
Stool Gluten Peptide Detection Is Superior to Urinary Analysis, Coeliac Serology, Dietary Adherence Scores and Symptoms in the Detection of Intermittent Gluten Exposure in Coeliac Disease: A Randomised, Placebo-Controlled, Low-Dose Gluten Challenge Study

 , and
, and
Abstract

1. Introduction
2. Materials and Methods
2.1. Overall Study Design
2.2. Ethics Statement
2.3. Participants
2.4. Run-in Period
2.5. Gluten or Placebo Cookies
2.6. Cookie Randomisation
2.7. Cookie Ingestion
2.8. Stool Collection
2.9. Symptom Record
2.10. Quantification of GIP in Stool
2.11. Analytical Performance
2.12. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Baseline Stool and Urine GIP
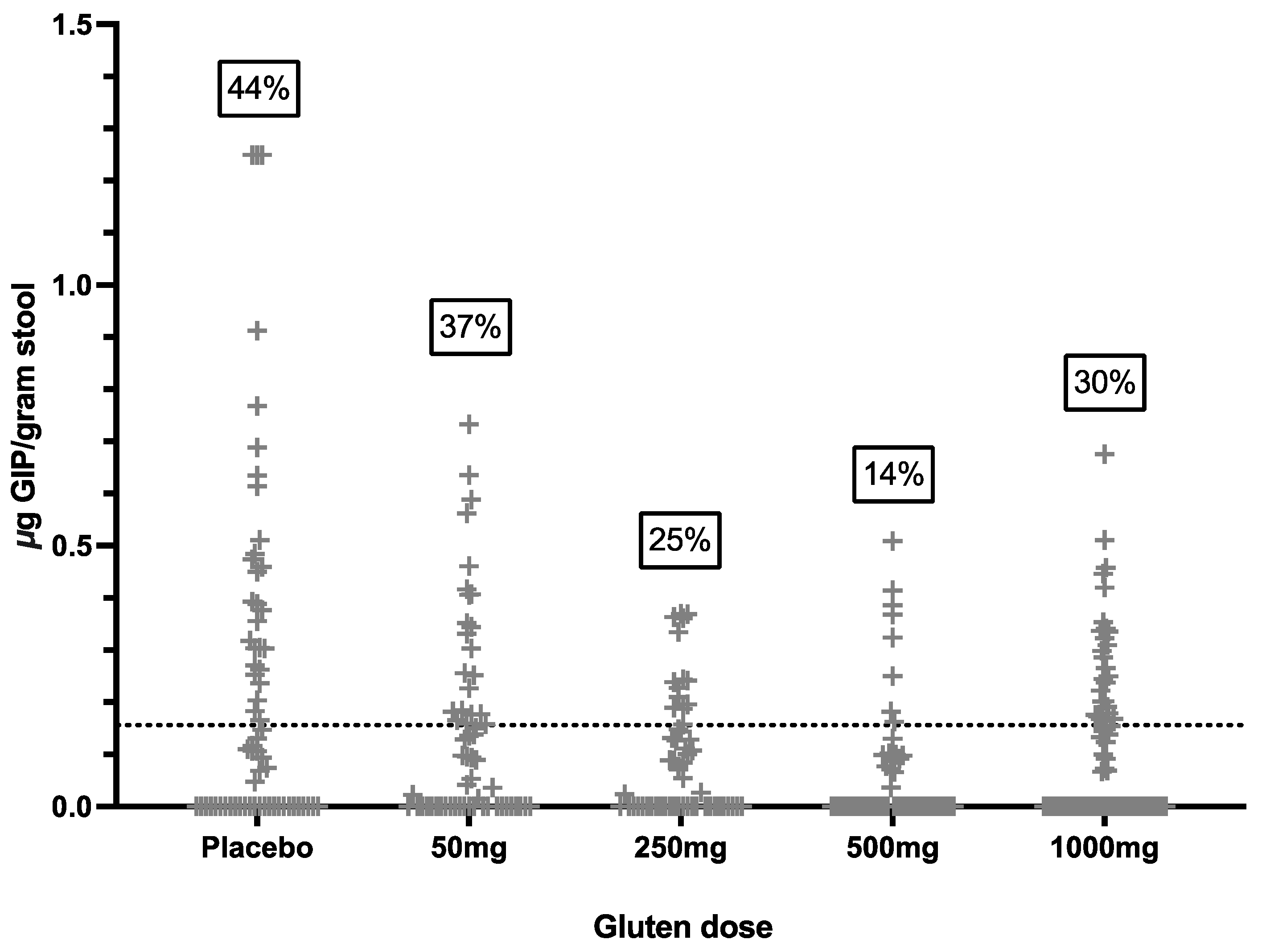
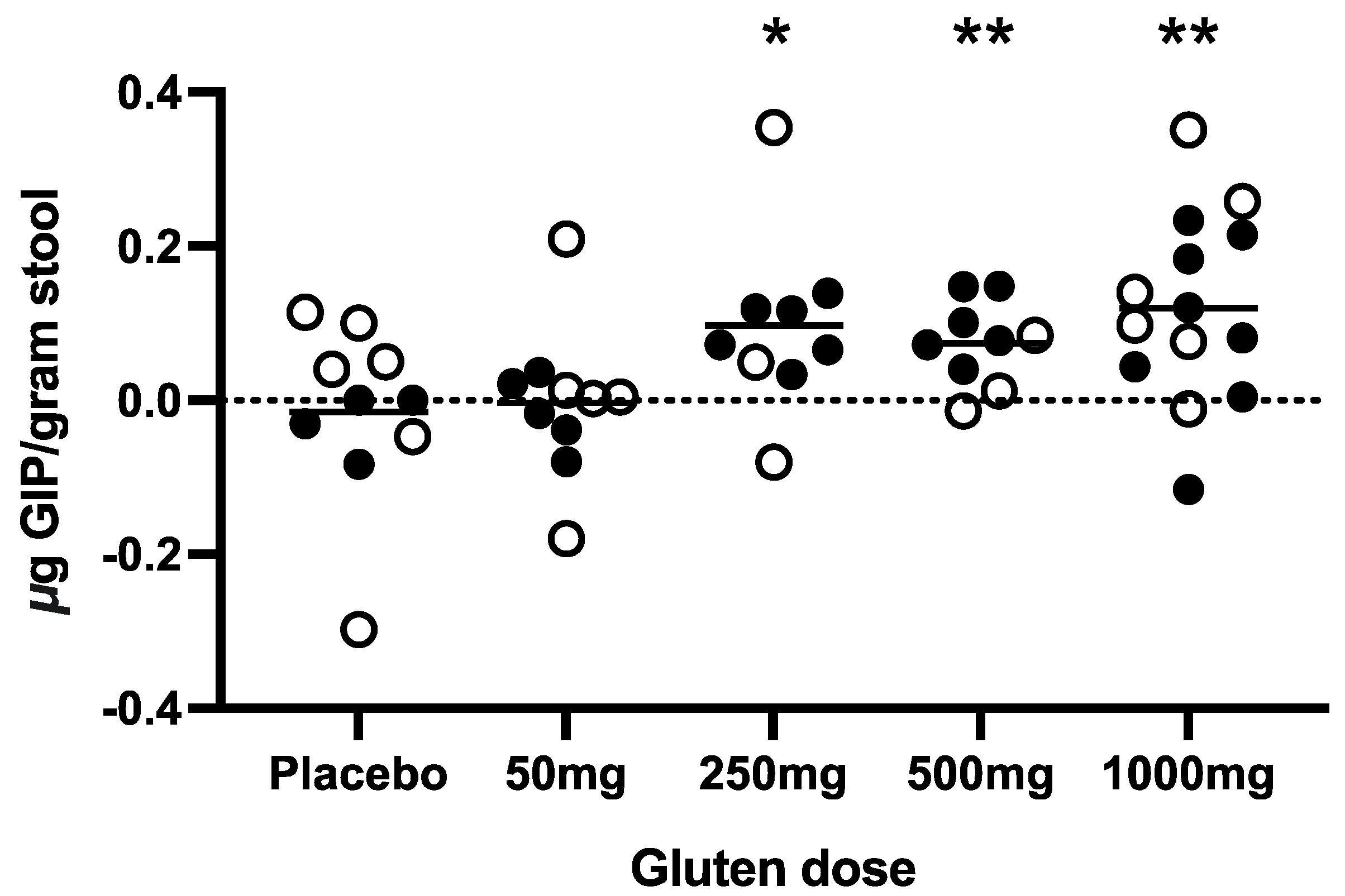
3.3. Stool GIP after Cookie Ingestion
3.4. Symptoms after Cookie Challenge
3.5. Correlation of Gluten Intake with Symptoms, Dietary Adherence Score and Coeliac Serology
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Tye-Din, J.A. Review article: Follow-up of coeliac disease. Aliment. Pharmacol. Ther. 2022, 56 (Suppl. S1), S49–S63. [Google Scholar] [CrossRef]
- Mearns, E.S.; Taylor, A.; Boulanger, T.; Craig, K.J.; Gerber, M.; Leffler, D.A.; Drahos, J.; Sanders, D.S.; Lebwohl, B. Systematic Literature Review of the Economic Burden of Celiac Disease. Pharmacoeconomics 2019, 37, 45–61. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Akbari, M.; Vanga, R.; Kelly, C.P.; Hansen, J.; Theethira, T.; Tariq, S.; Dennis, M.; Leffler, D.A. Patient perception of treatment burden is high in celiac disease compared with other common conditions. Am. J. Gastroenterol. 2014, 109, 1304–1311. [Google Scholar] [CrossRef]
- Falcomer, A.L.; Santos Araujo, L.; Farage, P.; Santos Monteiro, J.; Yoshio Nakano, E.; Puppin Zandonadi, R. Gluten contamination in food services and industry: A systematic review. Crit. Rev. Food Sci. Nutr. 2020, 60, 479–493. [Google Scholar] [CrossRef]
- Halmos, E.P.; Di Bella, C.A.; Webster, R.; Deng, M.; Tye-Din, J.A. Gluten in “gluten-free” food from food outlets in Melbourne: A cross-sectional study. Med. J. Aust. 2018, 209, 42–43. [Google Scholar] [CrossRef]
- Penny, H.A.; Rej, A.; Baggus, E.M.R.; Coleman, S.H.; Ward, R.; Wild, G.; Bouma, G.; Trott, N.; Snowden, J.A.; Wright, J.; et al. Non-Responsive and Refractory Coeliac Disease: Experience from the NHS England National Centre. Nutrients 2022, 14, 2776. [Google Scholar] [CrossRef]
- Silvester, J.A.; Kurada, S.; Szwajcer, A.; Kelly, C.P.; Leffler, D.A.; Duerksen, D.R. Tests for Serum Transglutaminase and Endomysial Antibodies Do Not Detect Most Patients with Celiac Disease and Persistent Villous Atrophy on Gluten-free Diets: A Meta-analysis. Gastroenterology 2017, 153, 689–701.e1. [Google Scholar] [CrossRef]
- Coleman, S.H.; Rej, A.; Baggus, E.M.R.; Lau, M.S.; Marks, L.J.; Hadjivassiliou, M.; Cross, S.S.; Leffler, D.A.; Elli, L.; Sanders, D.S. What is the Optimal Method Assessing for Persistent Villous Atrophy in Adult Coeliac Disease? J. Gastrointestin. Liver Dis. 2021, 30, 205–212. [Google Scholar] [CrossRef]
- Mahadev, S.; Murray, J.A.; Wu, T.T.; Chandan, V.S.; Torbenson, M.S.; Kelly, C.P.; Maki, M.; Green, P.H.; Adelman, D.; Lebwohl, B. Factors associated with villus atrophy in symptomatic coeliac disease patients on a gluten-free diet. Aliment. Pharmacol. Ther. 2017, 45, 1084–1093. [Google Scholar] [CrossRef] [PubMed]
- Moreno, M.L.; Rodriguez-Herrera, A.; Sousa, C.; Comino, I. Biomarkers to Monitor Gluten-Free Diet Compliance in Celiac Patients. Nutrients 2017, 9, 46. [Google Scholar] [CrossRef]
- Comino, I.; Segura, V.; Ortigosa, L.; Espin, B.; Castillejo, G.; Garrote, J.A.; Sierra, C.; Millan, A.; Ribes-Koninckx, C.; Roman, E.; et al. Prospective longitudinal study: Use of faecal gluten immunogenic peptides to monitor children diagnosed with coeliac disease during transition to a gluten-free diet. Aliment. Pharmacol. Ther. 2019, 49, 1484–1492. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.F.; Sugai, E.; Temprano, M.P.; Niveloni, S.I.; Vazquez, H.; Moreno, M.L.; Dominguez-Flores, M.R.; Munoz-Suano, A.; Smecuol, E.; Stefanolo, J.P.; et al. Gluten immunogenic peptide excretion detects dietary transgressions in treated celiac disease patients. World J. Gastroenterol. 2019, 25, 1409–1420. [Google Scholar] [CrossRef] [PubMed]
- Silvester, J.A.; Comino, I.; Kelly, C.P.; Sousa, C.; Duerksen, D.R.; Bernstein, C.N.; Cebolla, A.; Dominguez, M.R.; Graff, L.A.; Green, K.H.; et al. Most Patients With Celiac Disease on Gluten-Free Diets Consume Measurable Amounts of Gluten. Gastroenterology 2020, 158, 1497–1499.e1. [Google Scholar] [CrossRef]
- Silvester, J.A.; Comino, I.; Rigaux, L.N.; Segura, V.; Green, K.H.; Cebolla, A.; Weiten, D.; Dominguez, R.; Leffler, D.A.; Leon, F.; et al. Exposure sources, amounts and time course of gluten ingestion and excretion in patients with coeliac disease on a gluten-free diet. Aliment. Pharmacol. Ther. 2020, 52, 1469–1479. [Google Scholar] [CrossRef]
- Fernandez-Banares, F.; Beltran, B.; Salas, A.; Comino, I.; Ballester-Clau, R.; Ferrer, C.; Molina-Infante, J.; Rosinach, M.; Modolell, I.; Rodriguez-Moranta, F.; et al. Persistent Villous Atrophy in De Novo Adult Patients with Celiac Disease and Strict Control of Gluten-Free Diet Adherence: A Multicenter Prospective Study (CADER Study). Am. J. Gastroenterol. 2021, 116, 1036–1043. [Google Scholar] [CrossRef]
- Stefanolo, J.P.; Talamo, M.; Dodds, S.; de la Paz Temprano, M.; Costa, A.F.; Moreno, M.L.; Pinto-Sanchez, M.I.; Smecuol, E.; Vazquez, H.; Gonzalez, A.; et al. Real-World Gluten Exposure in Patients with Celiac Disease on Gluten-Free Diets, Determined From Gliadin Immunogenic Peptides in Urine and Fecal Samples. Clin. Gastroenterol. Hepatol. 2021, 19, 484–491.e1. [Google Scholar] [CrossRef] [PubMed]
- Coto, L.; Sousa, C.; Cebolla, A. Individual variability in patterns and dynamics of fecal gluten immunogenic peptides excretion after low gluten intake. Eur. J. Nutr. 2022, 61, 2033–2049. [Google Scholar] [CrossRef]
- Burger, J.P.W.; van Lochem, E.G.; Roovers, E.A.; Drenth, J.P.H.; Wahab, P.J. Dose-Escalating (50–500 mg) Gluten Administration Leads to Detectable Gluten-Immunogenic-Peptides in Urine of Patients with Coeliac Disease Which Is Unrelated to Symptoms, a Placebo Controlled Trial. Nutrients 2022, 14, 1771. [Google Scholar] [CrossRef]
- Leffler, D.A.; Dennis, M.; Edwards George, J.B.; Jamma, S.; Magge, S.; Cook, E.F.; Schuppan, D.; Kelly, C.P. A simple validated gluten-free diet adherence survey for adults with celiac disease. Clin. Gastroenterol. Hepatol. 2009, 7, 530–536.e2. [Google Scholar] [CrossRef] [PubMed]
- Svedlund, J.; Sjodin, I.; Dotevall, G. GSRS—A clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig. Dis. Sci. 1988, 33, 129–134. [Google Scholar] [CrossRef]
- Leffler, D.A.; Kelly, C.P.; Green, P.H.; Fedorak, R.N.; DiMarino, A.; Perrow, W.; Rasmussen, H.; Wang, C.; Bercik, P.; Bachir, N.M.; et al. Larazotide acetate for persistent symptoms of celiac disease despite a gluten-free diet: A randomized controlled trial. Gastroenterology 2015, 148, 1311–1319.e6. [Google Scholar] [CrossRef]
- Comino, I.; Fernandez-Banares, F.; Esteve, M.; Ortigosa, L.; Castillejo, G.; Fambuena, B.; Ribes-Koninckx, C.; Sierra, C.; Rodriguez-Herrera, A.; Salazar, J.C.; et al. Fecal Gluten Peptides Reveal Limitations of Serological Tests and Food Questionnaires for Monitoring Gluten-Free Diet in Celiac Disease Patients. Am. J. Gastroenterol. 2016, 111, 1456–1465. [Google Scholar] [CrossRef]
- Therrien, A.; Leffler, D.A. Gluten immunogenic peptides: Is knowing half the battle? Am. J. Clin. Nutr. 2020, 112, 1147–1148. [Google Scholar] [CrossRef]
- Moreno, M.L.; Cebolla, A.; Munoz-Suano, A.; Carrillo-Carrion, C.; Comino, I.; Pizarro, A.; Leon, F.; Rodriguez-Herrera, A.; Sousa, C. Detection of gluten immunogenic peptides in the urine of patients with coeliac disease reveals transgressions in the gluten-free diet and incomplete mucosal healing. Gut 2017, 66, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Radcliffe, S.; Sutzko, M.; Jiang, Z.; Freitag, D.; Swoboda, C.; Frank, L.; Rogers, A. Validation of the AgraStrip(R) gluten G12 test kit. J. AOAC Int. 2014, 97, 1638–1650. [Google Scholar] [CrossRef] [PubMed]
- Moron, B.; Cebolla, A.; Manyani, H.; Alvarez-Maqueda, M.; Megias, M.; Thomas Mdel, C.; Lopez, M.C.; Sousa, C. Sensitive detection of cereal fractions that are toxic to celiac disease patients by using monoclonal antibodies to a main immunogenic wheat peptide. Am. J. Clin. Nutr. 2008, 87, 405–414. [Google Scholar] [CrossRef]
- van Megen, F.; Skodje, G.I.; Lergenmuller, S.; Zuhlke, S.; Aabakken, L.; Veierod, M.B.; Henriksen, C.; Lundin, K.E.A. A Low FODMAP Diet Reduces Symptoms in Treated Celiac Patients with Ongoing Symptoms—A Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2022, 20, 2258–2266.e3. [Google Scholar] [CrossRef] [PubMed]
- Daveson, A.J.M.; Tye-Din, J.A.; Goel, G.; Goldstein, K.E.; Hand, H.L.; Neff, K.M.; Williams, L.J.; Truitt, K.E.; Anderson, R.P.; Group, R.C.S. Masked bolus gluten challenge low in FODMAPs implicates nausea and vomiting as key symptoms associated with immune activation in treated coeliac disease. Aliment. Pharmacol. Ther. 2020, 51, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Silvester, J.A.; Graff, L.A.; Rigaux, L.; Walker, J.R.; Duerksen, D.R. Symptomatic suspected gluten exposure is common among patients with coeliac disease on a gluten-free diet. Aliment. Pharmacol. Ther. 2016, 44, 612–619. [Google Scholar] [CrossRef]
- Silvester, J.A.; Graff, L.A.; Rigaux, L.; Bernstein, C.N.; Leffler, D.A.; Kelly, C.P.; Walker, J.R.; Duerksen, D.R. Symptoms of Functional Intestinal Disorders Are Common in Patients with Celiac Disease Following Transition to a Gluten-Free Diet. Dig. Dis. Sci. 2017, 62, 2449–2454. [Google Scholar] [CrossRef] [PubMed]
- Sainsbury, A.; Sanders, D.S.; Ford, A.C. Prevalence of irritable bowel syndrome-type symptoms in patients with celiac disease: A meta-analysis. Clin. Gastroenterol. Hepatol. 2013, 11, 359–365.e1. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.A.; Syage, J.A.; Wu, T.T.; Dickason, M.A.; Ramos, A.G.; Van Dyke, C.; Horwath, I.; Lavin, P.T.; Maki, M.; Hujoel, I.; et al. Latiglutenase Protects the Mucosa and Attenuates Symptom Severity in Patients with Celiac Disease Exposed to a Gluten Challenge. Gastroenterology 2022, 163, 1510–1521.e6. [Google Scholar] [CrossRef] [PubMed]
- Garzon-Benavides, M.; Ruiz-Carnicer, A.; Segura, V.; Fombuena, B.; Garcia-Fernandez, F.; Sobrino-Rodriguez, S.; Gomez-Izquierdo, L.; Montes-Cano, M.A.; Millan-Dominguez, R.; Del Carmen Rico, M.; et al. Clinical utility of urinary gluten immunogenic peptides in the follow-up of patients with coeliac disease. Aliment. Pharmacol. Ther. 2023, 57, 993–1003. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cookie (Placebo) | Cookie (Gluten 50 mg) | Cookie (Gluten 250 mg) | Cookie (Gluten 500 mg) | Cookie (Gluten 1000 mg) | All | p Value | |
|---|---|---|---|---|---|---|---|
| N = 10 | N = 10 | N = 9 | N = 9 | N = 14 | N = 52 | ||
| Median age (IQR), y | 63 (61–66) | 57 (46–65) | 53 (36–60) | 47 (36–50) | 53 (40–62) | 55 (44–62) | 0.026 * |
| Median age at diagnosis (IQR), y | 49 (46–54) | 52 (33–61) | 33 (24–45) | 41 (30–49) | 44 (28–48) | 46 (32–51) | 0.088 |
| Median time on GFD (IQR), y | 14 (9–17) | 5 (4–9) | 12 (10–20) | 3 (2–6) | 11 (4–14) | 10 (5–14) | 0.013 ^ |
| Females, n (%) | 7 (70) | 7 (70) | 5 (56) | 5 (56) | 12 (86) | 36 (69) | 0.498 |
| HLA genotype, n (%) | |||||||
| DQ2/x | 9 (90) | 8 (80) | 7 (78) | (7) 78 | 13 (93) | 44 (85) | 0.387 |
| DQ2/8 | 1 (10) | 0 (0) | 2 (22) | 0 (0) | 1 (7) | 4 (8) | |
| DQ8/x | 0 (0) | 2 (20) | 0 (0) | 1 (11) | 0 (0) | 3 (6) | |
| Unknown | 0 (0) | 0 (0) | 0 (0) | 1 (11) | 0 (0) | 1 (2) | |
| Baseline assessments | |||||||
| Median symptoms (GSRS) | 1.3 | 1.1 | 1.6 | 1.5 | 1.4 | 1.3 | 0.270 |
| Median adherence (CDAT) | 10 | 9 | 13 | 10 | 10 | 10 | 0.618 |
| tTG-IgA serology (negative %) | 100 | 100 | 100 | 100 | 100 | 100 | |
| DGP-IgG serology (negative %) | 100 | 100 | 100 | 100 | 100 | 100 | |
| Urine GIP (negative, %) | 100 | 100 | 100 | 100 | 100 | 100 | |
| Mean bowel movements per day (IQR) | 1.8 (1.2–1.9) | 1.4 (1.0–1.6) | 1.4 (1.2–1.6) | 1.4 (1.0–1.6) | 1.3 (0.9–1.8) | 1.5 (1.0–1.7) | 0.367 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russell, A.K.; Lucas, E.C.; Henneken, L.M.; Pizzey, C.J.; Clarke, D.; Myleus, A.; Tye-Din, J.A. Stool Gluten Peptide Detection Is Superior to Urinary Analysis, Coeliac Serology, Dietary Adherence Scores and Symptoms in the Detection of Intermittent Gluten Exposure in Coeliac Disease: A Randomised, Placebo-Controlled, Low-Dose Gluten Challenge Study. Nutrients 2024, 16, 279. https://doi.org/10.3390/nu16020279
Russell AK, Lucas EC, Henneken LM, Pizzey CJ, Clarke D, Myleus A, Tye-Din JA. Stool Gluten Peptide Detection Is Superior to Urinary Analysis, Coeliac Serology, Dietary Adherence Scores and Symptoms in the Detection of Intermittent Gluten Exposure in Coeliac Disease: A Randomised, Placebo-Controlled, Low-Dose Gluten Challenge Study. Nutrients. 2024; 16(2):279. https://doi.org/10.3390/nu16020279
Chicago/Turabian StyleRussell, Amy K., Erin C. Lucas, Lee M. Henneken, Catherine J. Pizzey, Dean Clarke, Anna Myleus, and Jason A. Tye-Din. 2024. "Stool Gluten Peptide Detection Is Superior to Urinary Analysis, Coeliac Serology, Dietary Adherence Scores and Symptoms in the Detection of Intermittent Gluten Exposure in Coeliac Disease: A Randomised, Placebo-Controlled, Low-Dose Gluten Challenge Study" Nutrients 16, no. 2: 279. https://doi.org/10.3390/nu16020279
APA StyleRussell, A. K., Lucas, E. C., Henneken, L. M., Pizzey, C. J., Clarke, D., Myleus, A., & Tye-Din, J. A. (2024). Stool Gluten Peptide Detection Is Superior to Urinary Analysis, Coeliac Serology, Dietary Adherence Scores and Symptoms in the Detection of Intermittent Gluten Exposure in Coeliac Disease: A Randomised, Placebo-Controlled, Low-Dose Gluten Challenge Study. Nutrients, 16(2), 279. https://doi.org/10.3390/nu16020279