, E.; Mumford, V. Compression Therapy Is Cost-Saving in the Prevention of Lower Limb Recurrent Cellulitis in Patients with Chronic Edema. Lymphat. Res. Biol. 2022. (Ahead of Print). [Google Scholar] [CrossRef] [PubMed]
- Chang, D.W.; Suami, H.; Skoracki, R. A prospective analysis of 100 consecutive lymphovenous bypass cases for treatment of extremity lymphedema. Plast. Reconstr. Surg. 2013, 132, 1305–1314. [Google Scholar] [CrossRef]
- Schiltz, D.; Kiermeier, N.; Müller, K.; Diesch, S.T.; Wenzel, C.; Biermann, N.; Prantl, L.; Taeger, C.D. Quality of life evaluation and lack of correlation with volumetric results after lymphovenous anastomoses in lymphedema therapy of the lower extremity. J. Vasc. Surg. Venous Lymphat. Disord. 2022, 10, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Venkatramani, H.; Shanmugakrishnan, R.R.; Kumaran, M.S.; Sabapathy, S.R. Surgical debulking, lymphatico venous anastomosis, vascularised lymph node transfer in lower limb lymphoedema. Plast. Aesthetic Res. 2020, 7, 19. [Google Scholar] [CrossRef]
- Yarmohammadi, H.; Rooddehghan, A.; Soltanipur, M.; Sarafraz, A.; Mahdavi Anari, S.F. Healthcare Practitioners’ Knowledge of Lymphedema. Int. J. Vasc. Med. 2021, 2021, 3806150. [Google Scholar] [CrossRef]
- Rockson, S.G. Lymphatic Medicine: Paradoxically and Unnecessarily Ignored. Lymphat. Res. Biol. 2017, 15, 315–316. [Google Scholar] [CrossRef]
- Vuong, D.; Nguyen, M.; Piller, N. Medical education: A deficiency or a disgrace. J. Lymphoedema 2011, 6, 44–49. [Google Scholar]
- Schulze, H.; Nacke, M.; Gutenbrunner, C.; Hadamitzky, C. Worldwide assessment of healthcare personnel dealing with lymphoedema. Health Econ. Rev. 2018, 8, 10–11. [Google Scholar] [CrossRef]
- Granger, D.N.; Skeff, K.M.; Chaite, W.; Rockson, S.G. Lymphatic biology and disease: Is it being taught? Who is listening? Lymphat. Res. Biol. 2004, 2, 86–95. [Google Scholar] [CrossRef] [PubMed]
- International Lymphoedema Framework. Lymphoedema Education Benchmark Statements. Available online: https://www.lympho.org/lymphoedema-education-benchmark-statements/ (accessed on 5 January 2022).
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef] [PubMed]
- Teitcher, J.E.; Bockting, W.O.; Bauermeister, J.A.; Hoefer, C.J.; Miner, M.H.; Klitzman, R.L. Detecting, preventing, and responding to “fraudsters” in internet research: Ethics and tradeoffs. J. Law Med. Ethics 2015, 43, 116–133. [Google Scholar] [CrossRef] [PubMed]
- Griffin, M.; Martino, R.J.; LoSchiavo, C.; Comer-Carruthers, C.; Krause, K.D.; Stults, C.B.; Halkitis, P.N. Ensuring survey research data integrity in the era of internet bots. Qual. Quant. 2021, 56, 2841–2852. [Google Scholar] [CrossRef] [PubMed]
- Cortina, J.M. What is coefficient alpha? An examination of theory and applications. J. Appl. Psychol. 1993, 78, 98. [Google Scholar] [CrossRef]
- Doubblestein, D.A. The lived experience of primary lymphoedema: A phenomenological study of personage and caregiver. J. Lymphoedema 2020, 15, 22–28. [Google Scholar]
- Piller, N. What about us? The patient perspective. J. Lymphoedema 2020, 15, 5. [Google Scholar]
- Wilting, J.; Becker, J. The lymphatic vascular system: Much more than just a sewer. Cell Biosci. 2022, 12, 157. [Google Scholar] [CrossRef]
- Rockson, S.G. Advances in lymphedema. Circ. Res. 2021, 128, 2003–2016. [Google Scholar] [CrossRef]
- Connell, F.; Brice, G.; Jeffery, S.; Keeley, V.; Mortimer, P.; Mansour, S. A new classification system for primary lymphatic dysplasias based on phenotype. Clin. Genet. 2010, 77, 438–452. [Google Scholar] [CrossRef]
- Connell, F.C.; Gordon, K.; Brice, G.; Keeley, V.; Jeffery, S.; Mortimer, P.S.; Mansour, S.; Ostergaard, P. The classification and diagnostic algorithm for primary lymphatic dysplasia: An update from 2010 to include molecular findings. Clin. Genet. 2013, 84, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Gordon, K.; Varney, R.; Keeley, V.; Riches, K.; Jeffery, S.; Van Zanten, M.; Mortimer, P.; Ostergaard, P.; Mansour, S. Update and audit of the St George’s classification algorithm of primary lymphatic anomalies: A clinical and molecular approach to diagnosis. J. Med. Genet. 2020, 57, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Potentially preventable hospitalisations in Australia by age groups and small geographic areas, 2017–18. Available online: https://www.aihw.gov.au/reports/primary-health-care/potentially-preventable-hospitalisations (accessed on 5 January 2021).
- Kumar, M.; Jindal, M.K.; Kumar, M. A Systematic Survey on CAPTCHA Recognition: Types, Creation and Breaking Techniques. Arch. Comput. Methods Eng. 2022, 29, 1107–1136. [Google Scholar] [CrossRef]
- Godinho, A.; Schell, C.; Cunningham, J.A. Out damn bot, out: Recruiting real people into substance use studies on the internet. Subst. Abus. 2020, 41, 3–5. [Google Scholar] [CrossRef]
- Medical Deans. 2021 Student Statistics Snapshot; Medical Deans Australia and New Zealand: Sydney, NSW, Australia, 2021. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | n (%) |
|---|---|
| Sex | |
| Male | 83 (36.1) |
| Female | 132 (57.4) |
| Non-binary | 3 (1.3) |
| Prefer not to say | 5 (2.2) |
| Missing | 7 (3.0) |
| Age (years); median, interquartile range (IQR) | 26, 25–28 |
| Enrolment Type | |
| Undergraduate | 70 (30.5) |
| Postgraduate | 153 (66.5) |
| Missing | 7 (3.0) |
| State/Territory of Medical Degree | |
| Queensland | 76 (33.1) |
| New South Wales | 46 (20.0) |
| Victoria | 57 (24.8) |
| South Australia | 14 (6.1) |
| Western Australia | 12 (5.2) |
| Tasmania | 5 (2.2) |
| Australian Capital Territory | 12 (5.2) |
| Northern Territory | 1 (0.4) |
| Missing | 7 (3.0) |
| State/Territory of Employment | |
| Queensland | 79 (34.4) |
| New South Wales | 51 (22.2) |
| Victoria | 53 (23.0) |
| South Australia | 14 (6.1) |
| Western Australia | 13 (5.7) |
| Tasmania | 3 (1.3) |
| Australian Capital Territory | 5 (2.2) |
| Northern Territory | 4 (1.7) |
| Outside Australia | 1 (0.4) |
| Missing | 7 (3.0) |
| Clinical Setting Type | |
| Public Hospital | 217 (94.4) |
| Private Hospital | 3 (1.4) |
| Community Health Facility | 1 (0.4) |
| General Practice | 1 (0.4) |
| Aged Care | 0 (0.0) |
| Other | 1 (0.4) |
| Missing | 7 (3.0) |
| Clinical Setting Location | |
| Metropolitan area | 133 (57.9) |
| Regional area | 79 (34.4) |
| Rural area | 10 (4.3) |
| Other | 1 (0.4) |
| Missing | 7 (3.0) |
| Characteristic | Understanding | Medical Curricula | ||||
|---|---|---|---|---|---|---|
| n | Mean (SD) | p-Value | n | Mean (SD) | p-Value | |
| Total sample (score ranging between 7–35) | 215 | 18.8 (4.4) | 205 | 17.4 (5.4) | ||
| Sex | 0.15 | 0.23 | ||||
| Male | 79 | 18.9 (4.7) | 75 | 18.1 (5.2) | ||
| Female | 131 | 18.9 (4.2) | 126 | 17.2 (5.3) | ||
| Non-binary | 3 | 13.3 (5.5) | 3 | 12.7 (8.1) | ||
| Prefer not to say | 2 | 16.0 (0.0) | 1 | 14.0 (-) | ||
| Age | 0.79 | 0.15 | ||||
| <25 | 96 | 18.8 (4.5) | 91 | 18.1 (5.2) | ||
| 26–30 | 85 | 18.8 (4.3) | 80 | 17 (5.0) | ||
| 31–35 | 19 | 17.8 (5.1) | 19 | 15.5 (7.0) | ||
| 36+ | 15 | 19.3 (3.9) | 15 | 18.7 (5.3) | ||
| Enrolment Type | 0.76 | 0.37 | ||||
| Undergraduate | 66 | 18.9 (4.0) | 62 | 18 (5.8) | ||
| Postgraduate | 149 | 18.7 (4.6) | 143 | 17.2 (5.1) | ||
| State/Territory of Medical Degree | 0.79 | 0.11 | ||||
| Queensland | 73 | 19.4 (4.6) | 71 | 18.2 (4.8) | ||
| New South Wales | 45 | 18.6 (4.4) | 43 | 16.2 (5.2) | ||
| Victoria | 55 | 18.1 (4.7) | 51 | 17.5 (6.1) | ||
| South Australia | 14 | 18.8 (3.9) | 13 | 15 (5.1) | ||
| Western Australia | 11 | 18.7 (2.9) | 11 | 20.3 (5.1) | ||
| Tasmania | 5 | 18.2 (4.4) | 4 | 19 (5.8) | ||
| Australian Capital Territory | 12 | 18.9 (4.2) | 12 | 16.7 (4.6) | ||
| Northern Territory | - | - | - | - | ||
| State/Territory of Employment | 0.21 | 0.24 | ||||
| Queensland | 77 | 19.4 (4.5) | 74 | 18.2 (4.9) | ||
| New South Wales | 50 | 19.2 (4.3) | 47 | 17.2 (5.3) | ||
| Victoria | 51 | 18.1 (4.2) | 48 | 17.2 (5.8) | ||
| South Australia | 14 | 18.8 (3.9) | 13 | 15.1 (5.2) | ||
| Western Australia | 12 | 18.0 (4.5) | 12 | 19.3 (6.0) | ||
| Tasmania | 3 | 15.3 (9.1) | 3 | 15.7 (7.6) | ||
| Australian Capital Territory | 5 | 18.8 (3.4) | 5 | 16.0 (2.9) | ||
| Northern Territory | 3 | 13.3 (5.0) | 3 | 12.3 (4.5) | ||
| Outside Australia | - | - | - | - | ||
| Clinical Setting Type | 0.44 | 0.15 | ||||
| Public Hospital | 210 | 18.7 (4.4) | 200 | 17.5 (5.3) | ||
| Private Hospital | 3 | 22.3 (5.7) | 3 | 21.7 (2.5) | ||
| Community Health Facility | 1 | 16.0 (-) | 1 | 8.0 (-) | ||
| General Practice | 1 | 16.0 (-) | 1 | 14.0 (-) | ||
| Aged Care | - | - | - | - | ||
| Other | - | - | - | - | ||
| Clinical Setting Location | 0.59 | 0.87 | ||||
| Metropolitan area | 127 | 19.0 (4.5) | 121 | 17.5 (5.2) | ||
| Regional area | 78 | 18.4 (4.5) | 74 | 17.3 (5.6) | ||
| Rural area | 10 | 19.4 (3.0) | 10 | 18.2 (5.4) | ||
| Other | - | - | - | - | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kruger, N.; Plinsinga, M.L.; Noble-Jones, R.; Piller, N.; Keeley, V.; Hayes, S.C. The Lymphatic System, Lymphoedema, and Medical Curricula–Survey of Australian Medical Graduates. Cancers 2022, 14, 6219. https://doi.org/10.3390/cancers14246219
Kruger N, Plinsinga ML, Noble-Jones R, Piller N, Keeley V, Hayes SC. The Lymphatic System, Lymphoedema, and Medical Curricula–Survey of Australian Medical Graduates. Cancers. 2022; 14(24):6219. https://doi.org/10.3390/cancers14246219
Chicago/Turabian StyleKruger, Natalie, Melanie L. Plinsinga, Rhian Noble-Jones, Neil Piller, Vaughan Keeley, and Sandra C. Hayes. 2022. "The Lymphatic System, Lymphoedema, and Medical Curricula–Survey of Australian Medical Graduates" Cancers 14, no. 24: 6219. https://doi.org/10.3390/cancers14246219
APA StyleKruger, N., Plinsinga, M. L., Noble-Jones, R., Piller, N., Keeley, V., & Hayes, S. C. (2022). The Lymphatic System, Lymphoedema, and Medical Curricula–Survey of Australian Medical Graduates. Cancers, 14(24), 6219. https://doi.org/10.3390/cancers14246219