

Predictive Power of MIB-1 vs. Mitotic Count on Progression-Free Survival in Skull-Base Meningioma

 , ,
, , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
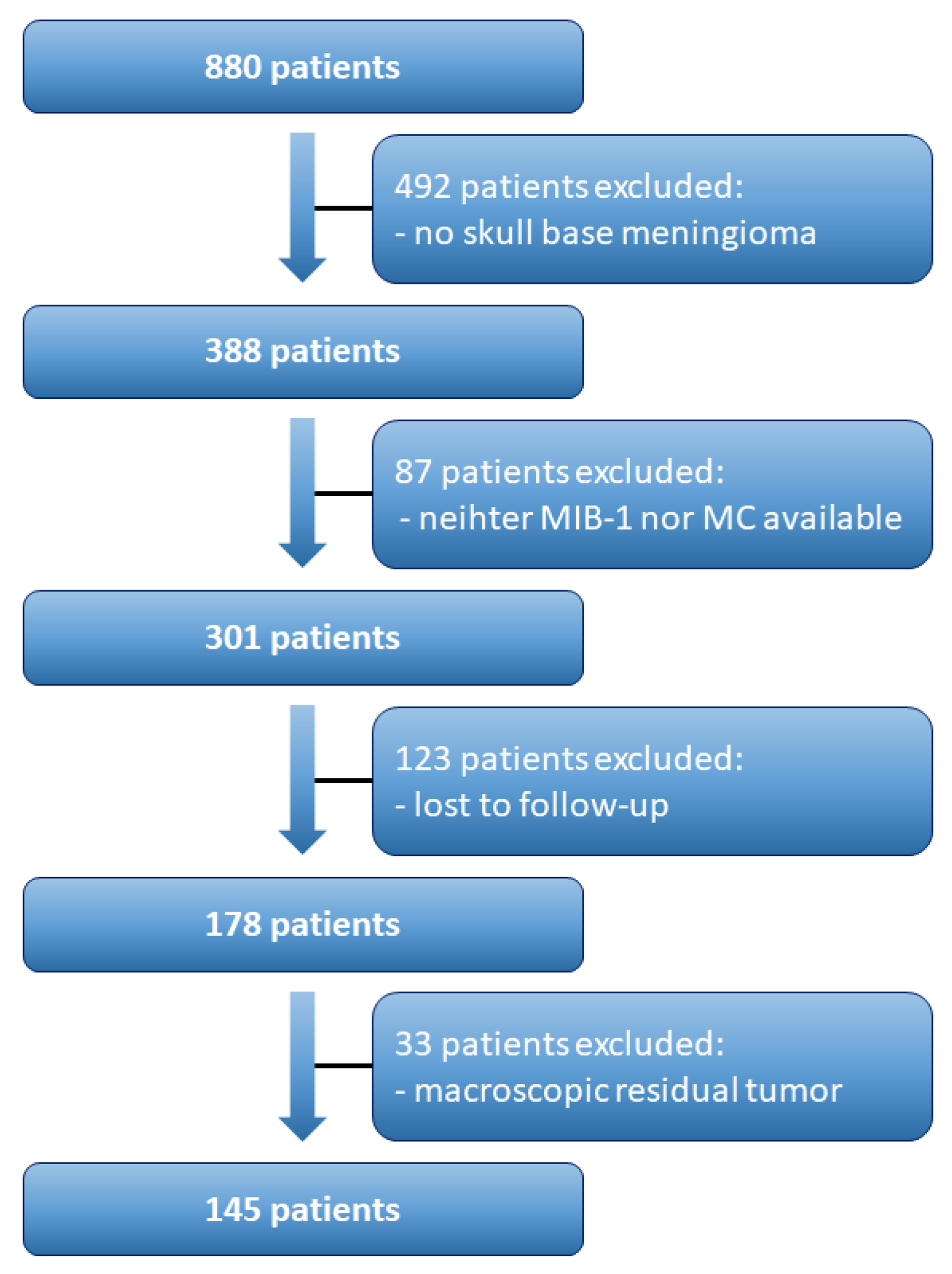
2.1. Study Design and Patient Characteristics
2.2. Data Recording
2.3. Histopathology
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
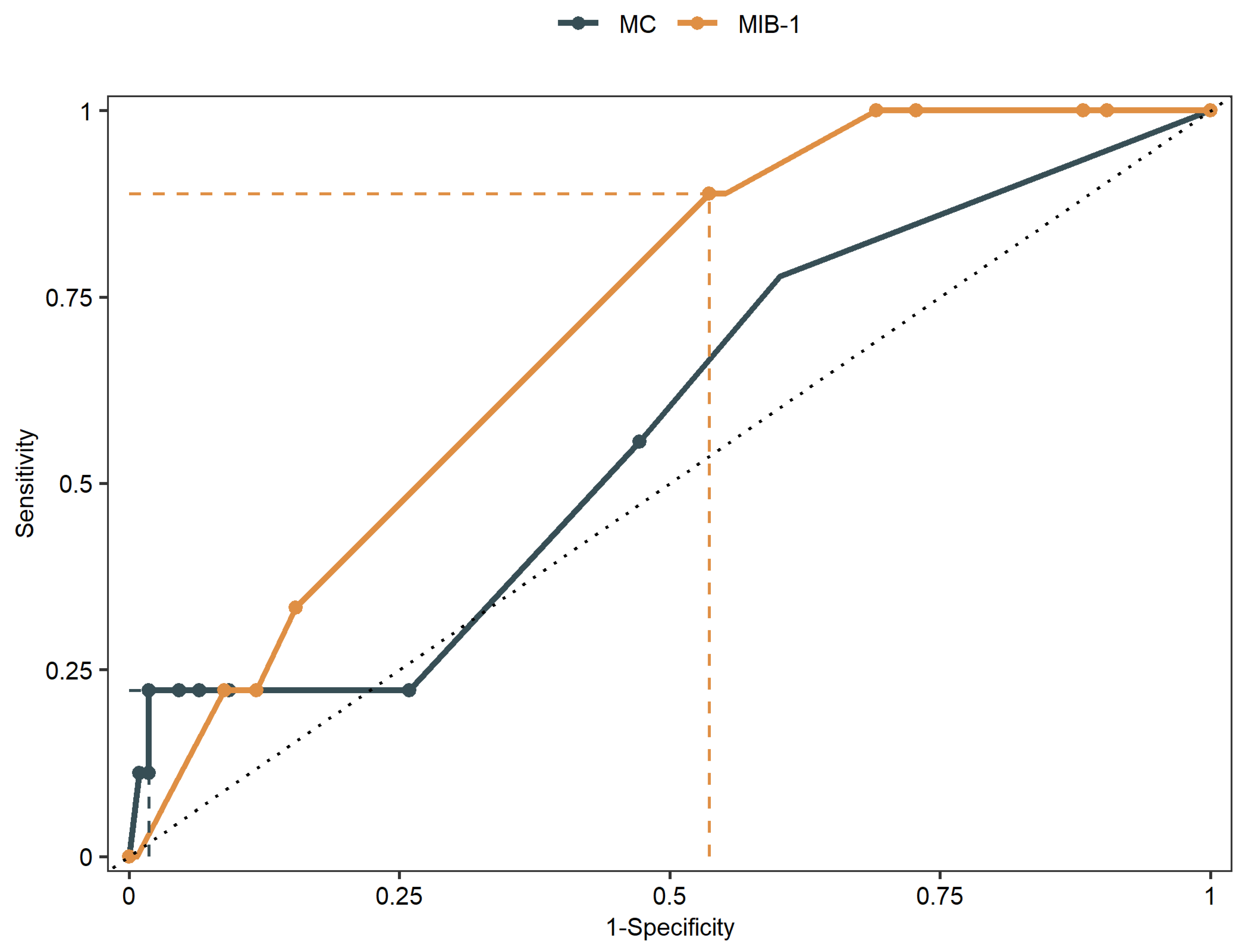
3.2. MIB-1 Labeling Index and Mitotic Count in Prediction of Recurrence of Skull-Base Meningioma
3.3. Time-Dependent Analysis of MIB-1 Labeling Index and Mitotic Count in Prediction of Recurrence of Skull-Base Meningioma
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef]
- Pettersson-Segerlind, J.; Orrego, A.; Lönn, S.; Mathiesen, T. Long-term 25-year follow-up of surgically treated parasagittal meningiomas. World Neurosurg. 2011, 76, 564–571. [Google Scholar] [CrossRef]
- Alexiou, G.A.; Gogou, P.; Markoula, S.; Kyritsis, A.P. Management of meningiomas. Clin. Neurol. Neurosurg. 2010, 112, 177–182. [Google Scholar] [CrossRef]
- van Diest, P.J.; Brugal, G.; Baak, J.P. Proliferation markers in tumours: Interpretation and clinical value. J. Clin. Pathol. 1998, 51, 716–724. [Google Scholar] [CrossRef]
- Olar, A.; Wani, K.M.; Sulman, E.P.; Mansouri, A.; Zadeh, G.; Wilson, C.D.; DeMonte, F.; Fuller, G.N.; Aldape, K.D. Mitotic Index is an Independent Predictor of Recurrence-Free Survival in Meningioma. Brain Pathol. 2015, 25, 266–275. [Google Scholar] [CrossRef]
- Oya, S.; Kawai, K.; Nakatomi, H.; Saito, N. Significance of Simpson grading system in modern meningioma surgery: Integration of the grade with MIB-1 labeling index as a key to predict the recurrence of WHO Grade I meningiomas. J. Neurosurg. 2012, 117, 121–128. [Google Scholar] [CrossRef]
- Vranic, A.; Popovic, M.; Cör, A.; Prestor, B.; Pizem, J. Mitotic count, brain invasion, and location are independent predictors of recurrence-free survival in primary atypical and malignant meningiomas: A study of 86 patients. Neurosurgery 2010, 67, 1124–1132. [Google Scholar] [CrossRef]
- Liu, N.; Song, S.-Y.; Jiang, J.-B.; Wang, T.-J.; Yan, C.-X. The prognostic role of Ki-67/MIB-1 in meningioma: A systematic review with meta-analysis. Medicine 2020, 99, e18644. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, K.H.; Lee, E.H.; Lee, Y.M.; Lee, S.-H.; Kim, H.D.; Kim, Y.Z. Results of immunohistochemical staining for cell cycle regulators predict the recurrence of atypical meningiomas. J. Neurosurg. 2014, 121, 1189–1200. [Google Scholar] [CrossRef]
- Maiuri, F.; Mariniello, G.; Guadagno, E.; Barbato, M.; Corvino, S.; Del Basso De Caro, M. WHO grade, proliferation index, and progesterone receptor expression are different according to the location of meningioma. Acta Neurochir. 2019, 161, 2553–2561. [Google Scholar] [CrossRef]
- Antinheimo, J.; Haapasalo, H.; Haltia, M.; Tatagiba, M.; Thomas, S.; Brandis, A.; Sainio, M.; Carpen, O.; Samii, M.; Jääskeläinen, J. Proliferation potential and histological features in neurofibromatosis 2-associated and sporadic meningiomas. J. Neurosurg. 1997, 87, 610–614. [Google Scholar] [CrossRef] [PubMed]
- Coons, S.W.; Johnson, P.C. Regional heterogeneity in the proliferative activity of human gliomas as measured by the Ki-67 labeling index. J. Neuropathol. Exp. Neurol. 1993, 52, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Landriel Ibañez, F.A.; Hem, S.; Ajler, P.; Vecchi, E.; Ciraolo, C.; Baccanelli, M.; Tramontano, R.; Knezevich, F.; Carrizo, A. A new classification of complications in neurosurgery. World Neurosurg. 2011, 75, 709–715; discussion 604-11. [Google Scholar] [CrossRef] [PubMed]
- Goldbrunner, R.; Minniti, G.; Preusser, M.; Jenkinson, M.D.; Sallabanda, K.; Houdart, E.; von Deimling, A.; Stavrinou, P.; Lefranc, F.; Lund-Johansen, M.; et al. EANO guidelines for the diagnosis and treatment of meningiomas. Lancet Oncol. 2016, 17, e383–e391. [Google Scholar] [CrossRef]
- Wach, J.; Lampmann, T.; Güresir, Á.; Vatter, H.; Becker, A.J.; Hölzel, M.; Toma, M.; Güresir, E. Combining FORGE Score and Histopathological Diagnostic Criteria of Atypical Meningioma Enables Risk Stratification of Tumor Progression. Diagnostics 2021, 11, 2011. [Google Scholar] [CrossRef]
- Wach, J.; Lampmann, T.; Güresir, Á.; Schuss, P.; Vatter, H.; Herrlinger, U.; Becker, A.; Hölzel, M.; Toma, M.; Güresir, E. FORGE: A Novel Scoring System to Predict the MIB-1 Labeling Index in Intracranial Meningiomas. Cancers 2021, 13, 3643. [Google Scholar] [CrossRef]
- Schneider, M.; Borger, V.; Güresir, Á.; Becker, A.; Vatter, H.; Schuss, P.; Güresir, E. High Mib-1-score correlates with new cranial nerve deficits after surgery for frontal skull base meningioma. Neurosurg. Rev. 2021, 44, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Majores, M.; Schick, V.; Engels, G.; Fassunke, J.; Elger, C.E.; Schramm, J.; Blümcke, I.; Becker, A.J. Mutational and immunohistochemical analysis of ezrin-, radixin-, moesin (ERM) molecules in epilepsy-associated glioneuronal lesions. Acta Neuropathol. 2005, 110, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Majores, M.; von Lehe, M.; Fassunke, J.; Schramm, J.; Becker, A.J.; Simon, M. Tumor recurrence and malignant progression of gangliogliomas. Cancer 2008, 113, 3355–3363. [Google Scholar] [CrossRef]
- Lemée, J.-M.; Corniola, M.V.; Meling, T.R. Benefits of re-do surgery for recurrent intracranial meningiomas. Sci. Rep. 2020, 10, 303. [Google Scholar] [CrossRef] [PubMed]
- Wach, J.; Güresir, Á.; Borger, V.; Schuss, P.; Becker, A.; Coch, C.; Schmitz, M.-T.; Hölzel, M.; Toma, M.; Herrlinger, U.; et al. Elevated baseline C-reactive protein levels predict poor progression-free survival in sporadic vestibular schwannoma. J. Neurooncol. 2022, 156, 365–375. [Google Scholar] [CrossRef]
- Heagerty, P.J.; Lumley, T.; Pepe, M.S. Time-dependent ROC curves for censored survival data and a diagnostic marker. Biometrics 2000, 56, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Mirian, C.; Skyrman, S.; Bartek, J.; Jensen, L.R.; Kihlström, L.; Förander, P.; Orrego, A.; Mathiesen, T. The Ki-67 Proliferation Index as a Marker of Time to Recurrence in Intracranial Meningioma. Neurosurgery 2020, 87, 1289–1298. [Google Scholar] [CrossRef] [PubMed]
- Gerdes, J.; Lemke, H.; Baisch, H.; Wacker, H.H.; Schwab, U.; Stein, H. Cell cycle analysis of a cell proliferation-associated human nuclear antigen defined by the monoclonal antibody Ki-67. J. Immunol. 1984, 133, 1710–1715. [Google Scholar]
- Robertson, S.; Acs, B.; Lippert, M.; Hartman, J. Prognostic potential of automated Ki67 evaluation in breast cancer: Different hot spot definitions versus true global score. Breast Cancer Res. Treat. 2020, 183, 161–175. [Google Scholar] [CrossRef]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.-J. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef]
- Duregon, E.; Cassenti, A.; Pittaro, A.; Ventura, L.; Senetta, R.; Rudà, R.; Cassoni, P. Better see to better agree: Phosphohistone H3 increases interobserver agreement in mitotic count for meningioma grading and imposes new specific thresholds. Neuro Oncol. 2015, 17, 663–669. [Google Scholar] [CrossRef]
- Meling, T.R.; Da Broi, M.; Scheie, D.; Helseth, E. Meningiomas: Skull base versus non-skull base. Neurosurg. Rev. 2019, 42, 163–173. [Google Scholar] [CrossRef]
- Wach, J.; Lampmann, T.; Güresir, Á.; Vatter, H.; Herrlinger, U.; Becker, A.; Cases-Cunillera, S.; Hölzel, M.; Toma, M.; Güresir, E. Proliferative Potential, and Inflammatory Tumor Microenvironment in Meningioma Correlate with Neurological Function at Presentation and Anatomical Location-From Convexity to Skull Base and Spine. Cancers 2022, 14, 1033. [Google Scholar] [CrossRef]
- Haddad, A.F.; Young, J.S.; Kanungo, I.; Sudhir, S.; Chen, J.-S.; Raleigh, D.R.; Magill, S.T.; McDermott, M.W.; Aghi, M.K. WHO Grade I Meningioma Recurrence: Identifying High Risk Patients Using Histopathological Features and the MIB-1 Index. Front. Oncol. 2020, 10, 1522. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean Age (±SD) [in Years] | 59.9 ± 13.2 |
|---|---|
| Sex | |
| Female | 105 (72.4%) |
| Male | 40 (27.6%) |
| Mean preoperative KPS (±SD) | 90.9 ± 11.0 |
| WHO grade | |
| 1 | 126 (86.9%) |
| 2 | 19 (13.1%) |
| Tumor location | |
| Medial skull-base | 44 (30.3%) |
| Lateral skull-base | 71 (49%) |
| Occipital fossa | 30 (20.7) |
| Multiple meningiomas | 8 (5.5%) |
| Sinus invasion | 27 (18.6%) |
| Peritumoral edema | 73 (50.3%) |
| Simpson grade | |
| Simpson grade I & II | 135 (93.1%) |
| Simpson grade III | 10 (6.9%) |
| Availability of | |
| MIB-1 | 145 |
| MC | 117 |
| Mean MIB-1 (±SD) (in %) | 4.9 ± 2.3 |
| WHO grade 1 | 4.8 ± 2.2 |
| WHO grade 2 | 5.4 ± 2.5 |
| High MC (≥4) | 9/117 (7.7%) |
| WHO grade 1 | 5/102 (4.9%) |
| WHO grade 2 | 4/15 (26.7%) |
| Mean MC (±SD) | 1.3 ± 2.2 |
| WHO grade 1 | 1.0 ± 1.6 |
| WHO grade 2 | 3.0 ± 4.4 |
| Mean Follow-Up (±SD) (in weeks) | 116 ± 106 |
| recurrence rate | 9/145 (6.2%) |
| WHO grade 1 | 7/126 (5.6%) |
| WHO grade 2 | 2/19 (10.5%) |
| Landriel Ibañez Classification | |
| None | 114 (78.6%) |
| Grade I a | 2 (1.4%) |
| Grade I b | 10 (6.9%) |
| Grade II a | 1 (0.7%) |
| Grade II b | 9 (6.2%) |
| Grade III a | 5 (3.4%) |
| Grade III b | 4 (2.8%) |
| Grade IV | 0 (0%) |
| PFS (weeks) | AUC | |
|---|---|---|
| MIB-1 | MC | |
| 49 | 0.61 | 0.61 |
| 50 | 0.60 | 0.63 |
| 52 | 0.61 | 0.59 |
| 73 | 0.61 | 0.61 |
| 81 | 0.60 | 0.58 |
| 92 | 0.61 | 0.58 |
| 97 | 0.61 | 0.58 |
| 132 | 0.60 | 0.60 |
| 183 | 0.64 | 0.63 |
| C-index | 0.61 | 0.60 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lampmann, T.; Wach, J.; Schmitz, M.-T.; Güresir, Á.; Vatter, H.; Güresir, E. Predictive Power of MIB-1 vs. Mitotic Count on Progression-Free Survival in Skull-Base Meningioma. Cancers 2022, 14, 4597. https://doi.org/10.3390/cancers14194597
Lampmann T, Wach J, Schmitz M-T, Güresir Á, Vatter H, Güresir E. Predictive Power of MIB-1 vs. Mitotic Count on Progression-Free Survival in Skull-Base Meningioma. Cancers. 2022; 14(19):4597. https://doi.org/10.3390/cancers14194597
Chicago/Turabian StyleLampmann, Tim, Johannes Wach, Marie-Therese Schmitz, Ági Güresir, Hartmut Vatter, and Erdem Güresir. 2022. "Predictive Power of MIB-1 vs. Mitotic Count on Progression-Free Survival in Skull-Base Meningioma" Cancers 14, no. 19: 4597. https://doi.org/10.3390/cancers14194597
APA StyleLampmann, T., Wach, J., Schmitz, M.-T., Güresir, Á., Vatter, H., & Güresir, E. (2022). Predictive Power of MIB-1 vs. Mitotic Count on Progression-Free Survival in Skull-Base Meningioma. Cancers, 14(19), 4597. https://doi.org/10.3390/cancers14194597