
Impact of Dietary Patterns on Metabolic Syndrome in Young Adults: A Cross-Sectional Study

 , , ,
, , ,
Abstract

1. Introduction
2. Material and Methods
2.1. Data Sources and Study Population
2.2. Metabolic Syndrome
2.3. Food Frequency Questionnaire (FFQ)
2.4. Physical Activity
2.5. Statistical Analysis
3. Results
3.1. Establishment of Dietary Patterns
3.2. Characteristics of Participants Grouped by Dietary Patterns
3.3. Relationship between Dietary Patterns and Metabolic Syndrome
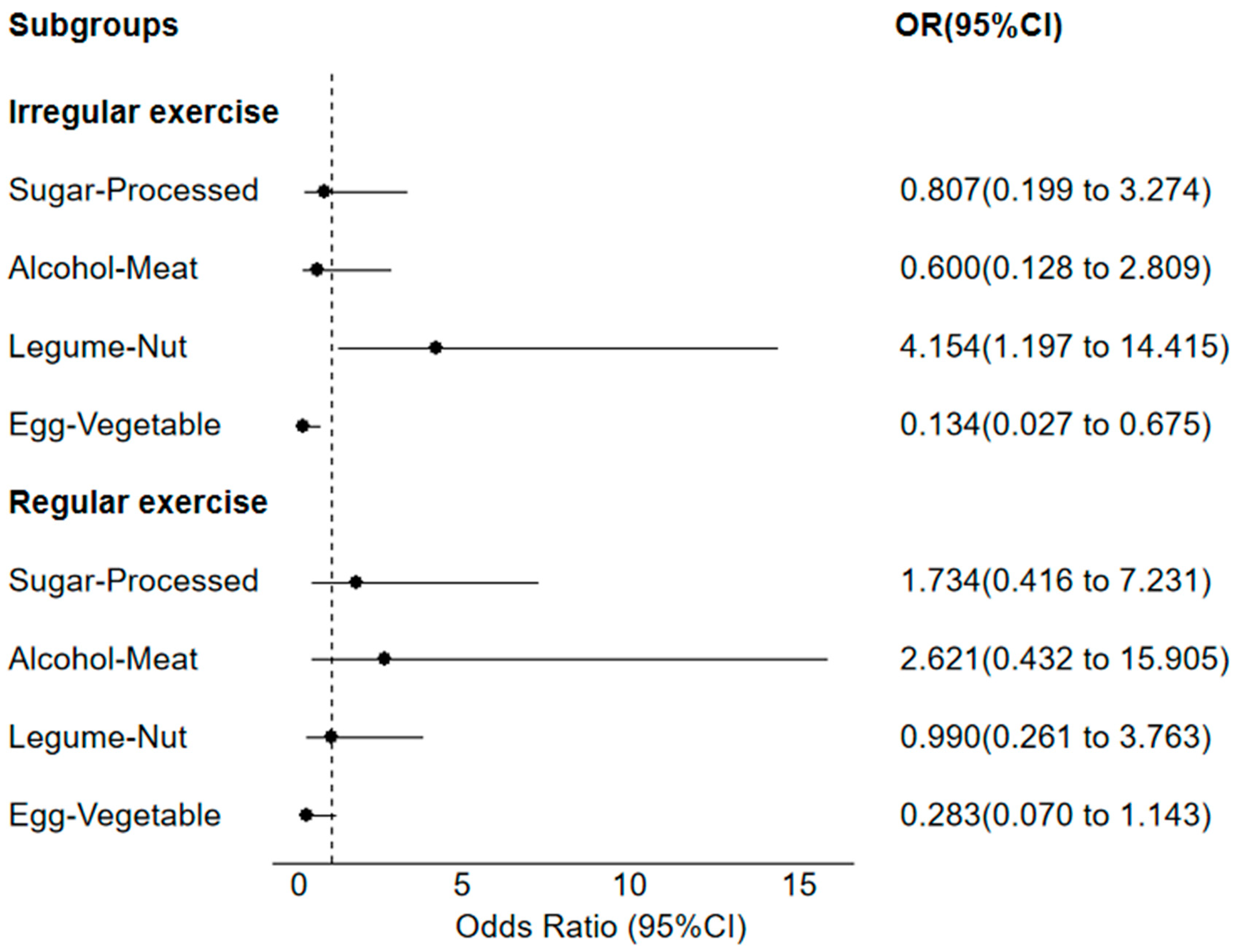
3.4. Subgroup Analysis in Physical Activity Frequency and Metabolic Syndrome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, J.; Gu, D.; Chen, C.S.; Wu, X.; Hamm, L.L.; Muntner, P.; Batuman, V.; Lee, C.H.; Whelton, P.K.; He, J. Association between the metabolic syndrome and chronic kidney disease in Chinese adults. Nephrol. Dial. Transplant. 2007, 22, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Nóbrega da Silva, V.; Goldberg, T.B.L.; Silva, C.C.; Kurokawa, C.S.; Fiorelli, L.N.M.; Rizzo, A.; Corrente, J.E. Impact of metabolic syndrome and its components on bone remodeling in adolescents. PLoS ONE 2021, 16, e0253892. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.M.; Chiou, J.Y.; Kuo, H.W.; Tan, J.Y.; Ko, S.H.; Lee, M.C. Associations Between Unhealthy Lifestyle Behaviors and Metabolic Syndrome by Gender in Young Adults. Biol. Res. Nurs. 2019, 21, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Wu, S.; Song, Y.; Tang, X.; Marshall, R.; Liang, M.; Wu, Y.; Qin, X.; Chen, D.; Hu, Y. Waist circumference, body mass index and waist to hip ratio for prediction of the metabolic syndrome in Chinese. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Sperling, L.S.; Mechanick, J.I.; Neeland, I.J.; Herrick, C.J.; Despres, J.P.; Ndumele, C.E.; Vijayaraghavan, K.; Handelsman, Y.; Puckrein, G.A.; Araneta, M.R.; et al. The CardioMetabolic Health Alliance: Working Toward a New Care Model for the Metabolic Syndrome. J. Am. Coll. Cardiol. 2015, 66, 1050–1067. [Google Scholar] [CrossRef] [PubMed]
- Tal, B.; Sack, J.; Yaron, M.; Shefer, G.; Buch, A.; Ben Haim, L.; Marcus, Y.; Shenkerman, G.; Sofer, Y.; Shefer, L.; et al. Increment in Dietary Potassium Predicts Weight Loss in the Treatment of the Metabolic Syndrome. Nutrients 2019, 11, 1256. [Google Scholar] [CrossRef] [PubMed]
- Stanhope, K.L. Sugar consumption, metabolic disease and obesity: The state of the controversy. Crit. Rev. Clin. Lab. Sci. 2016, 53, 52–67. [Google Scholar] [CrossRef] [PubMed]
- Koopman, R.; van Loon, L.J. Aging, exercise, and muscle protein metabolism. J. Appl. Physiol. (1985) 2009, 106, 2040–2048. [Google Scholar] [CrossRef]
- Savkur, R.S.; Philips, A.V.; Cooper, T.A. Aberrant regulation of insulin receptor alternative splicing is associated with insulin resistance in myotonic dystrophy. Nat. Genet. 2001, 29, 40–47. [Google Scholar] [CrossRef]
- Nazli, S.A.; Loeser, R.F.; Chubinskaya, S.; Willey, J.S.; Yammani, R.R. High fat-diet and saturated fatty acid palmitate inhibits IGF-1 function in chondrocytes. Osteoarthr. Cartil. 2017, 25, 1516–1521. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Rhee, T.M.; Park, H.E.; Han, K.; Choi, S.Y. Association between Cumulative Metabolic Risk Exposure and Cardiovascular Disease: A Nationwide Cohort of Over 3.6 Million Young Adults. Eur. J. Prev. Cardiol. 2024, 00, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Masrouri, S.; Shapiro, M.D.; Khalili, D.; Hadaegh, F. Impact of coronary artery calcium on mortality and cardiovascular events in metabolic syndrome and diabetes among younger adults. Eur. J. Prev. Cardiol. 2024, 31, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Ushula, T.W.; Mamun, A.; Darssan, D.; Wang, W.Y.S.; Williams, G.M.; Whiting, S.J.; Najman, J.M. Dietary patterns and the risks of metabolic syndrome and insulin resistance among young adults: Evidence from a longitudinal study. Clin. Nutr. 2022, 41, 1523–1531. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Livingstone, M.B.E.; Shinozaki, N.; Sugimoto, M.; Fujiwara, A.; Masayasu, S.; Sasaki, S. Food Combinations in Relation to the Quality of Overall Diet and Individual Meals in Japanese Adults: A Nationwide Study. Nutrients 2020, 12, 327. [Google Scholar] [CrossRef] [PubMed]
- Seo, E.H.; Kim, H.; Kwon, O. Association between Total Sugar Intake and Metabolic Syndrome in Middle-Aged Korean Men and Women. Nutrients 2019, 11, 2042. [Google Scholar] [CrossRef] [PubMed]
- Michels, K.B.; Schulze, M.B. Can dietary patterns help us detect diet-disease associations? Nutr. Res. Rev. 2005, 18, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Godoy-Izquierdo, D.; Ogallar, A.; Lara, R.; Rodriguez-Tadeo, A.; Arbinaga, F. Association of a Mediterranean Diet and Fruit and Vegetable Consumption with Subjective Well-Being among Adults with Overweight and Obesity. Nutrients 2021, 13, 1342. [Google Scholar] [CrossRef] [PubMed]
- Pelczynska, M.; Mikulska, A.A.; Czyzewska, K.; Bogdanski, P.; Grzelak, T. The Association of Serum Circulating Neuropeptide Q and Chemerin Levels with Cardiometabolic Risk Factors among Patients with Metabolic Syndrome. Biomolecules 2021, 11. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Ouyang, X.; Lou, Q.; Gu, L.; Ko, G.T.; Mo, Y.; Wu, H.; Bian, R. Anthropometric parameters and their associations with cardio-metabolic risk in Chinese working population. Diabetol. Metab. Syndr. 2015, 7, 37. [Google Scholar] [CrossRef]
- Lee, M.S.; Pan, W.H.; Liu, K.L.; Yu, M.S. Reproducibility and validity of a Chinese food frequency questionnaire used in Taiwan. Asia Pac. J. Clin. Nutr. 2006, 15, 161–169. [Google Scholar]
- Zhao, W.; Hasegawa, K.; Chen, J. The use of food-frequency questionnaires for various purposes in China. Public Health Nutr. 2002, 5, 829–833. [Google Scholar] [CrossRef]
- Hotz, C.; Abdelrahman, L. Simple methods to obtain food listing and portion size distribution estimates for use in semi-quantitative dietary assessment methods. PLoS ONE 2019, 14, e0217379. [Google Scholar] [CrossRef]
- Huang, Q.; Jiang, H.; Zhang, J.; Jia, X.; Huang, F.; Wang, H.; Zhang, B.; Wang, L.; Gu, M.; Huang, Y.; et al. Dietary Patterns Are Associated With Multi-Dimensional Cognitive Functions Among Adults Aged 55 and Older in China. Front. Nutr. 2022, 9, 806871. [Google Scholar] [CrossRef]
- Wang, X.; Li, T.; Li, H.; Li, D.; Wang, X.; Zhao, A.; Liang, W.; Xiao, R.; Xi, Y. Association of Dietary Inflammatory Potential with Blood Inflammation: The Prospective Markers on Mild Cognitive Impairment. Nutrients 2022, 14, 2417. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Zhao, B.; Li, W.; Liu, M.; Chen, L.; Jiang, H.; Li, F.; Wang, S.; Ding, N.; Wang, L.; Wang, Z. [Change of dietary pattern among young people aged 18-35 in China from 1989 to 2018]. Wei Sheng Yan Jiu 2024, 53, 419–434. [Google Scholar] [CrossRef]
- Rippe, J.M.; Angelopoulos, T.J. Sugars, obesity, and cardiovascular disease: Results from recent randomized control trials. Eur. J. Nutr. 2016, 55, 45–53. [Google Scholar] [CrossRef]
- Sievenpiper, J.L. Low-carbohydrate diets and cardiometabolic health: The importance of carbohydrate quality over quantity. Nutr. Rev. 2020, 78, 69–77. [Google Scholar] [CrossRef]
- Reynolds, A.N.; Akerman, A.P.; Mann, J. Dietary fibre and whole grains in diabetes management: Systematic review and meta-analyses. PLoS Med. 2020, 17, e1003053. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.H.; Lin, I.C.; Wu, C.W.; Hung, C.Y.; Liu, W.C.; Wu, C.Y.; Cheng, C.L.; Wu, K.L.H. High fructose induced osteogenic differentiation of human valve interstitial cells via activating PI3K/AKT/mitochondria signaling. Biomed. J. 2022, 45, 491–503. [Google Scholar] [CrossRef] [PubMed]
- Basciano, H.; Federico, L.; Adeli, K. Fructose, insulin resistance, and metabolic dyslipidemia. Nutr. Metab. 2005, 2, 5. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvado, J.; Garcia-Arellano, A.; Estruch, R.; Marquez-Sandoval, F.; Corella, D.; Fiol, M.; Gomez-Gracia, E.; Vinoles, E.; Aros, F.; Herrera, C.; et al. Components of the Mediterranean-type food pattern and serum inflammatory markers among patients at high risk for cardiovascular disease. Eur. J. Clin. Nutr. 2008, 62, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Zibaeenezhad, M.J.; Ghavipisheh, M.; Attar, A.; Aslani, A. Comparison of the effect of omega-3 supplements and fresh fish on lipid profile: A randomized, open-labeled trial. Nutr. Diabetes 2017, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.; Sacks, G.; Ravussin, E. Increased food energy supply is more than sufficient to explain the US epidemic of obesity. Am. J. Clin. Nutr. 2009, 90, 1453–1456. [Google Scholar] [CrossRef] [PubMed]
- Balakrishna, Y.; Manda, S.; Mwambi, H.; van Graan, A. Identifying Nutrient Patterns in South African Foods to Support National Nutrition Guidelines and Policies. Nutrients 2021, 13, 3194. [Google Scholar] [CrossRef]
- Jackson, S.L.; Cogswell, M.E.; Zhao, L.; Terry, A.L.; Wang, C.Y.; Wright, J.; Coleman King, S.M.; Bowman, B.; Chen, T.C.; Merritt, R.; et al. Association Between Urinary Sodium and Potassium Excretion and Blood Pressure Among Adults in the United States: National Health and Nutrition Examination Survey, 2014. Circulation 2018, 137, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Dahl, W.J.; Stewart, M.L. Position of the Academy of Nutrition and Dietetics: Health Implications of Dietary Fiber. J. Acad. Nutr. Diet. 2015, 115, 1861–1870. [Google Scholar] [CrossRef]
- Arentson-Lantz, E.; Clairmont, S.; Paddon-Jones, D.; Tremblay, A.; Elango, R. Protein: A nutrient in focus. Appl. Physiol. Nutr. Metab. 2015, 40, 755–761. [Google Scholar] [CrossRef]
- Torres-Moreno, M.; Torrescasana, E.; Salas-Salvado, J.; Blanch, C. Nutritional composition and fatty acids profile in cocoa beans and chocolates with different geographical origin and processing conditions. Food Chem. 2015, 166, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, A.E.; Gabriel, G.F.; Moreto, F.; Corrente, J.E.; McLellan, K.C.; Burini, R.C. Dietary factors associated with metabolic syndrome and its components in overweight and obese Brazilian schoolchildren: A cross-sectional study. Diabetol. Metab. Syndr. 2016, 8, 58. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Green, B.P.; James, L.J.; Stevenson, E.J.; Rumbold, P.L. The Effect of a Dairy-Based Recovery Beverage on Post-Exercise Appetite and Energy Intake in Active Females. Nutrients 2016, 8, 355. [Google Scholar] [CrossRef]
- Keeble, M.; Adams, J.; Vanderlee, L.; Hammond, D.; Burgoine, T. Associations between online food outlet access and online food delivery service use amongst adults in the UK: A cross-sectional analysis of linked data. BMC Public Health 2021, 21, 1968. [Google Scholar] [CrossRef]
- Holloszy, J.O. Exercise-induced increase in muscle insulin sensitivity. J. Appl. Physiol. (1985) 2005, 99, 338–343. [Google Scholar] [CrossRef]
- Finelli, C.; Tarantino, G. Is there any consensus as to what diet or lifestyle approach is the right one for NAFLD patients? J. Gastrointestin. Liver Dis. 2012, 21, 293–302. [Google Scholar]
- Sjodin, A.M.; Forslund, A.H.; Westerterp, K.R.; Andersson, A.B.; Forslund, J.M.; Hambraeus, L.M. The influence of physical activity on BMR. Med. Sci. Sports Exerc. 1996, 28, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Hawley, J.A.; Lessard, S.J. Exercise training-induced improvements in insulin action. Acta Physiol. 2008, 192, 127–135. [Google Scholar] [CrossRef]
- Kasapis, C.; Thompson, P.D. The effects of physical activity on serum C-reactive protein and inflammatory markers: A systematic review. J. Am. Coll. Cardiol. 2005, 45, 1563–1569. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Sugar–Processed | Alcohol–Meat | Legume–Nut | Egg–Vegetable | |
|---|---|---|---|---|
| Whole Grains | −0.053 | 0.124 | −0.007 | 0.439 |
| Tubers | 0.042 | −0.057 | 0.729 | −0.037 |
| Beans and Bean Products | −0.080 | −0.001 | 0.787 | −0.019 |
| Nuts | 0.158 | 0.181 | 0.678 | 0.002 |
| Fresh Vegetables | −0.102 | −0.483 | 0.334 | 0.483 |
| Fruits | 0.208 | −0.326 | 0.504 | 0.238 |
| White Meat | 0.042 | −0.033 | 0.623 | 0.276 |
| Red Meat | 0.121 | 0.517 | 0.277 | 0.420 |
| Processed Meats | 0.446 | 0.503 | 0.343 | 0.058 |
| Aquatic and Seafood | 0.207 | 0.304 | 0.536 | −0.025 |
| Milk and Dairy Products | 0.376 | −0.547 | 0.170 | 0.309 |
| Eggs | 0.069 | −0.068 | 0.144 | 0.706 |
| Cooking Oils | 0.134 | 0.037 | −0.09 | 0.753 |
| Fried Foods | 0.566 | 0.560 | 0.106 | 0.100 |
| Sugary Beverages | 0.836 | 0.072 | 0.054 | −0.006 |
| Alcoholic Beverages | 0.139 | 0.765 | 0.028 | 0.161 |
| Pastries | 0.791 | 0.044 | 0.077 | 0.048 |
| Characteristics | Total | MetS− N (%) or M ± SD | MetS+ N (%) or M ± SD | p χ2 or t |
|---|---|---|---|---|
| Sample size (N) | 442 | 361 | 81 | |
| Age (years) | 24.79 ± 4.97 | 24.53 ± 4.75 | 25.95 ± 5.74 | 0.041 |
| Gender | 0.344 | |||
| Male | 241 (54.52) | 193 | 48 | |
| Female | 201 (45.48) | 168 | 33 | |
| Height (cm) | 171.97 ± 8.50 | 171.98 ± 8.33 | 171.93 ± 9.26 | 0.958 |
| Weight (kg) | 66.12 ± 14.07 | 64.64 ± 13.17 | 72.70 ± 16.06 | <0.001 |
| Waist circumference (cm) | 77.56 ± 12.77 | 74.58 ± 10.75 | 90.83 ± 12.68 | <0.001 |
| Hypertension | <0.001 | |||
| No | 363 (82.13) | 358 | 5 | |
| Yes | 79 (17.87) | 3 | 76 | |
| Diabetes | <0.001 | |||
| No | 377 (85.29) | 354 | 23 | |
| Yes | 65 (14.71) | 7 | 58 | |
| Dyslipidemia | <0.001 | |||
| No | 380 (85.97) | 357 | 23 | |
| Yes | 62 (14.03) | 4 | 58 | |
| Residence | 0.196 | |||
| Urban area | 310 (70.14) | 258 | 52 | |
| Suburban area | 132 (29.86) | 103 | 29 | |
| Educational level completed | 0.012 | |||
| Junior middle school or below | 113 (25.57) | 85 | 28 | |
| High school or Vocational school | 94 (21.27) | 72 | 22 | |
| Bachelor’s degree or Junior college or above | 235 (53.17) | 204 | 31 | |
| Marital status | 0.017 | |||
| Unmarried | 320 (72.40) | 270 | 50 | |
| Married | 122 (27.60) | 91 | 31 | |
| Smoking status | 0.012 | |||
| No | 332 (75.11) | 280 | 52 | |
| Yes | 110 (24.89) | 81 | 29 | |
| Drinking status | 0.666 | |||
| No | 206 (46.60) | 170 | 36 | |
| Yes | 236 (53.39) | 191 | 45 | |
| Occupation type | 0.042 | |||
| Physical workers | 168 (38.01) | 135 | 33 | |
| Mental workers | 60 (13.57) | 43 | 17 | |
| Students | 214 (48.42) | 183 | 31 | |
| Sleep duration (hours/day) | 7.27 ± 0.82 | 7.47 ± 0.90 | 7.38 ± 1.05 | 0.452 |
| Physical activity frequency | 0.005 | |||
| Monthly or less | 202 (45.70) | 152 | 50 | |
| Weekly | 106 (23.98) | 97 | 9 | |
| 2–3 times per week | 95 (21.49) | 80 | 15 | |
| 4+ times per week | 39 (8.82) | 32 | 7 |
| Characteristics | N | Sugar-Processed | p | Alcohol-Meat | p | Legume-Nut | p | Egg-Vegetable | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1 (n = 111) | Q4 (n = 110) | Q1 (n = 111) | Q4 (n = 110) | Q1 (n = 111) | Q4 (n = 110) | Q1 (n = 111) | Q4 (n = 110) | ||||||
| Age (years) | 24.79 ± 4.97 | 25.41 ± 4.78 | 24.51 ± 5.32 | 0.100 | 23.42 ± 4.77 | 26.15 ± 4.82 | 0.001 | 24.28 ± 4.89 | 23.99 ± 4.73 | 0.033 | 21.86 ± 3.79 | 25.61 ± 5.01 | <0.001 |
| Gender | 0.215 | <0.001 | 0.006 | <0.001 | |||||||||
| Male | 241 | 55 | 65 | 26 | 87 | 49 | 67 | 27 | 84 | ||||
| Female | 201 | 56 | 45 | 85 | 23 | 62 | 43 | 84 | 26 | ||||
| Height (cm) | 171.97 ± 8.50 | 171.49 ± 8.24 | 171.78 ± 8.47 | 0.708 | 167.26 ± 7.75 | 174.87 ± 6.78 | <0.001 | 169.28 ± 8.67 | 174.51 ± 7.52 | <0.001 | 166.93 ± 6.76 | 175.67 ± 8.08 | <0.001 |
| Weight (kg) | 66.12 ± 14.07 | 62.37 ± 13.74 | 71.16 ± 15.20 | <0.001 | 58.10 ± 14.63 | 75.80 ± 12.66 | <0.001 | 63.64 ± 14.82 | 68.89 ± 14.83 | 0.039 | 57.06 ± 12.32 | 74.39 ± 13.19 | <0.001 |
| Waist circumference (cm) | 77.56 ± 12.77 | 75.41 ± 10.02 | 81.42 ± 16.75 | 0.002 | 72.92 ± 11.72 | 82.30 ± 15.69 | <0.001 | 77.00 ± 11.87 | 76.37 ± 15.23 | 0.339 | 72.83 ± 11.65 | 79.25 ± 15.21 | <0.001 |
| Hypertension | 0.028 | 0.110 | 0.131 | 0.750 | |||||||||
| No | 363 | 96 | 80 | 97 | 83 | 99 | 87 | 94 | 87 | ||||
| Yes | 79 | 15 | 30 | 14 | 27 | 12 | 23 | 17 | 23 | ||||
| Diabetes | 0.767 | 0.134 | 0.919 | 0.896 | |||||||||
| No | 377 | 96 | 91 | 100 | 90 | 96 | 92 | 95 | 96 | ||||
| Yes | 65 | 15 | 19 | 11 | 20 | 15 | 18 | 16 | 14 | ||||
| Dyslipidemia | 0.010 | 0.407 | 0.361 | 0.488 | |||||||||
| No | 380 | 103 | 85 | 99 | 91 | 100 | 92 | 91 | 94 | ||||
| Yes | 62 | 8 | 25 | 12 | 19 | 11 | 18 | 20 | 16 | ||||
| Residence | 0.740 | 0.821 | 0.034 | 0.901 | |||||||||
| Urban area | 310 | 80 | 75 | 77 | 74 | 80 | 68 | 80 | 77 | ||||
| Suburban area | 132 | 31 | 35 | 34 | 36 | 31 | 42 | 31 | 33 | ||||
| Educational level completed | 0.004 | 0.498 | 0.046 | 0.446 | |||||||||
| Junior middle school or below | 168 | 15 | 35 | 23 | 30 | 29 | 20 | 22 | 27 | ||||
| High school or Vocational school | 60 | 25 | 26 | 30 | 21 | 28 | 23 | 20 | 25 | ||||
| Bachelor's degree or Junior college or above | 214 | 71 | 49 | 58 | 59 | 54 | 67 | 69 | 58 | ||||
| Marital status | 0.565 | 0.065 | 0.363 | <0.001 | |||||||||
| Unmarried | 320 | 76 | 81 | 86 | 70 | 83 | 84 | 101 | 77 | ||||
| Married | 122 | 35 | 29 | 25 | 40 | 28 | 26 | 10 | 33 | ||||
| Smoking status | 0.037 | <0.001 | 0.220 | <0.001 | |||||||||
| No | 332 | 90 | 80 | 102 | 55 | 88 | 86 | 102 | 74 | ||||
| Yes | 110 | 21 | 30 | 9 | 55 | 23 | 24 | 9 | 36 | ||||
| Drinking status | 0.050 | <0.001 | 0.173 | <0.001 | |||||||||
| No | 206 | 60 | 45 | 75 | 25 | 57 | 56 | 83 | 42 | ||||
| Yes | 236 | 51 | 65 | 36 | 85 | 54 | 54 | 28 | 68 | ||||
| Occupation type | 0.445 | 0.098 | 0.006 | <0.001 | |||||||||
| Physical workers | 168 | 40 | 43 | 33 | 49 | 41 | 30 | 25 | 43 | ||||
| Mental workers | 60 | 18 | 17 | 14 | 16 | 10 | 16 | 8 | 17 | ||||
| Students | 214 | 53 | 50 | 64 | 45 | 60 | 64 | 78 | 50 | ||||
| Sleep duration (hours/day) | 7.45 ± 0.93 | 7.62 ± 0.79 | 7.28 ± 1.07 | 0.055 | 7.57 ± 0.87 | 7.31 ± 1.07 | 0.208 | 7.42 ± 0.92 | 7.47 ± 1.19 | 0.879 | 7.60 ± 1.14 | 7.42 ± 0.88 | 0.323 |
| Physical activity frequency | 0.004 | 0.268 | 0.005 | 0.073 | |||||||||
| Monthly or less | 202 | 40 | 63 | 44 | 54 | 56 | 41 | 40 | 50 | ||||
| Weekly | 106 | 30 | 15 | 30 | 22 | 28 | 20 | 33 | 20 | ||||
| 2-3 times per week | 95 | 26 | 22 | 30 | 20 | 23 | 29 | 31 | 26 | ||||
| 4+ times per week | 39 | 15 | 10 | 7 | 14 | 4 | 20 | 7 | 14 | ||||
| Metabolism Syndrome | 0.023 | 0.071 | 0.125 | 0.996 | |||||||||
| No | 361 | 16 | 31 | 97 | 82 | 99 | 86 | 91 | 89 | ||||
| Yes | 81 | 95 | 79 | 14 | 28 | 12 | 24 | 20 | 21 | ||||
| Energy intake (kcal/day) | 1908.5 ± 710.8 | 1443.0 ± 364.4 | 2632.4 ± 875.5 | <0.001 | 1424.5 ± 402.7 | 2622.0 ± 879.5 | <0.001 | 1694.2 ± 580.2 | 2341.2 ± 967.5 | <0.001 | 1475.0 ± 527.8 | 2462.9 ± 852.5 | <0.001 |
| Cluster | Model 1 | p | Model 2 | p | Model 3 | p | |
|---|---|---|---|---|---|---|---|
| OR, 95% CI | OR, 95% CI | OR, 95% CI | |||||
| Sugar–Processed | Q1 | ref | ref | ref | |||
| Q4 | 2.33 (1.19, 4.57) | 0.014 | 2.24 (1.11, 4.51) | 0.025 | 1.10 (0.42, 2.84) | 0.849 | |
| Alcohol–Meat | Q1 | ref | ref | ref | |||
| Q4 | 2.37 (1.17, 4.79) | 0.017 | 2.49 (1.13, 5.51) | 0.024 | 1.29 (0.45, 3.70) | 0.635 | |
| Legume–Nut | Q1 | ref | ref | ref | |||
| Q4 | 2.30 (1.09, 4.88) | 0.029 | 2.48 (1.14, 5.40) | 0.022 | 2.63 (1.08, 6.37) | 0.033 | |
| Egg–Vegetable | Q1 | ref | ref | ref | |||
| Q4 | 1.07 (0.55, 2.12) | 0.837 | 1.22 (0.57, 2.64) | 0.608 | 0.26 (0.10, 0.70) | 0.007 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, J.; Lu, W.; Lv, Q.; Wang, Y.; Xu, X.; He, Y.; Chang, H.; Zhao, Y.; Zhang, X.; Zang, X.; et al. Impact of Dietary Patterns on Metabolic Syndrome in Young Adults: A Cross-Sectional Study. Nutrients 2024, 16, 2890. https://doi.org/10.3390/nu16172890
Liu J, Lu W, Lv Q, Wang Y, Xu X, He Y, Chang H, Zhao Y, Zhang X, Zang X, et al. Impact of Dietary Patterns on Metabolic Syndrome in Young Adults: A Cross-Sectional Study. Nutrients. 2024; 16(17):2890. https://doi.org/10.3390/nu16172890
Chicago/Turabian StyleLiu, Jingwen, Wenfeng Lu, Qingyun Lv, Yaqi Wang, Xueying Xu, Yuan He, Hairong Chang, Yue Zhao, Xiaonan Zhang, Xiaoying Zang, and et al. 2024. "Impact of Dietary Patterns on Metabolic Syndrome in Young Adults: A Cross-Sectional Study" Nutrients 16, no. 17: 2890. https://doi.org/10.3390/nu16172890
APA StyleLiu, J., Lu, W., Lv, Q., Wang, Y., Xu, X., He, Y., Chang, H., Zhao, Y., Zhang, X., Zang, X., & Zhang, H. (2024). Impact of Dietary Patterns on Metabolic Syndrome in Young Adults: A Cross-Sectional Study. Nutrients, 16(17), 2890. https://doi.org/10.3390/nu16172890