
The Hepatic Innovation Team Collaborative: A Successful Population-Based Approach to Hepatocellular Carcinoma Surveillance

 , ,
, ,  , , , , and
, , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Cirrhosis and HCC Surveillance Definitions
2.2. Facility Variables
2.3. HIT Membership and Use of the Advanced Liver Disease Dashboard, and HCC Clinical Reminder
2.4. Analysis
3. Results
3.1. HIT Activities
3.2. Facility Characteristics and HIT Engagement
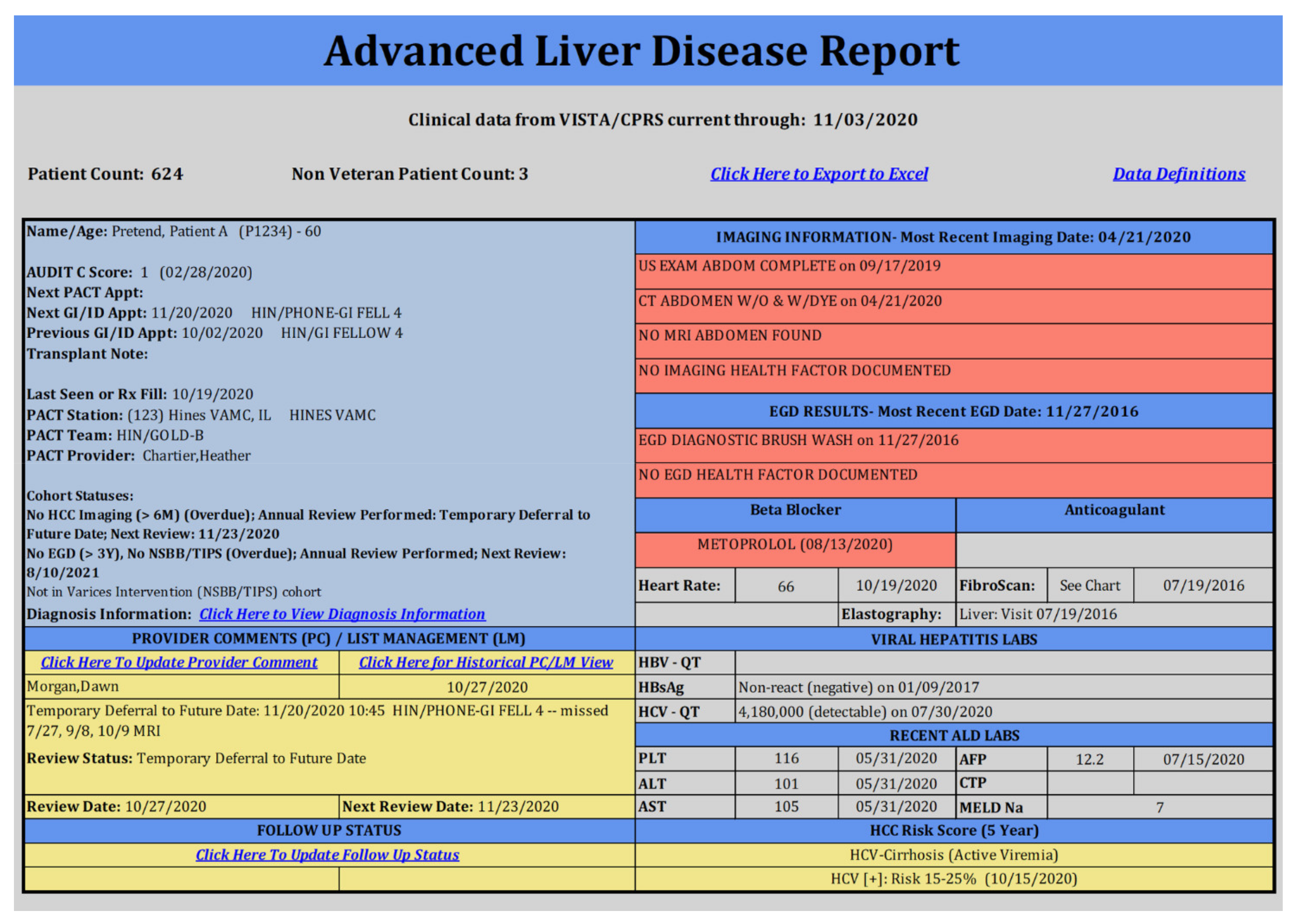
3.3. Advanced Liver Disease Dashboard
3.4. HCC Clinical Reminder
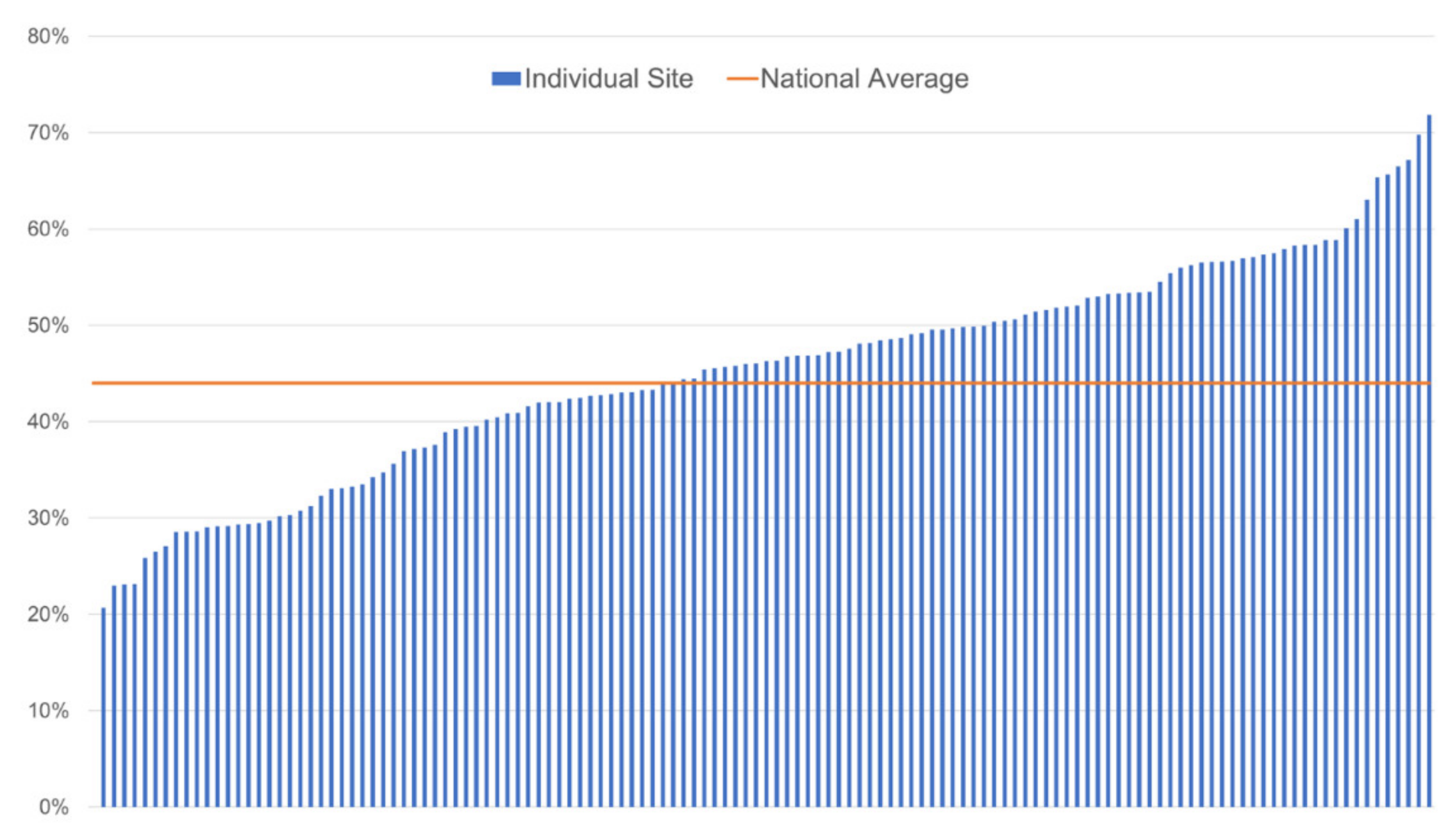
3.5. HCC Surveillance Rates
3.6. Factors Associated with HCC Surveillance in Multivariable Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kanwal, F.; Hoang, T.; Kramer, J.R.; Asch, S.M.; Goetz, M.B.; Zeringue, A.; Richardson, P.; El-Serag, H.B. Increasing prevalence of HCC and cirrhosis in patients with chronic hepatitis C virus infection. Gastroenterology 2011, 140, 1182–1188. [Google Scholar] [CrossRef] [PubMed]
- Beste, L.A.; Leipertz, S.L.; Green, P.K.; Dominitz, J.A.; Ross, D.; Ioannou, G.N. Trends in burden of cirrhosis and hepatocellular carcinoma by underlying liver disease in US veterans, 2001–2013. Gastroenterology 2015, 149, 1471–1482. [Google Scholar] [CrossRef]
- Ryerson, A.B.; Eheman, C.R.; Altekruse, S.F.; Ward, J.W.; Jemal, A.; Sherman, R.L.; Henley, S.J.; Holtzman, D.; Lake, A.; Noone, A.M.; et al. Annual Report to the Nation on the Status of Cancer, 1975–2012, featuring the increasing incidence of liver cancer. Cancer 2016, 122, 1312–1337. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.H.; Chen, C.M. Surveillance Report #105: Liver Cirrhosis Mortality in the United States: National, State, and Regional Trends, 2000–2013; National Institute on Alcohol Abuse and Alcoholism: Bethesda, MD, USA, 2016. [Google Scholar]
- Cadier, B.; Bulsei, J.; Nahon, P.; Seror, O.; Laurent, A.; Rosa, I.; Layese, R.; Costentin, C.; Cagnot, C.; Durand-Zaleski, I.; et al. Early detection and curative treatment of hepatocellular carcinoma: A cost-effectiveness analysis in France and in the United States. Hepatology 2017, 65, 1237–1248. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Y.; Hsu, Y.C.; Ho, H.J.; Chen, Y.J.; Lee, T.Y.; Lin, J.T. Association between ultrasonography screening and mortality in patients with hepatocellular carcinoma: A nationwide cohort study. Gut 2016, 65, 693–701. [Google Scholar] [CrossRef]
- Yang, J.D.; Mannalithara, A.; Piscitello, A.J.; Kisiel, J.B.; Gores, G.J.; Roberts, L.R.; Kim, W.R. Impact of surveillance for hepatocellular carcinoma on survival in patients with compensated cirrhosis. Hepatology 2018, 68, 78–88. [Google Scholar] [CrossRef]
- Davila, J.A.; Henderson, L.; Kramer, J.R.; Kanwal, F.; Richardson, P.A.; Duan, Z.; El-Serag, H.B. Utilization of surveillance for hepatocellular carcinoma among hepatitis C virus-infected veterans in the United States. Ann. Intern. Med. 2011, 154, 85–93. [Google Scholar] [CrossRef]
- Goldberg, D.S.; Valderrama, A.; Kamalakar, R.; Sansgiry, S.S.; Babajanyan, S.; Lewis, J.D. Hepatocellular carcinoma surveillance rates in commercially insured patients with noncirrhotic chronic hepatitis B. J. Viral Hepat. 2015, 22, 727–736. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century; The National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- De Koning, H.; Verver, J.P.; van den Heuvel, J.; Bisgaard, S.; Does, R.J. Lean six sigma in healthcare. J. Healthc. Qual. 2006, 28, 4–11. [Google Scholar] [CrossRef]
- Gilman, S.C.; Chokshi, D.A.; Bowen, J.L.; Rugen, K.W.; Cox, M. Connecting the dots: Interprofessional health education and delivery system redesign at the Veterans Health Administration. Acad. Med. 2014, 89, 1113–1116. [Google Scholar] [CrossRef] [PubMed]
- Lukas, C.V.; Holmes, S.K.; Cohen, A.B.; Restuccia, J.; Cramer, I.E.; Shwartz, M.; Charns, M.P. Transformational change in health care systems: An organizational model. Health Care Manag. Rev. 2007, 32, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Belperio, P.S.; Chartier, M.; Gonzalez, R.I.; Park, A.M.; Ross, D.B.; Morgan, T.R.; Backus, L.I. Hepatitis C Care in the Department of Veterans Affairs: Building a Foundation for Success. Infect. Dis. Clin. N. Am. 2018, 32, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Park, A.; Gonzalez, R.; Chartier, M.; Rogal, S.; Yakovchenko, V.; Ross, D.; Morgan, T.R. Screening and Treating Hepatitis C in the VA: Achieving Excellence Using Lean and System Redesign. Fed. Pract. 2018, 35, 24–29. [Google Scholar] [PubMed]
- Belperio, P.S.; Chartier, M.; Ross, D.B.; Alaigh, P.; Shulkin, D. Curing Hepatitis C Virus Infection: Best Practices From the U.S. Department of Veterans Affairs. Ann. Intern. Med. 2017, 167, 499–504. [Google Scholar] [CrossRef]
- Rogal, S.S.; Yakovchenko, V.; Waltz, T.J.; Powell, B.J.; Kirchner, J.E.; Proctor, E.K.; Gonzalez, R.; Park, A.; Ross, D.; Morgan, T.R.; et al. The association between implementation strategy use and the uptake of hepatitis C treatment in a national sample. Implement. Sci. 2017, 12, 60. [Google Scholar] [CrossRef]
- Rogal, S.S.; Yakovchenko, V.; Waltz, T.J.; Powell, B.J.; Gonzalez, R.; Park, A.; Chartier, M.; Ross, D.; Morgan, T.R.; Kirchner, J.E.; et al. Longitudinal assessment of the association between implementation strategy use and the uptake of hepatitis C treatment: Year 2. Implement. Sci. 2019, 14, 36. [Google Scholar] [CrossRef] [PubMed]
- Veterans Health Administration. VHA Facility Complexity Model 2015. Available online: http://opes.vssc.med.va.gov/FacilityComplexityLevels/Pages/default.aspx (accessed on 12 December 2016).
- Elsasser, E.J.; White, C.A.; Jones, M.R. Implementation of a transformational plan of care at a Veterans Affairs medical center. Am. J. Health Syst. Pharm. 2018, 75, S72–S76. [Google Scholar] [CrossRef]
- Abara, W.E.; Spradling, P.; Zhong, Y.; Moorman, A.; Teshale, E.H.; Rupp, L.; Gordon, S.C.; Schmidt, M.; Boscarino, J.A.; Daida, Y.G.; et al. Hepatocellular Carcinoma Surveillance in a Cohort of Chronic Hepatitis C Virus-Infected Patients with Cirrhosis. J. Gastrointest. Cancer 2020, 51, 461–468. [Google Scholar] [CrossRef]
- Wolf, E.; Rich, N.E.; Marrero, J.A.; Parikh, N.D.; Singal, A.G. Use of Hepatocellular Carcinoma Surveillance in Patients With Cirrhosis: A Systematic Review and Meta-Analysis. Hepatology 2021, 73, 713–725. [Google Scholar] [CrossRef]
- Singal, A.G.; Tiro, J.; Li, X.; Adams-Huet, B.; Chubak, J. Hepatocellular Carcinoma Surveillance Among Patients With Cirrhosis in a Population-based Integrated Health Care Delivery System. J. Clin. Gastroenterol. 2017, 51, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, E.R.; Rubenstein, L.; Kandrack, R.; Danz, M.; Belsher, B.; Motala, A.; Booth, M.; Larkin, J.; Hempel, S. Elusive search for effective provider interventions: A systematic review of provider interventions to increase adherence to evidence-based treatment for depression. Implement. Sci. 2018, 13, 99. [Google Scholar] [CrossRef]
- Thomson, M.J.; Lok, A.S.; Tapper, E.B. Optimizing medication management for patients with cirrhosis: Evidence-based strategies and their outcomes. Liver Int. 2018, 38, 1882–1890. [Google Scholar] [CrossRef] [PubMed]
- Harder, V.S.; Shaw, J.S.; McCulloch, C.E.; Kill, L.; Robinson, K.J.; Shepard, M.T.; Cabana, M.D.; Bardach, N.S. Statewide Asthma Learning Collaborative Participation and Asthma-Related Emergency Department Use. Pediatrics 2020, 146. [Google Scholar] [CrossRef]
- Penney, L.S.; Homoya, B.J.; Damush, T.M.; Rattray, N.A.; Miech, E.J.; Myers, L.J.; Baird, S.; Cheatham, A.; Bravata, D.M. Seeding Structures for a Community of Practice Focused on Transient Ischemic Attack (TIA): Implementing Across Disciplines and Waves. J. Gen. Intern. Med. 2021, 36, 313–321. [Google Scholar] [CrossRef]
- Quimby, K.D.; Kawatu, J.E.; Saul, K.M.; Schamus, L.A. Implementation of a Learning Collaborative Model Increases Chlamydia Screening at 37 Family Planning Clinics: Lessons Learned From 3 Cohorts. Sex Transm. Dis. 2021, 48, 5–11. [Google Scholar] [CrossRef]
- Cox, C.K.; Bugosh, M.D.; Fenner, D.E.; Smith, R.; Swenson, C.W. Antibiotic use during repair of obstetrical anal sphincter injury: A quality improvement initiative. Int. J. Gynaecol. Obstet. 2021. [Google Scholar] [CrossRef]
- Hysong, S.J.; Best, R.G.; Pugh, J.A. Audit and feedback and clinical practice guideline adherence: Making feedback actionable. Implement. Sci. 2006, 1, 9. [Google Scholar] [CrossRef] [PubMed]
- Ivers, N.; Jamtvedt, G.; Flottorp, S.; Young, J.M.; Odgaard-Jensen, J.; French, S.D.; O’Brien, M.A.; Johansen, M.; Grimshaw, J.; Oxman, A.D. Audit and feedback: Effects on professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2012, CD000259. [Google Scholar] [CrossRef]
- Ivers, N.M.; Sales, A.; Colquhoun, H.; Michie, S.; Foy, R.; Francis, J.J.; Grimshaw, J.M. No more ‘business as usual’ with audit and feedback interventions: Towards an agenda for a reinvigorated intervention. Implement. Sci. 2014, 9, 14. [Google Scholar] [CrossRef]
- Bajaj, P.; Kollipara, U.; Koganti, R.; Wang, D.C.; Chennu, N.; Bhat, D.; Mutz, J.; Willett, D.; Fish, J.; Karp, D. Coupled Effect of Electronic Medical Record Modifications and Lean Six Sigma Methodology on Rheumatoid Arthritis Disease Activity Measurement and Treat-to-Target Outcomes. ACR Open Rheumatol. 2021, 3, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Rogal, S.S.; Yakovchenko, V.; Morgan, T.; Bajaj, J.S.; Gonzalez, R.; Park, A.; Beste, L.; Miech, E.J.; Lamorte, C.; Neely, B.; et al. Getting to implementation: A protocol for a Hybrid III stepped wedge cluster randomized evaluation of using data-driven implementation strategies to improve cirrhosis care for Veterans. Implement. Sci. 2020, 15, 92. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Facilities n (%) |
|---|---|
| Facility complexity | |
| 1 (high) | 77 (59%) |
| 2 | 24 (18%) |
| 3 (low) | 29 (22%) |
| On-site GI specialty care | |
| Yes | 106 (82%) |
| No | 24 (18%) |
| HIT member at facility | |
| Yes | 113 (87%) |
| No | 17 (13%) |
| ALD Dashboard utilization | |
| High | 34 (26%) |
| Low | 96 (74%) |
| HCC Clinical Reminder use | |
| Yes | 20 (15%) |
| No | 110 (85%) |
| Facility Characteristics | HCC Surveillance Rate (%) | |||
|---|---|---|---|---|
| FY18 | p | FY19 | p | |
| Complexity | <0.001 | <0.001 | ||
| 1 (high) | 49 | 54 | ||
| 2 | 44 | 47 | ||
| 3 (low) | 36 | 44 | ||
| Quartile of case load | <0.001 | 0.35 | ||
| 1 (low) | 40 | 49 | ||
| 2 | 43 | 50 | ||
| 3 | 49 | 53 | ||
| 4 (high) | 49 | 51 | ||
| On-site GI specialty care | <0.001 | 0.003 | ||
| Yes | 48 | 53 | ||
| No | 37 | 41 | ||
| HIT member at facility | 0.12 | 0.003 | ||
| Yes | 41 | 52 | ||
| No | 46 | 42 | ||
| ALD Dashboard utilization | <0.001 | <0.001 | ||
| High | 51 | 57 | ||
| Low | 40 | 45 | ||
| HCC Clinical Reminder use | <0.001 | <0.001 | ||
| Yes | 53 | 58 | ||
| No | 44 | 47 | ||
| Covariates | FY18 | FY19 | ||||
|---|---|---|---|---|---|---|
| β | SE | p | β | SE | p | |
| Complexity | 0.068 | 0.022 | 0.002 | 0.042 | 0.027 | Ns |
| On-site GI specialty care | 0.036 | 0.024 | Ns | 0.066 | 0.030 | 0.026 |
| ALD Dashboard utilization | 0.067 | 0.018 | <0.001 | 0.072 | 0.022 | 0.001 |
| HCC Clinical Reminder | 0.054 | 0.025 | 0.029 | 0.076 | 0.023 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogal, S.S.; Yakovchenko, V.; Gonzalez, R.; Park, A.; Beste, L.A.; Rozenberg-Ben-Dror, K.; Bajaj, J.S.; Scott, D.; McCurdy, H.; Comstock, E.; et al. The Hepatic Innovation Team Collaborative: A Successful Population-Based Approach to Hepatocellular Carcinoma Surveillance. Cancers 2021, 13, 2251. https://doi.org/10.3390/cancers13092251
Rogal SS, Yakovchenko V, Gonzalez R, Park A, Beste LA, Rozenberg-Ben-Dror K, Bajaj JS, Scott D, McCurdy H, Comstock E, et al. The Hepatic Innovation Team Collaborative: A Successful Population-Based Approach to Hepatocellular Carcinoma Surveillance. Cancers. 2021; 13(9):2251. https://doi.org/10.3390/cancers13092251
Chicago/Turabian StyleRogal, Shari S., Vera Yakovchenko, Rachel Gonzalez, Angela Park, Lauren A. Beste, Karine Rozenberg-Ben-Dror, Jasmohan S. Bajaj, Dawn Scott, Heather McCurdy, Emily Comstock, and et al. 2021. "The Hepatic Innovation Team Collaborative: A Successful Population-Based Approach to Hepatocellular Carcinoma Surveillance" Cancers 13, no. 9: 2251. https://doi.org/10.3390/cancers13092251
APA StyleRogal, S. S., Yakovchenko, V., Gonzalez, R., Park, A., Beste, L. A., Rozenberg-Ben-Dror, K., Bajaj, J. S., Scott, D., McCurdy, H., Comstock, E., Sidorovic, M., Gibson, S., Lamorte, C., Nobbe, A., Chartier, M., Ross, D., Dominitz, J. A., & Morgan, T. R. (2021). The Hepatic Innovation Team Collaborative: A Successful Population-Based Approach to Hepatocellular Carcinoma Surveillance. Cancers, 13(9), 2251. https://doi.org/10.3390/cancers13092251