
Neoadjuvant Stereotactic Radiotherapy for Brain Metastases: Systematic Review and Meta-Analysis of the Literature and Ongoing Clinical Trials
 ,
,  ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Data Synthesis and Quality Assessment
2.5. Statistical Analysis
3. Results
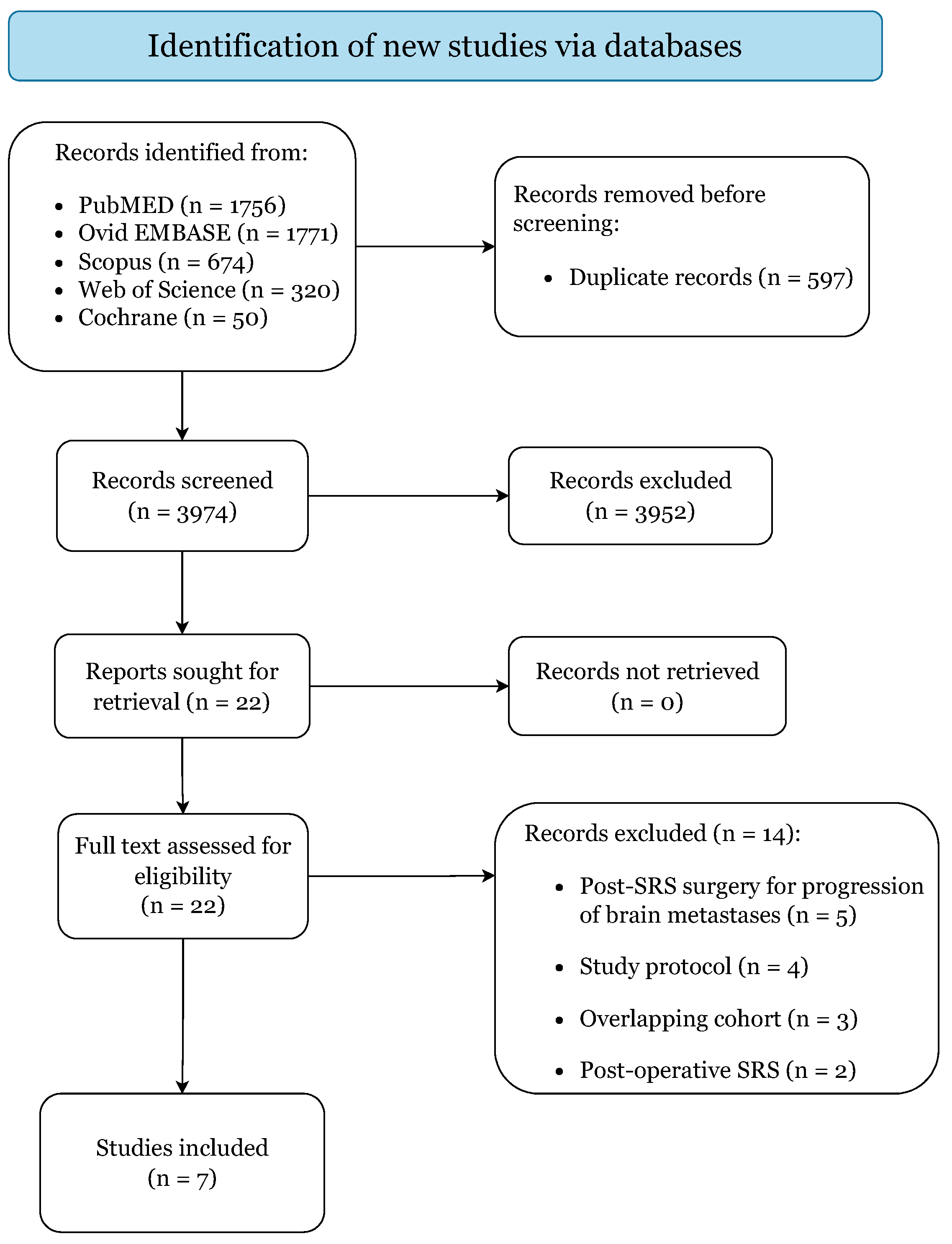
3.1. Study Selection
3.2. Demographics and Clinical Features
3.3. Patient Eligibility and Treatment Protocols
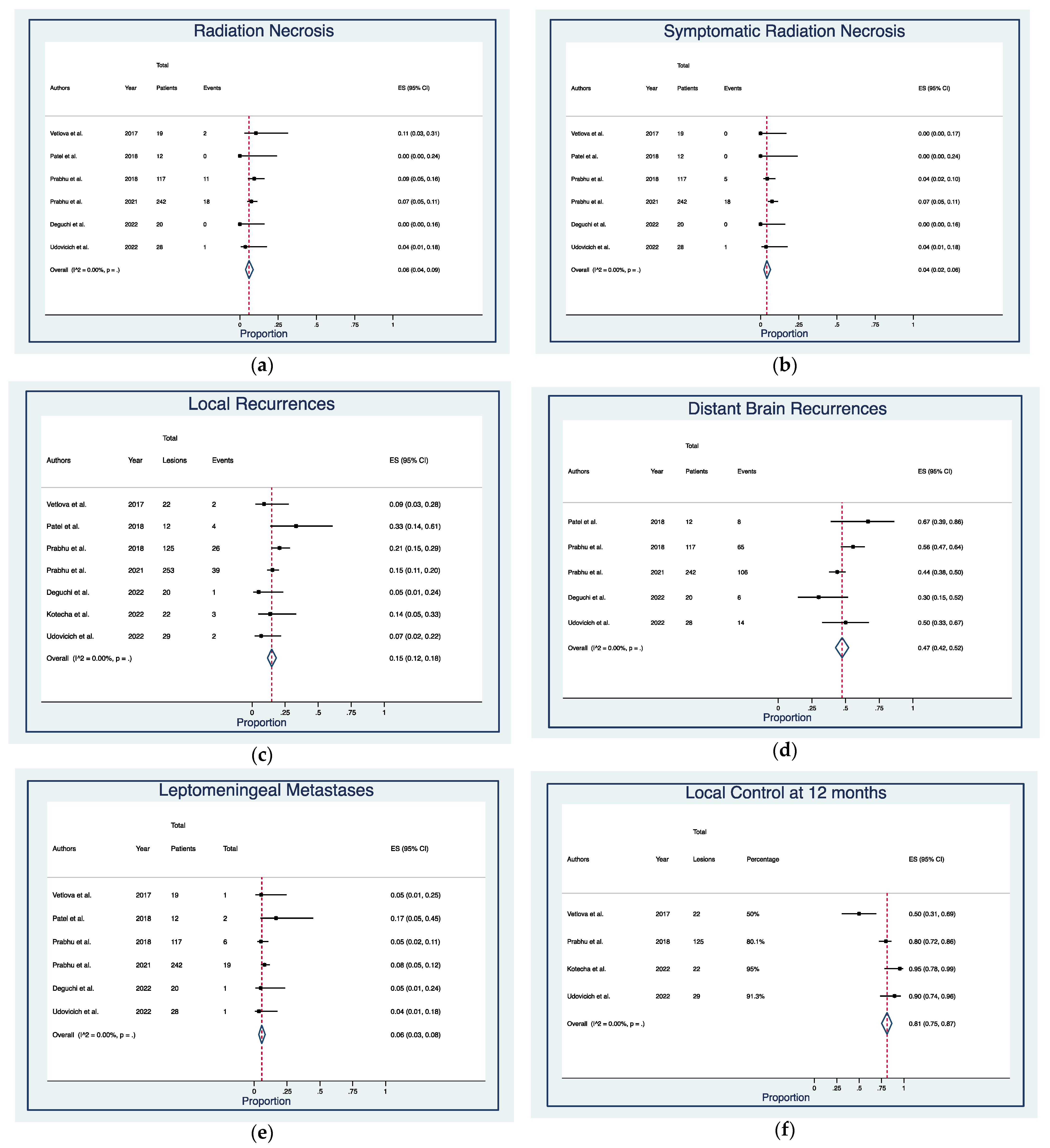
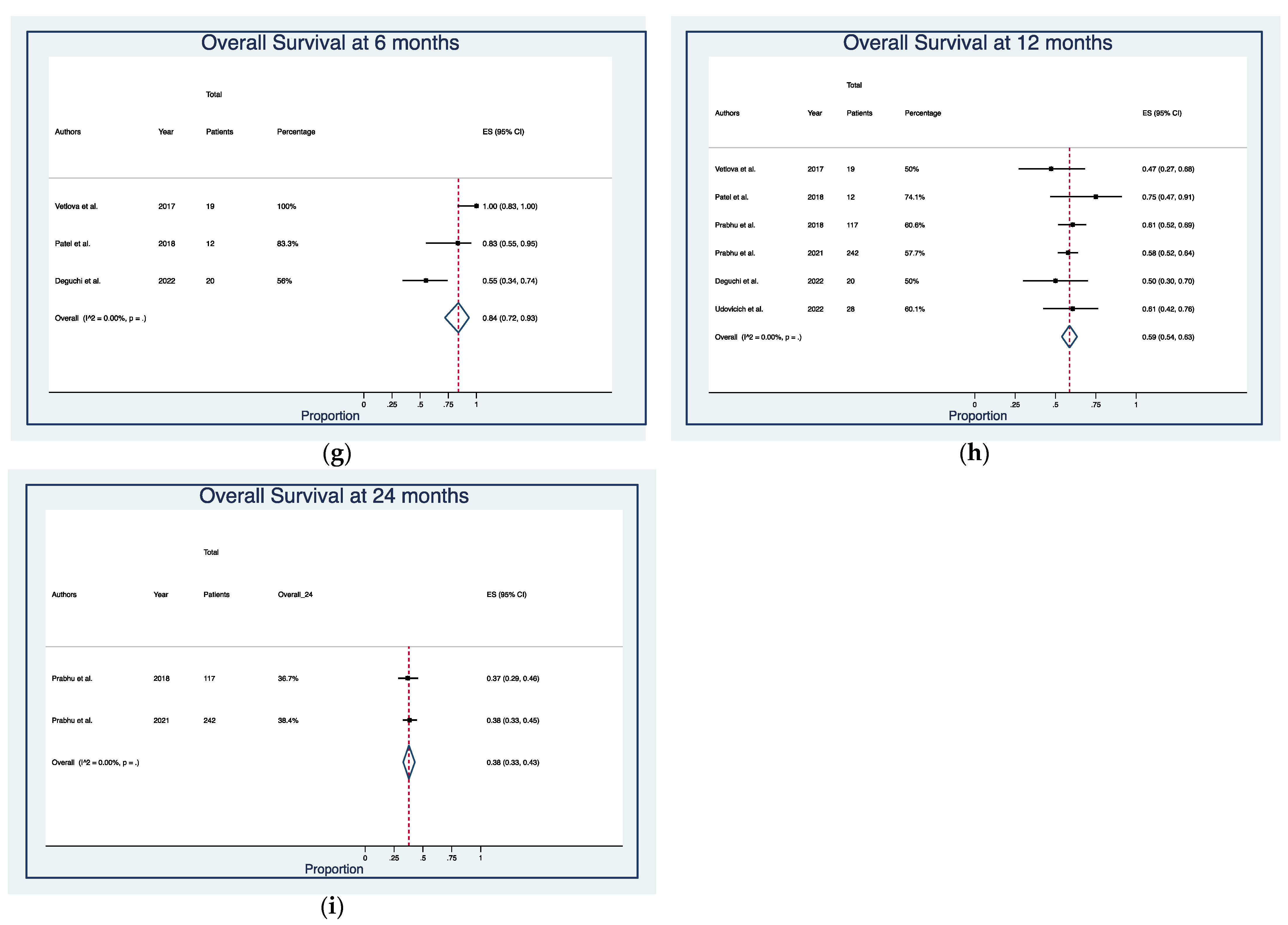
3.4. Outcomes, Complications, and Survival
3.5. Ongoing Clinical Trials: Eligibility Criteria, Protocols, and Outcome Measures
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Nayak, L.; Lee, E.Q.; Wen, P.Y. Epidemiology of Brain Metastases. Curr. Oncol. Rep. 2012, 14, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Barnholtz-Sloan, J.S.; Sloan, A.E.; Davis, F.G.; Vigneau, F.D.; Lai, P.; Sawaya, R.E. Incidence Proportions of Brain Metastases in Patients Diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J. Clin. Oncol. 2004, 22, 2865–2872. [Google Scholar] [CrossRef] [PubMed]
- Steeg, P.S.; Camphausen, K.A.; Smith, Q.R. Brain metastases as preventive and therapeutic targets. Nat. Rev. Cancer 2011, 11, 352–363. [Google Scholar] [CrossRef] [PubMed]
- Owonikoko, T.K.; Arbiser, J.; Zelnak, A.; Shu, H.-K.G.; Shim, H.; Robin, A.M.; Kalkanis, S.N.; Whitsett, T.G.; Salhia, B.; Tran, N.L.; et al. Current approaches to the treatment of metastatic brain tumours. Nat. Rev. Clin. Oncol. 2014, 11, 203–222. [Google Scholar] [CrossRef]
- Achrol, A.S.; Rennert, R.C.; Anders, C.; Soffietti, R.; Ahluwalia, M.S.; Nayak, L.; Peters, S.; Arvold, N.D.; Harsh, G.R.; Steeg, P.S.; et al. Brain metastases. Nat. Rev. Dis. Prim. 2019, 5, 5. [Google Scholar] [CrossRef]
- Patchell, R.A.; Tibbs, P.A.; Regine, W.F.; Dempsey, R.J.; Mohiuddin, M.; Kryscio, R.J.; Markesbery, W.R.; Foon, K.A.; Young, B. Postoperative Radiotherapy in the Treatment of Single Metastases to the Brain. JAMA 1998, 280, 1485–1489. [Google Scholar] [CrossRef]
- Brennan, C.; Yang, T.J.; Hilden, P.; Zhang, Z.; Chan, K.; Yamada, Y.; Chan, T.A.; Lymberis, S.C.; Narayana, A.; Tabar, V.; et al. A Phase 2 Trial of Stereotactic Radiosurgery Boost after Surgical Resection for Brain Metastases. Int. J. Radiat. Oncol. 2014, 88, 130–136. [Google Scholar] [CrossRef]
- Brown, P.D.; Ballman, K.V.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Whitton, A.C.; Greenspoon, J.; Parney, I.F.; Laack, N.N.I.; Ashman, J.B.; et al. Postoperative stereotactic radiosurgery compared with whole brain radiotherapy for resected metastatic brain disease (NCCTG N107C/CEC·3): A multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1049–1060. [Google Scholar] [CrossRef]
- Mahajan, A.; Ahmed, S.; McAleer, M.F.; Weinberg, J.S.; Li, J.; Brown, P.; Settle, S.; Prabhu, S.S.; Lang, F.F.; Levine, N.; et al. Post-operative stereotactic radiosurgery versus observation for completely resected brain metastases: A single-centre, randomised, controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1040–1048. [Google Scholar] [CrossRef]
- Rahimy, E.; Dudley, S.A.; von Eyben, R.; Pollom, E.L.; Seiger, K.; Modlin, L.; Wynne, J.; Fujimoto, D.; Jacobs, L.R.; Chang, S.D.; et al. Phase I/II Dose-Escalation Trial of 3-Fraction Stereotactic Radiosurgery for Resection Cavities from Large Brain Metastases. Am. J. Clin. Oncol. 2021, 44, 588–595. [Google Scholar] [CrossRef]
- Brown, P.D.; Jaeckle, K.; Ballman, K.V.; Farace, E.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Barker, F.G.; Deming, R.; Burri, S.H.; et al. Effect of Radiosurgery Alone vs Radiosurgery with Whole Brain Radiation Therapy on Cognitive Function in Patients with 1 to 3 Brain Metastases. JAMA 2016, 316, 401. [Google Scholar] [CrossRef]
- Asher, A.L.; Burri, S.H.; Wiggins, W.F.; Kelly, R.P.; Boltes, M.O.; Mehrlich, M.; Norton, H.J.; Fraser, R.W. A New Treatment Paradigm: Neoadjuvant Radiosurgery Before Surgical Resection of Brain Metastases with Analysis of Local Tumor Recurrence. Int. J. Radiat. Oncol. 2014, 88, 899–906. [Google Scholar] [CrossRef]
- Patel, K.R.; Burri, S.H.; Asher, A.L.; Crocker, I.R.; Fraser, R.W.; Zhang, C.; Chen, Z.; Kandula, S.; Zhong, J.; Press, R.H.; et al. Comparing Preoperative with Postoperative Stereotactic Radiosurgery for Resectable Brain Metastases. Neurosurgery 2016, 79, 279–285. [Google Scholar] [CrossRef]
- Prabhu, R.S.; Patel, K.R.; Press, R.H.; Soltys, S.G.; Brown, P.D.; Mehta, M.P.; Asher, A.L.; Burri, S.H. Preoperative Vs Postoperative Radiosurgery for Resected Brain Metastases: A Review. Neurosurgery 2019, 84, 19–29. [Google Scholar] [CrossRef]
- Udovicich, C.; Phillips, C.; Kok, D.L.; Tange, D.; Plumridge, N.M.; Prabhu, R.S.; Haghighi, N. Neoadjuvant Stereotactic Radiosurgery: A Further Evolution in the Management of Brain Metastases. Curr. Oncol. Rep. 2019, 21, 73. [Google Scholar] [CrossRef]
- Routman, D.M.; Yan, E.; Vora, S.; Peterson, J.; Mahajan, A.; Chaichana, K.L.; Laack, N.; Brown, P.D.; Parney, I.F.; Burns, T.C.; et al. Preoperative Stereotactic Radiosurgery for Brain Metastases. Front. Neurol. 2018, 9, 959. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Jones, B.; Dale, R.G.; Deehan, C.; Hopkins, K.I.; Morgan, D.A.L. The Role of Biologically Effective Dose (BED) in Clinical Oncology. Clin. Oncol. 2001, 13, 71–81. [Google Scholar] [CrossRef]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H. Explanation of the 2011 Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence (Background Document). Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 30 April 2022).
- Joanna Briggs Institute Checklist for Case Series. Available online: https://jbi.global/critical-appraisal-tools (accessed on 30 April 2022).
- Wilson, E.B. Probable Inference, the Law of Succession, and Statistical Inference. J. Am. Stat. Assoc. 1927, 22, 209–212. [Google Scholar] [CrossRef]
- Freeman, M.F.; Tukey, J.W. Transformations Related to the Angular and the Square Root. Ann. Math. Stat. 1950, 21, 607–611. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Vetlova, E.; Golbin, D.A.; Golanov, A.V.; Potapov, A.A.; Banov, S.M.; Antipina, N.; Kostjuchenko, V.V.; Usachev, D.Y.; Belyaev, A.Y.; Goryaynov, S. Preoperative Stereotactic Radiosurgery of Brain Metastases: Preliminary Results. Cureus 2017, 9, e1987. [Google Scholar] [CrossRef]
- Patel, A.R.; Nedzi, L.; Lau, S.; Barnett, S.L.; Mickey, B.E.; Moore, W.; Bindal, S.; Wardak, Z.; Dan, T.; Timmerman, R.; et al. Neoadjuvant Stereotactic Radiosurgery before Surgical Resection of Cerebral Metastases. World Neurosurg. 2018, 120, e480–e487. [Google Scholar] [CrossRef]
- Prabhu, R.S.; Miller, K.R.; Asher, A.L.; Heinzerling, J.H.; Moeller, B.J.; Lankford, S.P.; McCammon, R.J.; Fasola, C.E.; Patel, K.R.; Press, R.H.; et al. Preoperative stereotactic radiosurgery before planned resection of brain metastases: Updated analysis of efficacy and toxicity of a novel treatment paradigm. J. Neurosurg. 2019, 131, 1387–1394. [Google Scholar] [CrossRef]
- Prabhu, R.S.; Dhakal, R.; Vaslow, Z.K.; Dan, T.; Mishra, M.V.; Murphy, E.S.; Patel, T.R.; Asher, A.L.; Yang, K.; Manning, M.A.; et al. Preoperative Radiosurgery for Resected Brain Metastases: The PROPS-BM Multicenter Cohort Study. Int. J. Radiat. Oncol. 2021, 111, 764–772. [Google Scholar] [CrossRef]
- Deguchi, S.; Mitsuya, K.; Yasui, K.; Kimura, K.; Onoe, T.; Ogawa, H.; Asakura, H.; Harada, H.; Hayashi, N. Neoadjuvant fractionated stereotactic radiotherapy followed by piecemeal resection of brain metastasis: A case series of 20 patients. Int. J. Clin. Oncol. 2022, 27, 481–487. [Google Scholar] [CrossRef]
- Kotecha, R.; Tonse, R.; Menendez, M.A.R.; Williams, A.; Diaz, Z.; Tom, M.C.; Hall, M.D.; Mehta, M.P.; Alvarez, R.; Siomin, V.; et al. Evaluation of the impact of pre-operative stereotactic radiotherapy on the acute changes in histopathologic and immune marker profiles of brain metastases. Sci. Rep. 2022, 12, 4567. [Google Scholar] [CrossRef]
- Udovicich, C.; Ng, S.P.; Tange, D.; Bailey, N.; Haghighi, N. From Postoperative to Preoperative: A Case Series of Hypofractionated and Single-Fraction Neoadjuvant Stereotactic Radiosurgery for Brain Metastases. Oper. Neurosurg. 2022, 22, 208–214. [Google Scholar] [CrossRef]
- Patel, K.R.; Burri, S.H.; Boselli, D.; Symanowski, J.T.; Asher, A.L.; Sumrall, A.; Fraser, R.W.; Press, R.H.; Zhong, J.; Cassidy, R.J.; et al. Comparing pre-operative stereotactic radiosurgery (SRS) to post-operative whole brain radiation therapy (WBRT) for resectable brain metastases: A multi-institutional analysis. J. Neurooncol. 2017, 131, 611–618. [Google Scholar] [CrossRef]
- Prabhu, R.S.; Press, R.H.; Patel, K.R.; Boselli, D.M.; Symanowski, J.T.; Lankford, S.P.; McCammon, R.J.; Moeller, B.J.; Heinzerling, J.H.; Fasola, C.E.; et al. Single-Fraction Stereotactic Radiosurgery (SRS) Alone versus Surgical Resection and SRS for Large Brain Metastases: A Multi-institutional Analysis. Int. J. Radiat. Oncol. 2017, 99, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S. A Multicenter Prospective, Interventional, Randomized Trial of Preoperative Radiosurgery Compared with Postoperative Stereotactic Radiotherapy for Resectable Brain Metastases (NCT05124236). Available online: https://clinicaltrials.gov/ct2/show/NCT05124236 (accessed on 30 April 2022).
- Brun, L. Phase II Study to Assess Preoperative Hypofractionated Stereotactic Radiotherapy of Brain Metastases (NCT04503772). Available online: https://clinicaltrials.gov/ct2/show/NCT04503772 (accessed on 30 April 2022).
- Faruqi, M.; Patel, S. A Randomized Controlled Trial of Pre-operative versus Post-Operative Stereotactic Radiosurgery for Patients with Surgically Resectable Brain Metastases (NCT04474925). Available online: https://clinicaltrials.gov/ct2/show/NCT04474925 (accessed on 30 April 2022).
- Yeboa, D.N. A Phase III Trial of Pre-Operative Stereotactic Radiosurgery (SRS) versus Post-Operative SRS for Brain Metastases (NCT03741673). Available online: https://clinicaltrials.gov/ct2/show/NCT03741673 (accessed on 30 April 2022).
- Wu, M. Pre-operative Hypofractionated Stereotactic Radiosurgery for Resectable Brain Metastases (NCT05267587). Available online: https://clinicaltrials.gov/ct2/show/NCT05267587 (accessed on 30 April 2022).
- Bovi, J. A Pilot Study Analyzing Preoperative Stereotactic Radiosurgery (SRS) with Gamma Knife (GK) for Brain Metastases (NCT04545814). Available online: https://clinicaltrials.gov/ct2/show/NCT04545814 (accessed on 30 April 2022).
- Agrawal, N. A Phase II Study Analyzing Pre-Operative Stereotactic Radiosurgery Followed by Resection for Patients with 1–4 Brain Metastases (NCT03398694). Available online: https://clinicaltrials.gov/ct2/show/NCT03398694 (accessed on 30 April 2022).
- Shultz, D. Patients with Resectable Brain Mets Will Receive Neoadjuvant Stereotactic Radiosurgery Prior to Surgical Resection (NCT03368625). Available online: https://clinicaltrials.gov/ct2/show/NCT03368625 (accessed on 30 April 2022).
- Shiao, S. A Phase 1 Dose Escalation Trial of Neoadjuvant Radiosurgery for the Treatment of Metastatic Brain Tumors (NCT03163368). Available online: https://clinicaltrials.gov/ct2/show/NCT03163368 (accessed on 30 April 2022).
- Clump, D. Phase II Study Determining the Efficacy of Pre-Operative Stereotactic Radiosurgery Followed by Resection for Brain Metastases (NCT02514915). Available online: https://clinicaltrials.gov/ct2/show/NCT02514915 (accessed on 30 April 2022).
- Buchwald, Z. Preoperative Radiosurgery for Brain Metastases Planned for Surgical Resection: A Two Arm Pilot Study (NCT04895592). Available online: https://clinicaltrials.gov/ct2/show/NCT04895592 (accessed on 30 April 2022).
- Murphy, E. Neoadjuvant Radiosurgery for Resectable Brain Metastases: Phase I/II Study (NCT01891318). Available online: https://clinicaltrials.gov/ct2/show/NCT01891318 (accessed on 30 April 2022).
- Yan, E. Pre-Operative vs. Post-Operative Stereotactic Radiosurgery for Operative Metastatic Brain Tumors (NCT03750227). Available online: https://clinicaltrials.gov/ct2/show/NCT03750227 (accessed on 30 April 2022).
- Borgelt, B.; Gelber, R.; Kramer, S.; Brady, L.W.; Chang, C.H.; Davis, L.W.; Perez, C.A.; Hendrickson, F.R. The palliation of brain metastases: Final results of the first two studies by the radiation therapy oncology group. Int. J. Radiat. Oncol. 1980, 6, 1–9. [Google Scholar] [CrossRef]
- Bindal, R.K.; Sawaya, R.; Leavens, M.E.; Lee, J.J. Surgical treatment of multiple brain metastases. J. Neurosurg. 1993, 79, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Patchell, R.A.; Tibbs, P.A.; Walsh, J.W.; Dempsey, R.J.; Maruyama, Y.; Kryscio, R.J.; Markesbery, W.R.; Macdonald, J.S.; Young, B. A Randomized Trial of Surgery in the Treatment of Single Metastases to the Brain. N. Engl. J. Med. 1990, 322, 494–500. [Google Scholar] [CrossRef]
- Patel, A.J.; Suki, D.; Hatiboglu, M.A.; Abouassi, H.; Shi, W.; Wildrick, D.M.; Lang, F.F.; Sawaya, R. Factors influencing the risk of local recurrence after resection of a single brain metastasis. J. Neurosurg. 2010, 113, 181–189. [Google Scholar] [CrossRef]
- Inserra, F.; Barone, F.; Palmisciano, P.; Scalia, G.; Da Ros, V.; Abdelsalam, A.; Crea, A.; Sabini, M.G.; Tomasi, S.O.; Ferini, G.; et al. Hypofractionated Gamma Knife Radiosurgery: Institutional Experience on Benign and Malignant Intracranial Tumors. Anticancer Res. 2022, 42, 1851–1858. [Google Scholar] [CrossRef]
- Chang, E.L.; Wefel, J.S.; Hess, K.R.; Allen, P.K.; Lang, F.F.; Kornguth, D.G.; Arbuckle, R.B.; Swint, J.M.; Shiu, A.S.; Maor, M.H.; et al. Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: A randomised controlled trial. Lancet Oncol. 2009, 10, 1037–1044. [Google Scholar] [CrossRef]
- McCutcheon, I.E. Stereotactic Radiosurgery to Prevent Local Recurrence of Brain Metastasis after Surgery: Neoadjuvant versus Adjuvant. In Gamma Knife Neurosurgery in the Management of Intracranial Disorders II; Springer: Cham, Switzerland, 2021; pp. 85–100. [Google Scholar]
- Cifarelli, C.P.; Brehmer, S.; Vargo, J.A.; Hack, J.D.; Kahl, K.H.; Sarria-Vargas, G.; Giordano, F.A. Intraoperative radiotherapy (IORT) for surgically resected brain metastases: Outcome analysis of an international cooperative study. J. Neurooncol. 2019, 145, 391–397. [Google Scholar] [CrossRef]
- Wernicke, A.G.; Yondorf, M.Z.; Peng, L.; Trichter, S.; Nedialkova, L.; Sabbas, A.; Kulidzhanov, F.; Parashar, B.; Nori, D.; Clifford Chao, K.S.; et al. Phase I/II study of resection and intraoperative cesium-131 radioisotope brachytherapy in patients with newly diagnosed brain metastases. J. Neurosurg. 2014, 121, 338–348. [Google Scholar] [CrossRef]
- Martínez-Rovira, I.; Fois, G.; Prezado, Y. Dosimetric evaluation of new approaches in GRID therapy using nonconventional radiation sources. Med. Phys. 2015, 42, 685–693. [Google Scholar] [CrossRef]
- Ma, L.; Kwok, Y.; Chin, L.S.; Simard, J.M.; Regine, W.F. Concomitant GRID boost for Gamma Knife radiosurgery. Med. Phys. 2005, 32, 3419–3423. [Google Scholar] [CrossRef]
- Castorina, P.; Castorina, L.; Ferini, G. Non-Homogeneous Tumor Growth and Its Implications for Radiotherapy: A Phenomenological Approach. J. Pers. Med. 2021, 11, 527. [Google Scholar] [CrossRef]
- Ferini, G.; Castorina, P.; Valenti, V.; Illari, S.I.; Sachpazidis, I.; Castorina, L.; Marrale, M.; Pergolizzi, S. A Novel Radiotherapeutic Approach to Treat Bulky Metastases Even from Cutaneous Squamous Cell Carcinoma: Its Rationale and a Look at the Reliability of the Linear-Quadratic Model to Explain Its Radiobiological Effects. Front. Oncol. 2022, 12, 809279. [Google Scholar] [CrossRef]
- Ferini, G.; Valenti, V.; Tripoli, A.; Illari, S.I.; Molino, L.; Parisi, S.; Cacciola, A.; Lillo, S.; Giuffrida, D.; Pergolizzi, S. Lattice or Oxygen-Guided Radiotherapy: What If They Converge? Possible Future Directions in the Era of Immunotherapy. Cancers 2021, 13, 3290. [Google Scholar] [CrossRef]
- Hearn, N.; Atwell, D.; Cahill, K.; Elks, J.; Vignarajah, D.; Lagopoulos, J.; Min, M. Neoadjuvant Radiotherapy Dose Escalation in Locally Advanced Rectal Cancer: A Systematic Review and Meta-analysis of Modern Treatment Approaches and Outcomes. Clin. Oncol. (R. Coll. Radiol). 2021, 33, e1–e14. [Google Scholar] [CrossRef]
- Sousa, C.; Cruz, M.; Neto, A.; Pereira, K.; Peixoto, M.; Bastos, J.; Henriques, M.; Roda, D.; Marques, R.; Miranda, C.; et al. Neoadjuvant radiotherapy in the approach of locally advanced breast cancer. ESMO Open 2020, 4, e000640. [Google Scholar] [CrossRef]
- Vellayappan, B.A.; Doody, J.; Vandervoort, E.; Szanto, J.; Sinclair, J.; Caudrelier, J.M.; Malone, S. Pre-operative versus post-operative radiosurgery for brain metastasis: Effects on treatment volume and inter-observer variability. J. Radiosurg. SBRT 2018, 5, 89–97. [Google Scholar]
- Soliman, H.; Ruschin, M.; Angelov, L.; Brown, P.D.; Chiang, V.L.S.; Kirkpatrick, J.P.; Lo, S.S.; Mahajan, A.; Oh, K.S.; Sheehan, J.P.; et al. Consensus Contouring Guidelines for Postoperative Completely Resected Cavity Stereotactic Radiosurgery for Brain Metastases. Int. J. Radiat. Oncol. 2018, 100, 436–442. [Google Scholar] [CrossRef]
- Palmisciano, P.; Haider, A.S.; Nwagwu, C.D.; Wahood, W.; Aoun, S.G.; Abdullah, K.G.; El Ahmadieh, T.Y. Bevacizumab vs. laser interstitial thermal therapy in cerebral radiation necrosis from brain metastases: A systematic review and meta-analysis. J. Neurooncol. 2021, 154, 13–23. [Google Scholar] [CrossRef]
- Ward, J.F. The Complexity of DNA Damage: Relevance to Biological Consequences. Int. J. Radiat. Biol. 1994, 66, 427–432. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors—Year | Patients/ Lesions | Planning Target Volume cm3 Median (Range) | Dose (Gy) & Fraction (fr) Median (Range) | Extent of Resection | Radiation Necrosis/Symptomatic | Local Failure/Distant Failure | Overall Survival |
|---|---|---|---|---|---|---|---|
| Vetlova, 2017 [25] | 19/ 22 | 14.1 (3–57.1) | 18 Gy (12.6–24.4) in 1 fr | GTR 22 (100%) | 2 (10.5%)/ 0 (0%) | 2 (10.5%)/ N/A | 6 m 100% 1 y 50% |
| Patel, 2018 [26] | 12/ 12 | 14.7 (3.4–34.8) | 16 Gy (12–21) in 1 fr | GTR 12 (100%) | 0 (0%)/ 0 (0%) | 4 (33.3%)/ 8 (66.7%) | 6 m 83.3% 1 y 74.1% |
| Prabhu, 2018 [27] | 117/ 125 | 8.3 (4.6–13.3) | 15 Gy (14–17) in 1 fr | GTR 119 (95.2%) STR 6 (4.8%) | 11 (9.4%)/ 5 (4.3%) | 26 (20.8%)/ 65 (55.6%) | 1 y 60.6% 2 y 36.7% |
| Prabhu, 2021 [28] | 242/ 253 | 9.9 (5–17) | 15 Gy (14–16) in 1 fr (1–5) | GTR 237 (93.7%)/ STR 16 (6.3%) | 18 (7.1%)/ 18 (7.1%) | 15 Gy (14–16) in 1 fr (1–5) | 39 (15.4%)/ 106 (43.8%) |
| Deguchi, 2022 [29] | 20/ 20 | 17.6 (5.6–49.7) | 30 Gy (30–35) in 5 fr | GTR 17 (85%) STR 3 (15%) | 0 (0%)/ 0 (0%) | 1 (5%)/ 6 (30%) | 6 m 56% 1 y 50% |
| Kotecha, 2022 [30] | 22/ 22 | 14.2 (2.9–31.4) | 18 Gy (15–30) in 1 fr (1–5) | GTR 22 (100%) | N/A | 3 (1.6%)/ N/A | N/A |
| Udovicich, 2014 [31] | 28/ 29 | 4.5 (3.1–18.9) | 23 Gy (18–27.5) in 3 fr (1–5) | GTR 25 (86.2%) STR 4 (13.8%) | 1 (3.4%)/ 1 (3.4%) | 2 (7.1%)/ 14 (50%) | 1 y 60.1% |
| Characteristics | Value |
|---|---|
| Cohort size (no.) | |
| Patients | 460 |
| Lesions | 483 |
| Demographics | |
| Age (years), median (range) | 60 (30–80) |
| Gender (female) | 253 (55%) |
| Primary Tumor | No. (%) |
| Non-small cell lung carcinoma | 190 (41.4%) |
| Breast cancer | 86 (18.7%) |
| Melanoma | 67 (14.6%) |
| Renal cell carcinoma | 43 (9.3%) |
| Others | 74 (16.1%) |
| Number of Lesions Per-Patient | No. (%) |
| 1 | 321 (69.8%) |
| 2 | 79 (17.2%) |
| 3 | 38 (8.3%) |
| 4 | 15 (3.3%) |
| ≥5 | 7 (1.5%) |
| Location | No. (%) |
| Supratentorial | 358 (77.8%) |
| Infratentorial | 102 (22.2%) |
| Planning Target Volume (cm3), median (range) | 9.9 (2.9–57.1) |
| Radiotherapy Protocol | |
| Prescribed dose (Gy) | 16.5 (12.6–35) |
| Number of fractions | |
| 1 | 439 (7.5%) |
| 3 | 21 (6.9%) |
| 5 | 23 (4.9%) |
| Biologically effective dose (BED) (Gy10) | 39.6 (35.7–60) |
| Time from Radiotherapy to Surgery (day), median (range) | 1 (1–10) |
| Surgery Protocol | No. (%) |
| Type of resection | |
| Piecemeal | 180 (76.3%) |
| En bloc | 56 (23.7%) |
| Extent of resection | |
| Gross-total | 454 (94%) |
| Subtotal | 29 (6%) |
| Follow-up (months), median (range) | 19.2 (1–41.3) |
| Outcomes | No. (%) |
| Radiation necrosis (n = 438) | 32 (7.3%) |
| Symptomatic | 24 (5.5%) |
| Local recurrences | 77 (16.7%) |
| Distant brain recurrences (n = 419) | 199 (43.3%) |
| Leptomeningeal metastases (n = 438) | 30 (6.8%) |
| Local tumor control (n = 186) | |
| 1-year | 80% (50–95%) |
| Overall survival (n = 438) | |
| 6-month | 80% (56–100%) |
| 1-year | 58% (50–74.1%) |
| 2-year | 37.8% (36.7–38.4%) |
| Survival Status (n = 438) | No. (%) |
| Alive | 146 (33.3%) |
| Dead | 292 (66.7%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palmisciano, P.; Ferini, G.; Khan, R.; Bin-Alamer, O.; Umana, G.E.; Yu, K.; Cohen-Gadol, A.A.; El Ahmadieh, T.Y.; Haider, A.S. Neoadjuvant Stereotactic Radiotherapy for Brain Metastases: Systematic Review and Meta-Analysis of the Literature and Ongoing Clinical Trials. Cancers 2022, 14, 4328. https://doi.org/10.3390/cancers14174328
Palmisciano P, Ferini G, Khan R, Bin-Alamer O, Umana GE, Yu K, Cohen-Gadol AA, El Ahmadieh TY, Haider AS. Neoadjuvant Stereotactic Radiotherapy for Brain Metastases: Systematic Review and Meta-Analysis of the Literature and Ongoing Clinical Trials. Cancers. 2022; 14(17):4328. https://doi.org/10.3390/cancers14174328
Chicago/Turabian StylePalmisciano, Paolo, Gianluca Ferini, Ramlah Khan, Othman Bin-Alamer, Giuseppe E. Umana, Kenny Yu, Aaron A. Cohen-Gadol, Tarek Y. El Ahmadieh, and Ali S. Haider. 2022. "Neoadjuvant Stereotactic Radiotherapy for Brain Metastases: Systematic Review and Meta-Analysis of the Literature and Ongoing Clinical Trials" Cancers 14, no. 17: 4328. https://doi.org/10.3390/cancers14174328
APA StylePalmisciano, P., Ferini, G., Khan, R., Bin-Alamer, O., Umana, G. E., Yu, K., Cohen-Gadol, A. A., El Ahmadieh, T. Y., & Haider, A. S. (2022). Neoadjuvant Stereotactic Radiotherapy for Brain Metastases: Systematic Review and Meta-Analysis of the Literature and Ongoing Clinical Trials. Cancers, 14(17), 4328. https://doi.org/10.3390/cancers14174328