

Quality of Life Factors in Adults with Eosinophilic Oesophagitis in New Zealand


Abstract
1. Introduction
The Study Hypothesised That
- Individuals who report active symptoms of EoE, as defined by a DSQ score ≥ 14, have a lower QoL compared with those with inactive disease (DSQ < 14)
- Factors such as dietary restrictions, food bolus obstruction, and female gender are associated with lower QoL, as defined by an EoE-QoL-A score less than the median score.
2. Methods
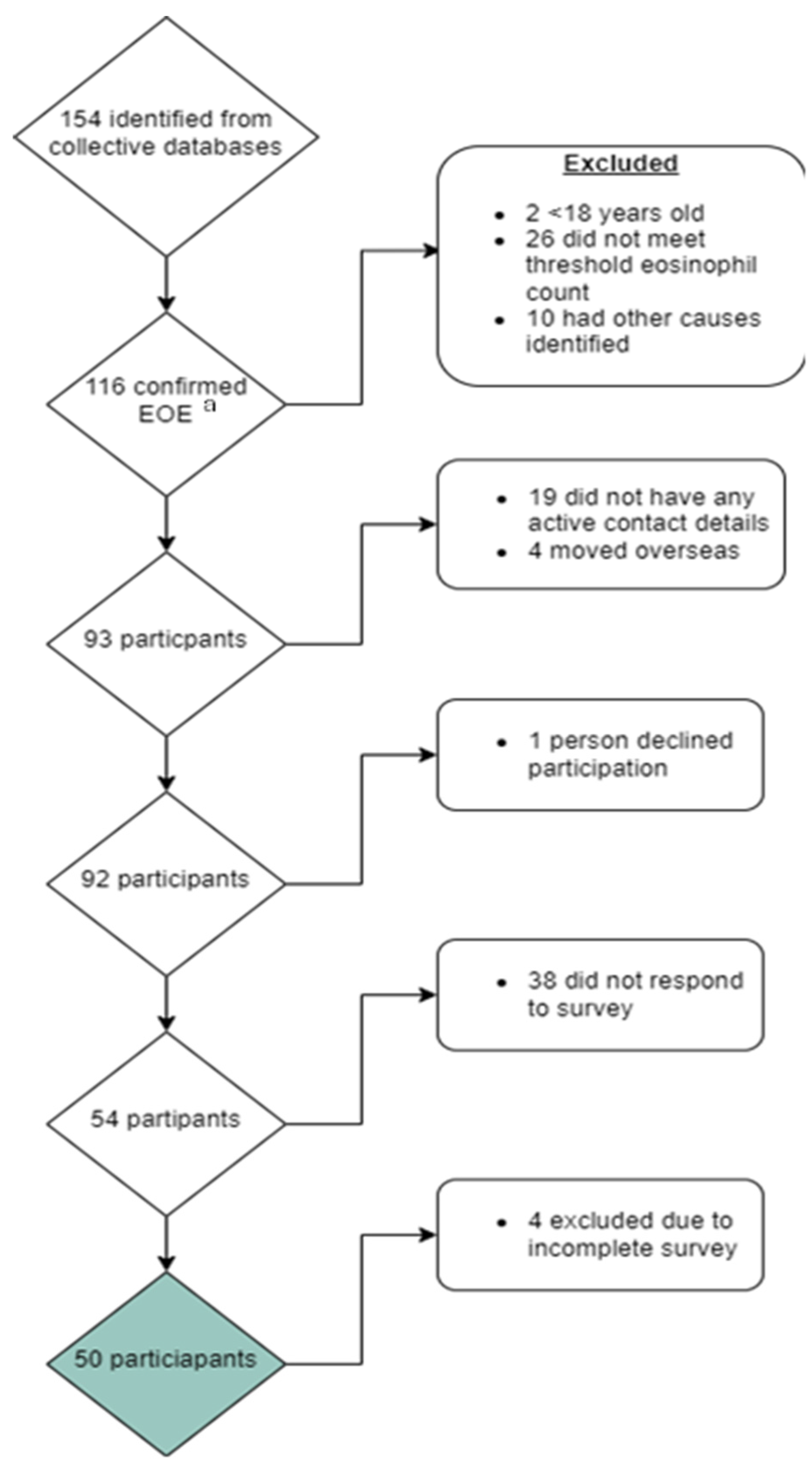
2.1. Study Participants
2.2. Study Related Questionnaires
2.3. Ethical Approval
2.4. Statistical Analyses
3. Results
Associations between Study Variables and EoE Disease Activity
4. Discussion
- Sample Size: Our sample size of 50 participants, although sufficient for preliminary insights, is relatively small and may restrict the generalisability of our findings.
- Absence of Set Normative Values for QoL and DSQ Scores: A significant challenge in our analysis was the lack of established normative values for the QoL and DSQ scores used. Their absence in our study may hinder the accurate interpretation and contextual understanding of our findings.
- Dichotomisation of DSQ and EoE-QoL-A Scores: The dichotomisation of the DSQ score in our study introduces a risk of misclassification, potentially skewing the correlation with QoL outcomes. This methodological approach may overlook subtle variations in disease severity and its impact on QoL. Similarly, the dichotomisation of EoE-QoL-A scores could simplify complex data, potentially overlooking critical aspects of patient experiences. Future research could explore alternative scoring methods to capture a more detailed spectrum of disease impact.
- Comparative Analysis with Known New Zealand QoL Data: Our findings, particularly the lower QoL scores in comparison with international studies, underscore the need for a comparative analysis with existing New Zealand QoL data. Such a comparison would not only validate our findings but also situate them within the unique healthcare and demographic landscape of New Zealand, offering vital insights for healthcare providers and policymakers.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Montoro-Huguet, M.A. Dietary and Nutritional Support in Gastrointestinal Diseases of the Upper Gastrointestinal Tract (I): Esophagus. Nutrients 2022, 14, 4819. [Google Scholar] [CrossRef] [PubMed]
- Dhar, A.; Haboubi, H.N.; Attwood, S.E.; Auth, M.K.H.; Dunn, J.M.; Sweis, R.; Morris, D.; Epstein, J.; Novelli, M.R.; Hunter, H.; et al. British Society of Gastroenterology (BSG) and British Society of Paediatric Gastroenterology, Hepatology and Nutrition (BSPGHAN) joint consensus guidelines on the diagnosis and management of eosinophilic oesophagitis in children and adults. Gut 2022, 71, 1459–1487. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, N.J.; Mukkada, V.; Eichinger, C.S.; Schofield, H.; Todorova, L.; Falk, G.W. Natural history of eosinophilic esophagitis: A systematic review of epidemiology and disease course. Dis. Esophagus 2018, 31, doy015. [Google Scholar] [CrossRef] [PubMed]
- Arias, Á.; Pérez-Martínez, I.; Tenías, J.M.; Lucendo, A.J. Systematic review with meta-analysis: The incidence and prevalence of eosinophilic oesophagitis in children and adults in population-based studies. Aliment. Pharmacol. Ther. 2016, 43, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Navarro, P.; Arias, Á.; Arias-González, L.; Laserna-Mendieta, E.J.; Ruiz-Ponce, M.; Lucendo, A.J. Systematic review with meta-analysis: The growing incidence and prevalence of eosinophilic oesophagitis in children and adults in population-based studies. Aliment. Pharmacol. Ther. 2019, 49, 1116–1125. [Google Scholar] [CrossRef]
- Weerasekera, K.; Sim, D.; Coughlan, F.; Inns, S. Eosinophilic esophagitis incidence in New Zealand: High but not increasing. Clin. Exp. Gastroenterol. 2019, 12, 367–374. [Google Scholar] [CrossRef]
- de Rooij, W.E.; Barendsen, M.E.; Warners, M.J.; van Rhijn, B.D.; Verheij, J.; Bruggink, A.H.; Bredenoord, A.J. Emerging incidence trends of eosinophilic esophagitis over 25 years: Results of a nationwide register-based pathology cohort. Neurogastroenterol. Motil. 2021, 33, e14072. [Google Scholar] [CrossRef]
- Hahn, J.W.; Lee, K.; Shin, J.I.; Cho, S.H.; Turner, S.; Shin, J.U.; Yeniova, A.; Koyanagi, A.; Jacob, L.; Smith, L.; et al. Global Incidence and Prevalence of Eosinophilic Esophagitis, 1976–2022: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2023, 21, 3270–3284.e77. [Google Scholar] [CrossRef] [PubMed]
- Schoepfer, A.M.; Safroneeva, E.; Bussmann, C.; Kuchen, T.; Portmann, S.; Simon, H.; Straumann, A. Delay in Diagnosis of Eosinophilic Esophagitis Increases Risk for Stricture Formation in a Time-Dependent Manner. Gastroenterology 2013, 145, 1230–1236.e2. [Google Scholar] [CrossRef]
- Mishra, A.; Wang, M.; Pemmaraju, V.R.; Collins, M.H.; Fulkerson, P.C.; Abonia, J.P.; Blanchard, C.; Putnam, P.E.; Rothenberg, M.E. Esophageal Remodeling Develops as a Consequence of Tissue Specific IL-5-Induced Eosinophilia. Gastroenterology 2008, 134, 204–214. [Google Scholar] [CrossRef]
- Aceves, S.S.; Newbury, R.O.; Dohil, R.; Bastian, J.F.; Broide, D.H. Esophageal remodeling in pediatric eosinophilic esophagitis. J. Allergy Clin. Immunol. 2007, 119, 206–212. [Google Scholar] [CrossRef]
- Visaggi, P.; Mariani, L.; Pardi, V.; Rosi, E.M.; Pugno, C.; Bellini, M.; Zingone, F.; Ghisa, M.; Marabotto, E.; Giannini, E.G.; et al. Dietary Management of Eosinophilic Esophagitis: Tailoring the Approach. Nutrients 2021, 13, 1630. [Google Scholar] [CrossRef]
- Dellon, E.S.; Gupta, S.K. A conceptual approach to understanding treatment response in eosinophilic esophagitis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2019, 17, 2149–2160. [Google Scholar] [CrossRef]
- Safroneeva, E.; Straumann, A.; Coslovsky, M.; Zwahlen, M.; Kuehni, C.E.; Panczak, R.; Haas, N.A.; Alexander, J.A.; Dellon, E.S.; Gonsalves, N.; et al. Symptoms Have Modest Accuracy in Detecting Endoscopic and Histologic Remission in Adults with Eosinophilic Esophagitis. Gastroenterology 2016, 150, 581–590.e4. [Google Scholar] [CrossRef]
- Safroneeva, E.; Coslovsky, M.; Kuehni, C.E.; Zwahlen, M.; Haas, N.A.; Panczak, R.; Taft, T.H.; Hirano, I.; Dellon, E.S.; Gonsalves, N.; et al. Eosinophilic oesophagitis: Relationship of quality of life with clinical, endoscopic and histological activity. Aliment. Pharmacol. Ther. 2015, 42, 1000–1010. [Google Scholar] [CrossRef] [PubMed]
- Molina-Infante, J. Nutritional and Psychological Considerations for Dietary Therapy in Eosinophilic Esophagitis. Nutrients 2022, 14, 1588. [Google Scholar] [CrossRef]
- Lucendo, A.J.; Arias-González, L.; Molina-Infante, J.; Arias, Á. Systematic review: Health-related quality of life in children and adults with eosinophilic oesophagitis-instruments for measurement and determinant factors. Aliment. Pharmacol. Ther. 2017, 46, 401–409. [Google Scholar] [CrossRef]
- Taft, T.H. When Not to Use a Generic: Measuring HRQoL in Chronic Digestive Disease Necessitates the Use of Disease-Specific Questionnaires. Dig. Dis. Sci. 2021, 66, 3219–3221. [Google Scholar] [CrossRef]
- Yarlas, A.; Maher, S.; Bayliss, M.; Lovley, A.; Cappelleri, J.C.; Bushmakin, A.G.; DiBonaventura, M.D. The Inflammatory Bowel Disease Questionnaire in Randomized Controlled Trials of Treatment for Ulcerative Colitis: Systematic Review and Meta-Analysis. J. Patient-Centered Res. Rev. 2020, 7, 189–205. [Google Scholar] [CrossRef]
- Ghisa, M.; Busa, F.; Barberio, B.; Tolone, S.; de Bortoli, N.; Laserra, G.; Zingone, F.; Savarino, V.; Savarino, E. Mo1204 Eosinophilic esophagitis quality of life questionnaire well correlates with disease activity and response to therapy in eosinophilic esophagitis patients. Gastroenterology 2020, 158 (Suppl. S1), S-826. [Google Scholar] [CrossRef]
- Lucendo, A.J.; Arias-González, L.; Molina-Infante, J.; Arias, Á. Determinant factors of quality of life in adult patients with eosinophilic esophagitis. United Eur. Gastroenterol. J. 2018, 6, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Hewett, R.; Alexakis, C.; Farmer, A.D.; Ainley, J.; Chhaya, V.; Hayat, J.O.; Poullis, A.; Kang, J.-Y. Effects of eosinophilic oesophagitis on quality of life in an adult UK population: A case control study. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2017, 30, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Pentiuk, S.; Putnam, P.E.; Collins, M.H.; Rothenberg, M.E. Dissociation between symptoms and histological severity in pediatric eosinophilic esophagitis. J. Pediatr. Gastroenterol. Nutr. 2009, 48, 152–160. [Google Scholar] [CrossRef]
- Straumann, A.; Conus, S.; Degen, L.; Frei, C.; Bussmann, C.; Beglinger, C.; Schoepfer, A.; Simon, H. Long-term budesonide maintenance treatment is partially effective for patients with eosinophilic esophagitis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2011, 9, 400–409.e1. [Google Scholar] [CrossRef]
- Alexander, J.A.; Jung, K.W.; Arora, A.S.; Enders, F.; Katzka, D.A.; Kephardt, G.M.; Kita, H.; Kryzer, L.A.; Romero, Y.; Smyrk, T.C.; et al. Swallowed fluticasone improves histologic but not symptomatic response of adults with eosinophilic esophagitis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2012, 10, 742–749.e1. [Google Scholar] [CrossRef]
- van Rhijn, B.D.; Smout, A.J.P.M.; Bredenoord, A.J. Disease duration determines health-related quality of life in adult eosinophilic esophagitis patients. Neurogastroenterol. Motil. 2014, 26, 772–778. [Google Scholar] [CrossRef]
- Taft, T.H.; Kern, E.; Keefer, L.; Burstein, D.; Hirano, I. Qualitative Assessment of Patient-reported Outcomes in Adults With Eosinophilic Esophagitis. J. Clin. Gastroenterol. 2011, 45, 769. [Google Scholar] [CrossRef]
- Rooij, W.E.d.; Evertsz, F.B.; Lei, A.; Bredenoord, A.J. General Well-being and Coping Strategies in Adult Eosinophilic Esophagitis Patients. J. Neurogastroenterol. Motil. 2022, 28, 390–400. [Google Scholar] [CrossRef]
- Schreiner, P.; Safroneeva, E.; Rossel, J.B.; Limacher, A.; Saner, C.; Greuter, T.; Schoepfer, A.; Straumann, A.; Biedermann, L. Sex Impacts Disease Activity But Not Symptoms or Quality of Life in Adults With Eosinophilic Esophagitis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2022, 20, 1729–1738.e1. [Google Scholar] [CrossRef]
- Kliewer, K.L.; Gonsalves, N.; Dellon, E.S.; A Katzka, D.; Abonia, J.P.; Aceves, S.S.; Arva, N.C.; A Besse, J.; A Bonis, P.; Caldwell, J.M.; et al. One-food versus six-food elimination diet therapy for the treatment of eosinophilic oesophagitis: A multicentre, randomised, open-label trial. Lancet Gastroenterol. Hepatol. 2023, 8, 408–421. [Google Scholar] [CrossRef]
- Pérez-Martínez, I.; Rodrigo, L.; Lucendo, A.J. Eosinophilic esophagitis: An evidenced-based approach to diagnosis and treatment. Med. Clin. 2019, 152, 444–449. [Google Scholar] [CrossRef]
- Chang, N.; Raja, S.; Betancourt, R.; Randall, C.; Keene, S.; Lilly, A.; Fowler, M.; Woosley, J.T.; Shaheen, N.J.; Dellon, E.S. Generic Measures of Quality of Life Are Not Correlated with Disease Activity in Eosinophilic Esophagitis. Dig. Dis. Sci. 2021, 66, 3312–3321. [Google Scholar] [CrossRef] [PubMed]
- Dellon, E.S.; Liacouras, C.A.; Molina-Infante, J.; Furuta, G.T.; Spergel, J.M.; Zevit, N.; Spechler, S.J.; Attwood, S.E.; Straumann, A.; Aceves, S.S.; et al. Updated International Consensus Diagnostic Criteria for Eosinophilic Esophagitis: Proceedings of the AGREE Conference. Gastroenterology 2018, 155, 1022–1033.e10. [Google Scholar] [CrossRef] [PubMed]
- Hirano, I.; Moy, N.; Heckman, M.G.; Thomas, C.S.; Gonsalves, N.; Achem, S.R. Endoscopic assessment of the oesophageal features of eosinophilic oesophagitis: Validation of a novel classification and grading system. Gut 2013, 62, 489–495. [Google Scholar] [CrossRef]
- Cristofori, F.; D’Abramo, F.S.; Rutigliano, V.; Dargenio, V.N.; Castellaneta, S.; Piscitelli, D.; De Benedittis, D.; Indrio, F.; Raguseo, L.C.; Barone, M.; et al. Esophageal Eosinophilia and Eosinophilic Esophagitis in Celiac Children: A Ten Year Prospective Observational Study. Nutrients 2021, 13, 3755. [Google Scholar] [CrossRef]
- Dellon, E.S.; Irani, A.M.; Hill, M.R.; Hirano, I. Development and field testing of a novel patient-reported outcome measure of dysphagia in patients with eosinophilic esophagitis. Aliment. Pharmacol. Ther. 2013, 38, 634–642. [Google Scholar] [CrossRef]
- Hudgens, S.; Evans, C.; Phillips, E.; Hill, M. Psychometric validation of the Dysphagia Symptom Questionnaire in patients with eosinophilic esophagitis treated with budesonide oral suspension. J. Patient-Rep. Outcomes 2017, 1, 3. [Google Scholar] [CrossRef]
- Taft, T.H.; Kern, E.; Kwiatek, M.A.; Hirano, I.; Gonsalves, N.; Keefer, L. The adult eosinophilic oesophagitis quality of life questionnaire: A new measure of health-related quality of life. Aliment. Pharmacol. Ther. 2011, 34, 790–798. [Google Scholar] [CrossRef]
- Stern, E.; Taft, T.; Zalewski, A.; Gonsalves, N.; Hirano, I. Prospective assessment of disease-specific quality of life in adults with eosinophilic esophagitis. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus 2018, 31, dox128. [Google Scholar] [CrossRef]
- Colonoscopy Wait Times NZ 2022. Available online: https://www.policywise.co.nz/resources/colonoscopy (accessed on 23 August 2024).
- Alhmoud, T.; Ghazaleh, S.; Ghanim, M.; Redfern, R.E. The Risk of Esophageal Food Impaction in Eosinophilic Esophagitis Patients: The Role of Clinical and Socioeconomic Factors. Clin. Exp. Gastroenterol. 2022, 15, 153–161. [Google Scholar] [CrossRef]
- Attwood, S.; Epstein, J. Eosinophilic oesophagitis: Recent advances and practical management. Frontline Gastroenterol. 2021, 12, 644–649. [Google Scholar] [CrossRef] [PubMed]
- Gyimah, D.A.; Khan, H.; Abdalla, B.; Haboubi, H. 171. Delayed diagnosis of eosinophilic esophagitis in those presenting to the emergency department with food bolus impaction. Dis. Esophagus 2022, 35 (Suppl. S2), doac051.171. [Google Scholar] [CrossRef]
- Corsello, A.; Pugliese, D.; Gasbarrini, A.; Armuzzi, A. Diet and Nutrients in Gastrointestinal Chronic Diseases. Nutrients 2020, 12, 2693. [Google Scholar] [CrossRef]
- Rossi, C.M.; Lenti, M.V.; Merli, S.; Cena, H.; Di Sabatino, A. Dietary Strategies in Adult Patients with Eosinophilic Esophagitis: A State-of-the-Art Review. Nutrients 2023, 15, 2409. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Score Range | |
|---|---|
| Overall Score | 0–96 |
| Eating/Diet Impact | 0–16 |
| Social Impact | 0–16 |
| Emotional Impact | 0–32 |
| Disease anxiety | 0–20 |
| Swallowing anxiety | 0–12 |
| Characteristics | Total Participants (n = 50) |
|---|---|
| Median Age (IQR) | 47 years (42–58) |
| Female participants (%) | 11 (22) |
| European participants (%) | 41 (82) |
| Previous food bolus admissions (%) | 33 (66) |
| Steroid use (oral or topical; %) | 7 (14) |
| Proton pump inhibitor use (%) | 30 (60) |
| Six food elimination diet (%) | 3 (6) |
| Median DSQ (IQR) | 49 (0–60) |
| Active EoE (DSQ ≥ 14, %) | 31 (62.0) |
| Median EoO-QOL-A (IQR) | 68 (48–80) |
| Impaired QoL, EoE-QOL-A < 68 (%) | 25 (50.0) |
| Median eating and diet QoL (IQR) | 10 (7–13) |
| Median social QoL (IQR) | 9 (5–13) |
| Median emotional QoL (IQR) | 26 (20–28) |
| Median disease anxiety QoL (IQR) | 14 (10–18) |
| Median swallowing anxiety QoL (IQR) | 8 (5–9) |
| Median DSQ Score Group 1 | Median DSQ Score Group 2 | p-Value | |
|---|---|---|---|
| Gender (Male = 1, female = 2) | 49 (0–56) | 56 (14–70) | 0.29 |
| Atopy/allergy/asthma (No = 1 vs. Yes = 2) | 49 (0–56) | 28 (0–70) | 1 |
| Oral/topical steroid use (No = 1 vs. Yes = 2) | 42 (0–56) | 70 (56–84) | 0.02 |
| Proton pump inhibitor use (No = 1 vs. Yes = 2) | 56 (42–70) | 7 (0–56) | 0.01 |
| History of food bolus obstruction (1 = No 2 = Yes) | 66 (0–63) | 42 (0–63) | 0.86 |
| All Participants (N = 50) | ||||||
|---|---|---|---|---|---|---|
| DSQ Score | EoE-QOL-A | Eating/Diet | Social Impact | Emotional Impact | Disease Anxiety | |
| EoE QoL | −0.37 ** | |||||
| Eating/diet | −0.54 *** | 0.87 *** | ||||
| Social impact | −0.30 * | 0.90 *** | 0.77 *** | |||
| Emotional impact | −0.44 ** | 0.94 *** | 0.82 *** | 0.82 *** | ||
| Disease anxiety | −0.20 | 0.84 *** | 0.65 *** | 0.67 *** | 0.74 *** | |
| Swallowing anxiety | −0.19 | 0.80 *** | 0.66 *** | 0.72 *** | 0.67 *** | 0.63 *** |
| Median EoE-QOL-A (IQR) Group 1 | Median EoE-QOL-A (IQR) Group 2 | p-Value | |
|---|---|---|---|
| Gender (Male = 1 vs. female = 2) | 70 (51–81) | 58 (40–75) | 0.11 |
| Comorbidities (No = 1 vs. Yes = 2) | 71 (50–80) | 67 (46–80) | 0.86 |
| Atopy/allergy/asthma (No = 1 vs. Yes = 2) | 71 (50–80) | 60 (45–84) | 0.56 |
| Oral/topical steroid use (No = 1 vs. Yes = 2) | 69 (50–80) | 54 (47–76) | 0.34 |
| Proton pump inhibitor use (No = 1 vs. Yes = 2) | 60 (45–74) | 75 (53–83) | 0.02 |
| Active disease (No = 1 vs. Yes = 1) | 75 (62–89) | 59 (46–76) | 0.02 |
| History of food bolus obstruction (1 = No 2 = Yes) | 66 (49–79) | 73 (48–81) | 0.71 |
| Odds Ratio | 95% CI | |
|---|---|---|
| Age | 0.97 | 0.93–1.01 |
| Female | 1.96 | 0.49–7.87 |
| Presence of any comorbidities | 1.38 | 0.45–4.20 |
| History of atopy | 3.63 | 0.66–20.12 |
| Steroids use | 2.88 | 0.50–16.48 |
| Proton pump inhibitor use | 0.36 | 0.11–1.16 |
| Food elimination use | 0.48 | 0.04–5.65 |
| DSQ score | 1.02 | 1.002–1.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McGarrigle, V.; Swaminathan, A.; Inns, S.J. Quality of Life Factors in Adults with Eosinophilic Oesophagitis in New Zealand. Nutrients 2024, 16, 3437. https://doi.org/10.3390/nu16203437
McGarrigle V, Swaminathan A, Inns SJ. Quality of Life Factors in Adults with Eosinophilic Oesophagitis in New Zealand. Nutrients. 2024; 16(20):3437. https://doi.org/10.3390/nu16203437
Chicago/Turabian StyleMcGarrigle, Vicki, Akhilesh Swaminathan, and Stephen James Inns. 2024. "Quality of Life Factors in Adults with Eosinophilic Oesophagitis in New Zealand" Nutrients 16, no. 20: 3437. https://doi.org/10.3390/nu16203437
APA StyleMcGarrigle, V., Swaminathan, A., & Inns, S. J. (2024). Quality of Life Factors in Adults with Eosinophilic Oesophagitis in New Zealand. Nutrients, 16(20), 3437. https://doi.org/10.3390/nu16203437