

The Prevalence of Disordered Eating Behaviours (DEBs) among Adolescent Female School Students in Riyadh, Saudi Arabia: A Cross-Sectional Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants and Recruitment
2.3. Procedure
2.4. Anthropometric Data
2.5. Questionnaire: Eating Attitudes Test (EAT-26)
2.6. Data Analysis
3. Results
3.1. Demographic Characteristics
3.2. EAT-26 Scores
3.3. EAT-26 Subscales (Dieting, Oral Control and Bulimia and Food Preoccupation)
3.4. Behavioural Questions
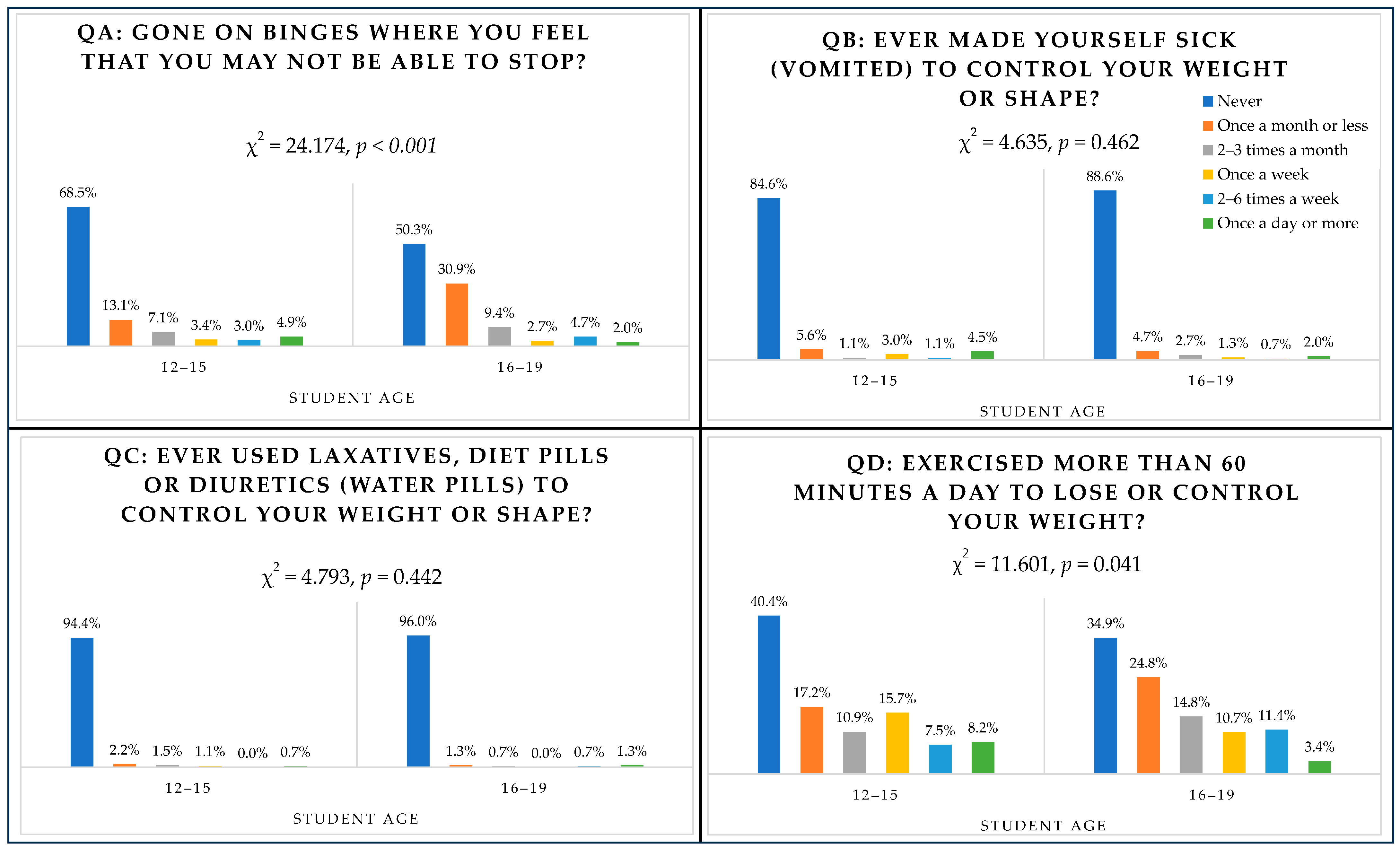
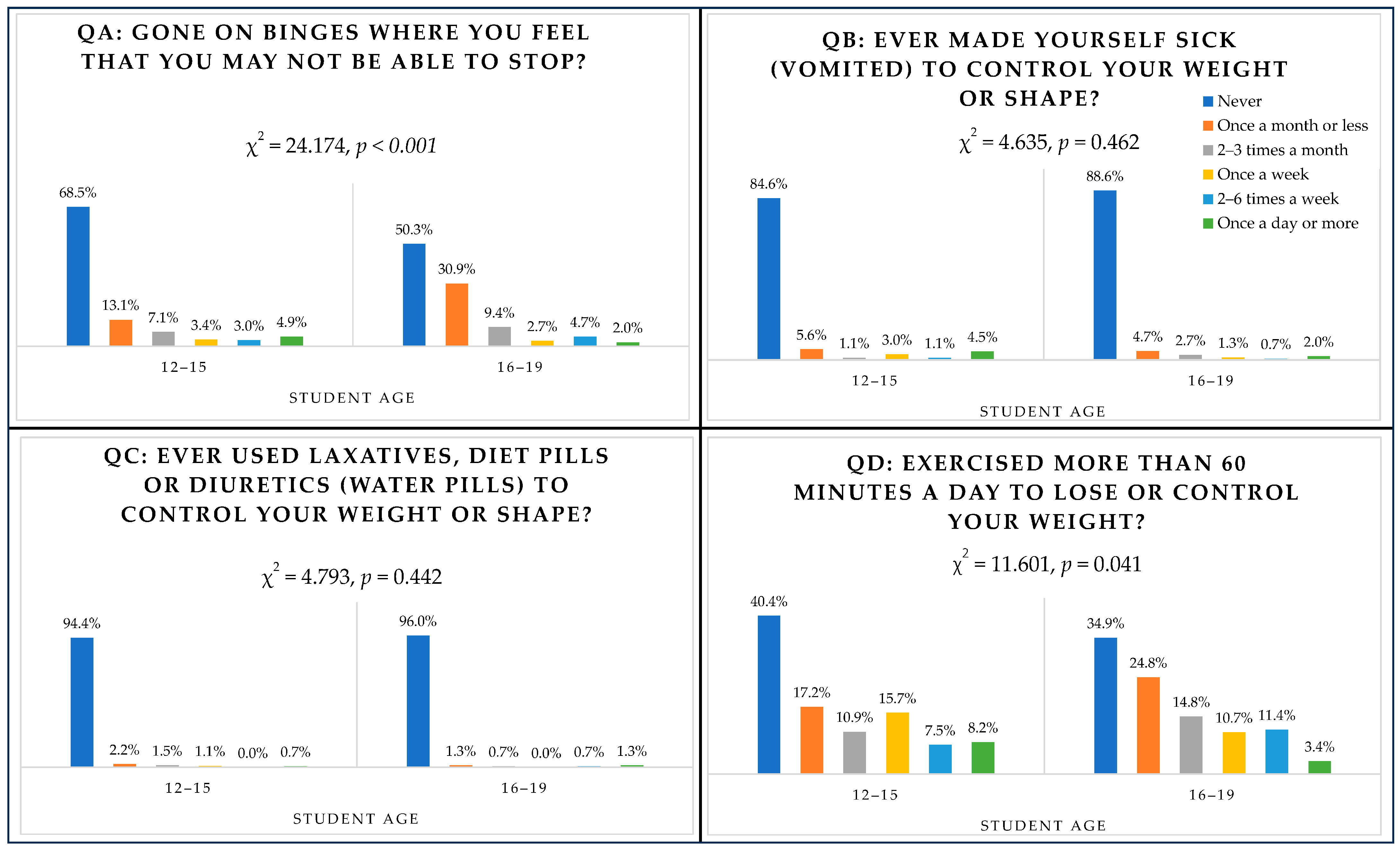
3.5. Behavioural Questions (QA Binge Eating, QB Vomiting, QC Laxatives, QD Exercising) and Age
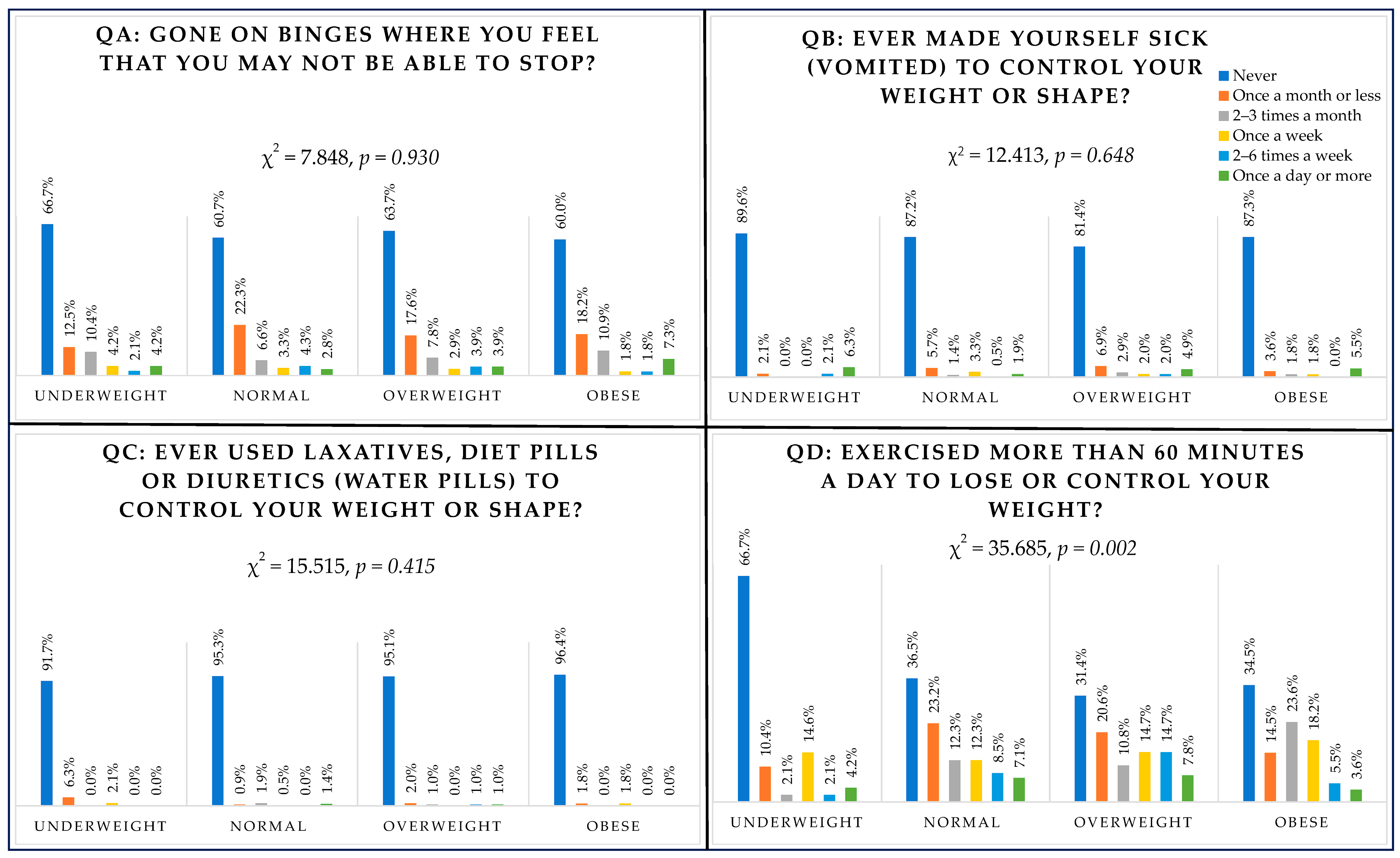
3.6. Behavioural Questions (QA Binge Eating, QB Vomiting, QC Laxatives, QD Exercising) and BMI
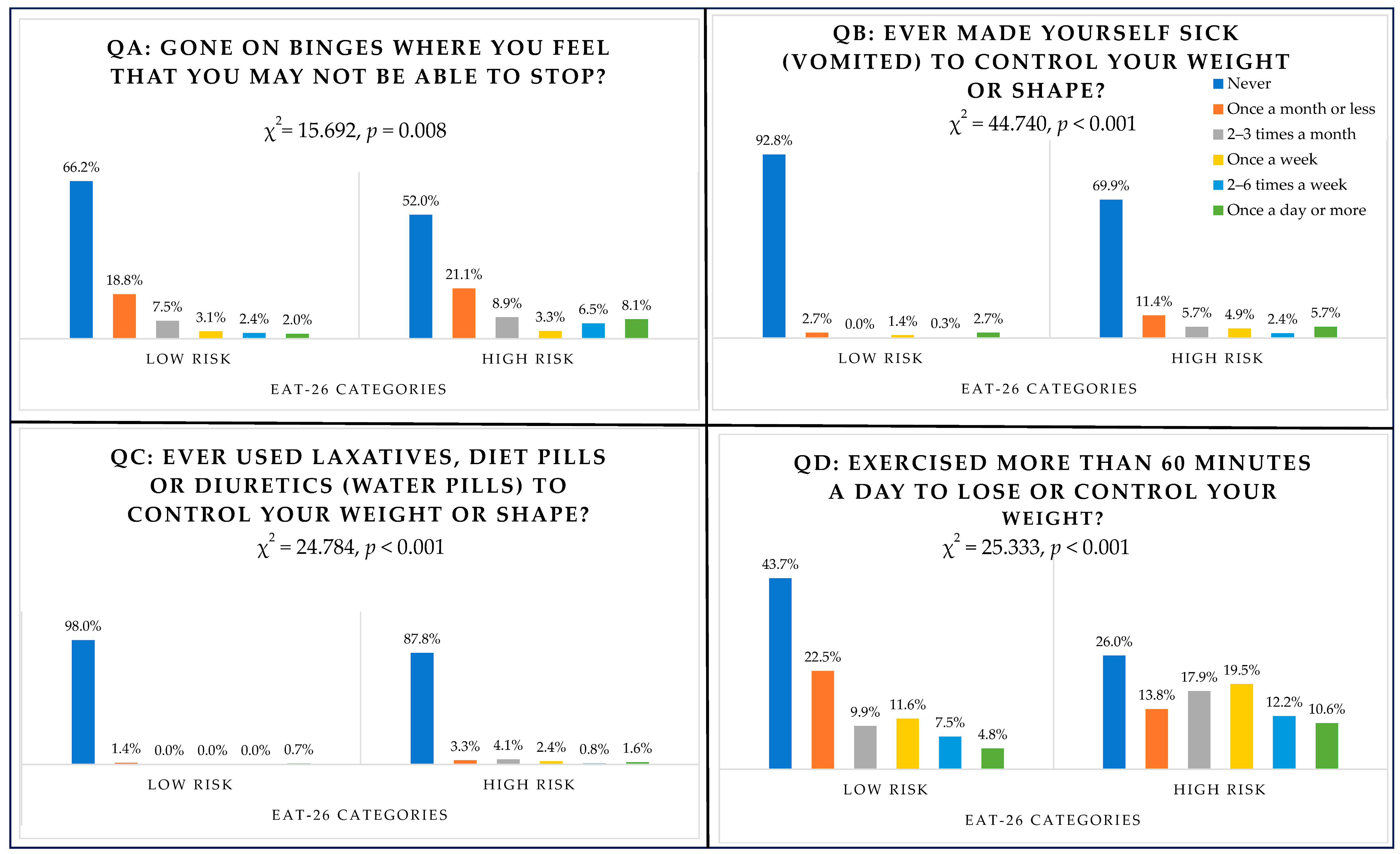
3.7. Behavioural Questions (QA Binge Eating, QB Vomiting, QC Laxatives, QD Exercising) and EAT-26 Scores (High Risk/Low Risk)
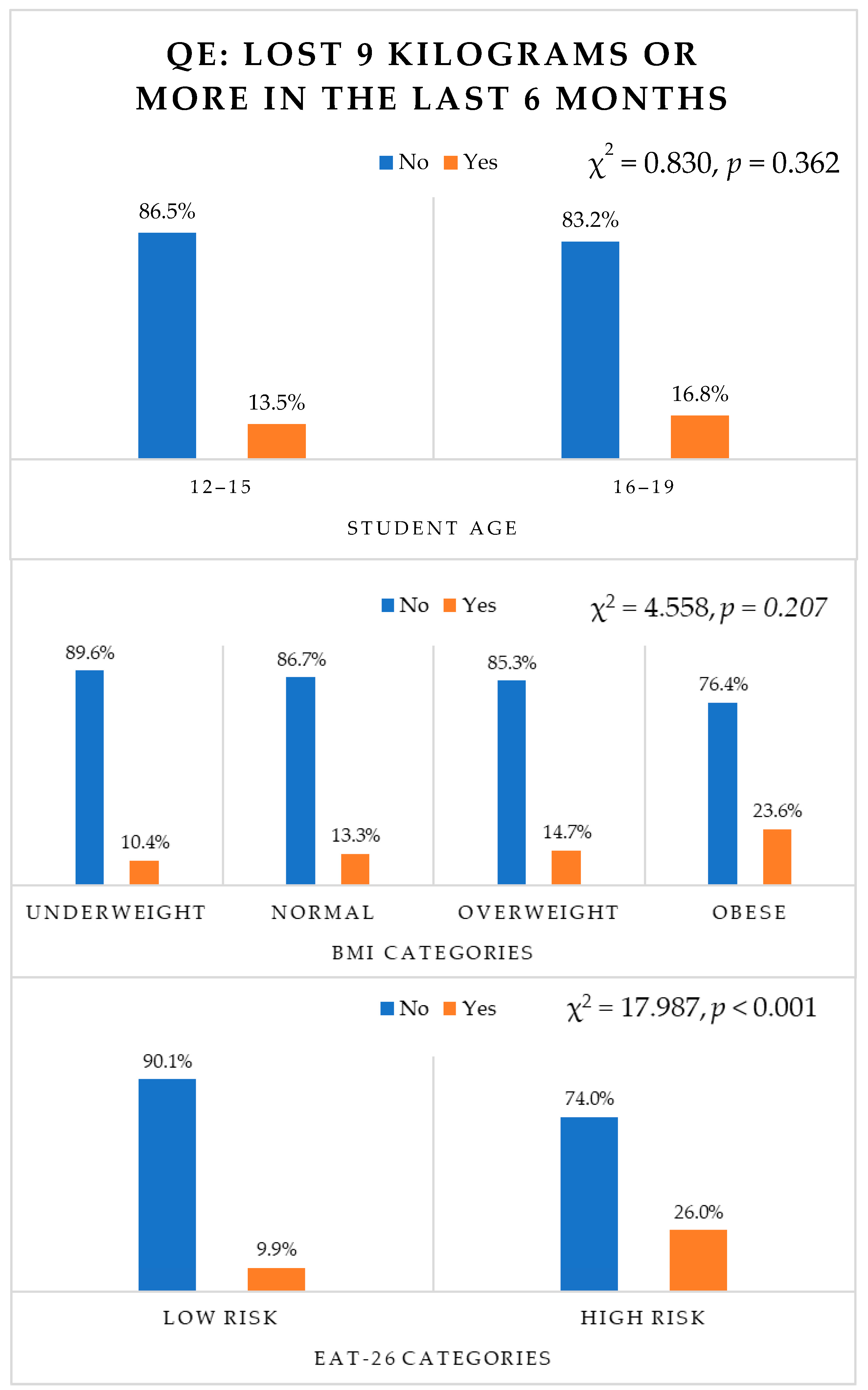
3.8. Behavioural Question E (Weight Loss) and Age, BMI, EAT-26 Scores (High/Low Risk)
3.9. Behavioural Questions and Schools (Regions)
3.10. Correlation between EAT-26 Subscales with Age and BMI
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ozier, A.D.; Henry, B.W. Position of the American Dietetic Association: Nutrition Intervention in the Treatment of Anorexia Nervosa, Bulimia Nervosa, and Other Eating Disorders. J. Am. Diet. Assoc. 2006, 106, 2073–2082. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Story, M.; Hannan, P.J.; Perry, C.L.; Irving, L.M. Weight-Related Concerns and Behaviors Among Overweight and Nonoverweight Adolescents. Arch. Pediatr. Adolesc. Med. 2002, 156, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Torstveit, M.K.; Aagedal-Mortensen, K.; Stea, T.H. More than half of high school students report disordered eating: A cross sectional study among Norwegian boys and girls. PLoS ONE 2015, 10, e0122681. [Google Scholar] [CrossRef] [PubMed]
- Micali, N.; Ploubidis, G.; De Stavola, B.; Simonoff, E.; Treasure, J. Frequency and patterns of eating disorder symptoms in early adolescence. J. Adolesc. Health 2014, 54, 574–581. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.F.; Alvarenga, M. Disordered Eating: Identifying, Treating, Preventing, and Differentiating It From Eating Disorders. Diabetes Spectr. 2007, 20, 141–148. [Google Scholar] [CrossRef]
- Harrison, A.N.; James Bateman, C.C.; Younger-Coleman, N.O.; Williams, M.C.; Rocke, K.D.; Clato-Day Scarlett, S.C.; Chang, S.M. Disordered eating behaviours and attitudes among adolescents in a middle-income country. Eat. Weight. Disord. -Stud. Anorex. Bulim. Obes. 2020, 25, 1727–1737. [Google Scholar] [CrossRef]
- Spear, B.A. Adolescent growth and development. J. Acad. Nutr. Diet. 2002, 102, S23-9. [Google Scholar] [CrossRef]
- Stang, J.S.; Stotmeister, B. Nutrition in adolescence. In Nutrition Guide for Physicians and Related Healthcare Professionals; Humana Press: Cham, Switzerland, 2017; pp. 29–39. [Google Scholar] [CrossRef]
- Yu, Z.; Tan, M. Disordered eating behaviors and food addiction among nutrition major college students. Nutrients 2016, 8, 673. [Google Scholar] [CrossRef]
- Stabouli, S.; Erdine, S.; Suurorg, L.; Jankauskienė, A.; Lurbe, E. Obesity and eating disorders in children and adolescents: The bidirectional link. Nutrients 2021, 13, 4321. [Google Scholar] [CrossRef]
- Jung, J.; Forbes, G.B. Multidimensional assessment of body dissatisfaction and disordered eating in Korean and US college women: A comparative study. Sex Roles 2006, 55, 39–50. [Google Scholar] [CrossRef]
- Musaiger, A.O.; Al-Mannai, M.; Tayyem, R.; Al-Lalla, O.; Ali, E.Y.; Kalam, F.; Benhamed, M.M.; Saghir, S.; Halahleh, I.; Djoudi, Z.; et al. Risk of Disordered Eating Attitudes Among Adolescents in Seven Arab Countries by Gender and Obesity: A Cross-Cultural Study. Appetite 2013, 60, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Haines, J.; Ziyadeh, N.J.; Franko, D.L.; McDonald, J.; Mond, J.M.; Austin, S.B. Screening high school students for eating disorders: Validity of brief behavioral and attitudinal measures. J. Sch. Health 2011, 81, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Francisco, R.; Espinoza, P.; González, M.L.; Penelo, E.; Mora, M.; Rosés, R.; Raich, R.M. Body dissatisfaction and disordered eating among Portuguese and Spanish adolescents: The role of individual characteristics and internalisation of sociocultural ideals. J. Adolesc. 2015, 41, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, Y.; Kida, K.; Nishizawa, K.; Hashiba, S.; Saito, K.; Mita, R. Perception of self-physique and eating behavior of high school students in Japan. Psychiatry Clin. Neurosci. 2003, 57, 189–196. [Google Scholar] [CrossRef]
- Yang, S.-J.; Choi, Y.; Lee, H.-Y. Eating attitude, ego-identity, and self-esteem among the urban high school girls. J. Korean Neuropsychiatr. Assoc. 2001, 40, 477–486. [Google Scholar]
- Fan, Y.; Li, Y.; Liu, A.; Hu, X.; Ma, G.; Xu, G. Associations between body mass index, weight control concerns and behaviors, and eating disorder symptoms among non-clinical Chinese adolescents. BMC Public Health 2010, 10, 314. [Google Scholar] [CrossRef] [PubMed]
- Al Sabbah, H.; Vereecken, C.A.; Elgar, F.J.; Nansel, T.; Aasvee, K.; Abdeen, Z.; Ojala, K.; Ahluwalia, N.; Maes, L. Body weight dissatisfaction and communication with parents among adolescents in 24 countries: International cross-sectional survey. BMC Public Health 2009, 9, 52. [Google Scholar] [CrossRef]
- Franklin, J.; Denyer, G.; Steinbeck, K.S.; Caterson, I.D.; Hill, A.J. Obesity and risk of low self-esteem: A statewide survey of Australian children. Pediatrics 2006, 118, 2481–2487. [Google Scholar] [CrossRef]
- Lynch, W.C.; Heil, D.P.; Wagner, E.; Havens, M.D. Ethnic differences in BMI, weight concerns, and eating behaviors: Comparison of Native American, White, and Hispanic adolescents. Body Image 2007, 4, 179–190. [Google Scholar] [CrossRef]
- Jacobi, C.; Hayward, C.; de Zwaan, M.; Kraemer, H.C.; Agras, W.S. Coming to terms with risk factors for eating disorders: Application of risk terminology and suggestions for a general taxonomy. Psychol. Bull. 2004, 130, 19. [Google Scholar] [CrossRef]
- Kotler, L.A.; Cohen, P.; Davies, M.; Pine, D.S.; Walsh, B.T. Longitudinal relationships between childhood, adolescent, and adult eating disorders. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1434–1440. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Wall, M.; Guo, J.; Story, M.; Haines, J.; Eisenberg, M. Obesity, disordered eating, and eating disorders in a longitudinal study of adolescents: How do dieters fare 5 years later? J. Am. Diet. Assoc. 2006, 106, 559–568. [Google Scholar] [CrossRef]
- Jones, J.M.; Bennett, S.; Olmsted, M.P.; Lawson, M.L.; Rodin, G. Disordered eating attitudes and behaviours in teenaged girls: A school-based study. Can. Med. Assoc. J. 2001, 165, 547–552. [Google Scholar]
- Martin, M.C.; Kennedy, P.F. Advertising and social comparison: Consequences for female preadolescents and adolescents. Psychol. Mark. 1993, 10, 513–530. [Google Scholar] [CrossRef]
- Hoare, P.; Cosgrove, L. Eating habits, body-esteem and self-esteem in Scottish children and adolescents. J. Psychosom. Res. 1998, 45, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Rosenblum, G.D.; Lewis, M. The relations among body image, physical attractiveness, and body mass in adolescence. Child Dev. 1999, 70, 50–64. [Google Scholar] [CrossRef] [PubMed]
- López-Gil, J.F.; García-Hermoso, A.; Smith, L.; Firth, J.; Trott, M.; Mesas, A.E.; Jiménez-López, E.; Gutiérrez-Espinoza, H.; Tárraga-López, P.J.; Victoria-Montesinos, D. Global proportion of disordered eating in children and adolescents: A systematic review and meta-analysis. JAMA Pediatr. 2023, 177, 363–372. [Google Scholar] [CrossRef]
- Alsheweir, A.; Goyder, E.; Alnooh, G.; Caton, S.J. Prevalence of Eating Disorders and Disordered Eating Behaviours amongst Adolescents and Young Adults in Saudi Arabia: A Systematic Review. Nutrients 2023, 15, 4643. [Google Scholar] [CrossRef]
- Rikani, A.A.; Choudhry, Z.; Maqsood Choudhry, A.; Ikram, H.; Waheed Asghar, M.; Kajal, D.; Waheed, A.; Jahan Mobassarah, N. A Critique of the Literature on Etiology of Eating Disorders. Ann. Neurosci. 2013, 20, 157–161. [Google Scholar] [CrossRef]
- Hay, P.; Mitchison, D. Urbanization and Eating Disorders: A Scoping Review of Studies from 2019 to 2020. Curr. Opin. Psychiatry 2020, 34, 287–292. [Google Scholar] [CrossRef]
- Al-Mendalawi, M.D.; Asghar, A.H. Frequency and antimicrobial susceptibility of Gram-negative bacteria isolated from 2 hospitals in Makkah, Saudi Arabia. Saudi Med. J. 2010, 31, 338. [Google Scholar] [PubMed]
- Fatima, W.; Ahmad, L.M. Prevalence of disordered eating attitudes among adolescent girls in Arar City, Kingdom of Saudi Arabia. Health Psychol. Res. 2018, 6, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Al-Subaie, A.S. Some correlates of dieting behavior in Saudi schoolgirls. Int. J. Eat. Disord. 2000, 28, 242–246. [Google Scholar] [CrossRef] [PubMed]
- General Authority for Statistics. Population Estimates in the Midyear of 2021. 2021. Available online: https://www.stats.gov.sa/sites/default/files/POP%20SEM2021E.pdf (accessed on 5 September 2023).
- Epi Info™. Division of Health Informatics & Surveillance (DHIS), Center for Surveillance, Epidemiology & Laboratory Services (CSELS). 2022. Available online: https://www.cdc.gov/csels/dhis/index.html (accessed on 20 October 2022).
- Dean, A.G.; Sullivan, K.M.; Soe, M.M. OpenEpi: Open Source Epidemiologic Statistics for Public Health 2013, Version 2.3.1. Available online: https://www.OpenEpi.com/ (accessed on 20 October 2022).
- Albrahim, T.; Alrubaish, A.A.; Alfadhliah, J.T.S.; Alaskar, M.K.; Alatawi, M.A.; Aldekhayyil, S.A. The spectrum of disordered eating attitudes among female university students: A cross-sectional study. Curr. Res. Nutr. Food Sci. J. 2019, 7, 698–707. [Google Scholar] [CrossRef]
- Alhazmi, A.H.; Al Johani, A. Prevalence and associated factors of eating disorders among students in Taiba University, Saudi Arabia: A cross-sectional study. Malays. J. Public Health Med. 2019, 19, 172–176. [Google Scholar] [CrossRef]
- Allihaibi, M. Disordered Eating Attitudes Among Secondary Schoolgirls in Al-Iskan Sector, Makkah Al-Mukarramah, Saudi Arabia. Int. J. Med. Sci. Public Health 2015, 4, 939. [Google Scholar] [CrossRef]
- Al-Qahtani, A.M.; Al-Harbi, L.M. Prevalence and risk factors of disordered eating attitudes and behaviors among high-school girls in Al-Madinah City, Saudi Arabia. Curr. Nutr. Food Sci. 2020, 16, 709–717. [Google Scholar] [CrossRef]
- Alsubaie, S.; Alalfard, A.; Muhaya, A.; Alalfard, H.; Abdullah, K.; Albishi, H. Prevalence of Eating Disorders and Obsessive-Compulsive Disorder Among Adolescents Schoolgirls: Sample From Abha City Southern Saudi Arabia. EC Psychol. Psychiatry 2017, 9, 1–10. [Google Scholar] [CrossRef]
- Alwosaifer, A.M.; Alawadh, S.A.; Wahab, M.M.A.; Boubshait, L.A.; Almutairi, B.A. Eating disorders and associated risk factors among Imam Abdulrahman bin Faisal university preparatory year female students in Kingdom of Saudi Arabia. Saudi Med. J. 2018, 39, 910. [Google Scholar] [CrossRef]
- Ghafouri, K.J.; Qadhi, A.H.; Ghaith, M.M.; Azhar, W.F.; Azzeh, F.S.; Habibullah, M.M. Eating disorders amongst adolescents in Makkah: Effects of stress and smoking. Med. Sci. 2021, 25, 767–775. [Google Scholar]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The Eating Attitudes Test: Psychometric Features and Clinical Correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef]
- Gleaves, D.H.; Pearson, C.A.; Ambwani, S.; Morey, L.C. Measuring Eating Disorder Attitudes and Behaviors: A Reliability Generalization Study. J. Eat. Disord. 2014, 2, 6. [Google Scholar] [CrossRef] [PubMed]
- Al-Adawi, S.; Dorvlo, A.; Burke, D.; Moosa, S.; Al-Bahlani, S. A survey of anorexia nervosa using the Arabic version of the EAT-26 and “gold standard” interviews among Omani adolescents. Eat. Weight. Disord. -Stud. Anorex. Bulim. Obes. 2002, 7, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Al-Subaie, A.; Al-Shammari, S.; Bamgboye, E.; Al-Sabhan, K.; Al-Shehri, S.; Bannah, A.R. Validity of the Arabic version of the eating attitude test. Int. J. Eat. Disord. 1996, 20, 321–324. [Google Scholar] [CrossRef]
- Bartholdy, S.; Allen, K.; Hodsoll, J.; O’Daly, O.G.; Campbell, I.C.; Banaschewski, T.; Bokde, A.L.; Bromberg, U.; Büchel, C.; Quinlan, E.B. Identifying disordered eating behaviours in adolescents: How do parent and adolescent reports differ by sex and age? Eur. Child Adolesc. Psychiatry 2017, 26, 691–701. [Google Scholar] [CrossRef] [PubMed]
- Rankin, J.L.; Lane, D.J.; Gibbons, F.X.; Gerrard, M. Adolescent self-consciousness: Longitudinal age changes and gender differences in two cohorts. J. Res. Adolesc. 2004, 14, 1–21. [Google Scholar] [CrossRef]
- Ferreiro, F.; Seoane, G.; Senra, C. Gender-related risk and protective factors for depressive symptoms and disordered eating in adolescence: A 4-year longitudinal study. J. Youth Adolesc. 2012, 41, 607–622. [Google Scholar] [CrossRef] [PubMed]
- Ocker, L.B.; Lam, E.T.; Jensen, B.E.; Zhang, J.J. Psychometric properties of the eating attitudes test. Meas. Phys. Educ. Exerc. Sci. 2007, 11, 25–48. [Google Scholar] [CrossRef]
- Musaiger, A.O.; Al-Kandari, F.I.; Al-Mannai, M.; Al-Faraj, A.M.; Bouriki, F.A.; Shehab, F.S.; Al-Dabous, L.A.; Al-Qalaf, W.B. Disordered eating attitudes among university students in Kuwait: The role of gender and obesity. Int. J. Prev. Med. 2016, 7, 67. [Google Scholar] [CrossRef]
- Solmi, F.; Hatch, S.L.; Hotopf, M.; Treasure, J.; Micali, N. Prevalence and correlates of disordered eating in a general population sample: The South East London Community Health (SELCoH) study. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1335–1346. [Google Scholar] [CrossRef]
- Nagata, J.M.; Garber, A.K.; Tabler, J.L.; Murray, S.B.; Bibbins-Domingo, K. Prevalence and correlates of disordered eating behaviors among young adults with overweight or obesity. J. Gen. Intern. Med. 2018, 33, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.N.; Pumariega, A.J. Culture and eating disorders: A historical and cross-cultural review. Psychiatry Interpers. Biol. Process. 2001, 64, 93–110. [Google Scholar] [CrossRef] [PubMed]
- Austin, S.B. Prevention research in eating disorders: Theory and new directions. Psychol. Med. 2000, 30, 1249–1262. [Google Scholar] [CrossRef] [PubMed]
- Mitchison, D.; Mond, J. Epidemiology of eating disorders, eating disordered behaviour, and body image disturbance in males: A narrative review. J. Eat. Disord. 2015, 3, 20. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n | % |
|---|---|---|
| Age (n = 416) | ||
| 12–13 years | 172 | 41.3 |
| 14–15 years | 95 | 22.8 |
| 16–17 years | 121 | 29.1 |
| 18–19 years | 28 | 6.7 |
| Mean ± SD | 14.56 ± 1.89 | |
| School (Region) | ||
| 128 Secondary School (North) | 63 | 15.1 |
| 213 Intermediate School (North) | 135 | 32.5 |
| 59 Secondary School (East) | 117 | 28.1 |
| 40 Intermediate School (West) | 101 | 24.3 |
| Grade | ||
| Intermediate Grade 7 | 174 | 41.8 |
| Grade 8 | 55 | 13.2 |
| Grade 9 | 7 | 1.7 |
| Secondary Grade 10 | 83 | 20 |
| Grade 11 | 41 | 9.9 |
| Grade 12 | 56 | 13.5 |
| Weight Mean ± SD | 56.39 ± 13.71 | |
| Height Mean ± SD | 157.8 ± 6.32 | |
| BMI Mean ± SD | 22.56 ± 4.92 | |
| Underweight | 48 | 11.5 |
| Normal | 211 | 50.7 |
| Overweight | 102 | 24.5 |
| Obese | 55 | 13.2 |
| EAT-26 Categories | p-Value | OR | 95% CI | ||
|---|---|---|---|---|---|
| High Risk (EAT-26 ≥ 20) | Low Risk (EAT-26 < 20) | ||||
| Age Younger (12–15 years) | 74 (27.7%) 1 | 193 (72.3%) | 0.017 * | 3.087 | 1.228–7.760 |
| Older (16–19 years) | 49 (32.9%) | 100 (67.1%) | |||
| BMI Underweight $ | 11 (22.9%) | 37 (77.1%) | 0.322 | ||
| Normal | 62 (29.4%) | 149 (70.6%) | 0.430 | 1.349 | 0.641–2.837 |
| Overweight | 29 (28.4%) | 73 (71.6%) | 0.433 | 1.382 | 0.616–3.103 |
| Obese | 21 (38.2%) | 34 (61.8%) | 0.080 | 2.194 | 0.911–5.286 |
| School (Region) 128 Secondary School (North) $ | 18 (28.6%) | 45 (71.4%) | 0.185 | ||
| 213 Intermediate School (North) | 40 (29.6%) | 95 (70.4%) | 0.047 * | 3.109 | 1.016–9.509 |
| 59 Secondary School (East) | 34 (29.1%) | 83 (70.9%) | 0.607 | 1.202 | 0.596–2.424 |
| 40 Intermediate School (West) | 31 (30.7%) | 70 (69.3%) | 0.047 * | 3.071 | 1.016–9.282 |
| Students’ Responses to EAT-26 Dieting Subscale | ||
|---|---|---|
| Q | Dieting Scale Questions | Mean ± SD |
| 1 | I am terrified about being overweight | 1.07 ± 1.25 |
| 6 | Aware of the calorie content of food that I eat | 0.64 ± 1.06 |
| 7 | Particularly avoid food with a high carbohydrate content (bread, rice, potatoes, etc.) | 0.28 ± 0.71 |
| 10 | Feel extremely guilty after eating | 0.48 ± 0.99 |
| 11 | Am preoccupied with a desire to be thinner | 1.06 ± 1.26 |
| 12 | Think about burning up calories when I exercise | 1.33± 1.31 |
| 14 | Am preoccupied with the thought of having fat on my body | 0.67 ± 1.09 |
| 16 | Avoid foods with sugar in them | 0.32 ± 0.72 |
| 17 | Eat diet foods | 0.35 ± 0.79 |
| 22 | Feel uncomfortable after eating sweets | 0.62 ± 1.06 |
| 23 | Engage in dieting behaviour | 0.26 ± 0.73 |
| 24 | Like my stomach to be empty | 0.53 ± 1.0 |
| 26 | Enjoy trying new rich foods | 0.74± 0.99 |
| Students’ Responses to EAT-26 Oral Control Subscale | ||
| Q | Oral Control Scale Questions | Mean ± SD |
| 2 | Avoid eating when I am hungry | 0.44 ± 0.87 |
| 5 | Cut my food into small pieces | 0.42 ± 0.89 |
| 8 | Feel that others would prefer if I ate more | 0.59 ± 1.05 |
| 13 | Other people think that I am too thin | 0.92 ± 1.24 |
| 15 | Take longer than others to eat my meals | 0.72 ± 1.11 |
| 19 | Display self-control around food | 1.37± 1.23 |
| 20 | Feel that others pressure me to eat | 0.71 ± 1.16 |
| Students’ Responses to EAT-26 Bulimia and Food Preoccupation Subscale | ||
| Q | Bulimia and Food preoccupation Scale Questions | Mean ± SD |
| 3 | Find myself preoccupied with food | 0.38 ± 0.79 |
| 4 | Have gone on eating binges where I feel that I may not be able to stop | 0.20 ± 0.63 |
| 9 | Vomit after I have eaten more | 0.14 ± 0.52 |
| 18 | Feel that food controls my life | 0.50 ± 0.93 |
| 21 | Give too much time and thought to food | 0.32 ± 0.83 |
| 25 | Have the impulse to vomit after meals | 0.22 ± 0.68 |
| Behavioural Questions | (n, %) | |||||
|---|---|---|---|---|---|---|
| Never | Once a Month or Less | 2–3 Times a Month | Once a Week | 2–6 Times a Week | Once a Day or More | |
| QA: Gone on binges where you feel that you may not be able to stop? | 258, 62% | 81, 19.5% | 33, 7.9% | 13, 3.2% | 15, 3.6% | 16, 3.8% |
| QB: Ever made yourself sick (vomited) to control your weight or shape? | 358, 86% | 22, 5.3% | 7, 1.7% | 10, 2.4% | 4, 1% | 15, 3.6% |
| QC: Ever used laxatives, diet pills or diuretics (water pills) to control your weight or shape? | 395, 95% | 8, 1.9% | 5, 1.2% | 3, 0.7% | 1, 0.2% | 4, 1% |
| QD: Exercised more than 60 min a day to lose or control your weight? | 160, 38.5% | 83, 20% | 51, 12.3% | 58, 13.9% | 37, 8.9% | 27, 6.4% |
| Yes | No | |||||
| QE: Lost 9 kg or more in the last 6 months. | 61, 14.7% | 355, 85.3% | ||||
| Dieting Scale | Oral Control Scale | Bulimia and Food Preoccupation Scale | |
|---|---|---|---|
| Age | 0.069 | −0.069 | 0.075 |
| BMI | 0.347 * | −0.299 * | 0.074 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsheweir, A.; Goyder, E.; Caton, S.J. The Prevalence of Disordered Eating Behaviours (DEBs) among Adolescent Female School Students in Riyadh, Saudi Arabia: A Cross-Sectional Study. Nutrients 2024, 16, 281. https://doi.org/10.3390/nu16020281
Alsheweir A, Goyder E, Caton SJ. The Prevalence of Disordered Eating Behaviours (DEBs) among Adolescent Female School Students in Riyadh, Saudi Arabia: A Cross-Sectional Study. Nutrients. 2024; 16(2):281. https://doi.org/10.3390/nu16020281
Chicago/Turabian StyleAlsheweir, Azzah, Elizabeth Goyder, and Samantha J. Caton. 2024. "The Prevalence of Disordered Eating Behaviours (DEBs) among Adolescent Female School Students in Riyadh, Saudi Arabia: A Cross-Sectional Study" Nutrients 16, no. 2: 281. https://doi.org/10.3390/nu16020281
APA StyleAlsheweir, A., Goyder, E., & Caton, S. J. (2024). The Prevalence of Disordered Eating Behaviours (DEBs) among Adolescent Female School Students in Riyadh, Saudi Arabia: A Cross-Sectional Study. Nutrients, 16(2), 281. https://doi.org/10.3390/nu16020281