
Effects of High Dose Bolus Cholecalciferol on Free Vitamin D Metabolites, Bone Turnover Markers and Physical Function
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
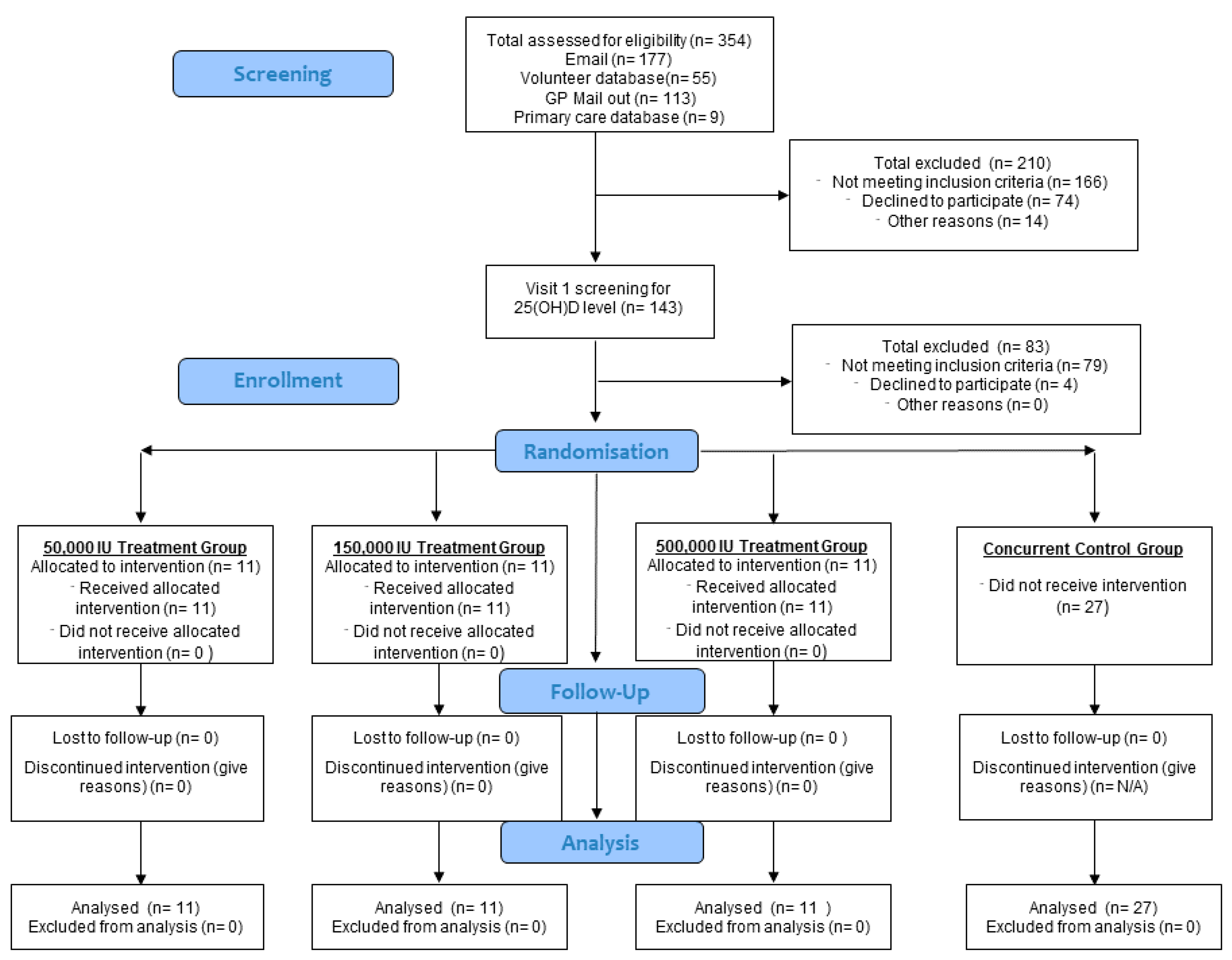
2.1. Study Design
2.2. Intervention
2.3. Participants
2.3.1. Recruitment
2.3.2. Inclusion Criteria
2.3.3. Exclusion Criteria
2.4. Study Visits
2.5. Sample Size
2.6. Materials and Measurements
2.6.1. Anthropometric Measurements
2.6.2. Blood Pressure and Pulse
2.6.3. Seven-Day Food Diary and Sunlight Exposure
2.6.4. Short Physical Performance Battery (SPPB)
2.6.5. Grip Strength
2.7. Biochemistry
2.7.1. Sample Collection and Handling
2.7.2. Total Vitamin D Metabolites
2.7.3. Free Vitamin D Metabolites
2.7.4. Vitamin D Binding Protein (VDBP)
2.7.5. Calcium and Phosphate Profiles
2.7.6. Bone Turnover Markers
2.7.7. Renin and Aldosterone
2.8. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Adverse Events
3.3. Dietary Vitamin D and Caclium Intake
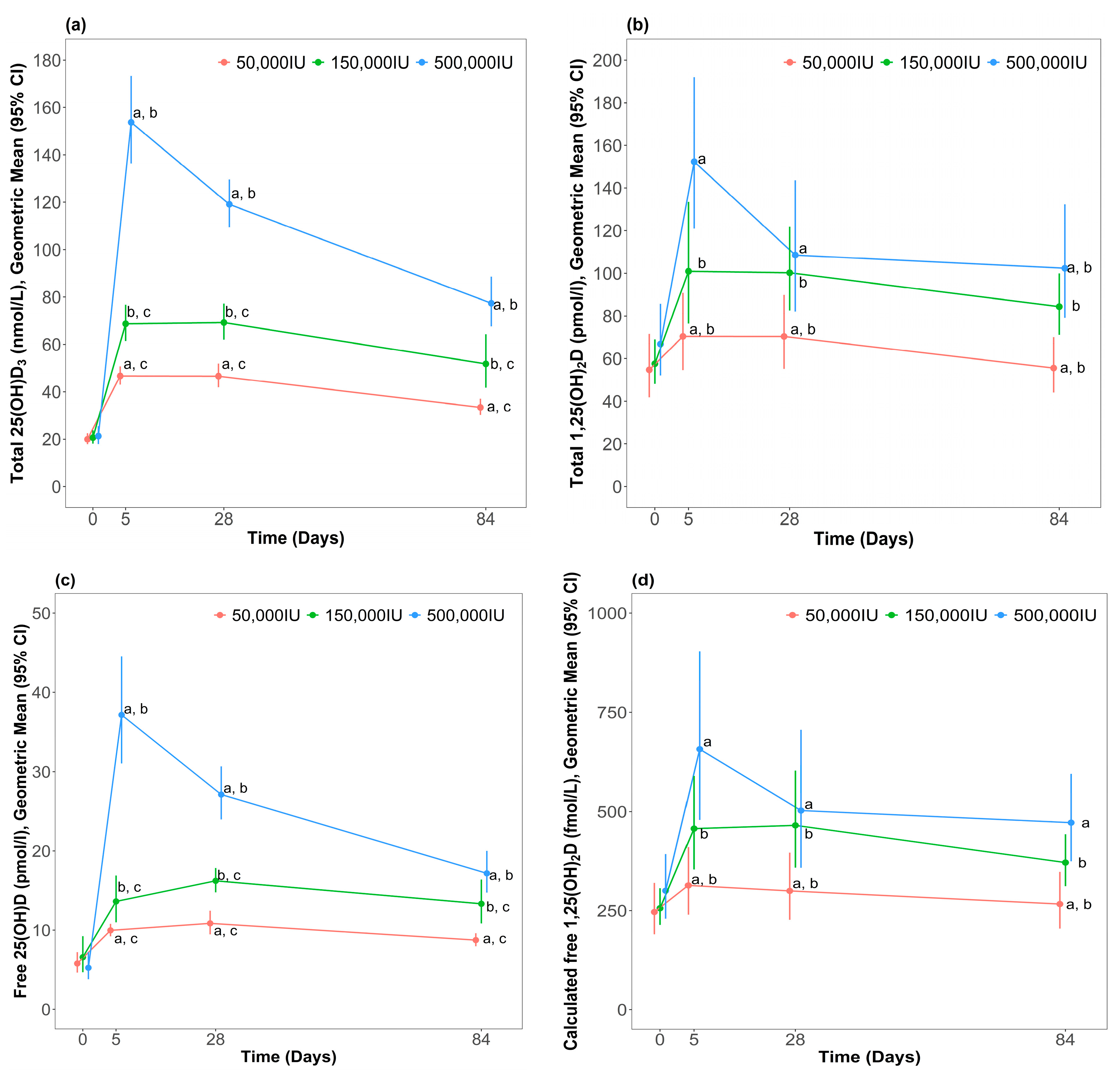
3.4. Change in Total Vitamin D Metabolites
3.4.1. Dose-Dependent Effects on Total Vitamin D Metabolites
3.4.2. Within-Group Changes for Total Vitamin D Metabolites
3.5. Change in Free Vitamin D Metabolites
3.5.1. Dose-Dependent Effects on Free Vitamin D Metabolites
3.5.2. Within-Group Changes for Free Vitamin D Metabolites
3.6. Change in Measures of Calcium Metabolism
3.6.1. Dose-Dependent Effects on Measures of Calcium Metabolism
3.6.2. Within-Group Changes for Measures of Calcium Metabolism
3.7. Change in Bone Turnover Markers
3.7.1. Dose-Dependent Effects on Bone Turnover Markers
3.7.2. Within-Group Changes for Bone Turnover Markers
3.8. Change in Muscle Function and Cardiovascular Parameters
3.8.1. Dose-Dependent Effects on Muscle Function and Cardiovascular Parameters
3.8.2. Within-Group Changes for Muscle Function and Cardiovascular Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sanfelix-Genoves, J.; Gil-Guillen, V.; Orozco-Beltran, D.; Giner-Ruiz, V.; Pertusa-Martinez, S.; Reig-Moya, B.; Carratala, C. Determinant Factors of Osteoporosis Patients’ Reported Therapeutic Adherence to Calcium and/Or Vitamin D Supplements A Cross-Sectional, Observational Study of Postmenopausal Women. Drugs Aging 2009, 26, 861–869. [Google Scholar] [CrossRef]
- Resch, H.; Walliser, J.; Phillips, S.; Wehren, L.E.; Sen, S.S. Physician and Patient Perceptions on the use of Vitamin D and Calcium in Osteoporosis Treatment: A European and Latin American Perspective. Curr. Med. Res. Opin. 2007, 23, 1227–1237. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.M.P.; Eslick, G.D.; Nowson, C.; Smith, C.; Bensoussan, A. Use of Calcium or Calcium in Combination with Vitamin D Supplementation to Prevent Fractures and Bone Loss in People Aged 50 Years and Older: A Meta-Analysis. Lancet 2007, 370, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Nowson, C.A. Prevention of Fractures in Older People with Calcium and Vitamin D. Nutrients 2010, 2, 975–984. [Google Scholar] [CrossRef]
- Unson, C.G.; Litt, M.; Reisine, S.; Mahoney-Trella, P.; Sheperd, T.; Prestwood, K. Adherence to Calcium/Vitamin D and Estrogen Protocols among Diverse Older Participants Enrolled in a Clinical Trial. Contemp. Clin. Trials 2006, 27, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Pekkarinen, T.; Valimaki, V.V.; Aarum, S.; Turpeinen, U.; Hamalainen, E.; Loyttyniemi, E.; Valimaki, M.J. The Same Annual Dose of 292000 IU of Vitamin D-3 (Cholecalciferol) on either Daily or Four Monthly Basis for Elderly Women: 1-Year Comparative Study of the Effects on Serum 25(OH)D-3 Concentrations and Renal Function. Clin. Endocrinol. 2010, 72, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Premaor, M.O.; Scalco, R.; da Silva, M.J.S.; Froehlich, P.E.; Furlanetto, T.W. The Effect of a Single Dose Versus a Daily Dose of Cholecalciferol on the Serum 25-Hydroxycholecalciferol and Parathyroid Hormone Levels in the Elderly with Secondary Hyperparathyroidism Living in a Low-Income Housing Unit. J. Bone Miner. Metab. 2008, 26, 603–608. [Google Scholar] [CrossRef]
- Sanders, K.M.; Stuart, A.L.; Williamson, E.J.; Simpson, J.A.; Kotowicz, M.A.; Young, D.; Nicholson, G.C. Annual High-Dose Oral Vitamin D and Falls and Fractures in Older Women a Randomized Controlled Trial. JAMA-J. Am. Med. Assoc. 2010, 303, 1815–1822. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.; Dawson-Hughes, B.; Orav, J.; Staehelin, H.B.; Meyer, O.W.; Theiler, R.; Dick, W.; Willett, W.C.; Egli, A. Monthly High-Dose Vitamin D Treatment for the Prevention of Functional Decline a Randomized Clinical Trial. JAMA Intern. Med. 2016, 176, 175–183. [Google Scholar] [CrossRef]
- Smith, H.; Anderson, F.; Raphael, H.; Maslin, P.; Crozier, S.; Cooper, C. Effect of Annual Intramuscular Vitamin D on Fracture Risk in Elderly Men and Womena Population-Based, Randomized, Double-Blind, Placebo-Controlled Trial. Rheumatology 2007, 46, 1852–1857. [Google Scholar] [CrossRef]
- Sanders, K.M.; Nicholson, G.C.; Ebeling, P.R. Is High Dose Vitamin D Harmful? Calcif. Tissue Int. 2013, 92, 191–206. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P. Vitamin D—Baseline Status and Effective Dose. N. Engl. J. Med. 2012, 367, 77–78. [Google Scholar] [CrossRef]
- Jones, G. Pharmacokinetics of Vitamin D Toxicity. Am. J. Clin. Nutr. 2008, 88, 582S–586S. [Google Scholar] [CrossRef]
- Rousseau, A.F.; Damas, P.; Ledoux, D.; Lukas, P.; Carlisi, A.; Le Goff, C.; Gadisseur, R.; Cavalier, E. Vitamin D Status After a High Dose of Cholecalciferol in Healthy and Burn Subjects. Burns 2015, 41, 1028–1034. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.B.; Gallagher, C.; Jorde, R.; Berg, V.; Walsh, J.; Eastell, R.; Evans, A.L.; Bowles, S.; Naylor, K.E.; Jones, K.S.; et al. Determination of Free 25(OH)D Concentrations and their Relationships to Total 25(OH)D in Multiple Clinical Populations. J. Clin. Endocrinol. Metab. 2018, 103, 3278–3288. [Google Scholar] [CrossRef] [PubMed]
- Nielson, C.M.; Jones, K.S.; Chun, R.F.; Jacobs, J.M.; Wang, Y.; Hewison, M.; Adams, J.S.; Swanson, C.M.; Lee, C.G.; Vanderschueren, D.; et al. Free 25-Hydroxyvitamin D: Impact of Vitamin D Binding Protein Assays on Racial-Genotypic Associations. J. Clin. Endocrinol. Metab. 2016, 101, 2226–2234. [Google Scholar] [CrossRef]
- Bikle, D.D.; Schwartz, J. Vitamin D Binding Protein, Total and Free Vitamin D Levels in Different Physiological and Pathophysiological Conditions. Front. Endocrinol. 2019, 10, 317. [Google Scholar] [CrossRef]
- Girgis, C.M. Vitamin D and Skeletal Muscle: Emerging Roles in Development, Anabolism and Repair. Calcif. Tissue Int. 2020, 106, 47–57. [Google Scholar] [CrossRef]
- Girgis, C.M.; Brennan Speranza, T.C. Vitamin D and Skeletal Muscle: Current Concepts from Preclinical Studies. J. Bone Miner. Res. Plus 2021, 5, e10575. [Google Scholar] [CrossRef]
- Duval, G.; Rolland, Y.; Schott, A.M.; Blain, H.; Dargent-Molina, P.; Walrand, S.; Duque, G.; Annweiler, C. Association of Hypovitaminosis D with Triceps Brachii Muscle Fatigability among Older Women: Findings from the EPIDOS Cohort. Maturitas 2018, 111, 47–52. [Google Scholar] [CrossRef]
- Harrison, S.; Ghosh, S. The Effect of Vitamin D Supplementation on Muscle Mass, Muscle Strength and Muscle Function in the Elderly: A Systematic Review and Meta-Analysis. Aging Med. Healthc. 2023, 14, 172–181. [Google Scholar] [CrossRef]
- Cipriani, C.; Romagnoli, E.; Carnevale, V.; Clerico, R.; Pepe, J.; Cilli, M.; Diacinti, D.; Savoriti, C.; Colangelo, L.; Minisola, S. Effect of a Single Oral Dose of 600,000 IU of Cholecalciferol on Muscle Strength: A Study in Young Women. J. Endocrinol. Investig. 2013, 36, 1051–1054. [Google Scholar]
- Li, Y.C. Vitamin D Regulation of the Renin-Angiotensin System. J. Cell. Biochem. 2003, 88, 327–331. [Google Scholar] [CrossRef]
- Li, Y.C.; Kong, J.; Wei, M.J.; Chen, Z.F.; Liu, S.Q.; Cao, L.P. 1,25-Dihydroxyvitamin D-3 is a Negative Endocrine Regulator of the Renin-Angiotensin System. J. Clin. Investig. 2002, 110, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Lind, L.; Hanni, A.; Lithell, H.; Hvarfner, A.; Sorensen, O.H.; Ljunghall, S. Vitamin-D is Related to Blood-Pressure and Other Cardiovascular Risk-Factors in Middle-Aged Men. Am. J. Hypertens. 1995, 8, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Kristal-Boneh, E.; Froom, P.; Harari, G.; Ribak, J. Association of 1,25 Dihydroxyvitamin D and Blood Pressure in Normotensive. J. Hypertens. 1998, 16, S262. [Google Scholar]
- Pilz, S.; Tomaschitz, A.; Ritz, E.; Pieber, T.R. Vitamin D Status and Arterial Hypertension: A Systematic Review. Nat. Rev. Cardiol. 2009, 6, 621–630. [Google Scholar] [CrossRef]
- Forman, J.P.; Giovannucci, E.; Holmes, M.D.; Bischoff-Ferrari, H.; Tworoger, S.S.; Willett, W.C.; Curhan, G.C. Plasma 25-Hydroxyvitamin D Levels and Risk of Incident Hypertension. Hypertension 2007, 49, 1063–1069. [Google Scholar] [CrossRef]
- Vilaca, T.; Gossiel, F.; Eastell, R. Bone Turnover Markers: Use in Fracture Prediction. J. Clin. Densitom. 2017, 20, 346–352. [Google Scholar] [CrossRef]
- Rossini, M.; Adami, S.; Viapiana, O.; Fracassi, E.; Idolazzi, L.; Povino, M.R.; Gatti, D. Dose-Dependent Short-Term Effects of Single High Doses of Oral Vitamin D-3 on Bone Turnover Markers. Calcif. Tissue Int. 2012, 91, 365–369. [Google Scholar] [CrossRef]
- Cantwell, M.M.; Millen, A.E.; Carroll, R.; Mittl, B.L.; Hermansen, S.; Brinton, L.A.; Potischman, N. A Debriefing Session with a Nutritionist can Improve Dietary Assessment using Food Diaries. J. Nutr. 2006, 136, 440–445. [Google Scholar] [CrossRef]
- Veronese, N.; Bolzetta, F.; Toffanello, E.D.; Zambon, S.; De Rui, M.; Perissinotto, E.; Coin, A.; Corti, M.; Baggio, G.; Crepaldi, G.; et al. Association between Short Physical Performance Battery and Falls in Older People: The Progetto Veneto Anziani Study. Rejuvenation Res. 2014, 17, 276–284. [Google Scholar] [CrossRef]
- Bhan, I.; Powe, C.E.; Berg, A.H.; Ankers, E.; Wenger, J.B.; Karumanchi, S.A.; Thadhani, R.I. Bioavailable Vitamin D is More Tightly Linked to Mineral Metabolism than Total Vitamin D in Incident Hemodialysis Patients. Kidney Int. 2012, 82, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Shimada, T.; Hasegawa, H.; Yamazaki, Y.; Muto, T.; Hino, R.; Takeuchi, Y.; Fujita, T.; Nakahara, K.; Fukumoto, S.; Yamashita, T. FGF-23 is a Potent Regulator of Vitamin D Metabolism and Phosphate Homeostasis. J. Bone Miner. Res. 2004, 19, 429–435. [Google Scholar] [CrossRef]
- Perwad, F.; Zhang, M.Y.H.; Tenenhouse, H.S.; Portale, A.A. Fibroblast Growth Factor 23 Impairs Phosphorus and Vitamin D Metabolism in Vivo and Suppresses 25-Hydroxyvitamin D-1 Alpha-Hydroxylase Expression in Vitro. Am. J. Physiol.-Ren. Physiol. 2007, 293, F1577–F1583. [Google Scholar] [CrossRef] [PubMed]
- Vieth, R. Vitamin D Toxicity, Policy, and Science. J. Bone Miner. Res. 2007, 22, V64–V68. [Google Scholar] [CrossRef] [PubMed]
- Romagnoli, E.; Mascia, M.L.; Cipriani, C.; Fassino, V.; Mazzei, F.; D’Erasmo, E.; Carnevale, V.; Scillitani, A.; Minisola, S. Short and Long-Term Variations in Serum Calciotropic Hormones After a Single very Large Dose of Ergocalciferol (Vitamin D(2)) Or Cholecalciferol (Vitamin D(3)) in the Elderly. J. Clin. Endocrinol. Metab. 2008, 93, 3015–3020. [Google Scholar] [CrossRef]
- Cipriani, C.; Romagnoli, E.; Scillitani, A.; Chiodini, I.; Clerico, R.; Carnevale, V.; Mascia, M.L.; Battista, C.; Viti, R.; Pileri, M.; et al. Effect of a Single Oral Dose of 600,000 IU of Cholecalciferol on Serum Calciotropic Hormones in Young Subjects with Vitamin D Deficiency: A Prospective Intervention Study. J. Clin. Endocrinol. Metab. 2010, 95, 4771–4777. [Google Scholar] [CrossRef]
- Henry, H.L. Regulation of Vitamin D Metabolism. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 531–541. [Google Scholar] [CrossRef]
- Norman, A.W. From Vitamin D to Hormone D: Fundamentals of the Vitamin D Endocrine System Essential for Good Health. Am. J. Clin. Nutr. 2008, 88, 491S–499S. [Google Scholar] [CrossRef]
- Dawson-Hughes, B.; Harris, S.S. High-Dose Vitamin D Supplementation Too Much of a Good Thing? JAMA-J. Am. Med. Assoc. 2010, 303, 1861–1862. [Google Scholar] [CrossRef] [PubMed]
- Beckman, M.J.; Johnson, J.A.; Goff, J.P.; Reinhardt, T.A.; Beitz, D.C.; Horst, R.L. The Role of Dietary Calcium in the Physiology of Vitamin-D Toxicity—Excess Dietary Vitamin-D-3 Blunts Parathyroid-Hormone Induction of Kidney 1-Hydroxylase. Arch. Biochem. Biophys. 1995, 319, 535–539. [Google Scholar] [CrossRef]
- Hansen, K.E. High-Dose Vitamin D: Helpful or Harmful? Curr. Rheumatol. Rep. 2011, 13, 257–264. [Google Scholar] [CrossRef]
- Mirhosseini, N.; Rainsbury, J.; Kimball, S.M. Vitamin D Supplementation, Serum 25(OH)D Concentrations and Cardiovascular Disease Risk Factors: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2018, 5, 87. [Google Scholar] [CrossRef]
- Chen, S.; Glenn, D.J.; Ni, W.; Grigsby, C.L.; Olsen, K.; Nishimoto, M.; Law, C.S.; Gardner, D.G. Expression of the Vitamin D Receptor is Increased in the Hypertrophic Heart. Hypertension 2008, 52, 1106–1112. [Google Scholar] [CrossRef]
- Wang, Y.J.; DeLuca, H.F. Is the Vitamin D Receptor found in Muscle? Endocrinology 2011, 152, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, C.; Romagnoli, E.; Pepe, J.; Russo, S.; Carlucci, L.; Piemonte, S.; Nieddu, L.; McMahon, D.J.; Singh, R.; Minisola, S. Long-Term Bioavailability After a Single Oral or Intramuscular Administration of 600,000 IU of Ergocalciferol or Cholecalciferol: Implications for Treatment and Prophylaxis. J. Clin. Endocrinol. Metab. 2013, 98, 2709–2715. [Google Scholar] [CrossRef] [PubMed]
- Pettifor, J.M.; Bikle, D.D.; Cavaleros, M.; Zachen, D.; Kamdar, M.C.; Ross, F.P. Serum Levels of Free 1,25-Dihydroxyvitamin-D in Vitamin-D Toxicity. Ann. Intern. Med. 1995, 122, 511–513. [Google Scholar] [CrossRef] [PubMed]
- Blank, S.; Scanlon, K.S.; Sinks, T.H.; Lett, S.; Falk, H. An Outbreak of Hypervitaminosis-D Associated with the Overfortification of Milk from a Home-Delivery Dairy. Am. J. Public Health 1995, 85, 656–659. [Google Scholar] [CrossRef]
- Vieth, R. The Mechanisms of Vitamin-D Toxicity. Bone Miner. 1990, 11, 267–272. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| 50,000 IU (n = 11) | 150,000 IU (n = 11) | 500,000 IU (n = 11) | Control (n = 27) | |
|---|---|---|---|---|
| Age (Years) | 63 (57–66) | 62 (58–69) | 62 (55–68) | 60 (58–64) |
| Height (cm) | 163 (157.5–166.7) | 157.2 (156.3–163.3) | 159.9 (156.6–163.6) | 160.0 (155–165.5) |
| Weight (kg) | 65.5 (60.8–74.0) | 64.3 (57.1–64.3) | 63.6 (59.3–67.0) | 66.1 (62.4–72.0) |
| BMI (kg/m2) | 24.6 (22.7–28.5) | 23.2 (22.6–28.1) | 23.6 (23.2–27.6) | 26.4 (23.0–28.7) |
| Total dietary vitamin D intake (µg/day) | 1.6 (1.4–4.0) | 0.87 (0.7–1.1) | 2.6 (1.5–2.6) | 2.2 (0.9–3.2) |
| Total dietary calcium intake (mg/day) | 677 (649–1048) | 637 (436–800) | 1013 (737–1071) | 806 (668–981) |
| Sunlight exposure score | 83 (72–122) | 83 (42–88) | 59 (34–108) | 80 (54–110) |
| Visit (Week/Day) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | Week 1 (5 ± 2) | Week 4 (28 ± 3) | Week 12 (84 ± 5) | ||||||
| Vitamin D Metabolite | Treatment Group | Geometric Mean (95% CI) | Ratio of Means (95% CI) | Geometric Mean (95% CI) | Change (95% CI) | Geometric Mean (95% CI) | Change (95% CI) | Geometric Mean (95% CI) | Change (95% CI) |
| Total 25(OH)D3 (nmol/L) | 50,000 IU | 20.0 | - | 46.7 | 133 | 46.6 | 131 | 33.4 | 66 |
| (17.8, 22.5) | (43.0, 50.7) | (1.05, 165) | (41.9, 51.9) | (101, 167) | (30.2, 37.1) | (45, 89) | |||
| 150,000 IU | 20.7 | - | 68.7 | 240 | 69.2 | 238 | 51.8 | 153 | |
| (18.1, 23.7) | (61.4, 76.7) | (197, 289) | (62.0, 77.2) | (196, 286) | (41.7, 64.3) | (121, 189) | |||
| 500,000 IU | 21.3 | - | 153.7 | 621 | 119.1 | 458 | 77.4 | 263 | |
| (17.9, 25.5) | (136.4, 173.3) | (534, 719) | (109.4, 129.6) | (391, 534) | (67.6, 88.6) | (219, 312) | |||
| Free 25(OH)D (pmol/L) | 50,000 IU | 5.8 | - | 10.0 | 72 | 10.9 | 88 | 8.7 | 51 |
| (4.6, 7.2) | (9.2, 10.8) | (38, 116) | (9.5, 12.4) | (49, 137) | (8.0, 9.6) | (1.21, 1.89) | |||
| 150,000 IU | 6.6 | - | 13.6 | 107 | 16.2 | 147 | 13.3 | 103 | |
| (4.7, 9.2) | (11.0, 16.9) | (64, 161) | (14.8, 17.8) | (96, 211) | (10.8, 16.4) | (61, 155) | |||
| 500,000 IU | 5.2 | - | 37.2 | 609 | 27.1 | 417 | 17.2 | 228 | |
| (3.8, 7.2) | (31.0, 44.5) | (466, 788) | (24.0, 30.7) | (313, 548) | (14.7, 20.0) | (162, 310) | |||
| Total 1,25(OH)2D (pmol/L) | 50,000 IU | 54.7 | - | 70.4 | 29 | 70.4 | 27 | 55.6 | 6 |
| (41.8, 71.6) | (54.6, 90.8) | (8, 53) | (55.2, 89.8) | (6, 53) | (44.1, 70.1) | (−11, 26) | |||
| 150,000 IU | 57.6 | - | 101.0 | 75 | 100.3 | 74 | 84.3 | 46 | |
| (48.1, 69.0) | (76.4, 133.4) | (47, 108) | (82.6, 121.8) | (47, 106) | (71.2, 100.0) | (24, 73) | |||
| 500,000 IU | 66.9 | - | 152.4 | 128 | 108.6 | 62 | 102.4 | 53 | |
| (52.2, 85.7) | (121.0, 191.9) | (93, 170) | (82.0, 143.6) | (37, 92) | (79.2, 132.3) | (29, 81) | |||
| Free 1,25(OH)2D (fmol/L) | 50,000 IU | 247 | - | 314 | 27 | 300 | 21 | 267 | 12 |
| (190, 320) | (240, 410) | (4, 55) | (227, 396) | (−2, 49) | (205, 348) | (−8, 36) | |||
| 150,000 IU | 256 | - | 457 | 78 | 465 | 82 | 372 | 45 | |
| (214, 307) | (354, 590) | (46, 116) | (359, 604) | (50, 120) | (312, 443) | (20, 75) | |||
| 500,000 IU | 300 | - | 658 | 119 | 503 | 67 | 472 | 57 | |
| (230, 393) | (479, 903) | (81, 165) | (358, 706) | (38, 103) | (375, 595) | (30, 90) | |||
| Visit (Week/Day) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | Week 1 (5 ± 2) | Week 4 (28 ± 3) | Week 12 (84 ± 5) | ||||||
| Biochemical Measurement | Treatment Group | Mean (95% CI) | Change (95% CI) | Mean (95% CI) | Change (95% CI) | Mean (95% CI) | Change (95% CI) | Mean (95% CI) | Change (95% CI) |
| PTH (pmol/L) | 50,000 IU | 4.2 | - | 4.2 | −5 | 3.9 | −12 | 3.4 | −20 |
| (3.3, 5.3) | (3.0, 6.1) | (−21, 14) | (3.1, 4.9) | (−26, 6) | (2.5, 4.6) | (−33, −5) | |||
| 150,000 IU | 4.4 | - | 3.5 | −21 | 3.9 | −12 | 3.6 | −17 | |
| (3.7, 5.2) | (2.9, 4.2) | (−37, −7) | (3.1, 4.8) | (−26, 6) | (3.0, 4.4) | (−31, −1) | |||
| 500,000 IU | 3.9 | - | 3.4 | −15 | 3.3 | −17 | 3.9 | −4 | |
| (3.1, 5.0) | (3.0, 3.8) | (−29, 1) | (2.8, 4.0) | (−30, −1) | (3.4, 4.5) | (−19, 15) | |||
| sCa (nmol/L) | 50,000 IU | 2.32 | - | 2.33 | 0 | 2.33 | 0 | 2.32 | 0 |
| (2.28, 2.36) | (2.29, 2.36) | (−1, 2) | (2.29, 2.37) | (−2, 2) | (2.27, 2.38) | (−2, 2) | |||
| 150,000 IU | 2.36 | - | 2.35 | −1 | 2.35 | 0 | 2.34 | −1 | |
| (2.33, 2.39) | (2.29, 2.41) | (−2, 1) | (2.29, 2.41) | (−2, 1) | (2.31, 2.38) | (−2, 1) | |||
| 500,000 IU | 2.30 | - | 2.30 | 0 | 2.30 | 0 | 2.29 | 0 | |
| (2.24, 2.35) | (2.26, 2.35) | (−1, 2) | (2.26, 2.35) | (−1, 2) | (2.24, 2.34) | (−2, 1) | |||
| iCa 1 (nmol/L) | 50,000 IU | 1.23 | - | 1.26 | 0.018 | 1.24 | 0.002 | 1.25 | 0.015 |
| (1.22, 1.26) | (1.23, 1.28) | (−0.0003, 0.036) | (1.22, 1.26) | (−0.016, 0.021) | (1.22, 1.28) | (−0.003, 0.032) | |||
| 150,000 IU | 1.25 | - | 1.25 | −0.003 | 1.25 | −0.001 | 1.25 | −0.001 | |
| (1.23, 1.27) | (1.23, 1.27) | (−0.021, 0.015) | (1.22, 1.27) | (−0.019, 0.017) | (1.22, 1.27) | (−0.018, 0.017) | |||
| 500,000 IU | 1.24 | - | 1.25 | 0.009 | 1.25 | 0.015 | 1.24 | 0.001 | |
| (1.22, 1.26) | (1.22, 1.27) | (−0.010, 0.027) | (1.23, 1.28) | (−0.003, 0.033) | (1.22, 1.26) | (−0.017, 0.019) | |||
| 24-h UCa:UCr 1 | 50,000 IU | 0.30 | - | 0.38 | 0.07 | 0.36 | 0.07 | 0.36 | 0.06 |
| (0.20, 0.41) | (0.23, 0.53) | (−0.01, 0.14) | (0.24, 0.47) | (−0.01, 0.14) | (0.24, 0.48) | (−0.01, 0.14) | |||
| 150,000 IU | 0.29 | - | 0.48 | 0.19 | 0.49 | 0.20 | 0.41 | 0.13 | |
| (0.25, 0.34) | (0.36, 0.60) | (0.12, 0.26) | (0.38, 0.59) | (0.13, 0.28) | (0.32, 0.50) | (0.06, 0.20) | |||
| 500,000 IU | 0.47 | - | 0.63 | 0.14 | 0.55 | 0.09 | 0.53 | 0.06 | |
| (0.37, 0.58) | (0.45, 0.81) | (0.06, 0.22) | (0.40, 0.70) | (0.01, 0.17) | (0.36, 0.70) | (−0.02, 0.13) | |||
| 24-h uCa excretion (mmol/L) 1 | 50,000 IU | 2.40 | - | 3.20 | 0.80 | 3.11 | 0.80 | 2.79 | 0.46 |
| (1.52, 3.28) | (2.11, 4.29) | (0.18, 1.42) | (2.21, 4.01) | (0.18, 1.38) | (1.70, 3.88) | (−0.14, 1.06) | |||
| 150,000 IU | 2.10 | - | 3.55 | 1.45 | 3.36 | 1.41 | 3.00 | 1.05 | |
| (1.68, 2.52) | (2.55, 4.56) | (0.87, 2.04) | (2.36, 4.36) | (0.80, 2.01) | (2.45, 3.55) | (0.44, 1.65) | |||
| 500,000 IU | 4.10 | - | 5.09 | 0.76 | 5.01 | 0.86 | 4.31 | 0.14 | |
| (2.68, 5.52) | (3.52, 6.66) | (0.11, 1.40) | (3.35, 6.67) | (0.21, 1.50) | (3.20, 5.42) | (−0.47, 0.74) | |||
| Visit (Week/Day) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | Week 1 (5 ± 2) | Week 4 (28 ± 3) | Week 12 (84 ± 5) | ||||||
| Biochemical Measurement | Treatment Group | Geometric Mean (95% CI) | Change (95% CI) | Geometric Mean (95% CI) | Change (95% CI) | Geometric Mean (95% CI) | Change (95% CI) | Geometric Mean (95% CI) | Change (95% CI) |
| sPh (nmol/L) | 50,000 IU | 1.17 | - | 1.24 | 6 | 1.25 | 8 | 1.23 | 5 |
| (1.10, 1.23) | (1.16, 1.31) | (0, 12) | (1.15, 1.37) | (2, 14) | (1.15, 1.32) | (0, 11) | |||
| 150,000 IU | 1.24 | - | 1.25 | 1 | 1.23 | 0 | 1.23 | 0 | |
| (1.16, 1.31) | (1.18, 1.33) | (−5, 7) | (1.17, 1.30) | (−6, 5) | (1.13, 1.34) | (−6, 5) | |||
| 500,000 IU | 1.17 | - | 1.25 | 6 | 1.21 | 3 | 1.16 | −2 | |
| (1.08, 1.27) | (1.15, 1.35) | (0, 12) | (1.11, 1.32) | (−2, 9) | (1.06, 1.27) | (−7, 4) | |||
| sCr (nmol/L) | 50,000 IU | 65.1 | - | 64.6 | −1 | 64.0 | −1 | 65.1 | 0 |
| (59.7, 71.0) | (59.4, 70.4) | (−6, 4) | (57.6, 71.0) | (−6, 4) | (60.2, 70.5) | (−5, 5) | |||
| 150,000 IU | 65.3 | - | 63.7 | −2 | 63.9 | −2 | 66.0 | 1 | |
| (61.0, 69.8) | (57.0, 71.0) | (−7, 3) | (58.4, 70.0) | (−7, 3) | (60.1, 72.4) | (−4, 6) | |||
| 500,000 IU | 64.2 | - | 64.4 | 0 | 65.3 | 2 | 67.1 | 4 | |
| (58.2, 70.9) | (58.4, 71.0) | (−5, 5) | (60.4, 70.6) | (−3, 7) | (61.2, 73.5) | (−1, 10) | |||
| Albumin (g/L) | 50,000 IU | 47 | - | 47 | −1 | 47 | −1 | 47 | 0 |
| (47, 48) | (45, 48) | (−4, 1) | (47, 48) | (−4, 1) | (46, 49) | (−3, 2) | |||
| 150,000 IU | 47 | - | 46 | −1 | 47 | 0 | 47 | 1 | |
| (46, 48) | (45, 48) | (−3, 1) | (46, 48) | (−2, 2) | (47, 48) | (−2, 3) | |||
| 500,000 IU | 47 | - | 47 | −2 | 46 | −2 | 47 | −2 | |
| (46, 49) | (45, 48) | (−4, 1) | (45, 48) | (−5, 0) | (45, 48) | (−4, 1) | |||
| DBP 1 (ug/mL) | 50,000 IU | 309 | - | 312 | 3 | 328 | 18 | 284 | −25 |
| (272, 345) | (272, 352) | (−29, 36) | (289, 368) | (−16, 51) | (239, 328) | (−57, 8) | |||
| 150,000 IU | 311 | - | 302 | −9 | 295 | −16 | 314 | 3 | |
| (265, 357) | (265, 339) | (−42, 25) | (250, 340) | (−48, 17) | (266, 362) | (−29, 36) | |||
| 500,000 IU | 302 | - | 322 | 19 | 295 | −8 | 294 | −8 | |
| (278, 327) | (270, 373) | (−13, 52) | (261, 328) | (−40, 25) | (265, 324) | (−40, 24) | |||
| FGF-23 (pg/mL) | 50,000 IU | 41.3 | - | 52.1 | 16 | 51.1 | 26 | 49.0 | 9 |
| (32.8, 51.9) | (42.5, 63.8) | (−5, 42) | (33.5, 77.8) | (3, 53) | (39.4, 61.0) | (−10, 34) | |||
| 150,000 IU | 50.8 | - | 58.7 | 9 | 52.0 | 2 | 50.0 | −2 | |
| (36.6, 70.5) | (42.6, 80.8) | (−11, 33) | (37.8, 71.7) | (−16, 24) | (35.3, 70.9) | (−19, 20) | |||
| 500,000 IU | 50.5 | - | 63.0 | 25 | 52.6 | 4 | 45.9 | −9 | |
| (38.6, 66.0) | (47.9, 82.7) | (3, 51) | (42.5, 65.1) | (−14, 26) | (33.0, 63.8) | (−25, 10) | |||
| Visit (Week/Day) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | Week 1 (5 ± 2) | Week 4 (28 ± 3) | Week 12 (84 ± 5) | ||||||
| Biochemical Measurement | Treatment Group | Geometric Mean (95% CI) | Change (95% CI) | Geometric Mean (95% CI) | Change (95% CI) | Geometric Mean (95% CI) | Change (95% CI) | Geometric Mean (95% CI) | Change (95% CI) |
| PINP (ng/mL) | 50,000 IU | 54.4 | - | 56.8 | 4 | 51.7 | −1 | 51.1 | −6 |
| (45.3, 65.3) | (44.8, 72.1) | (−5, 14) | (41.7, 63.9) | (−10, 8) | (40.1, 65.3) | (−14, 3) | |||
| 150,000 IU | 56.8 | - | 61.8 | 5 | 58.8 | 4 | 56.1 | −3 | |
| (44.9, 71.9) | (49.4, 77.3) | (−5, 15) | (48.1, 71.9) | (−5, 3) | (45.2, 69.6) | (−11, 7) | |||
| 500,000 IU | 56.9 | - | 62.1 | 9 | 65.6 | 15 | 56.1 | −1 | |
| (45.1, 71.9) | (48.5, 79.4) | (0, 19) | (52.7, 81.6) | (5, 26) | (45.8, 68.6) | (−10, 8) | |||
| OC (ng/mL) | 50,000 IU | 24.6 | - | 27.1 | 10 | 22.3 | −9 | 19.4 | −21 |
| (20.0, 30.2) | (22.4, 32.8) | (−7, 30) | (14.6, 34.1) | (−23, 8) | (14.1, 26.7) | (−33, −7) | |||
| 150,000 IU | 25.2 | - | 26.4 | 4 | 26.3 | 4 | 23.7 | −5 | |
| (12.0, 28.9) | (22.2, 31.3) | (−12, 23) | (20.7, 33.5) | (−12, 23) | (18.2, 30.7) | (−20, 13) | |||
| 500,000 IU | 25.0 | - | 30.9 | 23 | 27.7 | 11 | 23.8 | −5 | |
| (18.0, 34.9) | (23.7, 40.1) | (5, 45) | (19.7, 39.0) | (−6, 31) | (16.8, 33.7) | (−20, 12) | |||
| CTX-I (ng/mL) | 50,000 IU | 0.43 | - | 0.44 | 2 | 0.41 | −1 | 0.39 | −10 |
| (0.35, 0.54) | (0.33, 0.57) | (−13, 19) | (0.32, 0.53) | (−15, 16) | (0.30, 0.52) | (−22, 5) | |||
| 150,000 IU | 0.53 | - | 0.59 | 6 | 0.51 | −4 | 0.54 | 1 | |
| (0.43, 0.66) | (0.44, 0.79) | (−9, 24) | (0.38, 0.69) | (−7, 12) | (0.39, 0.73) | (−13, 17) | |||
| 500,000 IU | 0.49 | - | 0.62 | 26 | 0.54 | 10 | 0.52 | 6 | |
| (0.35, 0.67) | (0.46, 0.84) | (8, 47) | (0.40, 0.74) | (−6, 29) | (0.38, 0.73) | (−9, 24) | |||
| Visit (Week/Day) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | Week 1 (5 ± 2) | Week 4 (28 ± 3) | Week 12 (84 ± 5) | ||||||
| Variable | Treatment Group | Mean (95% CI) | Difference (95% CI) | Mean (95% CI) | Change (95% CI) | Mean (95% CI) | Change (95% CI) | Mean (95% CI) | Change (95% CI) |
| SPPB | 50,000 IU | 11.2 | - | 11.6 | 0.5 | 11.5 | 0.3 | 11.5 | 0.4 |
| (10.5, 11.8) | (11.2, 12.1) | (−0.3, 1.2) | (11.0, 11.9) | (−0.5, 1.0) | (10.9, 12.2) | (−0.4, 1.1) | |||
| 150,000 IU | 10.1 | - | 10.2 | 0.1 | 10.0 | −0.1 | 10.2 | 0.1 | |
| (8.9, 11.3) | (8.7, 11.7) | (−0.6, 0.8) | (8.5, 11.5) | (−0.8, 0.6) | (8.5, 11.8) | (−0.6, 0.8) | |||
| 500,000 IU | 11.1 | - | 11.2 | 0.1 | 10.4 | −0.7 | 11.1 | 0.0 | |
| (10.3, 11.9) | (10.4, 12.0) | (−0.6, 0.8) | (8.7, 12.0) | (−1.5, 0.003) | (10.4, 11.8) | (−0.7, 0.7) | |||
| Grip Strength (kg) | 50,000 IU | 22.1 | - | 21.9 | −0.1 | 21.4 | −0.6 | 21.2 | −0.9 |
| (18.3, 25.8) | (18.4, 25.4) | (−1.7, 1.5) | (17.9, 25.0) | (−2.2, 1.0) | (18.1, 24.3) | (−2.4, 0.7) | |||
| 150,000 IU | 21.0 | - | 20.2 | −0.8 | 19.5 | −1.4 | 20.9 | 0.1 | |
| (17.9, 24.0) | (17.2, 23.1) | (−2.4, 0.8) | (16.4, 22.7) | (−3.0, 0.1) | (17.9, 23.8) | (−1.7, 1.5) | |||
| 500,000 IU | 21.4 | - | 21.1 | −0.3 | 21.1 | −0.3 | 20.8 | −0.6 | |
| (18.1. 24.6) | (18.3, 23.8) | (−1.9, 1.3) | (18.8, 23.3) | (−1.9, 1.3) | (18.4, 23.1) | (−2.2, 1.0) | |||
| Laying/standing Systolic Blood Pressure Ratio | 50,000 IU | 0.98 | - | 1.03 | 0.05 | 1.05 | 0.06 | 1.04 | 0.05 |
| (0.94, 1.04) | (0.99, 1.07) | (−0.02, 0.11) | (0.97, 1.13) | (−0.01, 0.13) | (0.96, 1.11) | (−0.01, 0.12) | |||
| 150,000 IU | 1.05 | - | 1.02 | −0.03 | 1.01 | −0.03 | 0.99 | −0.06 | |
| (0.99, 1.11) | (0.99, 1.05) | (−0.09, 0.04) | (0.94, 1.09) | (−0.10, 0.03) | (0.91, 1.06) | (−0.13, 0.004) | |||
| 500,000 IU | 1.01 | - | 1.06 | 0.06 | 1.04 | 0.03 | 1.01 | 0.01 | |
| (0.95, 1.06) | (0.99, 1.14) | (−0.01, 0.13) | (0.99, 1.09) | (−0.04, 0.10) | (0.96, 1.06) | (−0.06, 0.07) | |||
| Laying/standing Diastolic Blood Pressure Ratio | 50,000 IU | 0.96 | - | 0.96 | −0.003 | 0.99 | 0.03 | 0.99 | 0.02 |
| (0.88, 1.04) | (0.90, 1.02) | (−0.08, 0.07) | (0.90, 1.08) | (−0.05, 0.10) | (0.93, 1.05) | (−0.05, 0.10) | |||
| 150,000 IU | 0.99 | - | 1.00 | 0.01 | 0.94 | −0.05 | 0.98 | −0.004 | |
| (0.92, 1.05) | (0.93, 1.06) | (−0.06, 0.08) | (0.86, 1.02) | (−0.12, 0.02) | (0.91, 1.06) | (−0.08, 0.07) | |||
| 500,000 IU | 0.95 | - | 0.99 | 0.03 | 0.97 | 0.02 | 0.94 | −0.02 | |
| (0.90, 1.01) | (0.92, 1.06) | (−0.04, 0.11) | (0.91, 1.04) | (−0.05, 0.09) | (0.88, 1.00) | (−0.09, 0.06) | |||
| ARR (ng/dl per ng/mL/h) | 50,000 IU | 4.61 | - | 4.59 | −0.02 | 3.14 | −1.08 | 4.04 | −0.57 |
| (2.66, 6.57) | (2.48, 6.71) | (−1.57, 1.53) | (1.97, 4.31) | (−2.68, 0.52) | (2.20, 5.89) | (−2.12, 0.98) | |||
| 150,000 IU | 3.08 | - | 3.92 | 0.78 | 3.48 | 0.40 | 3.11 | 0.03 | |
| (1.99, 4.18) | (1.47, 6.37) | (−0.77, 2.34) | (2.56, 4.40) | (−1.11, 1.90) | (2.05, 4.17) | (−1.48, 1.53) | |||
| 500,000 IU | 4.98 | - | 4.21 | −0.43 | 4.97 | −0.01 | 4.03 | −0.94 | |
| (1.64, 8.31) | (1.59, 6.82) | (−1.99, 1.12) | (2.81, 7.12) | (−1.51, 1.49) | (2.30, 5.76) | (−2.45, 0.55) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bowles, S.D.; Jacques, R.; Hill, T.R.; Eastell, R.; Walsh, J.S. Effects of High Dose Bolus Cholecalciferol on Free Vitamin D Metabolites, Bone Turnover Markers and Physical Function. Nutrients 2024, 16, 2888. https://doi.org/10.3390/nu16172888
Bowles SD, Jacques R, Hill TR, Eastell R, Walsh JS. Effects of High Dose Bolus Cholecalciferol on Free Vitamin D Metabolites, Bone Turnover Markers and Physical Function. Nutrients. 2024; 16(17):2888. https://doi.org/10.3390/nu16172888
Chicago/Turabian StyleBowles, Simon D., Richard Jacques, Thomas R. Hill, Richard Eastell, and Jennifer S. Walsh. 2024. "Effects of High Dose Bolus Cholecalciferol on Free Vitamin D Metabolites, Bone Turnover Markers and Physical Function" Nutrients 16, no. 17: 2888. https://doi.org/10.3390/nu16172888
APA StyleBowles, S. D., Jacques, R., Hill, T. R., Eastell, R., & Walsh, J. S. (2024). Effects of High Dose Bolus Cholecalciferol on Free Vitamin D Metabolites, Bone Turnover Markers and Physical Function. Nutrients, 16(17), 2888. https://doi.org/10.3390/nu16172888