
Enhanced Antitumor Effect of Trastuzumab and Duligotuzumab or Ipatasertib Combination in HER-2 Positive Gastric Cancer Cells

 , , ,
, , ,  , , ,
, , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
2. Results
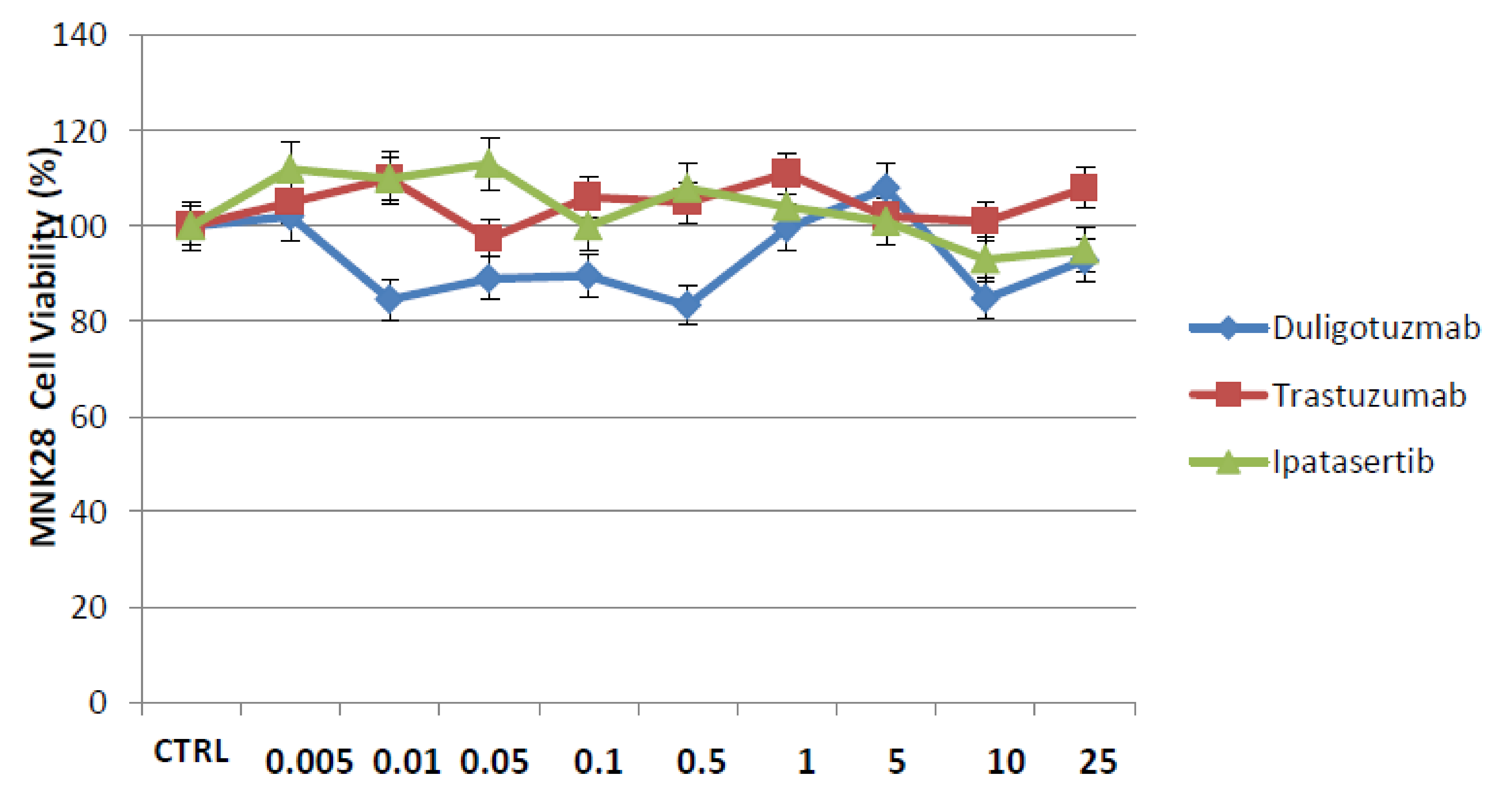
2.1. Effect of Duligotuzumab or Ipatasertib in Combination with Trastuzumab on Cell Proliferation in a Panel of Human Gastric Cancer Cell Lines
2.2. Effects of Duligotuzumab, Ipatasertib and Trastuzumab on Colony Formation and Migration Abilities of Human Gastric Cancer Cell Lines
2.3. Apoptosis Analysis of Human Gastric Cell Lines after Treatment with Duligotuzumab, Ipatasertib and Trastuzumab
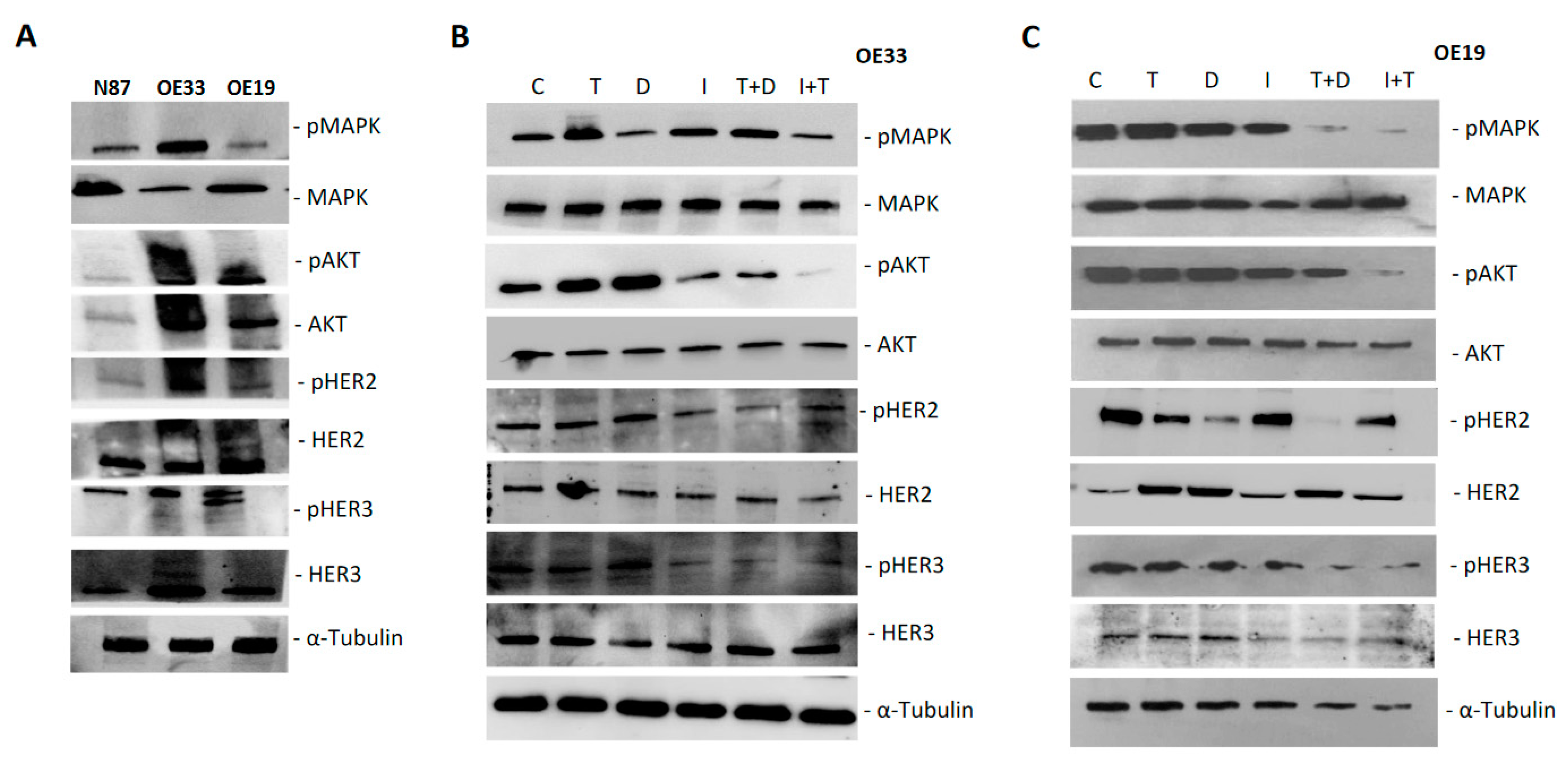
2.4. Protein Analysis of Intracellular Signaling Pathways in Human Gastric Cancer Cell Lines
3. Discussion
4. Materials and Methods
4.1. Cell Lines and Drugs
4.2. Cell Proliferation Assays
4.3. Colony-Forming Assays
4.4. Migration Assays
4.5. Evaluation of Apoptosis
4.6. Protein Expression Analysis
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.D.; Unverzagt, S.; Grothe, W.; Haerting, J.; Kleber, G.; Grothey, A.; Fleig, W.E. Chemotherapy for advanced gastric cancer. Cochrane Database. Syst. Rev. 2010, CD004064. [Google Scholar] [CrossRef]
- Nashimoto, A.; Akazawa, K.; Isobe, Y.; Miyashiro, I.; Katai, H.; Kodera, Y.; Tsujitani, S.; Seto, Y.; Furukawa, H.; Oda, I.; et al. Gastric cancer treated in 2002 in Japan: 2009 annual report of the JGCA nationwide registry. Gastric Cancer 2012, 16, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.A.; Khanin, R.; Tang, L.; Janjigian, Y.Y.; Klimstra, D.S.; Gerdes, H.; Kelsen, D.P. Molecular Classification of Gastric Cancer: A New Paradigm. Clin. Cancer Res. 2011, 17, 2693–2701. [Google Scholar] [CrossRef]
- Roukos, D.H. Targeting Gastric Cancer with Trastuzumab: New Clinical Practice and Innovative Developments to Overcome Resistance. Ann. Surg. Oncol. 2009, 17, 14–17. [Google Scholar] [CrossRef]
- Slamon, D.J.; Leyland-Jones, B.; Shak, S.; Fuchs, H.; Paton, V.; Bajamonde, A.; Fleming, T.; Eiermann, W.; Wolter, J.; Pegram, M.; et al. Use of Chemotherapy plus a Monoclonal Antibody against HER2 for Metastatic Breast Cancer That Overexpresses HER2. N. Engl. J. Med. 2001, 344, 783–792. [Google Scholar] [CrossRef]
- Hudis, C.A. Trastuzumab—Mechanism of Action and Use in Clinical Practice. N. Engl. J. Med. 2007, 357, 39–51. [Google Scholar] [CrossRef]
- Bang, Y.-J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Shimoyama, S. Unraveling trastuzumab and lapatinib inefficiency in gastric cancer: Future steps (Review). Mol. Clin. Oncol. 2014, 2, 175–181. [Google Scholar] [CrossRef]
- Satoh, T.; Xu, R.-H.; Chung, H.C.; Sun, G.-P.; Doi, T.; Xu, J.-M.; Tsuji, A.; Omuro, Y.; Li, J.; Wang, J.-W.; et al. Lapatinib Plus Paclitaxel Versus Paclitaxel Alone in the Second-Line Treatment ofHER2-Amplified Advanced Gastric Cancer in Asian Populations: TyTAN—A Randomized, Phase III Study. J. Clin. Oncol. 2014, 32, 2039–2049. [Google Scholar] [CrossRef]
- Hecht, J.R.; Bang, Y.-J.; Qin, S.K.; Chung, H.C.; Xu, J.M.; Park, J.O.; Jeziorski, K.; Shparyk, Y.; Hoff, P.M.; Sobrero, A.; et al. Lapatinib in Combination With Capecitabine Plus Oxaliplatin in Human Epidermal Growth Factor Receptor 2–Positive Advanced or Metastatic Gastric, Esophageal, or Gastroesophageal Adenocarcinoma: TRIO-013/LOGiC—A Randomized Phase III Trial. J. Clin. Oncol. 2016, 34, 443–451. [Google Scholar] [CrossRef]
- Thuss-Patience, P.; Shah, M.; Ohtsu, A.; Van Cutsem, E.; Ajani, J.; Castro, H.; Mansoor, W.; Chung, H.; Bodoky, G.; Shitara, K.; et al. Trastuzumab emtansine versus taxane use for previously treated HER2-positive locally advanced or metastatic gastric or gastro-oesophageal junction adenocarcinoma (GATSBY): An international randomised, open-label, adaptive, phase 2/3 study. Lancet Oncol. 2017, 18, 640–653. [Google Scholar] [CrossRef]
- Zuo, Q.; Liu, J.; Zhang, J.; Wu, M.; Guo, L.; Liao, W. Development of trastuzumab-resistant human gastric carcinoma cell lines and mechanisms of drug resistance. Sci. Rep. 2015, 5, srep11634. [Google Scholar] [CrossRef]
- Arcaro, A.; Guerreiro, A.S. The Phosphoinositide 3-Kinase Pathway in Human Cancer: Genetic Alterations and Therapeutic Implications. Curr. Genom. 2007, 8, 271–306. [Google Scholar] [CrossRef]
- Nahta, R.; O’Regan, R.M. Evolving strate-gies for overcoming resistance to HER2-directed therapy: Targeting the PI3K/Akt/mTOR pathway. Clin. Breast Cancer 2010, 10, S72–S78. [Google Scholar] [CrossRef]
- Liu, J.; Pan, C.; Guo, L.; Wu, M.; Guo, J.; Peng, S.; Wu, Q.; Zuo, Q. A new mechanism of trastuzumab resistance in gastric cancer: MACC1 promotes the Warburg effect via activation of the PI3K/AKT signaling pathway. J. Hematol. Oncol. 2016, 9, 1–15. [Google Scholar] [CrossRef]
- Luque-Cabal, M.; García-Teijido, P.; Fernández-Pérez, Y.; Sánchez-Lorenzo, L.; Palacio-Vázquez, I. Mechanisms behind the Resistance to Trastuzumab in HER2-Amplified Breast Cancer and Strategies to Overcome It. Clin. Med. Insights Oncol. 2016, 10s1, CMO.S34537-30. [Google Scholar] [CrossRef]
- Ma, J.; Lyu, H.; Huang, J.; Liu, B. Targeting of erbB3 receptor to overcome resistance in cancer treatment. Mol. Cancer 2014, 13, 105. [Google Scholar] [CrossRef]
- Arienti, C.; Zanoni, M.; Pignatta, S.; Del Rio, A.; Carloni, S.; Tebaldi, M.; Tedaldi, G.; Tesei, A. Preclinical evidence of multiple mechanisms underlying trastuzumab resistance in gastric cancer. Oncotarget 2016, 7, 18424–18439. [Google Scholar] [CrossRef]
- LoPiccolo, J.; Blumenthal, G.M.; Bernstein, W.B.; Dennis, P.A. Targeting the PI3K/Akt/mTOR pathway: Effective combinations and clinical considerations. Drug Resist. Updat. 2008, 11, 32–50. [Google Scholar] [CrossRef]
- Kruser, T.J.; Wheeler, D.L. Mechanisms of resistance to HER family targeting antibodies. Exp. Cell Res. 2010, 316, 1083–1100. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Saba, N.F.; Chen, Z.G. Advances in Targeting HER3 as an Anticancer Therapy. Chemother. Res. Pr. 2012, 2012, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nitulescu, G.M.; Margina, D.; Juzenas, P.; Peng, Q.; Olaru, O.T.; Saloustros, E.; Fenga, C.; Spandidos, D.A.; Libra, M.; Tsatsakis, A.M. Akt inhibitors in cancer treatment: The long journey from drug discovery to clinical use (Review). Int. J. Oncol. 2016, 48, 869–885. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; Kang, Y.K.; Alsina, M.; Wainberg, Z.A.; Chau, I.; Zhu, J.; Chan, W.Y.; Patel, P.H.; Meng, R.D.; Ajani, J.A. JAGUAR: A randomized phase II study of the AKT in-hibitor ipatasertib (GDC-0068) versus placebo in combination with mFOLFOX6 chemotherapy in patients (pts) with lo-cally advanced or metastatic HER2-negative gastric (G) or gastroesophageal junction (GEJ) adenocarcinoma. J. Clin. Oncol. 2014, 32, TPS4147. [Google Scholar]
- Huang, S.; Li, C.; Sliwkowski, M.X.; Harari, P.M. Abstract 637: MEHD7945A, an EGFR/ErbB3 dual specific antibody, overcomes acquired resistance to EGFR inhibitors in head and neck and lung tumors. Exp. Mol. Ther. 2011, 71, 637. [Google Scholar] [CrossRef]
- Fayette, J.; Wirth, L.; Oprean, C.; Udrea, A.; Jimeno, A.; Rischin, D.; Nutting, C.; Harari, P.M.; Csoszi, T.; Cernea, D.; et al. Randomized Phase II Study of Duligotuzumab (MEHD7945A) vs. Cetuximab in Squamous Cell Carcinoma of the Head and Neck (MEHGAN Study). Front. Oncol. 2016, 6, 232. [Google Scholar] [CrossRef]
- Tabernero, J.; Hoff, P.; Shen, L.; Ohtsu, A.; Shah, M.; Cheng, K.; Song, C.; Wu, H.; Eng-Wong, J.; Kang, Y.-K. Pertuzumab (P) + trastuzumab (H) + chemotherapy (CT) for HER2-positive metastatic gastric or gastro-oesophageal junction cancer (mGC/GEJC): Final analysis of a phase III study (JACOB). In Proceedings of the European Society for Medical Oncology (ESMO) 2017 Congress, Madrid, Spain, 8–12 September 2017. [Google Scholar]
- Nahta, R.; Yu, D.; Hung, M.-C.; Hortobagyi, G.N.; Esteva, F.J. Mechanisms of Disease: Understanding resistance to HER2-targeted therapy in human breast cancer. Nat. Clin. Pr. Oncol. 2006, 3, 269–280. [Google Scholar] [CrossRef]
- Matsuoka, T.; Yashiro, M. The Role of PI3K/Akt/mTOR Signaling in Gastric Carcinoma. Cancers 2014, 6, 1441–1463. [Google Scholar] [CrossRef]
- Cao, G.-D.; Chen, K.; Xiong, M.-M.; Chen, B. HER3, but Not HER4, Plays an Essential Role in the Clinicopathology and Prognosis of Gastric Cancer: A Meta-Analysis. PLoS ONE 2016, 11, e0161219. [Google Scholar] [CrossRef]
- Kim, J.; Fox, C.; Peng, S.; Pusung, M.; Pectasides, E.; Matthee, E.; Hong, Y.S.; Do, I.-G.; Jang, J.; Thorner, A.R.; et al. Preexisting oncogenic events impact trastuzumab sensitivity in ERBB2-amplified gastroesophageal adenocarcinoma. J. Clin. Investig. 2014, 124, 5145–5158. [Google Scholar] [CrossRef]
- Ramanathan, R.K.; McDonough, S.L.; Kennecke, H.F.; Iqbal, S.; Baranda, J.C.; Seery, T.E.; Lim, H.J.; Hezel, A.F.; Vaccaro, G.M.; Blanke, C.D. A phase II study of MK-2206, an allosteric inhibitor of AKT as second-line therapy for advanced gastric and gastroesophageal junction (GEJ) cancer: A SWOG Cooperative Group trial (S1005). J. Clin. Oncol. 2014, 32, 4041. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, X.; Shen, E.; Gao, J.; Cao, F.; Wang, X.; Li, Y.; Tian, T.; Wang, J.; Chen, Z.; et al. The anti-HER3 antibody in combination with trastuzumab exerts synergistic antitumor activity in HER2-positive gastric cancer. Cancer Lett. 2016, 380, 20–30. [Google Scholar] [CrossRef]
- Hudis, C.; Swanton, C.; Janjigian, Y.Y.; Lee, R.; Sutherland, S.; Lehman, R.; Chandarlapaty, S.; Hamilton, N.; Gajria, D.; Knowles, J.; et al. A phase 1 study evaluating the combination of an allosteric AKT inhibitor (MK-2206) and trastuzumab in patients with HER2-positive solid tumors. Breast Cancer Res. 2013, 15, R110. [Google Scholar] [CrossRef]
- Morgillo, F.; D’Aiuto, E.; Troiani, T.; Martinelli, E.; Cascone, T.; De Palma, R.; Orditura, M.; De Vita, F.; Ciardiello, F. Antitumor activity of bortezomib in human cancer cells with acquired resistance to anti-epidermal growth factor receptor tyrosine kinase inhibitors. Lung Cancer 2011, 71, 283–290. [Google Scholar] [CrossRef]
- Ciaramella, V.; Della Corte, C.M.; Di Mauro, C.; Tomassi, S.; Di Maro, S.; Troiani, T.; Martinelli, E.; Bianco, R.; Cosconati, S.; Pierantoni, R.; et al. Antitumor efficacy of Kisspeptin in human malignant mesothelioma cells. Oncotarget 2018, 9, 19273–19282. [Google Scholar] [CrossRef][Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laterza, M.M.; Ciaramella, V.; Facchini, B.A.; Franzese, E.; Liguori, C.; De Falco, S.; Coppola, P.; Pompella, L.; Tirino, G.; Berretta, M.; et al. Enhanced Antitumor Effect of Trastuzumab and Duligotuzumab or Ipatasertib Combination in HER-2 Positive Gastric Cancer Cells. Cancers 2021, 13, 2339. https://doi.org/10.3390/cancers13102339
Laterza MM, Ciaramella V, Facchini BA, Franzese E, Liguori C, De Falco S, Coppola P, Pompella L, Tirino G, Berretta M, et al. Enhanced Antitumor Effect of Trastuzumab and Duligotuzumab or Ipatasertib Combination in HER-2 Positive Gastric Cancer Cells. Cancers. 2021; 13(10):2339. https://doi.org/10.3390/cancers13102339
Chicago/Turabian StyleLaterza, Maria Maddalena, Vincenza Ciaramella, Bianca Arianna Facchini, Elisena Franzese, Carmela Liguori, Stefano De Falco, Paola Coppola, Luca Pompella, Giuseppe Tirino, Massimiliano Berretta, and et al. 2021. "Enhanced Antitumor Effect of Trastuzumab and Duligotuzumab or Ipatasertib Combination in HER-2 Positive Gastric Cancer Cells" Cancers 13, no. 10: 2339. https://doi.org/10.3390/cancers13102339
APA StyleLaterza, M. M., Ciaramella, V., Facchini, B. A., Franzese, E., Liguori, C., De Falco, S., Coppola, P., Pompella, L., Tirino, G., Berretta, M., Montella, L., Facchini, G., Ciardiello, F., & de Vita, F. (2021). Enhanced Antitumor Effect of Trastuzumab and Duligotuzumab or Ipatasertib Combination in HER-2 Positive Gastric Cancer Cells. Cancers, 13(10), 2339. https://doi.org/10.3390/cancers13102339