
Clinical Outcomes in Fibrolamellar Hepatocellular Carcinoma Treated with Immune Checkpoint Inhibitors

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Assessments and Analyses
3. Results
3.1. FLC Is Characterized by a Low Tumor Mutation Burden (TMB) and Low PD-L1 Positivity
3.2. Clinical Characteristics
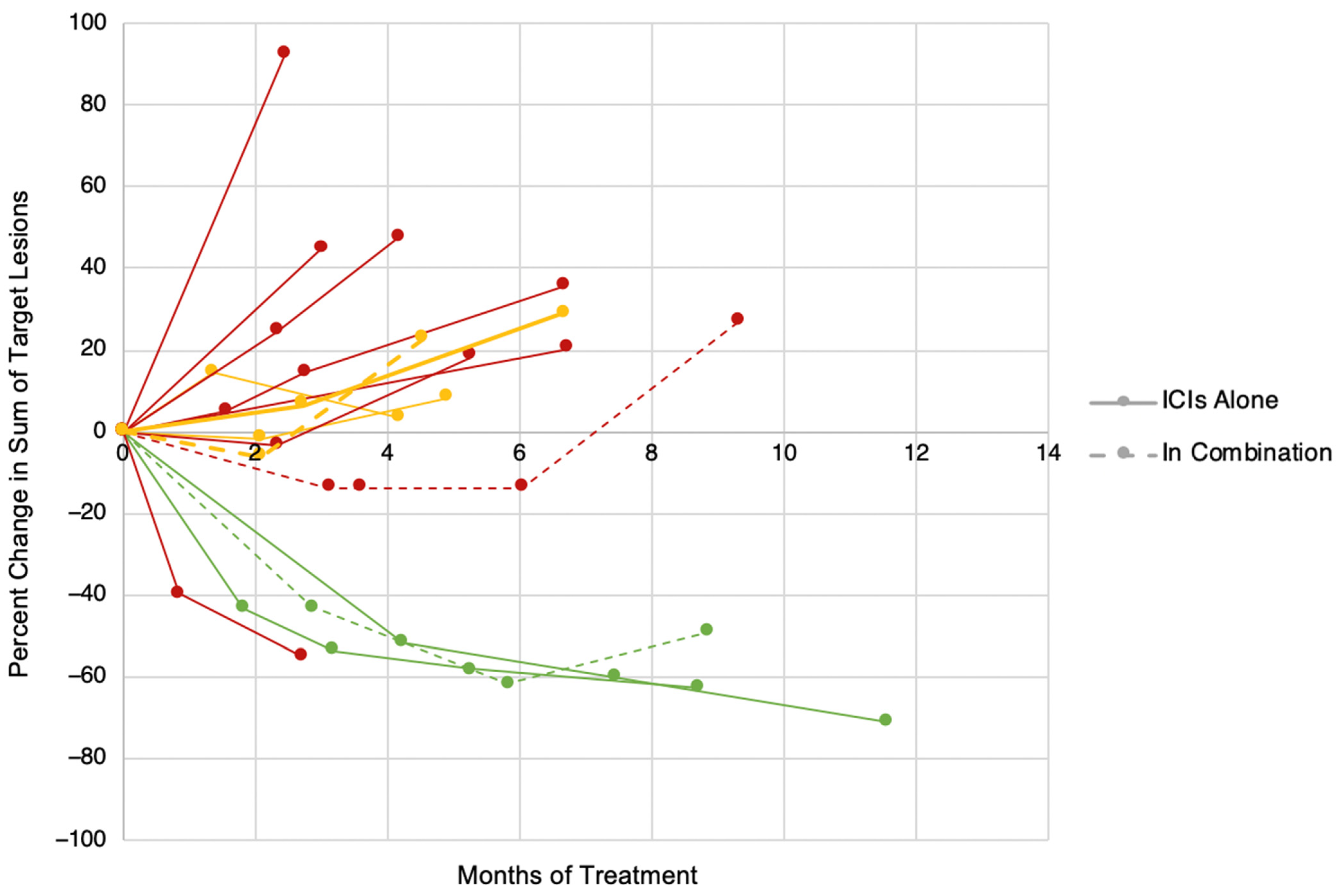
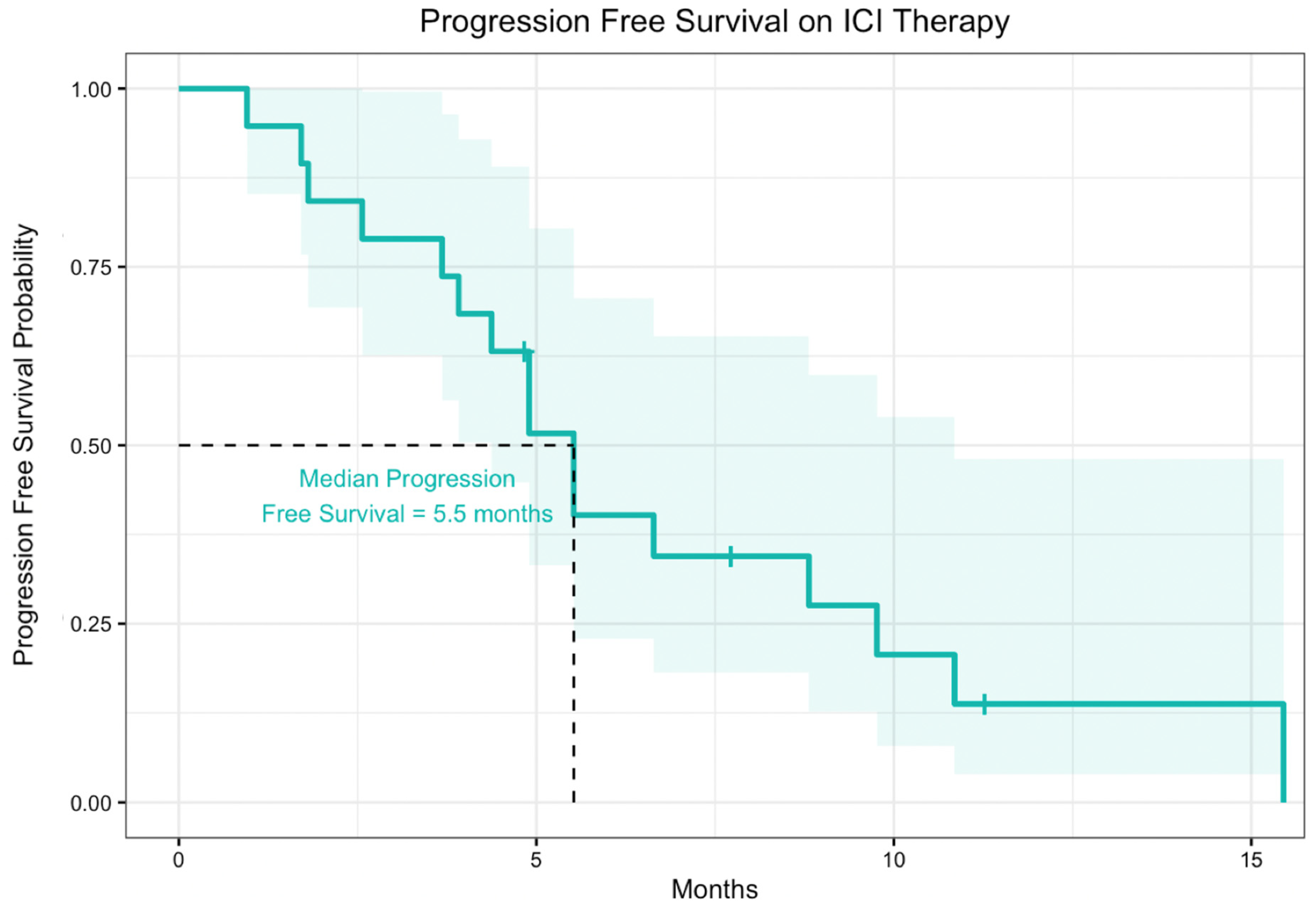
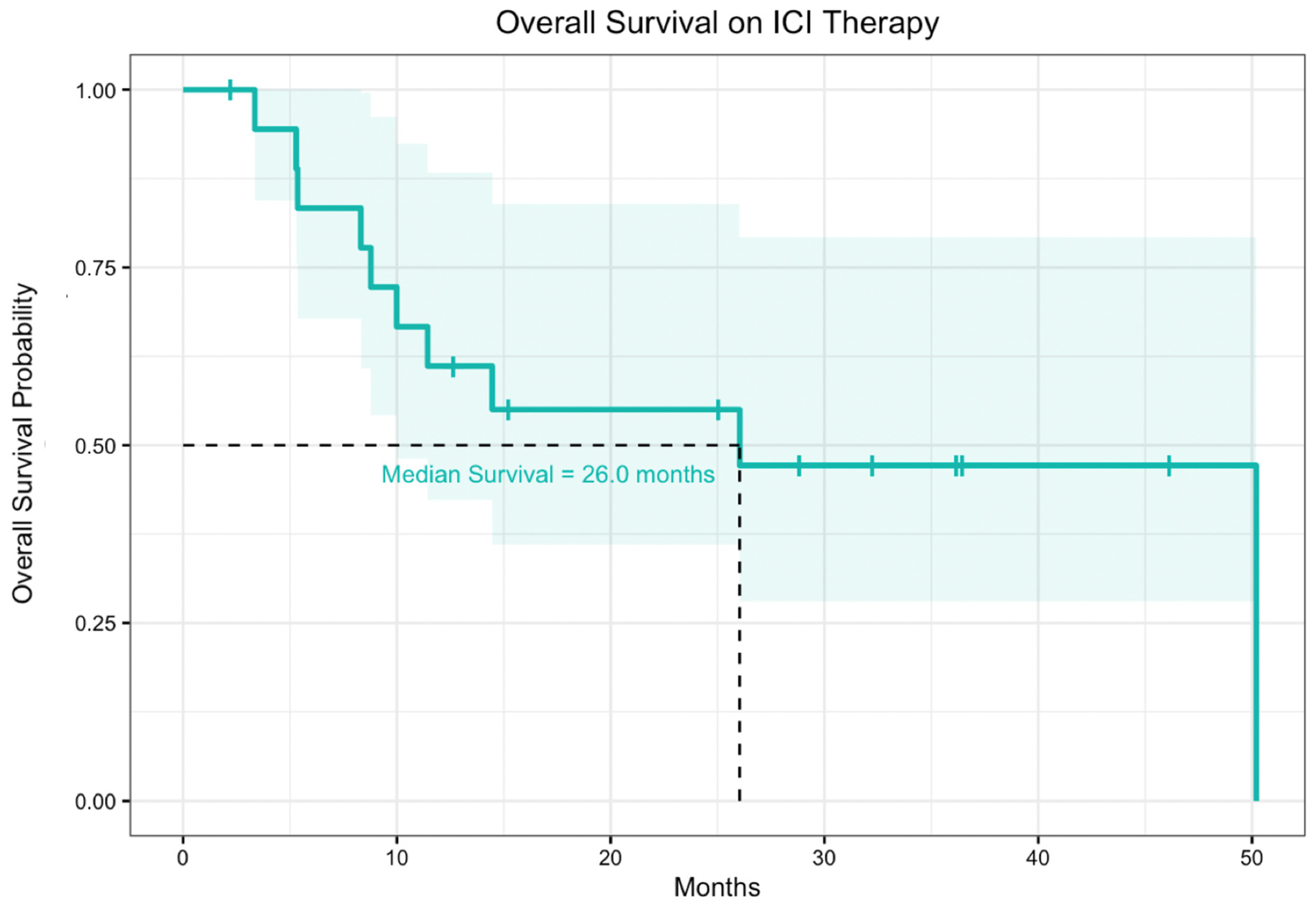
3.3. Efficacy
3.4. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Honeyman, J.N.; Simon, E.P.; Robine, N.; Chiaroni-Clarke, R.; Darcy, D.G.; Lim, I.I.P.; Gleason, C.E.; Murphy, J.M.; Rosenberg, B.R.; Teegan, L.; et al. Detection of a recurrent DNAJB1-PRKACA chimeric transcript in fibrolamellar hepatocellular carcinoma. Science 2014, 343, 1010–1014. [Google Scholar] [CrossRef] [PubMed]
- Graham, R.P.; Jin, L.; Knutson, D.L.; Kloft-Nelson, S.M.; Greipp, P.T.; Waldburger, N.; Roessler, S.; Longerich, T.; Roberts, L.R.; Oliveira, A.M.; et al. DNAJB1-PRKACA is specific for fibrolamellar carcinoma. Mod. Pathol. 2015, 28, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Kastenhuber, E.R.; Lalazar, G.; Houlihan, S.L.; Tschaharganeh, D.F.; Baslan, T.; Chen, C.C.; Requena, D.; Tian, S.; Bosbach, B.; Wilkinson, J.E.; et al. DNAJB1–PRKACA fusion kinase interacts with β-catenin and the liver regenerative response to drive fibrolamellar hepatocellular carcinoma. Proc. Natl. Acad. Sci. USA 2017, 114, 13076–13084. [Google Scholar] [CrossRef] [PubMed]
- Graham, R.P. Fibrolamellar Carcinoma: What Is New and Why It Matters. Surg. Pathol. Clin. 2018, 11, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Pawlik, T.; Lafaro, K. Fibrolamellar hepatocellular carcinoma: Current clinical perspectives. J. Hepatocell. Carcinoma 2015, 2, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Mavros, M.N.; Mayo, S.C.; Hyder, O.; Pawlik, T.M. A systematic review: Treatment and prognosis of patients with fibrolamellar hepatocellular carcinoma. J. Am. Coll. Surg. 2012, 215, 820–830. [Google Scholar] [CrossRef] [PubMed]
- Kassahun, W.T. Contemporary management of fibrolamellar hepatocellular carcinoma: Diagnosis, treatment, outcome, prognostic factors, and recent developments. World J. Surg. Oncol. 2016, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ang, C.S.; Kelley, R.K.; Choti, M.A.; Cosgrove, D.P.; Chou, J.F.; Klimstra, D.; Torbenson, M.S.; Ferrell, L.; Pawlik, T.M.; Fong, Y.; et al. Clinicopathologic characteristics and survival outcomes of patients with Fibrolamellar carcinoma: Data from the Fibrolamellar Carcinoma consortium. Gastrointest Cancer Res. 2013, 6, 3–9. [Google Scholar] [PubMed]
- Kaseb, A.O.; Shama, M.; Sahin, I.H.; Nooka, A.; Hassabo, H.M.; Vauthey, J.N.; Aloia, T.; Abbruzzese, J.L.; Subbiah, I.M.; Janku, F.; et al. Prognostic indicators and treatment outcome in 94 cases of fibrolamellar hepatocellular carcinoma. Oncology 2013, 85, 197–203. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, A.F.; Church, A.J.; Perez-Atayde, A.R.; Shaikh, R.; Marcus, K.J.; Vakili, K. Fibrolamellar carcinoma: An entity all its own. Curr. Probl. Cancer 2021, 45, 100770. [Google Scholar] [CrossRef] [PubMed]
- Donisi, C.; Puzzoni, M.; Ziranu, P.; Lai, E.; Mariani, S.; Saba, G.; Impera, V.; Dubois, M.; Persano, M.; Migliari, M.; et al. Immune Checkpoint Inhibitors in the Treatment of HCC. Front. Oncol. 2021, 10, 601240. [Google Scholar] [CrossRef] [PubMed]
- Yau, T.; Kang, Y.K.; Kim, T.Y.; El-Khoueiry, A.B.; Santoro, A.; Sangro, B.; Melero, I.; Kudo, M.; Hou, M.M.; Matilla, A.; et al. Nivolumab (NIVO) + ipilimumab (IPI) combination therapy in patients (pts) with advanced hepatocellular carcinoma (aHCC): Results from CheckMate 040. J. Clin. Oncol. 2019, 6, e204564. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.A.; Yarchoan, M.; Jaffee, E.; Swanton, C.; Quezada, S.A.; Stenzinger, A.; Peters, S. Development of tumor mutation burden as an immunotherapy biomarker: Utility for the oncology clinic. Ann. Oncol. 2018, 30, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Yarchoan, M.; Hopkins, A.; Jaffee, E.M. Tumor Mutational Burden and Response Rate to PD-1 Inhibition. N. Engl. J. Med. 2017, 377, 2500–2501; PMID: 29262275. [Google Scholar] [CrossRef] [PubMed]
- Fumet, J.D.; Truntzer, C.; Yarchoan, M.; Ghiringhelli, F. Tumour mutational burden as a biomarker for immunotherapy: Current data and emerging concepts. Eur. J. Cancer 2020, 131, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, Z.R.; Connelly, C.F.; Fabrizio, D.; Gay, L.; Ali, S.M.; Ennis, R.; Schrock, A.; Campbell, B.; Shlien, A.; Chmielecki, J.; et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017, 9, 34. [Google Scholar] [CrossRef]
- Marabelle, A.; Fakih, M.; Lopez, J.; Shah, M.; Shapira-Frommer, R.; Nakagawa, K.; Chung, H.C.; Kindler, H.L.; Lopez-Martin, J.A.; Miller, W.H.; et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: Prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol. 2020, 21, 1353–1365. [Google Scholar] [CrossRef] [PubMed]
- Yarchoan, M.; Albacker, L.A.; Hopkins, A.C.; Montesion, M.; Murugesan, K.; Vithayathil, T.T.; Zaidi, N.; Azad, N.S.; Laheru, D.A.; Frampton, G.M.; et al. PD-L1 expression and tumor mutational burden are independent biomarkers in most cancers. JCI Insight 2019, 4. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Ryoo, B.Y.; Merle, P.; Kudo, M.; Bouattour, M.; Lim, H.Y.; Breder, V.; Edeline, J.; Chao, Y.; Ogasawara, S.; et al. Pembrolizumab As Second-Line Therapy in Patients With Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. J. Clin. Oncol. 2020, 38, 193–202; PMID: 31790344. [Google Scholar] [CrossRef] [PubMed]
- Yau, T.; Park, J.W.; Finn, R.S.; Cheng, A.L.; Mathurin, P.; Edeline, J.; Kudo, M.; Han, K.H.; Harding, J.J.; Merle, P.; et al. CheckMate 459: A randomized, multi-center phase III study of nivolumab (NIVO) vs sorafenib (SOR) as first-line (1L) treatment in patients (pts) with advanced hepatocellular carcinoma (aHCC). Ann. Oncol. Elsevier BV 2019, 30, v874–v875. [Google Scholar] [CrossRef]
- Bauer, U.; Mogler, C.; Braren, R.F.; Algül, H.; Schmid, R.M.; Ehmer, U. Progression after Immunotherapy for Fibrolamellar Carcinoma. Visc. Med. 2019, 35, 39–42. [Google Scholar] [CrossRef] [PubMed]
- De Toni, E.N.; Roessler, D. Using dual checkpoint blockade to treat fibrolamellar hepatocellular carcinoma. Gut 2020, 69, 2056–2058. [Google Scholar] [CrossRef] [PubMed]
- Abou-Alfa, G.K.; Meyer, T.; Zhang, J.; Sherrin, S.; Yaqubie, A.; O’Neill, A.C.; Xu, F.; Eli, L.D.; Harding, J.J.; O’Reilly, E.M.; et al. Evaluation of neratinib (N), pembrolizumab (P), everolimus (E), and nivolumab (V) in patients (pts) with fibrolamellar carcinoma (FLC). Am. Soc. Clin. Oncol. 2021, 39 (Suppl. 3), 310. [Google Scholar] [CrossRef]
- Kim, A.K.; Gani, F.; Layman, A.J.; Besharati, S.; Zhu, Q.; Succaria, F.; Engle, E.L.; Bhaijee, F.; Goggins, M.B.; Llosa, N.J.; et al. Multiple immune-suppressive mechanisms in fibrolamellar carcinoma. Cancer Immunol. Res. 2019, 7, 805–812. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| PD-L1 by IHC | TMB (Mutations/MB) | Sequencing Provider |
|---|---|---|
| Negative (<1%) | 2.6 | Tempus |
| Negative (<1%) | 4.2 | Tempus |
| Negative (<1%) | 1.1 | Tempus |
| Negative (<1%) | 6 | Caris |
| Negative (<1%) | 4 | Caris |
| Negative (<1%) | 6 | Caris |
| N/A | 1 | Strata |
| Negative (<1%) | 1 | Caris |
| Negative (<1%) | 1 | Caris |
| N/A | 0.5 | Tempus |
| Negative (<1%) | 4 | Caris |
| Negative (<1%) | 0 | Tempus |
| N/A | 0.5 | Tempus |
| Negative (<1%) | 4.7 | Tempus |
| Variable | Classification | Overall | Fibrolamellar Registry | Johns Hopkins & UT Southwestern |
|---|---|---|---|---|
| Number of Patients | 19 | 11 | 8 (6 JH, 2 UTSW) | |
| Age at Diagnosis (years) | Mean = 22.9 (SD = 6.1) | Mean = 20.7 (SD = 6.0) | Mean = 25.875 (SD = 5.1) | |
| Gender | Male | 12 (63.2%) | 7 (63.6%) | 5 (62.5%) |
| Female | 7 (36.8%) | 4 (36.4%) | 3 (37.5%) | |
| FLC Stage at Diagnosis | BCLC A | 3 (15.8%) | 3 (27.3%) | 0 (0%) |
| BCLC B | 4 (21.1%) | 3 (27.3%) | 1 (12.5%) | |
| BCLC C | 12 (63.2%) | 5 (45.5%) | 7 (87.5%) | |
| FLC Stage at ICI Treatment | BCLC A | 0 (0%) | 0 (0%) | 0 (0%) |
| BCLC B | 1 (5.3%) | 1 (9.1%) | 0 (0%) | |
| BCLC C | 18 (94.7%) | 10 (90.9%) | 8 (100%) | |
| Number of Patients Receiving Various Treatments | Prior Systemic Treatment | 15 (78.9%) | 9 (81.8%) | 6 (75.0%) |
| Prior Surgery | 13 (68.4%) | 7 (63.6%) | 6 (75.0%) | |
| Prior Local Radiation | 4 (21.1%) | 2 (18.2%) | 2 (25.0%) | |
| Number of Prior Systemic Treatments | Median = 1 (range 0–8) | Median = 2 (range 0–8) | Median = 1 (range 0–5) | |
| Prior Sorafenib | 9 (47.3%) | 9 (81.8%) | 0 (0%) | |
| Treatment Setting | Academic | 18 | 10 (90.9%) | 8 (100%) |
| Community | 1 | 1 (9.1%) | 0 (0%) |
| Variable | Classification | N (%) |
|---|---|---|
| Immune Checkpoint Inhibitor | Nivolumab monotherapy | 9 (47.4%) |
| Nivolumab + 5FU + IFN | 1 (5.9%) | |
| Nivolumab + regorafenib | 1 (5.9%) | |
| Nivolumab + gemcitabine-based chemotherapy | 1 (5.9%) | |
| Nivolumab + ipilimumab | 2 (11.8%) | |
| Pembrolizumab monotherapy | 4 (23.5%) | |
| Atezolizumab + bevacizumab | 1 (5.3%) | |
| Time on Therapy (months) | Median = 5.1 (range 0–36.5) | |
| Any ICI Regimen | Progressive Disease | 12 (63.2%) |
| Stable Disease | 4 (21.1%) | |
| Partial Response | 3 (15.8%) | |
| Complete Response | 0 (0%) | |
| ICI Alone Subset (i.e., anti-PD1 +/− CTLA4) | Progressive Disease | 10 (66.7%) |
| Stable Disease | 3 (20%) | |
| Partial Response | 2 (13.3%) | |
| Complete Response | 0 (0%) |
| Number of patients who discontinued ICIs due to AE | 2 (10.1%) |
| Any grade III or IV AE | 4 (21.1%) |
| Specific AE Data | |
| Elevated LFTs | 4 (21.1%) |
| Fatigue | 4 (21.1%) |
| Hypothyroidism | 2 (10.1%) |
| Nausea | 2 (10.1%) |
| Anaphylaxis | 1 (5.3%) |
| Diarrhea | 1 (5.3%) |
| Hyperthyroidism | 1 (5.3%) |
| Pneumonitis | 1 (5.3%) |
| Pruritis | 1 (5.3%) |
| Pyrexia | 1 (5.3%) |
| Rash | 1 (5.3%) |
| Vomiting | 1 (5.3%) |
| Average Number of AEs experienced by patients | 1.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, K.Y.; Popovic, A.; Hsiehchen, D.; Baretti, M.; Griffith, P.; Bista, R.; Baghdadi, A.; Kamel, I.R.; Simon, S.M.; Migler, R.D.; et al. Clinical Outcomes in Fibrolamellar Hepatocellular Carcinoma Treated with Immune Checkpoint Inhibitors. Cancers 2022, 14, 5347. https://doi.org/10.3390/cancers14215347
Chen KY, Popovic A, Hsiehchen D, Baretti M, Griffith P, Bista R, Baghdadi A, Kamel IR, Simon SM, Migler RD, et al. Clinical Outcomes in Fibrolamellar Hepatocellular Carcinoma Treated with Immune Checkpoint Inhibitors. Cancers. 2022; 14(21):5347. https://doi.org/10.3390/cancers14215347
Chicago/Turabian StyleChen, Krista Y., Aleksandra Popovic, David Hsiehchen, Marina Baretti, Paige Griffith, Ranjan Bista, Azarakhsh Baghdadi, Ihab R. Kamel, Sanford M. Simon, Rachael D. Migler, and et al. 2022. "Clinical Outcomes in Fibrolamellar Hepatocellular Carcinoma Treated with Immune Checkpoint Inhibitors" Cancers 14, no. 21: 5347. https://doi.org/10.3390/cancers14215347
APA StyleChen, K. Y., Popovic, A., Hsiehchen, D., Baretti, M., Griffith, P., Bista, R., Baghdadi, A., Kamel, I. R., Simon, S. M., Migler, R. D., & Yarchoan, M. (2022). Clinical Outcomes in Fibrolamellar Hepatocellular Carcinoma Treated with Immune Checkpoint Inhibitors. Cancers, 14(21), 5347. https://doi.org/10.3390/cancers14215347